
Abstract
Aims/hypothesis
Studies in children have reported an association between increased BMI and risk for developing type 1 diabetes, but evidence in late adolescence is limited. We studied the association between BMI in late adolescence and incident type 1 diabetes in young adulthood.
Methods
All Israeli adolescents, ages 16–19 years, undergoing medical evaluation in preparation for mandatory military conscription between January 1996 and December 2016 were included for analysis unless they had a history of dysglycaemia. Data were linked with information about adult onset of type 1 diabetes in the Israeli National Diabetes Registry. Weight and height were measured at study entry. Cox proportional models were applied, with BMI being analysed both as a categorical and as a continuous variable.
Results
There were 777 incident cases of type 1 diabetes during 15,819,750 person-years (mean age at diagnosis 25.2±3.9 years). BMI was associated with incident type 1 diabetes. In a multivariable model adjusted for age, sex and sociodemographic variables, the HRs for type 1 diabetes were 1.05 (95% CI 0.87, 1.27) for the 50th–74th BMI percentiles, 1.41 (95% CI 1.11, 1.78) for the 75th–84th BMI percentiles, 1.54 (95% CI 1.23, 1.94) for adolescents who were overweight (85th–94th percentiles), and 2.05 (95% CI 1.58, 2.66) for adolescents with obesity (≥95th percentile) (reference group: 5th–49th BMI percentiles). One increment in BMI SD was associated with a 25% greater risk for incidence of type 1 diabetes (HR 1.25, 95% CI 1.17, 1.32).
Conclusions
Excessively high BMI in otherwise healthy adolescents is associated with increased risk for incident type 1 diabetes in early adulthood.
Graphical abstract

Similar content being viewed by others



Introduction
The incidence of type 1 diabetes peaks before the age of 20 years but more cases present in adulthood than in youth [1,2,3]. While genetic susceptibility plays an important role in the pathogenesis of type 1 diabetes [4], there is accumulating evidence to suggest a role for environmental and behavioural factors. This role is highlighted by the 2–3% annual global increase in type 1 diabetes incidence rates over recent decades [5, 6].
A parallel global increase in obesity rates has been observed across various countries and age groups [7]. This trend, together with the established role of obesity in the pathophysiology of type 2 diabetes, led to studies examining a possible link between obesity and type 1 diabetes. A few studies have reported a link between either high birthweight or early childhood obesity and childhood-onset type 1 diabetes, with a wide range in point estimates [8,9,10,11,12,13,14,15,16,17]. This discrepancy is probably related to use of recalled vs measured data for defining obesity, assessment of childhood BMI at various ages, and controlling for health status at baseline.
We recently reported that adolescent obesity increases the risk of type 2 diabetes in a nationwide cohort of adolescents who were medically assessed prior to mandatory military service, and whose data were linked with the Israel National Diabetes Registry (INDR) [18]. Given the paucity of evidence linking adolescent body weight and type 1 diabetes [9, 12, 13, 16, 17], our goal was to analyse the association between adolescent BMI and incident type 1 diabetes in the same cohort.
Methods
Study population
This was a nationwide population-based retrospective cohort study that comprised all male and female adolescents, ages 16 to 19 years, who were medically evaluated 1 year prior to compulsory military service between 1 January 1996 and 31 December 2016. This is the same cohort in which we recently reported an association between adolescent BMI and type 2 diabetes mellitus in young adulthood [18]. Participants with a history of diabetes or dysglycaemia, those with missing BMI records, or those who died before establishment of the INDR in 2012 were excluded (see electronic supplementary material [ESM] Fig. 1). Our final cohort included 1,426,362 adolescents who were followed continuously from the age of 17 years until the earliest date of diabetes onset, death, or 31 December 2016. This study was approved by the institutional ethical review boards of the Israel Defense Forces Medical Corps and Maccabi Health Services, an Israeli health maintenance organisation.
Diagnosis of type 1 diabetes
The primary outcome of this study was the incidence of type 1 diabetes. Since 2012, all Israeli health maintenance organisations have been required by law to annually report diabetes prevalence to the INDR. A diabetes case is reported to the INDR if at least one of the following criteria is met: (1) HbA1c ≥6.5% (47.5 mmol/mol), (2) a serum glucose concentration of 11.1 mmol/l (≥200 mg/dl) in two tests performed at least 1 month apart, or (3) three or more purchases of glucose-lowering medications in different months. Based on these criteria, the sensitivity for diabetes is 95.1%.
The registry does not regularly include any data regarding the type of diabetes, such as information about islet autoantibodies. However, in 2016, as part of a special project aimed at classifying diabetes type, the registry received data regarding the history of prescribed diabetes medications. Based on this information, type 1 diabetes was determined only in participants who met all the following criteria: (1) actively treated with short-acting insulin, (2) treatment with short-acting insulin was initiated within 1 year of diabetes onset, and (3) only insulin was prescribed, with no history of oral diabetes drugs. Individuals who were prescribed an oral glucose-lowering medication were classified as having type 2 diabetes, and individuals for whom data regarding glucose-lowering medications were unavailable were classified as ‘diabetes of uncertain type’. Both of the latter groups were excluded from the present analysis. Gestational diabetes cases were not reported to the registry.
Our study cohort was created by linking the data obtained from the central registry of the Israel Defense Forces, using a national unique identifier, as reported previously [19,20,21], with the data from the INDR and islet autoantibody data from Maccabi Health Services (MHS), the second largest health maintenance organisation in Israel. This allowed us to link medical data obtained during adolescence, including weight and height measurements, with diabetes status later in life.
Islet autoantibody data
Data regarding islet autoantibodies were available only for participants insured by MHS who were registered with type 1 diabetes in the INDR (n=271; 35% of type 1 cases in the study). The electronic medical records of participants insured by MHS who developed type 1 diabetes during the study period according to the INDR criteria were searched for the presence of islet autoantibodies relevant to the diagnosis of type 1 diabetes (anti-GAD, anti-islet cells or anti-insulin antibodies). For participants with missing islet autoantibodies data, we were unable to determine whether testing was never done or was performed outside of MHS, as hospital records and records from other health maintenance organisations were unavailable. In sub-analyses in which islet autoantibody presence was an additional criterion for the definition of type 1 diabetes, those with missing data regarding autoantibody testing were not considered as valid cases.
Islet autoantibody levels were analysed in certified hospital laboratories until 2013, after which levels were tested in one central MHS laboratory using commercial ELISA kits. Until 2013, anti-insulin antibodies were tested using commercial kits Orgentec anti-IAA Ab (Orgentec, Mainz, Germany) and afterwards using AESKULISA anti-insulin-IgG (AESKU Diagnostics, Wendelsheim, Germany). Anti-GAD antibodies were tested using commercial radioimmunoassay kits until 2013, and using AESKULISA GAD65 thereafter (AESKU Diagnostics, Wendelsheim, Germany). Anti-islet cell antibody and anti-GAD65 levels were assessed using Aesku IA2-GAD until 2013, and AESKULISA IA2-GAD65 thereafter (both from AESKU Diagnostics, Wendelsheim, Germany). Antibody detection was defined as positive when the titre of antibodies was above the upper limit of the normal range established by each manufacturer.
Data collection and study variables
Physician evaluation of adolescents preceding military conscription included a review of pre-existing medical records, taking of a medical history, and a physical examination. Weight and height were measured using a beam balance and stadiometer, with participants barefoot and wearing only light clothing. For the purpose of this study, adolescents were categorised as having ‘unimpaired health’ if they did not have an active condition requiring chronic medical care or treatment, a history of major surgery, or a history of cancer.
Sociodemographic data were reported at study entry from various governmental sources. Residential socioeconomic status was reported from the Central Statistical Bureau on a 1–10 scale, and was divided into three ordinal groups (low, medium or high) [21, 22]. Education level was categorised according to whether the participant attended formal schooling for ≤10 years, 11 years or 12 years, based on data received from the Ministry of Education. Cognitive performance was assessed by a general intelligence test [23], and was categorised as low (<−1 SD), medium (−1 to 1 SD) and high (>1 SD). BMI was classified according to age- and sex-matched percentiles based on criteria developed by the US Center for Disease Control and Prevention and validated for Israeli adolescents [22]: BMI<5th percentile (underweight), 5th≤BMI≤49th percentiles, 50th≤BMI≤74th percentiles, 75th≤BMI≤84th percentiles, 85th≤BMI≤94th percentiles (overweight) and BMI≥95th percentile (obesity). In certain sub-analyses with a more limited case density, the BMI categories in the normal BMI range were combined to a single category (5th–84th percentiles).
Statistical analysis
The incidence rate of type 1 diabetes was calculated per person-years of follow-up. Kaplan–Meier survival curves were computed for the BMI percentile categories with 95% CI. Cox proportional hazard models were used to estimate the HRs and 95% CIs for incident diabetes using the 5th–49th BMI percentile group as the reference. In sub-analyses with four BMI categories, the entire normal weight range was used as the reference group. We also analysed BMI as a continuous variable using absolute values or in its z score form to allow a better comparison of our findings with those of previous reports [8, 24, 25]. Cox models were either unadjusted, minimally adjusted (on the basis of sex, birth year and age at study entry), or adjusted for multiple variables including the minimal variables plus individual socioeconomic-related variables, education level and cognitive performance. Penalised spline models with four degrees of freedom were used to estimate the HR and 95% CI [26]. Spline models were fully adjusted and included all adolescents with BMI values between 12 and 35 kg/m2. The population-attributable risk percentage (PAR%) of type 1 diabetes incidence was calculated for overweight and obesity (≥85th BMI percentile) with an unverified assumption of causality as follows: PAR% = Pe × (HR − 1)/[Pe × (HR − 1) + 1] × 100, where HR is the unadjusted HR for type 1 diabetes for adolescents who are overweight or obese (vs those with BMI<85th percentile), and Pe is its mean prevalence.
Several sensitivity analyses were performed. (1) To minimise residual confounding by coexisting morbidities, we restricted the Cox analysis to those with unimpaired health status at study entry (n=979,668). (2) To ensure that the association between BMI and the risk for type 1 diabetes was not confounded by autoimmune conditions that may not require a specific therapy or routine follow-up and thus were not included in the sub-analysis, we excluded from analysis all participants with any history of autoimmune comorbidity other than type 1 diabetes (n=1,391,448). (3) We restricted the analysis to those who were enrolled in the study between 1996 and 2004 to allow minimal follow-up to at least 30 years of age (n=600,401). (4) We restricted analysis to participants with at least 6 months of follow-up (n=1,415,952). (5) We set the outcome measure as type 1 diabetes occurring before 25 years of age. (6) For examinees who were insured by MHS (n=574,720), we additionally included the presence of islet autoantibodies as a criterion for type 1 diabetes case definition. In these analyses we used the presence of at least one or two islet autoantibodies as a case criterion.
Results
Baseline characteristics of the 834,050 men and 592,312 women included in the study are shown in Table 1. Age at study entry was comparable across all BMI groups. Compared with the low to normal BMI groups, the overweight and obese groups had higher proportions of participants with lower residential socioeconomic status, lower scores on cognitive tests, and lower proportions of Israeli-born individuals.
There were 777 incident cases of type 1 diabetes recorded during 15,819,750 person-years (incidence=4.9 cases/100,000 person-years). The median follow-up period was 11.2 years (IQR 5.8–16.3), with shorter follow-up for individuals with a higher BMI. The crude incidence rate showed a consistent graded increase across BMI groups from underweight to obesity, from 3.6 to 8.4 cases per 100,000 person-years, respectively (Table 2). Kaplan–Meier survival analysis confirmed these findings (Fig. 1).

Kaplan–Meier survival analysis of the association between adolescent obesity and incident type 1 diabetes in young adulthood stratified by BMI categories (5th–49th percentiles, overweight and obese). The number of individuals at risk is indicated below each panel for the given BMI category as well as incidence in each time interval (I, 0–5 years; II, 5–10 years; III, 10–15 years; IV, 15–20 years)
The results persisted in Cox analyses, and were consistent overall, regardless of the level of variable adjustment. There was no interaction between BMI and any of the variables in the model. In a multivariable model adjusted for sex, birth year, age at study entry, education and cognitive performance, the HRs were 1.05 (95% CI 0.87, 1.27) for the 50th–74th BMI percentiles, 1.41 (95% CI 1.11, 1.78) for the 75th–84th BMI percentiles, 1.54 (95% CI 1.23, 1.94) for adolescents who were overweight, and 2.05 (95% CI 1.58, 2.66) for adolescents with obesity (Table 2). An increase in BMI of five units was associated with a 35% greater risk for incident type 1 diabetes (adjusted HR5unit-BMI=1.35; 95% CI 1.24, 1.47), and one increment in BMI SD was associated with 25% greater risk (adjusted HR=1.25; 95% CI 1.17, 1.32).
Sensitivity analyses
Similar findings were observed when the sample was limited to individuals with unimpaired health at baseline (ESM Table 1), after excluding those with any history of autoimmune conditions (ESM Table 1), when the analysis was limited to participants who were enrolled in the study up to 2004 (ESM Table 1), and when the outcome was defined as incident type 1 diabetes before age 25 years (ESM Table 1). We also observed consistent findings when the analysis was stratified by sex (ESM Table 2). The unadjusted HR for incident type 1 diabetes among adolescents who were overweight or obese was 1.66 (1.39–1.97) and the fraction of type 1 diabetes attributed to adolescent overweight and obesity (PAR%) was 10.1% (95% CI 6.3, 14.2). The projected PAR% based on the prevalence of overweight and obesity in 2016 in this cohort (22%) was 12.8% (95% CI 7.1, 17.8).
Assessing the association between adolescent BMI and type 1 diabetes using islet autoantibody data
Forty per cent of the study population (n=574,720) were insured by MHS, and their baseline characteristics were comparable to the rest of the cohort (n=851,642; ESM Table 3). Among the 271 incident cases of type 1 diabetes among this subgroup, 77 (28%) had no islet autoantibody data, 167 (62%) had at least one islet autoantibody detected, 93 (34%) had at least two islet autoantibodies detected, 15 (6%) had at least one negative and one missing islet autoantibody result, and 12 (4%) had negative tests for the presence of anti-islet, anti-GAD and anti-insulin antibodies.
Using diagnostic criteria that additionally included detection of at least one islet autoantibody, we observed a graded increase in crude incidence of type 1 diabetes across BMI categories (measured as cases per 100,000 person-years), with an incidence of 2.38 with normal BMI (5th–84th percentile), 3.15 with overweight, and 6.27 with obesity (see ESM Table 4 for detailed case incidence and follow-up data). The results of the Kaplan–Meier analysis are shown in ESM Fig. 2. The computed adjusted HRs were 1.40 (0.86–2.27) and 2.90 (1.80–4.68) for adolescents who were overweight or obese, respectively (ESM Table 4). These point estimates were accentuated when the diagnosis of type 1 diabetes was based on the presence of two islet autoantibodies in addition to the INDR criteria, with HRs of 1.93 (1.08–3.46) for overweight and 3.14 (1.68–5.88) for obesity. Underweight was not significantly associated with risk for type 1 diabetes irrespective of the model used, the diagnostic criteria for type 1 diabetes, or reference BMI group.
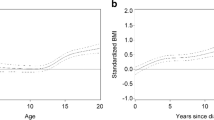
Cox regression spline models that present the adjusted HRs across the entire BMI continuum are shown in Fig. 2 for the entire cohort (grey) using INDR type 1 diabetes criteria, and for adolescents insured by MHS (orange) for whom the case definition additionally included the presence of at least one islet autoantibody. Both models showed a significant linear trend (p=1.7×10−11 and p=1.1×10−3, respectively), but not a non-linear trend (p=0.69 and p=0.28, respectively).

Cox regression spline models for the HR and 95% CI between BMI and incident type 1 diabetes. The penalised models were fitted using four degrees of freedom, and adjusted for sex, birth year, age at study entry, country of birth, education and cognitive performance. The primary spline model (grey) included all adolescents with adolescent BMI values between 12 and 35 kg/m2 (N=1,399,874) in whom 765 incident cases of type 1 diabetes were recorded according to INDR criteria. The secondary spline model (orange) included only adolescents insured by MHS (N=564,948), and for whom the outcome additionally included the presence of at least one islet autoantibody (164 events)
Discussion
In this large population-based retrospective study, we found that increased BMI in late adolescence was associated with incident type 1 diabetes in young adulthood. The HR for type 1 diabetes was 1.25 per unit of BMI z score increment, and the risk for type 1 diabetes was nearly doubled among obese adolescents. These point estimates withstood rigorous sensitivity analysis, and remained stable following adjustment for sociodemographic variables. When the presence of at least one islet autoantibody was added to the type 1 diabetes case definition, the HR increased to 1.40 (0.86–2.27) and 2.90 (1.80–4.68) for adolescents who were overweight or obese, respectively. When the analysis was restricted to individuals with at least two types of islet autoantibodies, the association was even more robust.
Although the methods of inclusion and exclusion are not consistent across epidemiological studies of type 1 diabetes, reported incidence rates are in line with the incidence rate of 4.9 in 100,000 person-years observed in our cohort, which had a mean baseline age of 17.3 years and a median follow-up of 11.2 years. For example, in nine centres across eight European countries, the reported incidence ranged from 4.8 to 13.4 per 100,000 person-years at ages 15–29 years from 1996–1997 [27]. Previous studies of the association between childhood BMI and incident type 1 diabetes reported a wide range of odds ratios. For children at ages 7–13 years, the reported ORs ranged between insignificance to 1.2 and 1.8 per unit z score [8, 24, 25]. A meta-analysis of nine studies reported ORs for type 1 diabetes within a range of 1.7–3.8 for children with obesity (pooled OR 2.0) [13]. A wide range of point estimates was also apparent in cohorts of young adult women with obesity (age range approximately 20–50 years), with reported HRs of 2.7 [10] and 4.7 [9]. Methodological factors that contribute to this discrepancy may include population selection, age of childhood BMI assessment, methods used to define type 1 diabetes (self-reported vs established diagnosis by various criteria), and measured vs recalled anthropometric data. Factors related to statistical methodology may also play a part, including controlling for health status at baseline and differential adjustment for potential confounders. In this regard, our study has several strengths, including a homogeneous and narrow age range at assessment, measured anthropometric data, and an established diagnosis of type 1 diabetes. Our results corroborate point estimates derived from a meta-analysis (pooled ORz score=1.25 vs HRz score=1.25 in our study) [13], as well as a smaller national-level study from Denmark (ORz score=1.21) [8].
There is growing evidence of a link between obesity and various autoimmune conditions [10, 28]. A possible explanation is that the elevated levels of adipokines and cytokines associated with obesity diminish self-tolerance by promoting proinflammatory processes. Additional factors associated with obesity may contribute to the development of autoimmunity, including vitamin D deficiency, consumption of a high-fat diet, and modulation of the gut microbiota. Given that, in our cohort, there was an association between obesity and type 1 diabetes even when excluding those with pre-existing autoimmune conditions, additional factors may link obesity specifically to type 1 diabetes. In fact, several biological mechanisms have been suggested to explain the association between obesity and type 1 diabetes. The ‘accelerator hypothesis’ [29] suggests that both type 1 and type 2 diabetes are caused by insulin resistance set against various genetic backgrounds that affect the rate of loss of beta cells and the disease phenotype. According to this hypothesis, the increasing demand for insulin renders the beta cells more antigenic, and thus accelerates their loss through autoimmune injury. High rates of insulin production may be associated with accumulation of misfolded proteins in insulin-producing cells, causing endoplasmic reticulum stress [30]. To adapt to endoplasmic reticulum stress, beta cells activate the unfolded protein response in order to increase endoplasmic reticulum folding capacity, but this signalling pathway also augments inflammation, attracting immune cells and triggering the exposure of neo-antigens [31]. In the TrialNet Pathway to Prevention Study of a cohort of relatives of people with type 1 diabetes, participants who were overweight and obese had an increased risk of islet autoantibody expression and developing type 1 diabetes, even in the absence of type 1 diabetes-related HLA alleles [32, 33]. While one population-based study [34] contradicted the view that excess weight is a risk factor for islet cell autoimmunity, this discordant outcome may be related to differences in study population characteristics, including baseline islet autoimmunity state, age of assessment, and proportions of type 1 diabetes-related HLA alleles.
There is increasing evidence for a shared and complex genetic basis for type 1 diabetes, type 2 diabetes and obesity [35]. For example, the SNP in TCF7L2 is considered to be a strong risk factor for type 2 diabetes and was recently also linked to increased risk for type 1 diabetes, primarily in adolescents aged 12 years or older [36]. This may explain why, in some patients, classic type 2 diabetes risk factors, such as excess weight, may influence islet autoimmunity. Finally, a Mendelian randomisation study supported an effect of childhood adiposity on childhood-onset type 1 diabetes risk (<17 years), with an OR of 1.32 per SD score in BMI [37].
It is possible that different mechanisms contribute to the observed association to different degrees in different populations. The accelerator hypothesis predicts that increased obesity prevalence lowers the threshold of genetic susceptibility, causing more individuals with a low-risk genetic profile to develop type 1 diabetes. Indeed, independent studies from Finland and the UK [38, 39] showed that the proportion of low-risk HLA haplotypes has increased among cases of incident type 1 diabetes over recent decades. Importantly, we observed consistent point estimates in both adolescent overweight and obesity groups that either limited follow-up to age 25 years (approximately 7 years) or limited follow-up to a minimum of 13 years. These results suggest that high BMI may indeed be a contributing factor to the pathogenesis of type 1 diabetes rather than merely unmasking a diminished capacity for insulin secretion.
Our findings have public health implications. The prevalence of adolescent obesity is rising worldwide at an alarming rate, with dire projections for the near future. Currently it is estimated that nearly 60% of US children will develop obesity by their early thirties, mostly by adolescence, with half progressing to severe obesity [40]. With rising levels of obesity, we may expect a continued rise in type 1 diabetes. We obtained a PAR% of 10.1% for adolescent overweight and obesity throughout the 20-year study period, with a projection of 12.8% based on recent prevalence of overweight and obesity. This expected increase in type 1 diabetes will most likely be accompanied by higher proportion of complications, as obesity appears to be a risk factor for the development of macrovascular and microvascular morbidities as well as for all-cause mortality among patients with type 1 diabetes [41,42,43,44].
Our study has limitations. First, classifying type 1 diabetes based on the lack of use of oral therapy in addition to short-acting insulin, or based on confirmed islet autoantibodies, as was done in one of the sub-analyses, increases specificity at the expense of lowering the sensitivity threshold. Due to occasional off-label prescribing, chiefly of metformin or sodium–glucose co-transporter 2 inhibitors, it is assumed that a small proportion of type 1 diabetes cases may have been missed, especially among obese participants who are more likely to be prescribed such medications. As a result, the association between obesity and type 1 diabetes incidence may be underestimated in our study. However, point estimates of the association were unchanged when analysis was limited to adolescents who entered the study before 2004, a time at which the use of sodium–glucose co-transporter 2 inhibitors or glucagon-like peptide 1 receptor analogues was uncommon. Second, due to the retrospective nature of our study, islet autoantibody data were missing in 28% of participants in the MHS sub-cohort with a diagnosis of type 1 diabetes. These missing data were unlikely to be associated with meaningful misclassification as the point estimates persisted when the latter were included or excluded from analysis. Third, adolescent BMI was based on a single weight measurement, and we lacked longitudinal data to assess trajectories or the cumulative effect of excessive BMI. To address this limitation, we performed a sub-analysis to examine the incidence of type 1 diabetes over a shorter follow-up period of 7 years or less. Fourth, we lacked data regarding other type 1 diabetes risk factors, such as maternal BMI or family history of type 1 diabetes [45]. Fifth, information about participants who were lost to follow-up due to emigration from Israel was unavailable. However, the rate of emigration was low and is expected to represent a non-differential misclassification error. Finally, our study design cannot infer a causal relationship between adolescent excessive BMI and incident type 1 diabetes. Our study also has a set of strengths, with systematic data collection and use of measured BMI, strict control of adolescent health at baseline, and well-defined diagnostic criteria for type 1 diabetes. Lastly, access to a large, national-level sample size allowed determination of the association of incident type 1 diabetes with BMI across the entire BMI range.
In conclusion, our study adds to the growing evidence regarding the health hazards associated with adolescent obesity. Not only is adolescent obesity correlated with adult onset of type 2 diabetes as previously reported [18], but also with type 1 diabetes. Further work needs to be done to unravel this association so that we can better address the full spectrum of risks posed by the obesity epidemic or identify common environmental factors affecting both weight and type 1 diabetes.
Data availability
The data are not publicly available due to privacy and ethical restrictions. Interested parties may contact the corresponding author.
Abbreviations
- INDR:
-
Israel National Diabetes Registry
- MHS:
-
Maccabi Health Services
- PAR%:
-
Population-attributable risk percentage
References
Rogers M, Kim C, Banerjee T, Lee JM (2017) Fluctuations in the incidence of type 1 diabetes in the United States from 2001 to 2015: a longitudinal study. BMC Med 15(1):1–9. https://doi.org/10.1186/s12916-017-0958-6
Thomas NJ, Jones SE, Weedon MN, Shields BM, Oram RA, Hattersley AT (2018) Frequency and phenotype of type 1 diabetes in the first six decades of life: a cross-sectional, genetically stratified survival analysis from UK biobank. Lancet Diabetes Endocrinol 6(2):122–129. https://doi.org/10.1016/S2213-8587(17)30362-5
Bruno G, Novelli G, Panero F et al (2009) The incidence of type 1 diabetes is increasing in both children and young adults in northern Italy: 1984-2004 temporal trends. Diabetologia 52(12):2531–2535. https://doi.org/10.1007/s00125-009-1538-x
Redondo MJ, Jeffrey J, Fain PR, Eisenbarth GS, Orban T (2008) Concordance for islet autoimmunity among monozygotic twins. N Engl J Med 359(26):2849–2850. https://doi.org/10.1056/nejmc0805398
Lawrence JM, Divers J, Isom S et al (2021) Trends in prevalence of type 1 and type 2 diabetes in children and adolescents in the US, 2001-2017. JAMA 326(8):717–727. https://doi.org/10.1001/jama.2021.11165
Patterson CC, Harjutsalo V, Rosenbauer J et al (2019) Trends and cyclical variation in the incidence of childhood type 1 diabetes in 26 European centres in the 25 year period 1989–2013: a multicentre prospective registration study. Diabetologia 62(3):408–417. https://doi.org/10.1007/s00125-018-4763-3
Dai H, Alsalhe TA, Chalghaf N, Riccò M, Bragazzi NL, Wu J (2020) The global burden of disease attributable to high body mass index in 195 countries and territories, 1990–2017: an analysis of the global burden of disease study. PLoS Med 17(7):e1003198. https://doi.org/10.1371/journal.pmed.1003198
Antvorskov JC, Aunsholt L, Buschard K et al (2018) Childhood body mass index in relation to subsequent risk of type 1 diabetes – a Danish cohort study. Pediatr Diabetes 19(2):265–270. https://doi.org/10.1111/pedi.12568
Ferrara CT, Geyer SM, Evans-Molina C et al (2017) The role of age and excess body mass index in progression to type 1 diabetes in at-risk adults. J Clin Endocrinol Metab 102(12):4596–4603. https://doi.org/10.1210/jc.2017-01490
Harpsøe MC, Basit S, Andersson M et al (2014) Body mass index and risk of autoimmune diseases: a study within the Danish National Birth Cohort. Int J Epidemiol 43(3):843–855. https://doi.org/10.1093/ije/dyu045
Hyppönen E, Virtanen SM, Kenward MG et al (2000) Obesity, increased linear growth, and risk of type 1 diabetes in children. Diabetes Care 23(12):1755–1760. https://doi.org/10.2337/diacare.23.12.1755
Svensson J, Carstensen B, Mortensen HB, Borch-Johnsen K (2007) Growth in the first year of life and the risk of type 1 diabetes in a Danish population. Paediatr Perinat Epidemiol 21(1):44–48. https://doi.org/10.1111/j.1365-3016.2007.00775.x
Verbeeten KC, Elks CE, Daneman D, Ong KK (2011) Association between childhood obesity and subsequent type 1 diabetes: a systematic review and meta-analysis. Diabet Med 28(1):10–18. https://doi.org/10.1111/J.1464-5491.2010.03160.X
Goldacre RR (2018) Associations between birthweight, gestational age at birth and subsequent type 1 diabetes in children under 12: a retrospective cohort study in England, 1998–2012. Diabetologia 61(3):616–625. https://doi.org/10.1007/S00125-017-4493-Y
The Eurodiab Substudy 2 Study Group (2002) Rapid early growth is associated with increased risk of childhood type 1. Diabetes Care 25(10):1755–1760. https://doi.org/10.2337/diacare.25.10.1755
Waernbaum I, Dahlquist G, Lind T (2019) Perinatal risk factors for type 1 diabetes revisited: a population-based register study. Diabetologia 62(7):1173–1184. https://doi.org/10.1007/s00125-019-4874-5
Lammi N, Moltchanova E, Blomstedt PA, Tuomilehto J, Eriksson JG, Karvonen M (2009) Childhood BMI trajectories and the risk of developing young adult-onset diabetes. Diabetologia 52(3):408–414. https://doi.org/10.1007/s00125-008-1244-0
Twig G, Zucker I, Afek A et al (2020) Adolescent obesity and early-onset type 2 diabetes. Diabetes Care 43(7):1487–1495. https://doi.org/10.2337/dc19-1988
Tsur AM, Hershkovich S, Zucker I et al (2021) Stuttering and incident type 2 diabetes: a population-based study of 2.2 million adolescents. J Clin Endocrinol Metab 106(4):978–987. https://doi.org/10.1210/clinem/dgaa988
Bardugo A, Bendor CD, Zucker I et al (2021) Adolescent nonalcoholic fatty liver disease and type 2 diabetes in young adulthood. J Clin Endocrinol Metab 106(1):e34–e44. https://doi.org/10.1210/clinem/dgaa753
Shapiro M, Arbel C, Zucker I et al (2021) Asthma in youth and early-onset type 2 diabetes: a nationwide study of 1.72 million Israeli adolescents. J Clin Endocrinol Metab 106(12):e5043–e50553. https://doi.org/10.1210/clinem/dgab542
Twig G, Yaniv G, Levine H et al (2016) Body-mass index in 2.3 million adolescents and cardiovascular death in adulthood. N Engl J Med 374(25):2430–2440. https://doi.org/10.1056/nejmoa1503840
Twig G, Tirosh A, Derazne E et al (2018) Cognitive function in adolescence and the risk for premature diabetes and cardiovascular mortality in adulthood. Cardiovasc Diabetol 17(1):154. https://doi.org/10.1186/s12933-018-0798-5
Viner RM, Hindmarsh PC, Taylor B, Cole TJ (2008) Childhood body mass index, breastfeeding and risk of type 1 diabetes: findings from a longitudinal national birth cohort. Diabet Med 25(9):1056–1061. https://doi.org/10.1111/j.1464-5491.2008.02525.x
Blom L, Persson LÅ, Dahlquist G (1992) A high linear growth is associated with an increased risk of childhood diabetes mellitus. Diabetologia 35(6):528–533. https://doi.org/10.1007/BF00400480
Govindarajulu US, Malloy EJ, Ganguli B, Spiegelman D, Eisen EA (2009) The comparison of alternative smoothing methods for fitting non-linear exposure–response relationships with cox models in a simulation study. Int J Biostat 5(1):article 2. https://doi.org/10.2202/1557-4679.1104
Kyvik KO, Nystrom L, Gorus F et al (2004) The epidemiology of type 1 diabetes mellitus is not the same in young adults as in children. Diabetologia 47(3):377–384. https://doi.org/10.1007/s00125-004-1331-9
Tsigalou C, Vallianou N, Dalamaga M (2020) Autoantibody production in obesity: is there evidence for a link between obesity and autoimmunity? Curr Obes Rep 9(3):245–254. https://doi.org/10.1007/s13679-020-00397-8
Wilkin TJ (2009) The accelerator hypothesis: a review of the evidence for insulin resistance as the basis for type I as well as type II diabetes. Int J Obes 33(7):716–726. https://doi.org/10.1038/ijo.2009.97
Kalwat MA, Scheuner D, Rodrigues-Dos-Santos K, Eizirik DL, Cobb MH (2021) The pancreatic β-cell response to secretory demands and adaption to stress. Endocrinology 162(11):173. https://doi.org/10.1210/endocr/bqab173
Mallone R, Eizirik DL (2020) Presumption of innocence for beta cells: why are they vulnerable autoimmune targets in type 1 diabetes? Diabetologia 63(10):1999–2006. https://doi.org/10.1007/s00125-020-05176-7
Ferrara-Cook C, Geyer SM, Evans-Molina C et al (2020) Excess BMI accelerates islet autoimmunity in older children and adolescents. Diabetes Care 43(3):580–587. https://doi.org/10.2337/dc19-1167
Ferrara CT, Geyer SM, Liu YF et al (2017) Excess BMI in childhood: a modifiable risk factor for type 1 diabetes development? Diabetes Care 40(5):698–701. https://doi.org/10.2337/dc16-2331
Winkler C, Marienfeld S, Zwilling M, Bonifacio E, Ziegler AG (2009) Is islet autoimmunity related to insulin sensitivity or body weight in children of parents with type 1 diabetes? Diabetologia 52(10):2072–2078. https://doi.org/10.1007/s00125-009-1461-1
Inshaw JRJ, Sidore C, Cucca F et al (2021) Analysis of overlapping genetic association in type 1 and type 2 diabetes. Diabetologia 64(6):1342–1347. https://doi.org/10.1007/s00125-021-05428-0
Redondo MJ, Geyer S, Steck AK et al (2018) TCF7L2 genetic variants contribute to phenotypic heterogeneity of type 1 diabetes. Diabetes Care 41(2):311–317. https://doi.org/10.2337/dc17-0961
Censin JC, Nowak C, Cooper N, Bergsten P, Todd JA, Fall T (2017) Childhood adiposity and risk of type 1 diabetes: a Mendelian randomization study. PLoS Med 14(8):e1002362. https://doi.org/10.1371/journal.pmed.1002362
Gillespie KM, Bain SC, Barnett PAH et al (2004) The rising incidence of childhood type 1 diabetes and reduced contribution of high-risk HLA haplotypes. Lancet 364(9446):1699–1700. https://doi.org/10.1016/S0140-6736(04)17357-1
Hermann R, Knip M, Veijola R et al (2003) Temporal changes in the frequencies of HLA genotypes in patients with type 1 diabetes – indication of an increased environmental pressure? Diabetologia 46(3):420–425. https://doi.org/10.1007/s00125-003-1045-4
Ward ZJ, Long MW, Resch SC, Giles CM, Cradock AL, Gortmaker SL (2017) Simulation of growth trajectories of childhood obesity into adulthood. N Engl J Med 377(22):2145–2153. https://doi.org/10.1056/nejmoa1703860
Corbin KD, Driscoll KA, Pratley RE, Smith SR, Maahs DM, Mayer-Davis EJ (2018) Obesity in type 1 diabetes: pathophysiology, clinical impact, and mechanisms. Endocr Rev 39(5):629–663. https://doi.org/10.1210/er.2017-00191
Purnell JQ, Hokanson JE, Marcovina SM, Steffes MW, Cleary PA, Brunzell JD (1998) Effect of excessive weight gain with intensive therapy of type 1 diabetes on lipid levels and blood pressure: results from the DCCT. Diabetes Control Complications Trial JAMA 280(2):140–146. https://doi.org/10.1001/jama.280.2.140
Edqvist J, Rawshani A, Adiels M et al (2019) BMI, mortality, and cardiovascular outcomes in type 1 diabetes: findings against an obesity paradox. Diabetes Care 42(7):1297–1304. https://doi.org/10.2337/dc18-1446
Dahlström EH, Sandholm N, Forsblom CM et al (2019) Body mass index and mortality in individuals with type 1 diabetes. J Clin Endocrinol Metab 104(11):5195–5204. https://doi.org/10.1210/jc.2019-00042
Lindell N, Carlsson A, Josefsson A, Samuelsson U (2018) Maternal obesity as a risk factor for early childhood type 1 diabetes: a nationwide, prospective, population-based case–control study. Diabetologia 61(1):130–137. https://doi.org/10.1007/s00125-017-4481-2
Authors’ relationships and activities
The authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Contribution statement
IZ conceived and designed the study, statistically analysed and interpreted the data, and drafted and revised the manuscript. AB and YZ statistically analysed and interpreted the data, and drafted and revised the manuscript. YC interpreted the data and critically revised the manuscript. ED and AMT performed statistical analysis, interpreted the data and contributed to the discussion and critically revised the manuscript. DT and CMC and ML acquired data and critically revised the manuscript. TC-Y, OP-H, IR, AA, AT, NM, GC and HCG contributed to the discussion and critically revised the manuscript. GT designed and supervised the study, statistically analysed and interpreted the data, and drafted and revised the manuscript. GT is the guarantor of this work, and as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. GT also takes full responsibility for the work as a whole, including the study design, access to data, and the decision to submit and publish the manuscript. All authors approved the final version to be published.
Funding
This study was partially funded by a research grant from the Medical Corps Israel Defense Forces (Israel) awarded to GT.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(PDF 498 kb)
Rights and permissions
About this article

Cite this article
Zucker, I., Zloof, Y., Bardugo, A. et al. Obesity in late adolescence and incident type 1 diabetes in young adulthood. Diabetologia 65, 1473–1482 (2022). https://doi.org/10.1007/s00125-022-05722-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-022-05722-5