
Abstract
Purpose
To facilitate effective learning, feedback on performance during arthroscopic training is essential. Less attention has been paid to feedback on monitoring safe handling of delicate tissues such as meniscus. The goal is to measure in vitro probing forces of menisci and compare them with a theoretical maximum probing force (TMPF).
Method
Menisci samples of ten cadavers were mounted on force platforms to measure probing forces up to 20 N in three directions. Nineteen subjects participated: six novices (experience <60 arthroscopies), ten intermediates (>60 arthroscopies), and three faculty (>250 a year). All had to perform three tasks on each meniscus sample with an arthroscopic probe: push three times on the superior meniscal surface, perform one continuous run on the superior meniscal surface, and push three times on the inferior meniscal surface. The absolute maximum probing force (AMPF) was determined for each condition. A multivariable linear regression analysis was performed to assess the influence of experience on the force magnitude (P < 0.05). AMPFs were compared to the TMPF (estimated to be 8.5 N).
Results
The AMPF of the push task was on average 2.8 N (standard deviation (SD) of 0.8 N), of the continuous run task 2.5 N (SD 0.9 N), and of the pull task 3.9 N (SD 2.0 N). Significant difference was present between experts and novices (P < 0.05). The AMPFs are in the same order of magnitude as the TMPF.
Conclusion
The results indicate the necessity of using a safety level for tissue manipulation when training arthroscopy and a value for is magnitude.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Feedback on performance is crucial to stimulate and support an efficient learning process of the trainee in arthroscopy. This is preferably done in a direct and systematic manner [7, 11]. For learning arthroscopy, this implies that the trainee’s performance can be subdivided into two categories: (a) capability of effective and efficient task completion and (b) guarantee patient safety.
Patient safety can be defined as prevention of damaging healthy tissues in the intra-articular joint space and around the access portals when performing surgical treatment. Meniscal and cartilage tissue especially need to be monitored for unintentional damage as they have little to no healing potential and are frequently probed even outside the arthroscopic view. Tissue damage occurs if the tissue is loaded with magnitudes beyond the tissue’s strength. Consequently, the magnitude of probing force qualifies as objective parameter for monitoring safety.
To facilitate adequate training, medical simulators should provide natural sensory feedback to train these specific arthroscopic skills. Apart from a natural appearance of the anatomic structures to offer realistic visual cues, the presence of realistic tactile feedback in an arthroscopy simulator is considered essential to imitate clinical practice adequately [10, 17]. Unfortunately, little to no quantitative data are available to set the maximum tolerable probing forces for safe manipulation, which can be used for training purposes [14]. Chami et al. [3] have measured forces exerted when performing a knee arthroscopy in vivo. However, the meniscal probing forces cannot be determined from these data, because measurements took place with a sensor attached to the handle of the probe. As a result, combined forces and moments were measured, so-called navigation forces and procedure force features (including probing force of meniscal tissue), which could not be discriminated [3]. The goal of this study is firstly to determine quantitative values of meniscal probing forces and secondly to compare those values with a theoretical maximum probing force. From these results, a guideline for safe manipulation of human menisci can be determined (and integrated in medical simulators). As in vivo measurement of meniscal probing forces is difficult, variations in meniscal probing forces were measured on cadaveric material.
Materials and methods
Theoretical maximum probing force (TMPF)
Meniscus tissue is a viscoelastic material with a non-linear relation between force and displacement [2, 5]. Macroscopic damage or rupture of the meniscus will be caused by a punching process where the meniscus is torn along the circumferential plane of the instrument in line with the probing force [16]. The punching process starts with elastic deformation of the tissue, followed by plastic deformation, and finally, pure shearing causes tissue rupture. To remain in a safe deformation zone with no chance of tissue damage, the probing force may not exceed the elastic deformation zone. As the transition between elastic and plastic deformation is difficult to determine, we propose the following. The TMPF is determined as the minimum force that is required to actually rupture meniscal tissue when pressing it with a probe. This can be calculated as follows:
where F is the resulting force, τ men is the shear stress for punching meniscal tissue, and A is the circumferential surface of the tissue that is punched. Equation (1) shows that an instrument with a small value of A requires less force to cause tissue rupture. As the probe has the smallest area (A) compared to other arthroscopic instruments, we chose this instrument to perform calculations for the value of TMPF. As a consequence, A is determined by the diameter of the tip of the probe (d) and displacement of the meniscal tissue beyond the elastic deformation zone caused by pressing the probe tip into the tissue (t). d is typically 1.5 mm, and the length of the hook of the tip is typically 3.5 mm. Results of force–displacement curves measured on cadaveric menisci showed that up to ~3 mm, a relative small force (<5 N) is required to deform the tissue [16]. This depth of 3 mm will be used as the limit for pure elastic deformation, leaving a maximum t of 0.5 mm that can cause undesired deformation (i.e., rupture). Furthermore, a mean shear stress of 6.9 N/mm2 (standard deviation (SD) 1.1) was determined for punching cadaveric menisci [16]. Taking into account the weakest menisci, the minimum shear stress is calculated as the mean shear stress minus three times its SD, which equals 3.6 N/mm2. Using Eq. 1, a TMPF of F is 8.5 N that can potentially cause meniscal tissue damage. Thus, this force level should not be exceeded for safe tissue manipulation.
Experiment
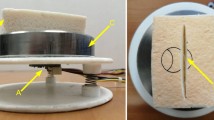
Ten menisci were acquired from previously freshly frozen cadaveric knees. Demographic data of the cadavers were five men vs. five women with age of death between 68 and 86 years. Fithian et al. [5] indicated the presence of significant difference in material properties between lateral and medial menisci. By choosing five lateral and five medial intact menisci for this experiment, the potential influence of different material properties on the variation in probing forces can be determined. The menisci were kept moist with saline solution in between each test cycle. A pair consisting of one lateral and one medial meniscus (from two different cadavers) was mounted on a custom-made fixation plate of aluminum (Fig. 1). Each meniscus was firmly secured with two clamps combined with needles to prevent slip. Thus, anatomic attachment was imitated as closely as possible. The fixation plate was mounted on a platform system with a single screw. To simulate the arthroscopic situation, a Perspex cylinder was placed over the force platform system in which access portals were made through which a routinely used probe could be inserted (Fig. 1). Only the probing forces were recorded exerted by the tip of the probe on the tissue with a force platform that was specifically developed as an affordable tool to monitor force parameters for tissue manipulation tasks [8]. The force platform consists of an optoelectronic 6D mouse that is surrounded by three springs that determine the maximum force range. For this study, springs were selected that allowed measurement up to 20 N in three directions: x- and y-directions in the horizontal plane perpendicular to each other and the vertical z-direction that corresponds to a perfect push–pull direction (Fig. 1). The force platform has a mean accuracy for measuring forces of 0.1 N. A threshold set at 0.7 N prevents the untouched force platform from drifting. Until this threshold force is reached, the output values are zero. Forces were recorded on a notebook PC at a rate of 60 Hz with custom-made software written in C++. The force platform is easy to build, affordable, accurate, and sensitive enough to reflect the differences in maximal probing force. In total, five such force platforms were set up with different menisci samples.

One of the five force platforms with two menisci mounted. a Perspex cylinder with several portals to probe the meniscus located on the opposite site. b Meniscus sample. c Clamps to mount the menisci securely to the fixation plate. d Force platform with on the left the coordinate system indicating the directions of force measurement
Nineteen participants were recruited at the annual Total Knee Arthroplasty residency course at the Academic Medical Centre (Amsterdam, The Netherlands) in November 2009. They were divided into three groups having different levels of arthroscopic experience: Novices who were residents that had performed up to 60 arthroscopies (n = 6), intermediates who had performed more than 60 arthroscopies (n = 10), and faculty who had performed more than 250 arthroscopies a year (n = 3). This boundary level of 60 arthroscopies was based on the average opinion of fellowship directors who were asked to estimate the number of operations that should be performed to allow a trainee to perform unsupervised meniscectomies [12].
The participants were asked to fill out a short questionnaire, indicating their sex (all were male), dominant hand (16 right vs. 3 left), their glove size (4 had size 7.5, 12 had size 8, and 1 had size 8.5), their experience, and to indicate a safety factor as percentage of the maximum probing force. Each participant was asked to perform one sequence of three probing tasks on each of the 10 menisci (Fig. 2). The tasks were chosen from the protocol as described by Chami et al. [3]:

Probing sequence on one meniscus sample. The arrows indicate the motion direction of the arthroscopic probe. a Push the middle superior meniscal surface. b Continuous run on the superior meniscal surface back and forth. c Pull the middle inferior meniscal surface
-
Push—Probe middle superior meniscal surface (3 subsequent repetitions)
-
Continuous run on superior meniscal surface (1 time back and forth)
-
Pull—probe/lift middle inferior meniscal surface (3 subsequent repetitions)
Explicit instructions were given to probe the menisci with the force they would normally apply during a knee arthroscopy. With this protocol, a participant could complete the test in less than 10 min. The participants were asked to indicate a safety factor as a percentage of the TMPF to guarantee safe manipulation in all cases.
Statistical analysis
The data were processed with Matlab (version 7.0.4.365 (R14), The Mathworks, Natick, USA) and SPSS (15.0.1, SPSS Inc., Chicago, IL, USA). The force signals in x-, y- and z-directions were filtered with a second-order Butterworth filter with a normalized cut-off frequency of 0.1 to suppress high-frequency noise. The absolute maximum probing force (AMPF) was calculated from the force components in the three directions for each of the three tasks per participant and per meniscus (total of 570 measurements).
The presence of normal distributions was determined with the Kolmogorov–Smirnov test. Based on exploration of the data, we dichotomized for subsequent menisci: Phase 1 consists of probing menisci 1–4 and Phase 2 consists of probing menisci 5–10. Subsequently, a multivariable linear regression analysis with backward selection procedure was performed to determine the factors that significantly influenced the AMPFs of the push, continuous run, and pull task. The factors, experience and phase, were initially tested in a univariate analysis and, when significantly associated with the AMPFs, entered in the multivariable regression model. Univariate level of significance was set at 0.1 to enter the multivariate model. The level of significance was set at 0.05 for factors in the multivariable model. Finally, the means added with two times the standard deviations of the AMPFs of Phase 2 were calculated per task and experience level. These represent the maximum probing levels within a group of orthopedic surgeons and were compared with the TMPF.
Results
Typical force patterns were found for each of the three tasks (Fig. 3), where the push task has three peaks, the continuous run has a less distinctive pattern, and the pull task has a plateau with oscillation or also shows three peaks. The plateau with oscillation pattern is a result of the fact that some participants kept a base pull load on the meniscus. The continuous run task requires the smallest forces and the pull task the highest forces. The intermediate pulls harder on the meniscus compared to the expert, and the novice uses overall less force than the expert and intermediate (Fig. 3).

Typical force patterns of a probing sequence (three tasks) performed on one meniscus sample by an expert, an intermediate, and a novice. In these graphs, the force components in the x-, y-, and z-directions (Fig. 1) are shown, where the z-direction corresponds to a perfect push–pull direction. A negative force value indicates a push action, and a positive value indicates a pull action
No significant difference was found for AMPF levels between the menisci samples per task, which implies that the variation between the participants was dominant for loading levels. The multivariable linear regression analysis demonstrated that Phases 1 and 2 had significantly different absolute forces for all three tasks (P < 0.05), where the push and continuous run task were performed with higher forces in Phase 2, and the pull task with lower forces (Table 1). This indicates the presence of a learning curve in task performance. Statistically significant differences were found between the novices and experts (P < 0.05), where the experts performed all tasks with higher forces (Table 1). Additionally, a significant difference was found between the forces applied by the intermediates vs. the experts for the continuous run task.
The maximum probing force levels of AMPF per task and experience ranged from 3.4–9.1 N (Fig. 4). These are in the same order of magnitude compared to the value of 8.5 N as calculated for the TMPF; and for one condition (pull task executed by intermediates), this value is exceeded. The participants indicated a safety factor as percentage of the TMPF: subgroup: experts (20%) that equals a maximum safe probing force of 6.8 N, intermediates (10–80%) that equals 1.7–7.7 N, and novices (10–60%) that equals 1.7–3.4 N.

Results of the absolute maximum probing forces (AMPF) for each of the three tasks of Phase 2 per experience level. The means are plotted with two times the standard deviation. The horizontal black line represents the theoretical maximum probing force (TMPF), which was calculated to be 8.5 N
Discussion
The most important finding of the present study was that the use of a safety level for probing tissue with minimal healing potential is necessary during arthroscopic training, and based on this study, forces exceeding 8.5 N should be avoided. Arthroscopic probing force of menisci could serve as objective parameter to monitor safe manipulation. The difference in AMPF per meniscus and task was not significant and small compared to the variation between AMPF levels of the surgeons. But a clear distinction was found between the AMPFs of the first 4 menisci compared (Phase 1) to the last 6 (Phase 2) per experience level (Table 1). The fact that there was also a difference for the expert group between Phase 1 and Phase 2 indicates that a learning curve was present for all participants to familiarize with the experimental setup even though the tasks were fairly simple and the arthroscopic situation was imitated as closely as possible. Therefore, only the results of the last six menisci were used for comparison with the maximum probing forces (Table 1).
For the push task, the AMPF was on average 2.8 N (standard deviation (SD) of 0.8 N), for the continuous run task 2.5 N (SD 0.9 N), and for the pull task 3.9 N (SD 2.0 N). Comparison of these data with those by Chami et al. [3] is possible, if it is assumed that the moment arm of the probe inside the medial portal when probing the medial meniscus is between 30 and 50 mm. Using the torques registered in that study for the expert surgeon, the average force for probing the superior surface is estimated between 2.8 and 4.7 N and for the inferior surface is between 1.8 and 3.0 N. As these values are similar to the forces measured in this study, the experimental setup appears to be valid for representing the real-life situation adequately. Tashiro et al. [14] investigated the possibility of the use of force data to use as performance measure for arthroscopic training. Forces were measured during arthroscopic probing of artificial menisci on a knee bench model. The peak forces measured during this task were in order of 15–18 N. The difference in magnitude compared with our study is caused by the fact that their force sensor measured all forces exerted on the knee bench model, thus not isolating meniscal probing force.
In order to determine the necessity of monitoring safe tissue manipulation, the maximum probing levels per task and experience level were compared with the TMPF (Fig. 4). Their range lays in the same order of magnitude. As the TMPF is estimated, it would be recommended to correct this value with a safety factor. In engineering, using a safety factor of 50% is common approach to guarantee that for example a structure will not collapse. The participants were also asked to indicate a safety factor, but their answers varied largely, maybe because their unfamiliarity with this approach. Even if the safety factor is chosen according to the suggestion of the three experts (20%), the maximum probing force for safe tissue manipulation is close the measured maximum AMPF. This confirms the necessity of monitoring probing forces to train safe arthroscopic tissue manipulation. Another interesting result is that the experts showed more pronounced AMPFs compared to the novice group. This result is in accordance with two other studies by Chami et al. [3, 4] who concluded that this difference was larger for difficult tasks. In addition to preventing tissue overloading, monitoring of the arthroscopic probing forces can also be used to encourage novices to probe more firmly for proper diagnosis of the tissue quality.
This study has limitations. All measurements were taken on cadaveric tissue, which is usually stiffer and therefore might have resisted higher forces. On the other hand, the tissue was recruited from elderly whose general conditions are usually less than young healthy people. Giving the fact that the difference between the probing forces on the different menisci samples was not significant and compared to an in vivo study [3] was in the same order of magnitude, it is suggested that the results can be safely used for arthroscopic training purposes. Another weakness is the small number of experts that participated and number of menisci that could be used. However, their probing behavior was similar and showed the least variation. Furthermore, we were aiming to measure a range of probing forces as possible to determine if setting a safety level would be relevant. In that sense, the force patterns from less-experienced surgeons were more important. Five force platforms were available, which limited the study to include ten different menisci samples. However, the results of the study indicate that the differences in the probing forces were not significant between the menisci but were dominated by differences between the surgeons. As it is acknowledged that arthroscopic skills should be preferably trained by including the handling of actual instruments [13], medical simulators are attractive candidates to facilitate this. But before they can be used on a large scale, their degree of realism should be sufficient and their capability of performance tracking should be well defined and complete. At this stage, attention has mainly been paid to task completion. This study focuses on an equally important performance category: guaranteeing patient safety. It confirms that arthroscopic probing forces can be used as an objective measure to monitor safe tissue manipulation. This is in agreement with the study by Tashiro et al. [14]. The exact maximum allowable safe probing level remains to be determined, as this partly depends on the safety factor that is chosen, but based on this study values exceeding 8.5 N should be avoided. Both virtual and physical medical simulators can benefit by implementing the results into their performance monitoring systems [1, 6, 9, 14, 15]. This way not only task completion can be monitored, but safe tissue manipulation as well, which is equally important.
Conclusion
The results indicate that it is necessary to use a safety level for tissue manipulation when training arthroscopy and that a force exceeding 8.5 N should be avoided when probing meniscus tissue.
References
Bayona S, Fernandez-Arroyo JM, Martin I, Bayona P (2008) Assessment study of insightARTHRO VR arthroscopy virtual training simulator: face, content, and construct validities. J Rob Surg 2:151–158
Buchner M (2009) Aktueller Stand der arthro- skopischen Meniskuschirurgie. Sport Orthop Traum 25:171–178
Chami G, Ward J, Wills D, Phillips R, Sherman K (2006) Smart tool for force measurements during knee arthroscopy: in vivo human study. Stud Health Technol Inform 119:85–89
Chami G, Ward JW, Phillips R, Sherman KP (2008) Haptic feedback can provide an objective assessment of arthroscopic skills. Clin Orthop Relat Res 466:963–968
Fithian DC, Kelly MA, Mow VC (1990) Material properties and structure-function relationships in the menisci. Clin Orthop Relat Res 252:19–31
Gomoll AH, Pappas G, Forsythe B, Warner JJ (2008) Individual skill progression on a virtual reality simulator for shoulder arthroscopy: a 3-year follow-up study. Am J Sports Med 36:1139–1142
Harewood GC, Murray F, Winder S, Patchett S (2008) Evaluation of formal feedback on endoscopic competence among trainees: the EFFECT trial. Ir J Med Sci 177:253–256
Horeman T, Rodrigues S, Jansen F, Dankelman J, Dobbelsteen Jvd (2010) Force measurement platform for training and assessment of laparoscopic skills. Surg Endosc PMID: 20464416
Howells NR, Gill HS, Carr AJ, Price AJ, Rees JL (2008) Transferring simulated arthroscopic skills to the operating theatre: a randomised blinded study. J Bone Joint Surg Br 90:494–499
Moody L, Waterworth A, McCarthy AD, Harley P, Smallwood R (2008) The feasibility of a mixed reality surgical training environment. Virtual Reality 12:77–86
O’Connor A, Schwaitzberg SD, Cao CG (2008) How much feedback is necessary for learning to suture? Surg Endosc 22:1614–1619
O’Neill PJ, Cosgarea AJ, Freedman JA, Queale WS, McFarland EG (2002) Arthroscopic proficiency: a survey of orthopaedic sports medicine fellowship directors and orthopaedic surgery department chairs. Arthroscopy 18:795–800
Pedowitz RA, Esch J, Snyder S (2002) Evaluation of a virtual reality simulator for arthroscopy skills development. Arthroscopy 18:E29
Tashiro Y, Miura H, Nakanishi Y, Okazaki K, Iwamoto Y (2009) Evaluation of skills in arthroscopic training based on trajectory and force data. Clin Orthop Relat Res 467:546–552
Tuijthof GJ, van Sterkenburg MN, Sierevelt IN, van OJ, van Dijk CN, Kerkhoffs GM (2010) First validation of the PASSPORT training environment for arthroscopic skills. Knee Surg Sports Traumatol Arthrosc 18:218–224
Tuijthof G, Meulman H, Herder J, van Dijk C (2009) Meniscal shear stress for punching. J Appl Biomat Biomech 7:97–103
Zivanovic A, Dibble E, Davies B, Moody L, Waterworth A (2003) Engineering requirements for a haptic simulator for knee arthroscopy training. Stud Health Technol Inform 94:413–418
Acknowledgments
The authors wish to thank the five students from Delft University of Technology that helped to make this experiment a success.
Conflict of interest
None of the researchers or an affiliated institute has received (or agreed to receive) from a commercial entity something of value related in any way to this manuscript or research. The authors did not have any financial and personal relationships with other people or organizations that could inappropriately influence (bias) their work.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Tuijthof, G.J.M., Horeman, T., Schafroth, M.U. et al. Probing forces of menisci: what levels are safe for arthroscopic surgery. Knee Surg Sports Traumatol Arthrosc 19, 248–254 (2011). https://doi.org/10.1007/s00167-010-1251-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-010-1251-9