
Abstract
Objective
To assess the role of the water environment in the Pseudomonas aeruginosa colonization of patients in intensive care units in the absence of a recognized outbreak.
Design and setting
Prospective, single-centre study over an 8-week period in two adult ICUs at a university hospital. Environmental samples were taken from the water fittings of rooms once per week, during a 8-week period. Patients were screened weekly for P. aeruginosa carriage. Environmental and humans isolates were genotyped by using pulsed-field gel electrophoresis.
Results
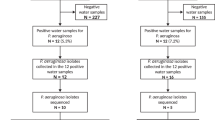
P. aeruginosa was detected in 193 (86.2%) of the 224 U-bend samples and 10 of the 224 samples taken from the tap (4.5%). Seventeen of the 123 patients admitted were colonized with P. aeruginosa. Only one of the 14 patients we were able to evaluate was colonized by a clone present in the water environment of his room before the patient's first positive sample was obtained.
Conclusion
The role of the water environment in the acquisition of P. aeruginosa by intensive care patients remains unclear, but water fittings seem to play a smaller role in non-epidemic situations than expected by many operational hospital hygiene teams.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In the past few decades, Pseudomonas aeruginosa has become a major hospital pathogen, due to both the number and severity of the infections it causes. A national prevalence survey indicated that P. aeruginosa was responsible for 10% of all nosocomial infections in France, only slightly fewer than Escherichia coli and Staphylococcus aureus [1]. In the hospital setting, intensive care units (ICUs) have a high endemic potential for this bacterium, which causes 18% of nosocomial infections in such units, versus only 6% in surgical and non-surgical units [2]. In many departments, P. aeruginosa is frequently involved in broncho-pulmonary infections and, to a lesser extent, urinary infections, infections of surgical sites, and bacteremia. The severity and excess mortality observed in cases of pulmonary infection and bacteremia are due to a combination of the intrinsic properties of the bacteria – virulence factors and the natural resistance to antibiotics – and the immunocompromized status of the infected patients [3].
P. aeruginosa is an environmental bacterium. It exists as a saprophyte on damp soil, plant material, and in freshwater, wastewater, and seawater [4]. It is independent of humans but may be found as a commensal organism in the digestive tract. P. aeruginosa is rarely carried by subjects in good health, being found in only 2–10% of individuals, whereas it may be found in 50–60% of hospitalized patients, particularly on burns and scabs. The survival of P. aeruginosa seems to be particularly favored by damp environments, such as sinks, taps, shower heads, and other water fittings [5, 6]. This enables this bacterium to contaminate medical and surgical equipment, hospital fittings, and other material [7]. Numerous hospital outbreaks have been blamed on the colonization of diverse items of equipment and/or damp materials [8, 9]. As a result, many hospital hygiene teams place great emphasis on the role of water in all infections with P. aeruginosa, particularly those occurring in ICUs in the absence of an outbreak.
The aim of this study was to evaluate the role of the water environment on the colonization of patients hospitalized in ICUs in the absence of a recognized epidemic.
Materials and methods
Background
This study was carried out in the two adult ICUs (one surgical and one medical) at Besançon University Hospital. Each of these two units has 15 beds, all of which are in individual rooms for the surgical ICU, with two double rooms for the medical ICU. This study was carried out (collection of data and strains) over 8 weeks, from 20 February to 10 April 2006. It was approved by the hospital's review board.
Design of the study
Environmental samples were taken weekly from the water fittings of the rooms, regardless of the P. aeruginosa infection status of the patients in the rooms. P. aeruginosa colonization status was monitored by testing samples taken for diagnostic purposes and samples taken weekly for screening purposes. We tested for isogenicity between clinical and environmental samples by determining macrorestriction profiles of total DNA, by pulsed-field gel electrophoresis (PFGE).
Clinical samples
The clinical samples tested were taken for diagnostic and epidemiological (screening) purposes. Diagnostic samples were not taken systematically: they were taken only if there were clinical reasons to suspect infection, and the sampling site was chosen according to the site of suspected infection. Screening samples were taken systematically on admission of the patient to the ICU and once per week thereafter, throughout the patient's stay. They were taken from the nose, the rectum, and from tracheal aspirates. Colonization was defined as a positive result for at least one sample.
Environmental samples
Two types of environmental samples were taken once per week from the water fittings in each intensive care room: 10 ml of water from the U-bend under the sink and 150 ml of cold water taken directly from the tap immediately after activating. The various volumes of water sampled were collected into sterile flasks containing sodium thiosulphate to inhibit the effects of water chlorination.
Culture
Diagnostic samples were plated on agar Columbia broth supplemented with 5% horse blood. Screening samples were plated on agar Muëller–Hinton broth. Environmental samples were plated on cetrimide agar after filtration and 24 h enrichment in trypticase-soy (TS) broth. Cetrimide agar plates were incubated for 72 h at 41°C.
Identification
Cetrimide agar is selective for P. aeruginosa, but other bacterial species may nevertheless develop. Identification of P. aeruginosa was based on positive oxidase activity, resistance to kanamycin, growth at 41°C and not at 4°C, and confirmed by biochemical tests (ID 32 GN, Biomérieux, Marcy l'étoile, France).
Genotyping
Isolates were typed by determination of their total DNA macrorestriction profile (pulsotype) following digestion with DraI (Boehringer, Mannheim, Germany) as assessed by PFGE (CHEF DRIII, Bio-Rad Ivry sur Seine, France), according to a technique previously developed by our laboratory [10]. We used Gel-Compar (Applied Math, Kortrijk, Belgium) to establish a similarity matrix for the DNA based on calculation of the Dice coefficient (pairwise comparison of strains). A dendrogram was generated with the UPGMA (unweighted pair group using arithmetic means) hierarchical algorithm. We compared gels using S. aureus NCTC 8325 as a reference strain. Typing results were interpreted according to international recommendations [11].
Definitions
Clones including clinical isolates were defined as sporadic if they were isolated from only a single patient, microepidemic if they were found in two or three patients, and epidemic if from more than three patients. Clones including environmental isolates were defined as unique if the isolates were found in a single room and multiple if the isolates were present in several rooms.
Statistical analysis
The data were analyzed with EpiInfo version 6.04 (EpiInfo, CDC, Atlanta, GA, USA). Confidence intervals were calculated by the quadratic method of Fleiss.
Results
Incidence of colonization/infection
In total, 123 patients were admitted to the two ICUs (69 to the medical unit and 54 to the surgical unit) for a total of 1416 days of hospitalization (720 in the medical unit and 696 in the surgical unit). Seventeen patients (8 in the medical unit and 9 in the surgical unit) presented at least one sample positive for P. aeruginosa. The overall incidence of colonization was 13.8 (range 8.5–21.5) per 100 patients admitted: 11.6 (range 5.5–22.1) for the medical unit and 16.66 (range 8.4–29.8) for the surgical unit. The overall incidence density was 12.0 (range 7.2–19.6) per 1000 days of hospitalization: 11.1 (range 5.9–22.7) for the medical unit and 12.93 (range 8.3–25.3) for the surgical unit. In total, 63 samples tested positive for P. aeruginosa: 46 screening samples from 16 patients and 17 diagnostic samples from 7 patients.
Positivity of the water environment
In total, 448 samples were taken from both ICUs. P. aeruginosa was detected in 193 (86.2%) of the 224 U-bend samples and 10 of the 224 samples taken from the tap (4.5%; Table 1). More than half the samples taken from U-bends contained more than one strain of P. aeruginosa, with some samples containing up to four strains. Permanent colonization of the U-bend was observed in five of the 28 rooms. Two of these rooms were in the surgical ICU and the other three were in the medical ICU.
Molecular typing
The clinical isolates belonged to 17 clones. Sixteen of these 17 clones were sporadic (isolated from a single patient), and one clone was microepidemic including isolates from two patients. We typed 203 environmental isolates in all. These 203 environmental isolates belonged to 82 pulsotypes – 37 present in the medical ICU, 33 in the surgical ICU and 12 in both units; 54 of these 82 pulsotypes were isolated only once – 29 in the medical unit and 25 in the surgical unit – and the other 28 pulsotypes were multiple. Eight of these strains were present in the medical unit, 8 in the surgical unit, and 12 were present in both units (Table 1). Only two multiple clones included both clinical and environmental isolates: one was isolated from 7 environmental samples and 1 patient, and the other was isolated from 8 environmental samples and 2 patients. The time course of colonization was investigated by considering the timing of the clinical and environmental samples taken for the 17 patients colonized with P. aeruginosa (Table 2). Only 1 patient was colonized with a clone present in the water environment of his room before he gave his first positive sample. In the 3 cases without environmental sample E1, the environment perhaps acted as a reservoir, too. The environment was therefore a possible reservoir for the colonization of patients in 1 of 14 cases. In half the cases, the water environment (U-bends and taps) of the room contained several clones of P. aeruginosa. For a given water fitting, in 9 cases of 10, the tap and the U-bend were colonized with identical clones.
Discussion
In this study, the incidence of colonization by P. aeruginosa was high, but molecular typing showed that there was no clonal outbreak. This high incidence was revealed by identification of simple colonization through testing screening samples. If diagnostic samples only had been used, the measured incidence would have been about half that reported. The water environment played only a minor role because only one of the 14 cases that could be evaluated was consistent with a colonization from the water sources tested (7.2% of cases).
Testing samples taken from water fittings in surgical and medical intensive care rooms in this study showed, nevertheless, that U-bends were frequently contaminated with P. aeruginosa, consistent with published findings [5, 6, 12, 13]. In half the cases, the water environment (U-bends and taps) of the room contained several clones of P. aeruginosa. This, together with the clonal diversity of the strains isolated from U-bends (differences between and within U-bends), provides evidence for colonization of the U-bend from the exterior rather than originating from the water supply. In addition, the presence of identical strains in the U-bends of sinks in both these physically independent units not shared by the same patients is suggestive of retro-colonization of the U-bend by the microflora present in wastewater pipes, via the biofilm, as previously proposed [14].
The role of the water environment in the P. aeruginosa colonization of patients was the key issue in this study. Many studies have attributed a major role to water fittings in the incidence of patient colonization with P. aeruginosa in ICUs [5, 12, 14]. Other studies have reported only a weak epidemiological link between environmental colonization and the occurrence of infections in patients [4, 15, 16]. All these previous studies were carried out during outbreaks. Some prospective studies have been published and they report frequencies of patient colonization by the environment of 14.2–50% [3, 6, 12–14, 17, 18]. In our study, in the absence of clonal epidemic, the frequency of colonization of patients via the water environment of their rooms seemed to be lower. Regardless of the epidemiological situation, which may differ between departments, measurement of the frequency with which this event arises requires three methodological conditions which have never before been fulfilled:
-
1.
The identification of all patients colonized by epidemiological sampling (screening) of patients. We found that the use of diagnostic samples alone would have identified only about half the colonized/infected patients.
-
2.
The collection of samples from water fittings should be generalized and carried out regularly to make it possible to determine when the patients became infected or colonized. This is rarely the case in surveys motivated by the suspicion of an epidemic.
-
3.
Strain comparisons should be based on a highly reproducible and discriminant typing method. The determination of the total DNA macrorestriction profile by PFGE can be considered to be the gold standard method for typing [10, 19].
The frequency of strains widely present in the environment (multiple clones) but never isolated from patients was high. Observations of this type led Valles et al. to suggest that there may be two different genetic groups in this species: one group of strains that are mostly environmental and not very pathogenic in humans; and one group of strains better adapted to humans with a much higher pathogenic potential [13]. This view is supported by virulence surveys, analyses of bacterial populations by multi-locus sequence typing, and the application of several typing methods to strains of two different origins (clinical and environmental) [4, 20, 21].
Conclusion
In conclusion, although water fittings clearly play a role in the acquisition of P. aeruginosa by patients hospitalized in ICUs, the contribution of this phenomenon in non-epidemic situations appears to be much smaller than generally believed by many operational hospital infection control teams.
References
Enquête nationale de prévalence des infections nosocomiales 2006. (2007) Résultats préliminaires au 12/01/2007. Institut de veille sanitaire (InVS). available at http://www.invs.sante.fr
Bertrand X, Thouverez M, Patry C, Balvay P, Talon D (2001) Pseudomonas aeruginosa: antibiotic susceptibility and genotypic characterization of strains isolated in the intensive care unit. Clin Microbiol Infect 7:706–708
Berthelot P, Grattard F, Mahul P, Pain P, Jospe R, Venet C, Carricajo A, Aubert G, Ros A, Dumont A, Lucht F, Zeni F, Auboyer C, Bertrand JC, Pozzetto B (2001) Prospective study of nosocomial colonization and infection due to Pseudomonas aeruginosa in mechanically ventilated patients. Intensive Care Med 27:503–512
Ruiz L, Dominguez MA, Ruiz N, Vinas M (2004) Relationship between clinical and environmental isolates of Pseudomonas aeruginosa in a hospital setting. Arch Med Res 35:251–257
Lasheras A, Guisset O, Boulestreau H, Rogues AM, Fiore M, Szajner S, Bezian MC, Gabinski C, Gachie JP (2006) Reservoirs and transmission of Pseudomonas aeruginosa in intensive care unit. Med Mal Infect 36:99–104
Blanc DS, Nahimana I, Petignat C, Wenger A, Bille J, Francioli P (2004) Faucets as a reservoir of endemic Pseudomonas aeruginosa colonization/infections in intensive care units. Intensive Care Med 30:1964–1968
Schelenz S, French G (2000) An outbreak of multidrug-resistant Pseudomonas aeruginosa infection associated with contamination of bronchoscopes and an endoscope washer-disinfector. J Hosp Infect 46:23–30
Cobben NA, Drent M, Jonkers M, Wouters EF, Vaneechoutte M, Stobberingh EE (1996) Outbreak of severe Pseudomonas aeruginosa respiratory infections due to contaminated nebulizers. J Hosp Infect 33:63–70
Bert F, Maubec E, Bruneau B, Berry P, Lambert-Zechovsky N (1998) Multi-resistant Pseudomonas aeruginosa outbreak associated with contaminated tap water in a neurosurgery intensive care unit. J Hosp Infect 39:53–62
Talon D, Cailleaux V, Thouverez M, Michel-Briand Y (1996) Discriminatory power and usefulness of pulsed-field gel electrophoresis in epidemiological studies of Pseudomonas aeruginosa. J Hosp Infect 32:135–145
Tenover FC, Arbeit RD, Goering RV, Mickelsen PA, Murray BE, Persing DH, Swaminathan B (1995) Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J Clin Microbiol 33:2233–2239
Trautmann M, Michalsky T, Wiedeck H, Radosavljevic V, Ruhnke M (2001) Tap water colonization with Pseudomonas aeruginosa in a surgical intensive care unit (ICU) and relation to Pseudomonas infections of ICU patients. Infect Control Hosp Epidemiol 22:49–52
Valles J, Mariscal D, Cortes P, Coll P, Villagra A, Diaz E, Artigas A, Rello J (2004) Patterns of colonization by Pseudomonas aeruginosa in intubated patients: a 3-year prospective study of 1,607 isolates using pulsed-field gel electrophoresis with implications for prevention of ventilator-associated pneumonia. Intensive Care Med 30:1768–1775
Trautmann M, Lepper PM, Haller M (2005) Ecology of Pseudomonas aeruginosa in the intensive care unit and the evolving role of water outlets as a reservoir of the organism. Am J Infect Control 33:S41–S49
Talon D, Mulin B, Rouget C, Bailly P, Thouverez M, Viel JF (1998) Risks and routes for ventilator-associated pneumonia with Pseudomonas aeruginosa. Am J Respir Crit Care Med 157:978–984
Bonten MJ, Bergmans DC, Speijer H, Stobberingh EE (1999) Characteristics of polyclonal endemicity of Pseudomonas aeruginosa colonization in intensive care units. Implications for infection control. Am J Respir Crit Care Med 160:1212–1219
Reuter S, Sigge A, Wiedeck H, Trautmann M (2002) Analysis of transmission pathways of Pseudomonas aeruginosa between patients and tap water outlets. Crit Care Med 30:2222–2228
Ferroni A, Nguyen L, Pron B, Quesne G, Brusset MC, Berche P (1998) Outbreak of nosocomial urinary tract infections due to Pseudomonas aeruginosa in a paediatric surgical unit associated with tap-water contamination. J Hosp Infect 39:301–307
Speijer H, Savelkoul PH, Bonten MJ, Stobberingh EE, Tjhie JH (1999) Application of different genotyping methods for Pseudomonas aeruginosa in a setting of endemicity in an intensive care unit. J Clin Microbiol 37:3654–3661
Fenner L, Richet H, Raoult D, Papazian L, Martin C, La Scola B (2006) Are clinical isolates of Pseudomonas aeruginosa more virulent than hospital environmental isolates in amebal co-culture test? Crit Care Med 34:823–828
Vernez I, Hauser P, Bernasconi MV, Blanc DS (2005) Population genetic analysis of Pseudomonas aeruginosa using multilocus sequence typing. FEMS Immunol Med Microbiol 43:29–35
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Cholley, P., Thouverez, M., Floret, N. et al. The role of water fittings in intensive care rooms as reservoirs for the colonization of patients with Pseudomonas aeruginosa . Intensive Care Med 34, 1428–1433 (2008). https://doi.org/10.1007/s00134-008-1110-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-008-1110-z