
Abstract
Aims/hypothesis
The PlA1/A2 polymorphism of platelet glycoprotein IIIa (GPIIIa) has been implicated in the pathogenesis of type 2 diabetes. We studied this polymorphism in a homogenous, extensively phenotyped cohort using the candidate gene approach.
Methods
The PlA1/A2 polymorphism was determined in 1051 patients with type 2 diabetes and in 2247 individuals without type 2 diabetes.
Results
In patients with type 2 diabetes, genotype frequencies were as follows: PlA1/A1 71.4%, PlA1/A2 26.0%, and PlA2/A2 2.7%. In individuals without type 2 diabetes, genotype frequencies were 71.6%, 25.7% and 2.8%, respectively. The PlA2 allele was not associated with fasting and postprandial glucose, glycated haemoglobin, insulin, proinsulin, C-peptide and calculated indices of insulin resistance or pancreatic beta cell function. The PlA2 allele was also not significantly associated with angiographic CHD (adjusted odds ratio [OR] 1.13; 95% CI, 0.93–1.39) or with a history of previous myocardial infarction (adjusted OR 1.09; 95% CI, 0.87–1.37).
Conclusions/interpretation
The GPIIIa PlA1/A2 polymorphism is not associated with type 2 diabetes, glucose metabolism, angiographic CHD or myocardial infarction.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
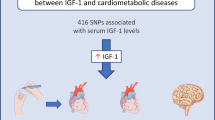
Platelet glycoprotein IIb/IIIa is a membrane receptor for fibrinogen and von Willebrand factor. The PlA1/A2 polymorphism of the glycoprotein IIIa (GPIIIa) subunit results from a T to C transition of the GPIIIa gene, replacing leucine by proline at amino acid residue 33 of GPIIIa [1]. This polymorphism has been implicated in vascular disease (review see [2]). A recent case-control study of 215 subjects reported a more than two-fold higher prevalence of PlA2 in patients with type 2 diabetes than in individuals with normal glucose metabolism [3]. In an attempt to substantiate this observation, we analysed the association between the GPIIIa PlA1/PlA2 polymorphism and type 2 diabetes and CHD in 3298 individuals.
Subjects and methods
Study design
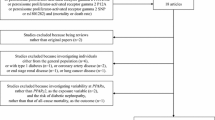
Our study includes Caucasian patients hospitalised for coronary angiography [4]. Clinically relevant CHD was defined as the presence of a visible luminal narrowing (≥20% stenosis) in at least one of 15 coronary segments [5]. Patients with type 1 diabetes were excluded from this analysis. The study was approved by the ethics review committee at the “Landesärztekammer Rheinland-Pfalz” (Medical Council of Rhineland Palatinate, Mainz, Germany) and written informed consent was obtained from the participants.
Laboratory procedures
Fasting blood glucose was determined enzymatically using the hexokinase method (Roche Diagnostics, Mannheim, Germany). Cholesterol and triglycerides were measured using enzymatic reagents from Wako (Neuss, Germany) [4]. LDL and HDL cholesterol were measured by a combined ultracentrifugation–precipitation method [4]. HbA1c was determined by high-performance liquid chromatography (DIAMAT, Chromsystem Instruments & Chemicals, Martinsried, Germany). Enzyme immunoassays were used to determine the following: insulin (AIA-PACK IRI, Eurogenetics, Eschborn, Germany), C-peptide (AIA-PACK C-peptide, Eurogenetics), and pro-insulin (IBL, Hamburg, Germany). The GPIIIa PlA1/A2 polymorphism was determined with a multilocus genotyping assay [6]. The accuracy of this assay has recently been evaluated by direct sequencing or restriction fragment length analysis [7]. We determined the reproducibility of this method in a subset of 165 individuals who were enrolled for a second or third investigation in the Ludwigshafen Risk and Cardiovascular Health Study (n=147 twice, n=18 three times). A total of 183 (147+18+18) additional DNA samples were genotyped in a blinded fashion. In each of the 183 samples, we obtained consistent results.
Metabolic studies
An OGTT was performed in individuals not previously diagnosed as having type 2 diabetes. Normoglycemia, IGT and type 2 diabetes were diagnosed according to the American Diabetes Association (ADA) criteria [8]. In addition, individuals with a history of diabetes or treatment with hypoglycaemic agents were defined as diabetic. Insulin sensitivity and pancreatic beta cell function were estimated using HOMA-IR and %beta respectively [9]. Subjects with LDL cholesterol levels greater than 4.1 mmol/l or triglyceride levels greater than 2.3 mmol/l or HDL cholesterol lower than 1 mmol/l were considered dyslipidaemic.
Statistical analysis
Continuous variables between CHD patients and control subjects were compared by analysis of variance, adjusting for sex and age (Table 1). Associations between genotypes and clinical and biochemical variables (Table 2) were evaluated by the Mann–Whitney rank sum test. Associations between categorical variables were examined by logistic regression analysis, including covariables as indicated (Table 3). In models assuming a co-dominant (additive) effect of the PlA2-allele, the genotypes PlA1/A1, PlA1/A2 and PlA2/A2 were coded as 0, 1, and 2 respectively. When assuming a dominant effect, genotype PlA1/A1 was coded as 0, and PlA1/A2 and PlA2/A2 combined as 1. When assuming a recessive effect, genotypes PlA1/A1 and PlA1/A2 were coded as 0, and PlA2/A2 as 1. The SPSS statistical package, version 11.0 for Windows (SPSS, Chicago, Ill., USA) was used.
Results
Patients with type 2 diabetes (n=1051) were significantly older and had a higher mean BMI than individuals without type 2 diabetes (n=2247). Current or past smoking was less prevalent in the former; angiographic CHD and hypertension were more frequent. More patients with type 2 diabetes than those without were taking ACE inhibitors and calcium channel blockers, had higher systolic blood pressure, higher fasting glucose, higher triglycerides and lower HDL cholesterol. Mean LDL cholesterol was significantly lower in patients with type 2 diabetes than in subjects who did not have type 2 diabetes (Table 1).
The genotypes PlA1/A1, PlA1/A2, PlA2/A2 occurred at similar frequencies both in patients with type 2 diabetes (71.4%, 26.0%, and 2.7% respectively), and in non-diabetic individuals (71.6%, 25.7%, and 2.8% respectively). Logistic regression analysis assuming co-dominant (additive), dominant or recessive effects of the PlA2 allele did not reveal any association with type 2 diabetes, regardless of whether or not we included age, sex, BMI or CHD status as co-variables (data not shown).
To investigate whether the GPIIIa PlA1/A2 polymorphism affected glucose metabolism, we analysed 1997 individuals, in whom an OGTT was performed and who were not being treated with oral hypoglycaemic agents or insulin. This subgroup consisted of subjects with normal glucose tolerance, IGT and newly diagnosed type 2 diabetes. The PlA1/A2 polymorphism was not significantly associated with any of the measures of glucose metabolism (Table 2).
The A2 allele was also not significantly associated with the prevalence of angiographic CHD and a history of myocardial infarction. Adjustments for established cardiovascular risk factors including age, sex, BMI, type 2 diabetes, smoking, hypertension and dyslipidaemia slightly increased ORs, but none of the associations reached statistical significance (Table 3).
Discussion
The current study has two key results. First, we did not obtain any evidence for a relationship between the PlA1/A2 polymorphism and glucose metabolism. Second, the PlA1/A2 polymorphism was not associated with CHD or with a history of myocardial infarction, a finding which is completely consistent with previous findings [2].
Type 2 diabetes is influenced by genetic factors. So far, linkage scans and association studies have revealed only few consistent susceptibility loci for type 2 diabetes [10]. As classical linkage may be of limited merit in the genetic analysis of polygenic diseases, association studies might be the strategy of choice to unravel the genetic causes of type 2 diabetes [11]. However, association studies have produced highly discrepant results, especially when numbers of cases and controls have been small. In many instances, the positive associations seen in small studies have been disproven in subsequent studies of large cohorts. A recent study [3], claiming an association between the GPIIIa PlA1/A2 polymorphism and type 2 diabetes, included 112 patients with type 2 diabetes and 103 control subjects, with the two groups originating from different clinical settings. The type 2 diabetes patients enrolled in that study were recruited at a diabetes clinic, the control subjects were people presenting with chest-pain at a cardiology department. This recruitment strategy is clearly different from that used in our study, which exclusively enrolled patients scheduled for angiography. An important reason for the false-positive findings by Tschoepe and co-workers [3] may be that the PlA2 allele occurred at a frequency of 14.6% only in their non-diabetic control subjects, a value substantially lower than the prevalence of 28.5% found in the current study and the prevalence of 26.2% found in a recent meta-analysis of 8829 individuals without previous myocardial infarction [2].
Our study, however, may still have limitations. We exclusively enrolled individuals with clinically indicated coronary angiography, and this may have resulted in a referral bias. As to the definition of the coronary artery status, this is also a possible strength of our study. The prevalence of clinically asymptomatic coronary atherosclerosis has been reported to be high at or above 50 years of age [12]. Hence, angiography-based recruitment of control subjects rules out the possibility of individuals with significant, yet clinically unapparent coronary artery disease being inadvertently allocated to the control group. Surprisingly, our control group appears well representative, since the major cardiovascular risk factors occur at a frequency similar to that found in the general population. The prevalence of hypertension is close to that found in a random probability sample from Germany [13]. Diabetes mellitus appears two to three times more frequently than in the German population [14]. This, however, is probably due to the fact that we did not rely on self-reports. Rather, we measured fasting glucose and performed an oral glucose challenge in individuals not previously known to have diabetes mellitus. Based on clinical history or fasting glucose measurements, the National Health and Nutrition Examination survey 1999–2000 reports prevalences of diabetes mellitus of 9.2% in adults between 40 and 59 years of age and and 19.3% in adults older than 60 years [15]. In the current study, 12.1% of the control subjects had diabetes mellitus according to this criterion, while another 5.6% were detected by elevated post-challenge glucose only.
In summary, our results strongly argue against a role of this polymorphism in the development of type 2 diabetes and indicate that sample sizes have to be adequately large in genetic association studies to avoid false positive findings.
Abbreviations
- GPIIIa:
-
glycoprotein IIIa
- OR:
-
odds ratio
References
Newman PJ, Derbes RS, Aster RH (1989) The human platelet alloantigens, PlA1 and PlA2, are associated with a leucine33/proline33 amino acid polymorphism in membrane glycoprotein IIIa, and are distinguishable by DNA typing. J Clin Invest 83:1778–1781
Morgan TM, Coffey CS, Krumholz HM (2003) Overestimation of genetic risks owing to small sample sizes in cardiovascular studies. Clin Genet 64:7–17
Tschoepe D, Menart B, Ferber P et al. (2003) Genetic variation of the platelet- surface integrin GPIIb-IIIa (PIA1/A2-SNP) shows a high association with Type 2 diabetes mellitus. Diabetologia 46:984–989
Winkelmann BR, März W, Boehm BO et al. (2001) Rationale and design of the LURIC study—a resource for functional genomics, pharmacogenomics and long-term prognosis of cardiovascular disease. Pharmacogenomics 2:S1–S73
Austen WG, Edwards JE, Frye RL et al (1975) A reporting system on patients evaluated for coronary artery disease. Report of the ad hoc committee for grading of coronary artery disease. Circulation 50:7–40
Hoppe C, Cheng S, Grow M et al. (2001) A novel multilocus genotyping assay to identify genetic predictors of stroke in sickle cell anaemia. Br J Haematol 114:718–720
Tobin MD, Braund PS, Burton PR et al. (2004) Genotypes and haplotypes predisposing to myocardial infarction: a multilocus case-control study. Eur Heart J 25:459–467
No authors listed (1997) Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 20:1183–1197
Levy JC, Matthews DR, Hermans MP (1998) Correct homeostasis model assessment (HOMA) evaluation uses the computer program. Diabetes Care 21:2191–2192
Florez JC, Hirschhorn J, Altshuler D (2003) The inherited basis of diabetes mellitus: implications for the genetic analysis of complex traits. Annu Rev Genomics Hum Genet 4:257–291
Altshuler D, Hirschhorn JN, Klannemark M, et al. (2000) The common PPARgamma Pro12Ala polymorphism is associated with decreased risk of type 2 diabetes. Nat Genet 26:76–80
Tuzcu EM, Kapadia SR, Tutar E et al. (2001) High prevalence of coronary atherosclerosis in asymptomatic teenagers and young adults: evidence from intravascular ultrasound. Circulation 103:2705–2710
Wolf-Maier K, Cooper RS, Banegas JR et al. (2003) Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. JAMA 289:2363–2369
Hauner H, Koster I, von Ferber L (2003) [Prevalence of diabetes mellitus in Germany 1998–2001. Secondary data analysis of a health insurance sample of the AOK in Hesse/KV in Hessen. Dtsch Med Wochenschr 128:2632–2637
Centers for Disease Control and Prevention (CDC) (2003) Prevalence of diabetes and impaired fasting glucose in adults—United States, 1999–2000. MMWR Morb Mortal Wkly Rep 52:833–837
Acknowledgements
We thank Andrea Müller and Manuela Gutenkunst for technical assistance. We also thank Dr Suzanne Cheng, Roche Diagnostics, Alameda, Calif., USA for providing the multilocus genotyping assay and financial support. The study was in part supported by research grants to B.O. Boehm (DFG SFB 518 and IZKF project A1 University of Ulm).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
März, W., Boehm, B.O., Winkelmann, B.R. et al. The PlA1/A2 polymorphism of platelet glycoprotein IIIa is not associated with the risk of type 2 diabetes. The Ludwigshafen Risk and Cardiovascular Health Study. Diabetologia 47, 1969–1973 (2004). https://doi.org/10.1007/s00125-004-1557-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-004-1557-6