
Abstract
Purpose
This register-based study examined the trajectories of depression or anxiety disorder-related work disability during and following long-term psychotherapy and identified sociodemographic factors that indicate membership in different trajectory groups.
Methods
Data were drawn from national registers (Statistics Finland, Social Insurance Institution of Finland). Participants included a random sample of Finnish working-age individuals (18–55 years) who started psychotherapy treatment between 2011 and 2014 and were followed for 5 years: 1 year before and 4 years after the onset of psychotherapy (N = 3 605 individuals; 18 025 person-observations across five time points). Group-based trajectory modeling was applied to assign individuals to work disability trajectories by the number of annual mental health-related work disability months. Multinomial logistic regression was used to examine the associations between trajectory group membership and baseline sociodemographic factors of age, gender, occupational status, and geographical area of residence.
Results
Four mental health-related work disability trajectories were identified: stable very low (72%), decrease (11%), persistent low (9%) and persistent high (7%). Those with older age, female gender, lower occupational status, and living in sparsely populated geographical areas were more likely to belong to the most unfavorable trajectory group of persistent high work disability. The presence of multiple risk characteristics substantially increased the probability of belonging to the most adverse trajectory group.
Conclusions
Sociodemographic factors were associated with the course of mental health-related work disability in association with psychotherapy. Rehabilitative psychotherapy does not function as an equal support resource for work ability in all parts of the population.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Depression and anxiety disorders are among the leading causes of work disability globally [1,2,3]. These disorders have a significant impact on the ability to study or work, the number of sick leaves, direct and indirect health expenditures, work productivity, and societal burden [4,5,6,7,8]. Occupational classes have been shown to differ in the risk of depression and anxiety-related work disability [4, 9, 10] and such differences in the risk increase over the life course [11, 12].
Psychotherapeutic treatments are widely acknowledged as effective for depression and anxiety disorders symptom reduction [13]. The treatments remove obstacles to workability and reduce mental health-related sickness absences and work disability [14, 15]. However, these person-centered treatments may not be equally efficient in improving functioning between occupations with varying work-related risk factors. Adverse work characteristics have been associated with common mental health disorders: psychosocial stressors such as imbalanced job design (i.e., low job control and high demands), occupational uncertainty and perceived lack of value and respect in the workplace (i.e., effort-reward imbalance) are linked with higher mental distress [16, 17] and the risk for work disability due to poor work characteristics have proved to be pronounced among low occupational status individuals [18, 19]. Thus, as individuals with lower occupational status are at greater risk of being exposed to such adverse work characteristics [20] psychotherapeutic treatments might not be as effective for them in comparison to individuals with higher occupational status. However, to date, information is scarce on occupational status’ role in response to psychotherapy treatment when aiming to improve and maintain the workability of those at high risk of work disability because of mental disorders.
Furthermore, previous research has shown significant regional variation in mental health-related work disability [21]. Studies have observed differences in mental health care practices between urban and rural areas suggesting more detrimental effects for those living outside urban areas: together with different clinical practices [21, 22] it might be that in a country like Finland, long regional distances might lead to suboptimal treatment use. Furthermore, the influence of mental distress on work disability might be more pronounced in more disadvantaged areas with fewer occupational opportunities. Thus, previous studies suggest an existing association between a geographical area of residence and mental health outcomes but whether outcomes differ among those who receive psychotherapy treatment remains unknown.
Studies on the effectiveness of psychotherapeutic treatments have mainly focused on examining changes in outcomes of the mean level of change [23,24,25]. Such methodological approaches may, however, overlook subgroups of clients who are unable to benefit from psychotherapy or whose pattern of change during the treatment differs from the mean [23, 24]. Previous studies have shown that clinical characteristics such as baseline symptom severity and psychological functioning influence clients’ trajectories of change so that some improve at the initial phases of the treatment whereas others progress more gradually or even show a decrease in functioning during the treatment [24, 26, 27]. The advantages and resources related to occupational status or geographical area might influence this variation between treatment trajectories. However, while the interest in trajectories of change has increased, there is a lack of information on such contextual factors intervening change process.
Person-centered approaches have been designed to address this variability across clients’ responses to the treatment and to reveal patterns of change in a longitudinal setting [28, 29]. To assess whether occupational status or geographical area influences clients’ ability to benefit from the treatment, such an analytic approach could be used to determine a continuous change process over time among groups with different statuses. Improving understanding of how psychotherapy works among different groups of clients may help to improve the practices when aiming to intervene in socioeconomic inequalities in mental health-related work disability.
In Finland, rehabilitative psychotherapy is the major single form of publicly provided rehabilitation. It is targeted at those at risk for disability to work or study because of mental disorders [30]. It is granted for a yearly period (maximum 3 years), a maximum of 80 sessions per year and 200 sessions per 3 years and could be cognitive, cognitive behavioral, cognitive analytic, psychodynamic, integrative, solution-focused or family therapy. From 2011 on it has been statutorily granted for all at risk. Despite the statutory status, a patient needs a psychiatrist’s referral to psychotherapy. The referral must be preceded by a minimum of three-month follow-up to assess whether first-line treatments (mainly pharmacological or in some cases short psychological counseling) are efficient for improving functioning and workability. After the referral, a patient needs to find an available psychotherapist from the private healthcare sector. Results from two recent studies suggest that rehabilitation was associated with somewhat better labor market outcomes [31, 32]. However, there is no information on whether occupational status or area of residence influence work disability progress during and after rehabilitation and to what extent disability trajectories have differed among individuals who started rehabilitative psychotherapy after it became accessible to all eligible for the benefit. Our study extends research on this issue by identifying work disability trajectories over 1 year before and 4 years after the onset of rehabilitative psychotherapy using nationally representative data. Further, to assess whether there are social position-related inequalities in achieving improvement during therapy examined the associations of occupational status and area of residence with differences in work disability trajectories.
Aims of the study and research questions
Our aim was to (i) ascertain psychotherapy clients’ typical depression or anxiety-related work disability trajectories and (ii) examine whether sociodemographic factors (age, gender, occupational status, and geographical area of residence) are associated with work disability trajectory group membership. Our research questions were: “What kind of work disability trajectories can be recognized among a cohort of rehabilitative psychotherapy users?” and “Do sociodemographic factors predict the users’ trajectory group membership?”.
Hypothesis
Based on earlier studies [18,19,20,21,22], we hypothesized that low occupational status and living in sparsely populated areas together with older age are associated with poor and prolonged work disability outcomes during and following the treatment.
Methods
Sample
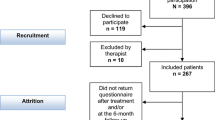
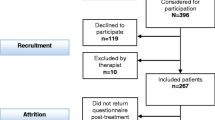
We used data from the Rise of Mental Vulnerability project [32, 33], in which cohorts of 33% random samples of the working-age population in the census of 2010, N = 772 663 were drawn from the Statistics Finland population database. We selected 18–55-year-old individuals who began rehabilitative psychotherapy between 2011 and 2014 (N = 10,497). We excluded those who had had discretionary rehabilitative psychotherapy before the legislation change in 2011 but whose rehabilitation was still ongoing (n = 2240), those not in paid employment (students, unemployed, self-employed persons) during the study period (from the year before the onset of psychotherapy until a three-year follow-up, N = 4641) as well those who were on permanent disability pension before the onset of psychotherapy (N = 11), resulting in a sample size of 3605 individuals.
Measures
Work disability
The primary outcome was work disability due to depression and anxiety disorders (ICD-10 codes F32-33 and F40-F43), measured at five time points relative to psychotherapy onset: the year preceding onset (baseline), the year of onset, and one through 3 years following the onset of psychotherapy. For each individual, the annual number of disability months (0–12) was calculated based on their totaled annual compensated sickness absence (SA) and disability pension (DP) days in these diagnostic categories. First, the annual number of compensated SA days due to depression or anxiety disorders was extracted from the registers of the Social Insurance Institution. Shorter SA periods (lasting less than ten working days) are not compensated by the Social Insurance Institution and therefore data on shorter absences were not available for this study. Second, the annual number of compensated DP days due to depression or anxiety disorders was extracted from the registers of the Finnish Centre for Pensions. Part-time DP days were converted into whole days so that two part-time DP days counted as one whole day. The total number of work disability days was converted into months: no work disability months for ≤ 7 annual work disability days; 1 month for 8–29 days; 2 months for 30–59 days and so forth (see [9]).
Rehabilitative psychotherapy
The onset of psychotherapy treatment was determined as the year (between 2011 and 2014) when the individual first received reimbursement for psychotherapy from the Social Insurance Institution of Finland. The duration of psychotherapy was calculated by using the information on reimbursements for psychotherapy during the years following psychotherapy onset. Because very few participants (3%) had a psychotherapy duration of more than four calendar years, the variable was top-coded at 4 years.
Sociodemographic characteristics
Data on sociodemographic characteristics were obtained from the year preceding the onset of psychotherapy (baseline) from the Statistics of Finland register. These included age, gender, occupational status, and geographical area of residence. Occupational status was coded according to the socioeconomic group into upper-level and lower-level employees and manual workers. Regarding the geographical area of residence, the Finnish health care system is divided into five regional specialized university hospital districts with 700 000–2 200 000 inhabitants. Geographical area was classified according to the university hospital districts, located in southern (Helsinki University Hospital), central (Tampere University Hospital), western (Turku University Hospital), eastern (Kuopio University Hospital) and northern (Oulu University Hospital) Finland.
Statistical analysis
We conducted group-based trajectory analysis using the STATA plugin TRAJ [34] to identify subgroups of individuals who follow similar courses of work disability due to mental disorders before, during and after rehabilitative psychotherapy. For the analysis, time was normalized so that time t0 corresponds to the onset of psychotherapy. The trajectories of the annual number of work disability months from t-1 (baseline) to t3 were modeled with a zero-inflated Poisson distribution. In the zero-inflated Poisson model with the TRAJ plugin, both an “order” and an “iorder” option can be specified. Whereas the order option refers to trajectory shapes, the iorder option refers to the degree to which zero-inflation in the trajectory groups varies over time (i.e., the pattern of excessive zeros). We initially fitted models with an intercept and a linear and quadratic term for two to five trajectory solutions. A combination of several criteria was used to determine the optimal number of groups: the Bayesian Information Criterion (BIC), trajectory group size (minimum group size of 5%), and whether the model captured new distinctive features of the data (i.e., whether increasing the group size resulted in new distinct trajectories) [35]. We chose parsimony over complexity in model selection to avoid performing a high number of group comparisons at the next stage of the analysis, where the associations between client characteristics and trajectory group membership were examined. Once the optimal number of groups was established, the shape of the trajectory for each group was refined to its final form by testing higher-order (cubic) terms for the trajectories and higher-order terms for the zero-inflation and removing the highest-order terms that were nonsignificant. After this, individuals were assigned to a trajectory group to which they most likely belonged based on estimates of their posterior probability of group membership. Although it would have been possible to estimate the probability of latent trajectory group membership and the effects of client characteristics on the group membership probability in a joint model, we chose to estimate the trajectory groups in their “pure” form. This two-step approach, where the associations between risk factors and trajectory group membership are examined after the groups are identified, is widely used in the literature. We performed an analysis of variance for continuous variables and χ2 tests for categorical variables to investigate whether the trajectory subgroups differed in their sociodemographic characteristics. Multinomial logistic regression was performed to estimate the multivariate associations between client characteristics and membership in various disability trajectories. Age, gender, occupational status, and geographical area of residence were entered as predictors of trajectory group membership. The regression models were adjusted for the duration of psychotherapy and the calendar year of the onset of psychotherapy. The resulting estimates were obtained using the most favorable trajectory as a reference category and expressed as relative risk ratios (RRR, sometimes called a multinomial odds ratio) and 95% confidence intervals (CIs). The interpretation of the RRR is that for a unit change in the predictor variable, the odds of the outcome relative to the reference group are expected to change by its respective RRR estimate, holding all other variables in the model constant. The analyses were conducted on STATA 17 and visualizations were produced using R 4.0.5 with ggplot2 [36].
Results
A total of 3605 participants were included (79% female, mean age 37 years), contributing 18,025 person-year-observations across five time points from t−1 to t3. Of the participants, 24.9% had started psychotherapy in 2011 (n = 896); 24.2% in 2012 (n = 872); 24.9% in 2013 (n = 899); and 26.0% in 2014 (N = 938). The mean duration of psychotherapy was 3.23 years.
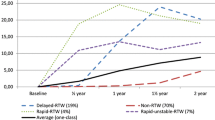
Table 1 presents model statistics for the tested trajectory models (see Supplementary material for a more detailed description of the model selection and refinement process). We identified four distinct trajectory groups of mental health-related work. The first, most favorable trajectory group, “stable very low” (n = 2 604, 72.2% of participants), had a very low work disability trajectory across the follow-up. The second trajectory group, “persistent low” (n = 405, 11.2% of participants), had a low but constant work disability trajectory across the follow-up. The third group, “decrease” (n = 328, 9.1%), showed a persistent decline from a higher baseline level of work disability to a lower level of work disability starting in the second year of psychotherapy. The fourth group, “persistent high” (n = 268, 7.4%), had the highest level of work disability at the onset of psychotherapy. In this unfavorable work disability trajectory group, work disability increased at the onset of therapy and remained significantly higher than in other groups during the follow-up. See Fig. 1 for a visual representation of the trajectories and Table 2 for the characteristics of participants by trajectory groups. The groups differed on all sociodemographic factors except occupational status.

Depression or anxiety-related work disability trajectories were identified using group-based trajectory modeling. The solid lines are based on the parameter estimates of the model (with a 95% confidence interval as shaded area), whereas the dots are calculated with the actual data where the responses are weighted based on posterior probabilities of group membership. The dashed vertical line indicates the onset year of psychotherapy
Overall, with regards to our hypothesis, the results of multinomial logistic regression (Fig. 2) showed that low occupational status and living in sparsely populated areas and older age are associated with poor work disability outcomes. In addition to our hypothesis, female gender was associated with poor work disability outcomes: relative to the stable very low group, higher age, female gender, manual or lower-level occupational status, and Central area of residence were associated with membership in the persistent low trajectory group. Furthermore, as for the comparison between stable very low and the persistent high trajectory group, higher age, female gender, manual or lower-level occupational status, and residence outside the Southern area, especially in the Northern or Eastern area of residence were associated with an increased risk of membership in the persistent high group. As for the comparison between stable very low and persistent low, again higher age, lower lever occupational status, and residence outside the Southern area, especially in the Eastern area or Central geographical area of residence were associated with an increased risk of membership in the persistent high group. Based on non-overlapping confidence intervals, particularly older age differentiated the persistent high from the decrease or stable very low groups and Easter and Northern area of residence from the decrease group (see Fig. 2). There were also differences in the duration of psychotherapy between the groups. Compared with the stable very low trajectory group, the treatment duration was shorter in the decrease (RRR = 0.86, 95% CI 0.76–0.97) and longer in the persistent high (RRR = 1.29, 95% CI 1.11–1.51) trajectory groups.

The associations between psychotherapy client background characteristics and membership in “Persistent decrease”, “Persistent low” and “Persistent high” work disability trajectories with membership in “Stable very low” as the reference category. Dots indicate relative risk ratios (i.e., multinomial odds ratios) and the bars indicate 95% confidence intervals
To measure the combined effects of sociodemographic characteristics on trajectory group membership, we calculated marginal probabilities of assignment to the most unfavorable, persistent high group from the results of the regression analysis. More specifically, we estimated the probability of assignment to the persistent high work disability trajectory group among males and females by age (30 or 50 years), occupational status (upper-level employees or manual workers), and geographical area. The presence of multiple risk factors substantially increased the probability of assignment to the persistent high trajectory group (see Fig. 3). For example, for a 50-year-old female manual worker living in Northern Finland, the probability of being assigned to the persistent high group was 25.8% (95% CI 15.2–36.5), whereas, for a 30-year-old upper-level male employee living in Southern Finland, the probability was 1.4% (95% CI 0.9–2.1). The full details of all possible combinations are shown in Supplementary Table 1.

Estimated marginal probabilities from the multinomial regression model showing the combined effects of sociodemographic characteristics on persistent high-trajectory group membership
Discussion
We investigated sociodemographic and regional factors that were associated with depression or anxiety disorder-related work disability trajectories in a nationally representative sample of working-age Finnish receiving psychotherapy. Four different trajectories were found: most of the cohort (72%) showed stable very low work disability during the follow-up and one-tenth of the cohort (11%) showed a decrease in work disability. Of the sample, 7% showed persistent high and 9% showed persistent low work disability over a year before and 4 years after the onset of psychotherapy. Older age, female gender, lower occupational status and living in more sparsely populated areas such as the Eastern area of Finland were associated with higher and persistent work disability. Individuals with a persistent high and persistent low work disability received rehabilitative psychotherapy slightly longer than individuals in other groups.
In this register study, those whose work disability remained very low can be considered a favorable group suggesting that therapy maintains these clients’ ability to work as intended in the legislation of public rehabilitation services. The results are in line with previous studies suggesting that younger age, higher occupational status and shorter length of preceding disability were associated with better outcomes in psychotherapy [37, 38] and vocational rehabilitation [39] and with earlier return to work after mental disorder -related sick leave [40, 41]. Similarly, those whose work disability decreased during the therapy, labeled as the decrease group, can also be considered as a favorable group as workability outcomes improved in association with rehabilitative psychotherapy. On the contrary, in two other groups, work disability remained poor or very poor in association with psychotherapy. Female gender and living in sparsely populated areas of Finland stand out as risk factors for prolonged work disability. Notably, work disability in the least favorable persistent high group was higher at the onset of therapy than in the other groups and multiple risk factors were associated with the increased risk of persistent high work disability.
According to our hypothesis, low occupational status was associated with persistent work disability, the results point out work-related contextual differences in the ability to benefit from person-centered rehabilitative psychotherapy. There is cumulative evidence that the burden of adverse work characteristics on work disability and early exit from working life is pronounced among low occupational status individuals [18, 19, 40, 42, 43]. Thus, as the impact of working life structures on work disability has shown to differ among occupational classes, persistent work disability trajectories seen in our study may reflect occupation-related possibilities for rehabilitation rather than individuals’ workability per se. i.e., possibilities for job accommodations that support working despite the mental health condition may be better in upper occupational positions. The association between occupational status and work disability may be also enhanced by gendered occupational statuses: it has been shown that among women low occupational status is associated with increased mental ill health [44]. Thus, the influence of adverse work-related risk factors on ability to benefit from psychotherapy may be more pronounced among women as our results suggest. Furthermore, there is some evidence that a combination of various practical, psychological, and cultural barriers influences treatment engagement and gaining from psychotherapy among employees with lower occupational status [45, 46]. In our study, those with persistent high work disability had a slightly longer treatment duration when compared with the stable very low group. This might reflect the practical challenges in attending regular treatment sessions among manual workers and thus lengthening the treatment. Furthermore, in their recent study, Williams et al. also showed that those in routine or manual work found their work less meaningful than those in higher occupational classes [47]. Thus, these characteristics related to labor market structures, possibilities to engage in rehabilitation and factors influencing working-life attachment may jointly increase the risk of prolonged disability due to mental health reasons among employees with lower status. Thus, the stagnation in trajectories of these groups suggests that individual-based rehabilitation is not sufficient to support workability in cases with persistent disability. Reducing prolonged disability due to mental disorders might require broader interventions that combine individual-based rehabilitation and occupational adjustments.
Although two recent studies have suggested that rehabilitative psychotherapy associates with better labor market outcomes [31, 32], there has been only scarce information on factors influencing individuals’ outcomes in association with long-term psychotherapy comparable to our study. Results from Helsinki Psychotherapy Study suggest that similarly to our study, most clients’ work disabilities remain stable or improved during long-term psychotherapy [15]. In a 10-year follow-up, workability among clients receiving long-term psychotherapy improved significantly more than in groups with shorter (12–20 sessions during 5–8 months) psychotherapy [15]. However, after 10 years of follow-up, only about 60% were in remission and 33% of them used some auxiliary psychiatric treatment during the follow-up. These results made the authors suggest, that the treatment given during that long period was not particularly effective in providing long-term benefits for individuals with relatively long-standing work disability related to depression or anxiety disorders [15]. Similar conclusions can be drawn from our results where high baseline disability was associated with poor outcomes during follow-up.
Thus, a persistent high work disability should be considered in a broader context of health and correlates that modify health outcomes. Mental disorders have been associated with physical comorbidity [48, 49] and the number of comorbidities was associated with work disability in terms of low work productivity, frequent sick leaves and a lower rate of return to work after sick leave [40, 50]. These findings were especially prominent in older age groups and related to low socioeconomic status [12, 40, 51,52,53]. Furthermore, the incidence rates of depressive and anxiety disorders have shown to be approximately two-fold among women in comparison to men [54, 55], in line with the overall greater burden of ill health and functional problems among women [56]. As previously outlined, together with the severity of the condition, psychosocial work characteristics have been indicated to predict sick leave outcomes [19]. Thus, the relevance of the treatment for those with persistent high work disability should be evaluated more carefully as poor baseline functioning, comorbidities and workplace attitudes towards disorder might hinder an individual’s possibilities to benefit from mere psychotherapy [23, 24, 57] and correlates of occupational position might influence this association.
As a novel finding, our study shows that also the work disability associated with psychotherapeutic treatment differs between geographical areas. It might be that the lower regional availability of psychotherapy in sparsely populated Northern and Eastern areas of Finland [58] might hinder receiving psychotherapy timely in these areas. Furthermore, when considering the regional differences in the impact of common mental disorders on losses of workability, quality of life, increased health expenditures and mortality, Northern and Eastern areas show the largest burden of health [59]. This might reflect larger regional differences in mental health services that might result in too-late rehabilitation for individuals in persistent high disability groups. Such assumptions are supported by a recent study by Karolaakso et al. who found corresponding evidence on regional differences in risk of disability pension related to mood disorders. Although one could suggest that the influence of work-related risk factors on work disability is more pronounced in more disadvantaged areas with fewer occupational opportunities, their results were not fully explained by socioeconomic factors [21]. Thus, together these results seem to illustrate the divergent functioning of mental health care services across different geographical areas.
This study has several strengths. It is based on reliable register-based national data combined from multiple sources and with a considerably long follow-up period. We combined information on individuals’ work disability months based on medical diagnoses, information on psychotherapy use and information on sociodemographic factors recorded independently from each other. A population-based cohort of all psychotherapy users during the research period gave us satisfactory power for the analyses and allowed us to assess the latent sub-groups with similar work disability trajectories over time [60] in a representative sample of Finnish employees. Further studies should widen the scope of the target group also to students or self-employed persons to assess diversity in response to treatment in such groups of psychotherapy clients.
Our study also has limitations. Given the descriptive nature of this study without comparison groups (those who did not receive any treatment or received some other type of treatment), the trajectories found in this study may not fully reflect the response to the treatment but also, as was discussed above, result from regional differences in the labor market structures and the organization of health care. Although the Social Insurance Institution register covers most sickness absence days due to mental disorders in Finland, our work disability outcome was somewhat crude as information on shorter than ten-day sick leaves was not available. Also, rehabilitative psychotherapy is targeted at those who already are disabled to work but also at those at risk for work disability. Thus, the results may not reflect the whole spectrum of work disability or the association between the treatment and work disability risk factors. Furthermore, the follow-up related to the treatment was relatively short and we were unable to assess the stability of the results. We looked only at the association between psychotherapy use and work disability trajectories and thus we cannot make further assumptions about the effectiveness of various types of treatment on work disability. Although we were unable to assess the influence of more detailed characteristics of the treatment and individuals on the outcome, differencing work disability trajectories raise the question of whether the type of treatment or treatment intensity reflected the patients’ needs. Also, approximately 90% of the rehabilitation psychotherapies have been shown to be related to depressive and anxiety disorders [61] suggesting a high correlation between reasons for work disability and psychotherapy. However, we cannot rule out that some individuals included in our study may have received psychotherapy for some other reason (for example due to eating disorders). Further studies are thus needed to assess the coverage and needs of various target groups and the choice of psychotherapy. In addition, suitability to the treatment should be considered based on personalized needs including both personal [62, 63] and contextual factors such as work-related characteristics to understand their interaction on workability outcomes.
Conclusions
This population-level register-based study shows that several sociodemographic characteristics are associated with subsequent work disability trajectories among individuals who attend long-term psychotherapy. Older age, female gender, lower occupational status, and living in sparsely populated geographical areas of Finland were associated with cumulatively greater risk for persistent high work disability. These findings indicate that despite the equal admission criteria for the treatment there are inequalities in achieving improvement in workability in association with long-term rehabilitative psychotherapy. Further studies should focus on these factors reflecting societal barriers to recovery of workability in conjunction with morbidity and work-related characteristics.
Data availability
Data in this study were used under its’ license approved by Statistics Finland, Social Security Institution of Finland, Finnish Centre for Pensions. They are not publicly available. Currently, the Finnish Social and Health Data Permit Authority (Findata) coordinates the permissions for similar datasets, and they are available to researchers under permission (https://findata.fi/en/). The THL’S morbidity indexes are publicly available from the Sotkanet Indicator Bank, an information portal provided by THL (https://sotkanet.fi/sotkanet/en/haku?g=284). Provenance and peer review: not commissioned; externally peer-reviewed.
References
Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M et al (2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396(10258):1204–1222
Baxter AJ, Scott KM, Vos T, Whiteford HA (2013) Global prevalence of anxiety disorders: a systematic review and meta-regression. Psychol Med 43(5):897–910
Finnish Centre for Pensions (2019) Statistical yearbook of pensioners in Finland 2018. Helsinki
Karolaakso T, Autio R, Näppilä T, Nurmela K, Pirkola S (2020) Socioeconomic factors in disability retirement due to mental disorders in Finland. Eur J Pub Health 30(6):1218–1224
König H, König H-H, Konnopka A (2020) The excess costs of depression: a systematic review and meta-analysis. Epidemiol Psychiatr Sci 29:e30. https://doi.org/10.1017/S2045796019000180
Mrazek DA, Hornberger JC, Altar CA, Degtiar I (2014) A review of the clinical, economic, and societal burden of treatment-resistant depression: 1996–2013. Psychiatr Serv 65(8):977–987
Konnopka A, König H (2020) Economic burden of anxiety disorders: a systematic review and meta-analysis. Pharmacoeconomics 38(1):25–37
Hakulinen C, Elovainio M, Arffman M, Lumme S, Pirkola S, Keskimäki I et al (2019) Mental disorders and long-term labour market outcomes: Nationwide Cohort Study of 2,055,720 individuals. Acta Psychiatr Scand 140(4):371–381
Hiilamo A, Shiri R, Kouvonen A, Mänty M, Butterworth P, Pietiläinen O et al (2019) Common mental disorders and trajectories of work disability among midlife public sector employees–A 10-year follow-up study. J Affect Disord 247:66–72
Ervasti J, Vahtera J, Pentti J, Oksanen T, Ahola K, Kivimäki M et al (2013) Depression-related work disability: socioeconomic inequalities in onset, duration and recurrence. PLoS One 8(11):e79855
Lorant V, Deliège D, Eaton W, Robert A, Philippot P, Ansseau M (2003) Socioeconomic inequalities in depression: a meta-analysis. Am J Epidemiol 157(2):98–112
Green MJ, Benzeval M (2013) The development of socioeconomic inequalities in anxiety and depression symptoms over the lifecourse. Soc Psychiatry Psychiatr Epidemiol 48(12):1951–1961
Cuijpers P (2019) Targets and outcomes of psychotherapies for mental disorders: an overview. World Psychiatry 18(3):276–285
Nieuwenhuijsen K, Verbeek JH, Neumeyer-Gromen A, Verhoeven AC, Bültmann U, Faber B (2020) Interventions to improve return to work in depressed people. Cochrane Database Syst Rev (10):CD006237. https://doi.org/10.1002/14651858.CD006237.pub4
Knekt P, Virtala E, Härkänen T, Vaarama M, Lehtonen J, Lindfors O (2016) The outcome of short-and long-term psychotherapy 10 years after start of treatment. Psychol Med 46(6):1175–1188
Harvey SB, Modini M, Joyce S, Milligan-Saville JS, Tan L, Mykletun A et al (2017) Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup Environ Med 74(4):301–310
Theorell T, Hammarström A, Aronsson G, TräskmanBendz L, Grape T, Hogstedt C et al (2015) A systematic review including meta-analysis of work environment and depressive symptoms. BMC Public Health 15(1):738
Hoven H, Siegrist J (2013) Work characteristics, socioeconomic position and health: a systematic review of mediation and moderation effects in prospective studies. Occup Environ Med 70(9):663–669
Knardahl S, Johannessen HA, Sterud T, Härmä M, Rugulies R, Seitsamo J et al (2017) The contribution from psychological, social, and organizational work factors to risk of disability retirement: a systematic review with meta-analyses. BMC Public Health 17(1):1–31
Landsbergis PA, Grzywacz JG, LaMontagne AD (2014) Work organization, job insecurity, and occupational health disparities. Am J Ind Med 57(5):495–515
Karolaakso T, Autio R, Näppilä T, Leppänen H, Rissanen P, Tuomisto MT et al (2021) Contextual and mental health service factors in mental disorder-based disability pensioning in Finland—a regional comparison. BMC Health Serv Res 21(1):1081
Halonen JI, Koskinen A, Kouvonen A, Varje P, Pirkola S, Väänänen A (2018) Distinctive use of newer and older antidepressants in major geographical areas: a nationally representative register-based study. J Affect Disord 229:358–363
Lin T, Farber BA (2021) Trajectories of depression in psychotherapy: how client characteristics predict clinical improvement. J Clin Psychol 77(6):1354–1370
Cuijpers P, van Lier PA, van Straten A, Donker M (2005) Examining differential effects of psychological treatment of depressive disorder: an application of trajectory analyses. J Affect Disord 89(1–3):137–146
Laurenceau J-P, Hayes AM, Feldman GC (2007) Some methodological and statistical issues in the study of change processes in psychotherapy. Clin Psychol Rev 27(6):682–695
Owen J, Adelson J, Budge S, Wampold B, Kopta M, Minami T et al (2015) Trajectories of change in psychotherapy. J Clin Psychol 71(9):817–827
Koffmann A (2020) Early trajectory features and the course of psychotherapy. Psychother Res 30(1):1–12
Laursen B, Hoff E (2006) Person-centered and variable-centered approaches to longitudinal data. Merrill Palmer Q 1982-:377–389
Muthén B, Muthén LK (2000) Integrating person-centered and variable-centered analyses: growth mixture modeling with latent trajectory classes. Alcoholism 24(6):882–891
The Social Insurance Institution of Finland (Kela). Rehabilitative psychotherapy. https://www.kela.fi/rehabilitative-psychotherapy. Accessed 30 June 2023
Peutere L, Ravaska T, Bӧckerman P, Virtanen P (2022) Effects of rehabilitative psychotherapy on labour market success: evaluation of a nationwide programme. Scand J Public Health. https://doi.org/10.1177/14034948221074974
Kausto J, Gluschkoff K, Turunen J, Selinheimo S, Peutere L, Väänänen A (2022) Psychotherapy and change in mental health-related work disability: a prospective Finnish population-level register-based study with a quasi-experimental design. J Epidemiol Community Health 76(11):925–930
Olakivi A, Kouvonen A, Koskinen A, Kemppainen L, Kokkinen L, Väänänen A (2023) Sickness absence in migrant and non-migrant care workers in Finland: a register-based follow-up study. Scand J Public Health. https://doi.org/10.1177/14034948231168434
Jones BL, Nagin DS (2013) A note on a stata plugin for estimating group-based trajectory models. Sociol Methods Res 42(4):608–613
Nagin DS (2005) Group-based modeling of development. Harvard University Press. https://doi.org/10.4159/9780674041318
Wickham H (2016) ggplot2: elegant graphics for data analysis. Springer Verlag New York. Retrieved from https://ggplot2.tidyverse.org.
Cuijpers P, Karyotaki E, Eckshtain D, Ng MY, Corteselli KA, Noma H et al (2020) Psychotherapy for depression across different age groups: a systematic review and meta-analysis. JAMA Psychiat 77(7):694–702
Joutsenniemi K, Laaksonen M, Knekt P, Haaramo P, Lindfors O (2012) Prediction of the outcome of short-and long-term psychotherapy based on socio-demographic factors. J Affect Disord 141(2–3):331–342
Leinonen T, Solovieva S, Husgafvel-Pursiainen K, Laaksonen M, Viikari-Juntura E (2019) Do individual and work-related factors differentiate work participation trajectories before and after vocational rehabilitation? PLoS One 14(2):e0212498
Ervasti J, Joensuu M, Pentti J, Oksanen T, Ahola K, Vahtera J et al (2017) Prognostic factors for return to work after depression-related work disability: a systematic review and meta-analysis. J Psychiatr Res 95:28–36
de Vries H, Fishta A, Weikert B, Rodriguez Sanchez A, Wegewitz U (2018) Determinants of sickness absence and return to work among employees with common mental disorders: a scoping review. J Occup Rehabil 28(3):393–417
Carr E, Fleischmann M, Goldberg M, Kuh D, Murray ET, Stafford M et al (2018) Occupational and educational inequalities in exit from employment at older ages: evidence from seven prospective cohorts. Occup Environ Med 75(5):369–377
Ebbinghaus B, Radl J (2015) Pushed out prematurely? Comparing objectively forced exits and subjective assessments of involuntary retirement across Europe. Res Soc Stratif Mobil 41:115–130
Halonen JI, Koskinen A, Varje P, Kouvonen A, Hakanen JJ, Väänänen A (2018) Mental health by gender-specific occupational groups: profiles, risks and dominance of predictors. J Affect Disord 238:311–316
Krupnick JL, Melnikoff SE (2012) Psychotherapy with low-income patients: lessons learned from treatment studies. J Contemp Psychother 42(1):7–15
Levy LB, O’Hara MW (2010) Psychotherapeutic interventions for depressed, low-income women: a review of the literature. Clin Psychol Rev 30(8):934–950
Williams M, Gifford J, Zhou Y (2022) Social stratification in meaningful work: occupational class disparities in the United Kingdom. Br J Soc 73(3):536–553
Härter M, Baumeister H, Reuter K, Jacobi F, Höfler M, Bengel J et al (2007) Increased 12-month prevalence rates of mental disorders in patients with chronic somatic diseases. Psychother Psychosom 76(6):354–360
Verhaak PF, Heijmans MJ, Peters L, Rijken M (2005) Chronic disease and mental disorder. Soc Sci Med 60(4):789–797
Cabral GG, de Souza ACD, Barbosa IR, Jerez-Roig J, Souza DL (2019) Multimorbidity and its impact on workers: a review of longitudinal studies. Saf Health Work 10(4):393–399
Ahola K, Virtanen M, Honkonen T, Isometsä E, Aromaa A, Lönnqvist J (2011) Common mental disorders and subsequent work disability: a population-based Health 2000 Study. J Affect Disord 134(1–3):365–372
Jacobi F, Wittchen H-U, Hölting C, Höfler M, Pfister H, Müller N et al (2004) Prevalence, co-morbidity and correlates of mental disorders in the general population: results from the German Health Interview and Examination Survey (GHS). Psychol Med 34(4):597–611
Cornelius LR, van der Klink JJL, Groothoff JW, Brouwer S (2011) Prognostic factors of long term disability due to mental disorders: a systematic review. J Occup Rehabil 21(2):259–274
Van de Velde S, Bracke P, Levecque K (2010) Gender differences in depression in 23 European countries. Cross-national variation in the gender gap in depression. Soc Sci Med 71(2):305–313
McLean CP, Asnaani A, Litz BT, Hofmann SG (2011) Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res 45(8):1027–1035
Crimmins EM, Kim JK, Solé-Auró A (2011) Gender differences in health: results from SHARE, ELSA and HRS. Eur J Pub Health 21(1):81–91
Volz H-P, Bartečků E, Bartova L, Bessa J, De Berardis D, Dragasek J et al (2022) Sick leave duration as a potential marker of functionality and disease severity in depression. Int J Psychiatry Clin Pract 26:1–11
Patana P 2014 Mental Health Analysis Profiles (MhAPs): Finland.
The Finnish Institute for Health and Welfare. Morbidity index 2011–2016. Helsinki 2021. https://sotkanet.fi/sotkanet/en/index. Accessed 19 Oct 2021
Nagin DS (2010) Group-based trajectory modeling: an overview. In: Piquero AR, Weisburd D (eds) Handbook of Quantitative Criminology. Springer, New York, NY, pp. 53–67
Tuulio-Henriksson A, Toikka T, Heino P, Laukkala T (2019) Kuntoutuspsykoterapia tukee työssä pysymistä (in English: Employment after psychotherapy). Finnish Med J 74(13):816–824
Jobst A, Brakemeier E-L, Buchheim A, Caspar F, Cuijpers P, Ebmeier KP et al (2016) European psychiatric association guidance on psychotherapy in chronic depression across Europe. Eur Psychiatry 33(1):18–36
Alanne C, Heinonen E, Knekt P, Rissanen J, Virtala E, Lindfors O (2021) Predicting improvement of work ability in modalities of short-and long-term psychotherapy: the differential impact of reflective ability and other aspects of patient suitability. J Clin Psychol. https://doi.org/10.1002/jclp.23128
Acknowledgements
This study was financially supported by the Social Insurance Institution of Finland (18/26/2020) and (45/26/2021).
Funding
This study was funded by the Social Insurance Institution of Finland (18/26/2020 to AV) and (45/26/2021 to SS).
Author information
Authors and Affiliations
Contributions
Conceptualization and methodology SS, AV, KG, JK, JT, and AK; writing-original draft preparation: SS; statistical analyses KG; writing-review and editing: SS, AV, KG, JK, and JT. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The ethics committee of the Finnish Institute of Occupational Health has approved the study.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Consent for publication was obtained for every individual person’s data included in the study.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Selinheimo, S., Gluschkoff, K., Kausto, J. et al. The association of sociodemographic characteristics with work disability trajectories during and following long-term psychotherapy: a longitudinal register study. Soc Psychiatry Psychiatr Epidemiol 59, 621–630 (2024). https://doi.org/10.1007/s00127-023-02523-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-023-02523-y