
Abstract
Purpose
Damage control orthopaedics (DCO) und early total care (ETC) are well-established strategies for managing severely injured patients. There is no definitive evidence of the superiority of DCO over ETC in polytrauma patients. We conducted this study to assess the probability of a polytraumatised patient undergoing DCO. In addition, the effect of DCO on complications and mortality was investigated.
Methods
We analysed data from 12,569 patients with severe trauma (Injury Severity Score ≥ 16) who were enrolled in the trauma registry of the German Trauma Society (TraumaRegister DGU®) from 2009 to 2016 and had undergone surgery for extremity or pelvic fractures. These patients were allocated to a DCO or an ETC group. We used the propensity score to identify factors supporting the use of DCO. For a comparison of mortality rates, the groups were stratified and matched on the propensity score.
Results
We identified relevant differences between DCO and ETC. DCO was considerably more often associated with packed red blood cell (pRBC) transfusions (33.9% vs. 13.4%), catecholamine therapy (14.1% vs. 6.8%), lower extremity injuries (72.4% vs. 53.5%), unstable pelvic fractures (41.0% vs. 25.9%), penetrating injuries (2.8% vs. 1.5%), and shock (20.5% vs. 10.8%) and unconsciousness (23.7% vs. 16.3%) on admission. Based on the propensity score, patients with penetrating trauma, pRBC transfusions, unstable pelvic fractures, and lower extremity injuries were more likely to undergo DCO. A benefit of DCO such as reduced complications or reduced mortality was not detected.
Conclusion
We could identify some parameters of polytrauma patients used in the trauma registry (Traumaregister DGU®), which led more likely to a DCO therapy. The propensity score did not demonstrate the superiority of DCO over ETC in terms of outcome or complications. It did not appear to adequately adjust for the variables used here. Definitive evidence for or against the use of DCO remains unavailable.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The term ‘damage control’ refers to a treatment strategy that aims to keep the impact of initial surgical treatment to the minimum level necessary in severely injured patients [24]. Rotondo et al. proposed the damage control approach in 1993 in order to address the large incidence of penetrating injuries in the United States [49]. The concept of damage control surgery focuses on ensuring the immediate survival of injured patients by reducing the initial treatment measures, which are usually surgical in nature, and on rapidly stabilising patients in the medical intensive care setting. Based on this concept, damage control orthopaedics (DCO) describes a similar approach for the management of injuries to the musculoskeletal system. This applies in particular to the stabilisation of pelvic and extremity fractures, usually with the use of external fixation systems, until definitive care can be provided [17]. By contrast, early total care (ETC) refers to the primary definitive treatment of such injuries, for example with primary intramedullary nailing or plate fixation.
Since the 1980s, clinical research has addressed the question of whether it is more appropriate for polytrauma patients to undergo DCO or ETC. Behrman et al. and Harvin et al. showed in their retrospective studies that the early fixation of femur fractures was associated with a reduction in pulmonary complications and health care costs [2, 21]. They investigated, however, only patients who underwent intramedullary nailing, which is a typical ETC approach in the group of patients who received early definitive care. Charash et al. carried out a retrospective study to determine whether early intramedullary nailing of femoral fractures in polytrauma patients with an Injury Severity Score (ISS) ≥ 18 led to a higher rate of pulmonary complications when thoracic trauma was present or absent [7]. They reported that the risk of pulmonary complications, the length of hospital stay, and the length of stay in the intensive care unit (ICU) tended to be greater in patients with delayed intramedullary nailing of femur fractures regardless of whether or not they had sustained thoracic trauma. The differences between the patient groups, however, were not significant.
In 2016, Liu et al. conducted a meta-analysis and they too found no significant differences in the rate of pulmonary complications, multiple organ failure, and mortality between early and delayed intramedullary nailing of femur fractures in patients with concomitant severe thoracic trauma [33]. Early definitive care thus does not appear to have any disadvantages in comparison to delayed definitive treatment. The aforementioned studies, however, investigated the timing of surgery and did not directly compare DCO and ETC. Pape et al. addressed this issue in 2007 and conducted a prospective randomised clinical study on patients with multiple injuries [40]. They compared stable patients and patients at risk of complications (borderline patients). ETC for femur fractures in stable patients was associated with shorter ventilation times and a lower incidence of pulmonary failure and sepsis than DCO. By contrast, borderline patients who underwent ETC had a significantly higher rate of pulmonary complications than those who received DCO. Unstable patients were excluded. Tuttle et al. compared multiply injured patients who underwent either DCO (n = 55) or ETC (n = 42) for femoral shaft fractures and found no significant differences between the groups for adult respiratory distress syndrome (ARDS), multiple organ failure, ICU length of stay, and hospital length of stay [54]. DCO patients, however, had a significantly shorter operative time and less estimated blood loss from their initial surgical procedure. According to Giannoudis, ETC is indicated in patients with stable haemodynamics, stable oxygen saturation, a lactate level < 2 mmol/L, no coagulation disturbances, a normal temperature, urinary output > 1 mL/kg/hour, and no requirement for inotropic support [13]. Although this description of patients who are suitable for ETC is different from the definition of stable patients by Pape et al. [40], they point in the same direction. In other studies investigating different treatment strategies, the role of DCO in the management of polytrauma patients is controversial [1, 22, 23, 36, 37, 45, 52, 53]. Rixen et al. noted, for example, that there was no data that met the requirements of evidence-based medicine and demonstrated the superiority of damage control orthopaedics over early total care [47].
As described above, the decision to use the DCO approach in the management of patients depends on a variety of factors including patient-related variables such as age and gender as well as injury-related and treatment-related variables. Examples of injury-related variables are injury severity and the mechanism of injury. Treatment-related variables are the level of the treating trauma centre and the time of treatment. Additional variables may be taken into consideration as well [31].
These variables provide the basis for propensity score analyses. The propensity score is defined as the probability that a patient receives a given treatment [6, 29]. In our study, this treatment is the management of an extremity injury using the DCO approach. The propensity score is also used to estimate the effects of treatment according to DCO principles on outcome, which is of particular interest here. The propensity score is a useful alternative method for analysing non-randomised studies and registry data [29,30,31].
In the study presented here, we hypothesised that the management of polytrauma patients on the basis of DCO principles is superior to an ETC approach in terms of outcome and complications. By this we agree with Scalea, who writes in 2002 that polytrauma patients benefit from initial surgical care that addresses only the haemorrhage, and are then further stabilised (in intensive care) [51]. Final stabilisation could then be done later. He writes this based on his impressions from the drug wars of the 1980s and 1990s, where patients with multiple injuries died despite successful interventions.
The main objectives of our study were:
-
(1)
to assess what variables are associated with the use of DCO on the basis of data from the trauma registry of the German Trauma Society (TraumaRegister DGU®) and on the basis of the propensity scores that we calculated using these registry data and
-
(2)
to evaluate the effect of DCO on complications and outcome on the basis of propensity scores.
Material and methods
TraumaRegister DGU®
The TraumaRegister DGU® of the German Trauma Society (Deutsche Gesellschaft für Unfallchirurgie, DGU) was founded in 1993. The aim of this multi-centre database is the pseudonymised and standardised documentation of severely injured patients. Data are collected prospectively in four consecutive time phases from the site of the accident until discharge from hospital: (A) prehospital phase, (B) emergency/resuscitation room and initial surgery, (C) intensive care unit, and (D) discharge.
Documentation includes detailed information on demographics, injury patterns, comorbidities, prehospital and inhospital management, the course on the intensive care unit, relevant laboratory findings including data on transfusion, and outcome. Included are patients who are admitted to hospital via the resuscitation room and subsequently receive intensive or intermediate care and patients who arrive at hospital with vital signs and die before admission to the intensive care unit. The infrastructure for documentation, data management, and data analysis is provided by the Academy for Trauma Surgery (Akademie der Unfallchirurgie GmbH, AUC), which is affiliated to the German Trauma Society. Scientific leadership is provided by the Committee on Emergency Medicine, Intensive Care and Trauma Management (Sektion NIS) of the German Trauma Society. Participating hospitals submit their pseudonymised data to a central database via a web-based application. Scientific data analysis is approved according to a peer review process described in the publication guideline of TraumaRegister DGU®. The participating hospitals are primarily located in Germany (90%), but a growing number of hospitals in other countries contribute data as well (i.e. Austria, Belgium, Finland, Luxembourg, Slovenia, Switzerland, the Netherlands, and the United Arab Emirates). Currently, approximately 30,000 cases from more than 650 hospitals are entered into the database per year. Participation in the TraumaRegister DGU® is voluntary. For hospitals associated with TraumaNetzwerk DGU®, however, the entry of at least a basic data set is obligatory for reasons of quality assurance.
The study presented here was performed in accordance with the publication guideline of the TraumaRegister DGU® and is registered as TR-DGU Project ID 2016-011.
Patients
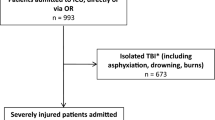
We analysed data from 12,569 patients who were enrolled in the trauma registry from 2009 to 2016. Figure 1 shows how these patients were identified from the 238,360 data sets that were available in the TraumaRegister DGU® from 2009 to 2016. Included were patients with an Injury Severity Score (ISS) ≥ 16 who had been admitted to hospital via the resuscitation room, had undergone surgery, and had then been transferred to the intensive care unit. Only primary admissions to local, regional or supraregional trauma centres in Germany were included. The patients who were enrolled in the study had been treated in a total of 176 hospitals. Only data from standard documentation forms were used since the QM documentation form does not include relevant parameters. Excluded were patients without a fracture of the pelvis, femur, tibia, fibula, humerus, radius, or ulna. In the last line of Fig. 1, 5567 patients were excluded, because they had not undergone surgery. 1679 of them died during their hospital stay, 1132 of them within the first 24 h after arrival. The remaining 3888 patients had not undergone surgery (e.g. conservative therapy) or the documentation of the surgical procederes were not available.

Patient identification process
Patient groups
The 12,569 patients who were included in the study were divided into two groups. The damage control orthopaedics (DCO) group consisted of patients who were managed on the basis of damage control principles and patients who were treated with external fixation of at least one long bone fracture and/or a pelvis fracture. Patients in the DCO group were compared with all other patients who underwent surgery, so the fractures of those patients were treated only with a definitive technique such as a medullary nail or a plate without getting an external fixator first. These patients formed the early total care (ETC) group.
Statistical analysis
Descriptive statistics were expressed as percentages and numbers for categorical variables and as means and standard deviations (SDs) for metric variables. Median and interquartile ranges (IQRs) were reported for highly skewed data. The chi-square test was used for comparing frequencies and the Mann–Whitney U test for metric data (regardless of data distribution). Because of the large number of patients and the wide variety of comparisons, statistical significance should be interpreted with caution.
The propensity score is defined as the probability that a given intervention or treatment is provided [31]. In our study, we calculated the probability that a patient underwent DCO. Treatment according to DCO principles was the dependent variable and the transfusion of packed red blood cells (pRBCs), patient age, etc. were independent or predictor variables.
Propensity scores were obtained using logistic regression. This approach allowed adjusted effects of possible predictors to be calculated and presented using odds ratios (ORs).
The goodness-of-fit of the model was assessed using coefficients of determination, i.e. the Cox and Snell pseudo-R2 and the Nagelkerke pseudo-R2. The value of coefficients of determination is between 0 and 1. The higher the value, the better the goodness-of-fit of the model.
Propensity scores were used to form deciles of probability for comparisons of outcome (mortality). In addition, propensity scores were used for exact matching on the basis of rounded percentages. A patient from the DCO group was matched with a patient from the ETC group with the same propensity score.
Data were analysed using the SPSS software package (version 24, IBM Inc., Armonk, NY, United States).
We divided the variables in the TraumaRegister DGU® into groups of variables. Propensity scores were calculated on the basis of the variables listed in Table 1.
Ethics committee
The Ethics Committee of the University of Ulm informed us on 12 June 2017 that our study did not need ethical approval.
Results
Baseline characteristics
A total of 12,569 patients were included in the study. Of these, 8199 (65%) were allocated to the DCO group and 4370 (35%) to the ETC group. Tables 2 and 3 provide an overview of baseline characteristics of the patients in the DCO and ETC groups (i.e. demographics, mechanism of trauma, injuries, prehospital physiology and treatment, inhospital care, complications and outcome).
A comparison of the treatment groups showed a much higher percentage of penetrating trauma and a much lower percentage of falls from a height of less than 3 m in the DCO group. The percentages of patients with lower extremity injuries and unstable pelvic injuries were also considerably higher in the DCO group. The same applies to the presence of shock (defined as a blood pressure ≤ 90 mmHg) and unconsciousness, prehospital catecholamine therapy, pRBC transfusions in the resuscitation room, and the total number of surgical procedures. A comparison of patient outcomes showed that the patients in the DCO group had longer ICU lengths of stay, had sepsis more frequently, and had considerably higher mortality rates than the ETC group.
Propensity score
We were able to calculate propensity scores for 12,033 patients (96%) with complete data. The following variables were found to have no major effect (p > 0.10): gender, abdominal trauma, upper extremity injury, and coagulopathy. In accordance with Pape et al. [39], coagulopathy was defined as a prolonged partial thromboplastin time (PTT) of 50 s or more or an International Normalised Ratio (INR) of 1.4 or higher.
Based on odds ratios, the variables that were most strongly associated with the DCO approach were lower extremity fractures, unstable pelvic fractures, and transfusion requirements prior to admission to the ICU, the presence of penetrating trauma, and the number of injuries. Odds ratios suggested that ETC was most commonly used in young patients (under 16 years of age) and in patients whose injuries resulted from a fall from a low height. Table 4 provides an overview of these data. A forest plot graphically displaying the logistic regression is shown in Fig. 2. It demonstrates, for example, that there were no relevant differences between treatment provided in supraregional and regional trauma centres since the confidence intervals for the odds ratios were close to 1. Most parameters were very close to 1. The closer the values are to 1, the more difficult it is to identify an independent variable. In our study, an odds ratio of 1 meant that the DCO approach and the ETC approach were equally likely to be used in the management of patients.

Forest plot displaying the results of the logistic regression. AIS Abbreviated Injury Scale, pRBC packed red blood cell(s)
Table 5 shows the propensity scores, i.e. the probability of a patient receiving DCO, for different strata. The results confirm that patients with high probability values actually underwent DCO. Regardless of the probability of a patient receiving DCO, as indicated by the propensity score, mortality associated with DCO treatment was, however, always higher than mortality after ETC (Fig. 3).

Inhospital mortality for stratified DCO and ETC groups and probability of a patient receiving DCO (propensity scores). DCO damage control orthopaedics, ETC early total care
We also used the propensity score for matching patients who received DCO with patients who underwent ETC treatment. We were able to match 3663 patients in the DCO group (45% of all DCO patients) with 3663 patients in the ETC group (84% of all ETC patients). The results for the matched groups of patients are shown in Table 6. For most variables, similar results were obtained for the two groups. Mortality in the DCO group, however, was more than twice as high as in the ETC group. Complications related to the treatment of a polytrauma patient, such as sepsis, multiple organ failure and pulmonary failure, were also relevantly higher in the DCO group than in the ETC group.
Discussion
The primary objective of this study was to assess the probability that a severely injured patient receives treatment according to the principles of damage control orthopaedics. For this purpose, we calculated propensity scores, which we also used to investigate the effects of DCO, as described by Kuss et al. [29], and to compare the outcomes of damage control orthopaedics and early total care.
In this study, the propensity score allowed us to identify a few variables that make it considerably more probable that the DCO approach is used in the management of patients compared to ETC. Contrary to our expectations, however, our study, which was based on data from the TraumaRegister DGU®, did not demonstrate the superiority of DCO over ETC concerning the occurrence of complications such as multi-organ failure, pulmonary failure and sepsis, as well as mortality, although the propensity score is described in the literature as well suited to analysing registry data [29, 31]. Is this problem to prove the advantage of damage control strategies limited to DCO/ETC in polytrauma care? A recent study of DCS in abdominal trauma, also based on data from the Traumaregister DGU® struggled to demonstrate a clear advantage for damage control therapy as well[57]. In another study using data from the Traumaregister DGU®, it was possible to show that observed and expected mortality using the RISC score in trauma patients with an AIS max of ≥ 3 in extremity injuries and at least one femur fracture decreased over the years from 2002 to 2018, while the proportion of temporary fixation compared to early total care of the femur increased [5]. In their data analysis, Bläsius et al. found that mainly more severely injured patients with a higher ISS and concomitant injuries received damage control orthopaedics. In addition, this patient group had a higher mortality and a higher rate of multi-organ failure and sepsis. This indicates that the more severely injured patients with an expected worse outcome were more likely to receive DCO therapy, making comparability between ETC and DCO much more difficult. In contrast, in our study we did not look at changes in care over time, but focused on the possible motivations and decisive parameters for using Damage Control Orthopedics. In addition, when using the propensity score in our study, we not only looked at which parameters made a DCO treatment more likely, but also used propensity score matching to make the outcome between ETC and DCO more comparable.
There are two possible reasons for our results. Either DCO is indeed associated with poorer survival than ETC, or adjustment for the variables included here was insufficient to explain why a decision to use or not to use DCO was made. The patient groups showed major differences even in some baseline characteristics (e.g. ISS, shock, massive transfusions) that revealed that patients who received DCO were much sicker than patients in the ETC group. For this reason, we used propensity score matching in order to reduce any possible bias. Even after propensity score matching, the patients in the groups still show differences for example in ISS. These differences are also statistically significant. Whether this difference is relevant due to the very large number of patients is for the reader to decide. Giannoudis et al. reported that the key factors in identifying patients who benefitted the most from DCO were the patients’ overall physiological state and injury characteristics [14]. Following initial care in the resuscitation room, polytrauma patients can be divided into four groups, i.e. stable, borderline, unstable, and in extremis, as proposed by Pape et al. [41]. The more stable the patient is, the more suitable he or she is for ETC. The more unstable the patient is, the more sensible it is to use DCO [41]. However, the presented result in this publication is still only a retrospective study using the propensity score and not a multicenter, prospective randomised trial.
Another possible explanation for the higher mortality and complication rate in our DCO group is that the decision either for or against DCO was made after a relatively long period of time. In severely injured patients who sustained injuries to the chest, abdomen and the extremities, torso injuries are often treated first [19]. During the time from the beginning of care in the resuscitation room and the end of treatment of torso injuries, treatment can have considerable effects on patient stability. These effects are not reflected in the data that are available in the TraumaRegister DGU®. In theory, a patient who is initially stable in the resuscitation room and then becomes unstable would be unlikely to receive ETC. DCO would then be associated with a higher probability of mortality because of the patient’s unstable condition. By contrast, a patient who is unstable in the resuscitation room and requires massive transfusions would in general be sufficiently stable to receive ETC after having undergone treatment for torso injuries and damage control resuscitation (DCR). DCR is a group of measures, such as permissive hypotension, early use of blood products, and the limited use of crystalloid fluids, that effectively address the lethal triad of coagulopathy, metabolic acidosis, and hypothermia [12, 32]. In this case, an initially unstable patient would have a lower probability of mortality after ETC. The focus on the patient’s condition in the dynamic initial phase has led to an approach that is referred to as early appropriate care (EAC) [1, 3]. Parameters such as acidosis seem to have emerged that allow early appropriate care after successful damage control resuscitation, despite an initially unstable patient [34]. The proven effectiveness of DCR [42] could also explain why Feldman et al. could not demonstrate an advantage of DCO over ETC in the treatment of femoral shaft fractures [11]. This is because their DCO group consisted of patients from 2007 to 2019, a period in which DCR was increasingly implemented. The ETC group consisted of patients from 1996 to 2006, so it is more than questionable whether a comparison between ETC and DCO is methodological possible at all. That DCR is effective in stabilising unstable patients could also explain the results of the study by Rixen et al., who randomised patients to either DCO or ETC [46]. Rixen et al. reported that the surgeon decided to shift from DCO to ETC or vice versa in three of the 33 patients who had undergone surgery before the study had to be terminated. The surgeon explained that the decisions to perform either DCO (n = 1) or ETC (n = 2), which were the result of randomisation prior to surgery, were no longer acceptable. The results of our study suggest that propensity scores work more effectively when treatment decisions and the assessment of variables are closely related in time.
Against this background, the results reported by Yamamoto et al. are particularly surprising [58]. They too used the propensity score and propensity score matching as well in order to compare inhospital mortality after ETC and DCO and reported that DCO was associated with a significantly lower mortality rate. This difference between DCO and ETC was probably attributable to the selection of patients. Yamamoto et al. included all patients who presented with long bone fractures and an AIS ≥ 2 and who underwent definitive care during their hospital stay. They thus excluded all patients who died after initial treatment and before definitive care. This applied to more than 50% of the patients with extremity injuries and thus led to a bias. This approach could also explain why the pulmonary complications in the DCO group were not higher as it is in our study. This is supported by a retrospective study by Santolini et al., who reported that definitive internal fixation after DCO was performed no earlier than after a mean period of 6.7 (± 4.5) days [50]. In our study, 34% of the patients who died in the hospital died within the first 24 h. The proportion of patients who died within the first 24 h is similar to that reported by Bieler et al. in a study on trauma patients [4].
Logistic regression identified a number of parameters that increased the probability of a severely injured patient to receive damage control orthopaedics. These parameters were the transfusion of pRBCs, penetrating trauma, an unstable pelvic fracture, and a lower extremity injury. These parameters are useful predictors of DCO. Many parameters had values close to 1 in the logistic regression. This means that these parameters cannot be clearly allocated to either DCO or ETC. By contrast, polytrauma in children and adolescents and falls from a low height were good predictors of ETC. This is in line with current research on trauma care for severely injured children [26].
The majority of severely injured patients were treated with DCO. Based on the data sets that were analysed in this study, 65.2% of the patients received DCO and 34.8% underwent ETC. This confirms a study that was conducted in 2002 by Pape et al., who reported that the number of polytrauma patients who were treated with DCO continued to increase [38]. When it comes to the management of polytrauma patients in supraregional trauma centres, we found in our study that the number of patients who underwent DCO was almost twice as high as the number of patients who received ETC. In local trauma centres, by contrast, more patients were treated with ETC compared to DCO. Kuhmola et al. reported, however, that only 22% of polytrauma patients were treated with DCO for femoral shaft fractures in a tertiary trauma centre from 2006 to 2018 while 78% underwent ETC [28]. Giannoudis et al. too reported that approximately 20% of polytrauma patients were treated with DCO. They did not state, however, whether this percentage applied to the total group of polytrauma patients or only to polytrauma patients with extremity or pelvic injuries [14]. DCO for the management of polytrauma patients accounted for a percentage of less than 25% in another study as well [9]. Against the background of these percentages, our distribution between the groups studied is nevertheless very surprising. One possible explanation could be that we assigned all patients to the DCO group as soon as only one long bone fracture or a pelvic fracture had been treated with an external fixator in the surgical treatment, even if other fractures had already been definitively treated. After all, almost 60% of the patients in the DCO group had multiple extremity injuries. In the study by Bläsius et al. of the 11409 patients who received surgical treatment, 6241 patients were treated with an external fixator [5]. This means that 54% received a temporary external fixator. This study is also based on the data of Traumaregister DGU®, but focuses exclusively on femur fractures, while we look at all long bone and pelvic fractures.
A closer look at our patient group shows that the DCO group included a higher number of patients with signs of shock and consumption coagulopathy, a higher rate of prehospital reanimation, higher pRBC requirements, and a lower Glasgow Coma Scale score. Although most differences between the DCO and the ETC group were not relevant, all investigated clinical parameters suggested that patients in the DCO group at least tended to be sicker and less stable than patients in the ETC group. This finding confirms the results of a study that was published in 2005 by Rixen et al., who investigated the management of femoral shaft fractures in severely injured patients on the basis of TraumaRegister DGU® data [45]. The DCO approach was more commonly applied in patients with a high ISS not only in our study but also in other studies [8, 10, 15, 27, 37, 45]. More severely injured patients are more often treated in supraregional trauma centres and more often undergo DCO. This is confirmed by our results. A comparison of the two treatment approaches during and outside normal hours showed that the percentage of patients who underwent DCO in the on-call setting (67.9% of the DCO patients) was higher than the percentage of patients who received ETC by on-call staff (64.6% of the ETC patients). The difference, however, was not relevant. Dei Guidici et al. [9] too found no relevant difference in the treatment strategies for polytrauma patients who were treated on weekends and those who were admitted on weekdays, although the percentage of DCO patients in their Level 2 trauma centre was much lower than in our study. The objective of DCO is to avoid the burden of the additional surgical trauma associated with ETC, although this implies that a higher number of surgical procedures must be accepted in order to improve patient outcome. There is, however, no clearly defined parameter for outcome. Instead, a variety of outcome parameters can be investigated and defined. In the present study, we analysed the length of stay in the intensive care unit, the mean duration of ventilation (intubation days), the length of hospital stay, the rate of sepsis according to the criteria defined in the TraumaRegister DGU®, the rate of patients with multiple organ failure, pulmonary failure, mortality within the first 24 h, and inhospital mortality. Our results revealed some relevant differences between the two patient groups. DCO was associated with a considerably longer ICU length of stay, a considerably higher rate of sepsis, considerably higher rate of pulmonary failure, considerably higher rate of multi-organ failure, considerably higher mortality within the first 24 h, and considerably higher inhospital mortality. Even in our matched groups the rates of sepsis, multi-organ failure, pulmonary failure and mortality were higher in the DCO group. By contrast, Pape et al., who conducted a retrospective cohort study on the treatment of patients with femoral shaft fractures during three different time periods, reported that the increasing use of the DCO approach had led to a decrease in the incidence of multiple organ failure [38]. This finding was confirmed by another study, which also found that DCO treatment was associated with a less severe systemic inflammatory response than ETC [23]. In 2007, Pape et al. published a prospective randomised multi-centre study and reported that even stable patients who were treated with the DCO approach had considerably shorter duration of ventilation and a lower rate of sepsis than patients who underwent primary intramedullary nailing of the femur [40]. Pape et al., however, excluded all critically injured and unstable patients. In a more recent study using data from the Traumaregister DGU®, Bläsius et al. found a higher sepsis rate in severely injured patients who had been treated with an external fixator [5].
Many of the studies mentioned in this paper refer only to the treatment of femoral fractures in their comparison between ETC and DCO, respectively between early and delayed definitive fixation [2, 21, 23, 38, 40]. In some cases, these studies only distinguished between primary treatment with an intramedullary nail (ETC) and primary application of an external fixator (DCO). However, if the aim of the damage control techniques is also to minimise the second hit through initial surgical treatment [17, 18, 24], these studies show only part of the truth, as they do not take into account the treatment of all other limb fractures and the treatment by other ETC techniques. In our study fractures of the pelvis as well as all fractures of long bones of the extremities were included. This could also be a possible explanation why, in contrast to our study, these studies often showed a significant reduction in complications such as ARDS and multi-organ failure when using DCO, because the use of an intramedullary nail for femoral fractures is relatively often associated with pulmonary complications [25, 56]. On the other hand, there is a consensus among experts that early stabilisation of long bone fractures is widely accepted among experts in the treatment of severely injured patients, while other DCO indications have been dropped [44].
The way the DCO and ETC groups were formed in our study has its limitations, which must be kept in mind when our results are discussed. For example, the DCO group included patients who had been treated with external fixation of pelvic and/or long bone fractures. We cannot be sure that external fixation was always used as a DCO technique. It is possible that external fixation was used as a definitive fracture fixation procedure. In addition, documentation may have been incomplete or incorrect so that patients may have been allocated to the wrong group. This may have affected the accuracy of differentiation between the study groups. In addition, it is possible that the patient in the DCO group received a mixed treatment partly by means of ETC and DCO, as we assigned the patients to the DCO group as soon as at least one extremity and/or pelvic fracture was treated with an external fixator. But stabilising of all long bone fractures with an external fixator can be an overuse of external fixators, so the strategy of safe definitive surgery (SDS) was established, which is a dynamic synthesis of ETC and DCO depending on clinical parameters and repeated reassessments [35, 55]. Against this background, it has to be discussed whether the DCO group of our study is not actually an SDS group according to Pape and Pfeiffer [43], since in many cases both temporary fracture stabilisation and early total care were performed in combination and our study included patients from the years 2009 to 2015, and thus DCR with the repeated reassessments was certainly already established. The way we formed our groups could thus also explain why about 65% of our patients were assigned to the DCO group, even though Bläsius et al. also found a significant increase in the use of the DCO concept [5]. In their study 47.1% were treated with an external fixator. As described earlier in the chapter, the proportion of DCO increases in this study to 54.3% when conservatively treated patients are excluded as in our study.
Another limitation of our study is that we only included patients with pelvic fractures and fractures of the long bones. Patients with e.g. spinal injuries without pelvic and/or extremity injuries were not considered, although damage control procedures are described here as well [16].
The time between the patient's arrival and the treatment was not taken into account. However, this is in line with the changed approach that not all fractures have to be stabilised within 24 h after the trauma [42], even though it should be done if possible [44].
For these reasons, our study cannot provide definitive evidence for the superiority of ETC over DCO although the results appear to do so at first glance. Furthermore, terms such as ETC, DCO, EAC and SDS do not seem to be one hundred percent sharply defined. They are rather terms that are used to try to describe certain surgical and tactical strategies. Hafner et al. as well as Rondanelli et al. come to the conclusion that after the establishment of ETC and DCO as well as in the further course of EAC and SDS, patients in an initially unclear condition (borderline patients) now also can be treated as quickly as possible with an individually adapted treatment concept [20, 48].
Conclusions
There is clear evidence supporting the damage control orthopaedics approach in the management of patients. Based on the propensity score, however, our study could not show that DCO, defined in this study as early temporary fracture stabilisation with an external fixator of at least one fracture of the pelvis and/or extremity long bone fracture was superior to ETC, which we defined as early definitive fracture fixation without prior temporary stabilisation concerning typical complications such as multi-organ failure, pulmonary failure and sepsis as well as the mortality in severely injured patients. Certain parameters of polytrauma patients used in the trauma registry (Traumaregister DGU®) are more frequently associated with the use of DCO therapy.
The use of terms such as DCO and ETC helps on the one hand to describe different strategies. In everyday clinical practice, however, the different terms and strategies mentioned in this study are sometimes merged with each other in such a way that a very clear separation hardly seems possible for a retrospective analysis of registry data.
Abbreviations
- AIS:
-
Abbreviated Injury Scale
- ARDS:
-
Adult respiratory distress syndrome
- BP:
-
Blood pressure
- DCO:
-
Damage control orthopaedics
- DCR:
-
Damage control resuscitation
- DGU:
-
German Trauma Society
- ETC:
-
Early total care
- INR:
-
International Normalised Ratio
- GCS:
-
Glasgow Coma Scale
- ICU:
-
Intensive care unit
- IQR:
-
Interquartile range
- ISS:
-
Injury Severity Score
- pRBC:
-
Packed red blood cell(s)
- OR:
-
Odds ratio
- PTT:
-
Partial thromboplastin time
- SD:
-
Standard deviation
References
Bates P, Parker P, Mcfadyen I, et al. Demystifying damage control in musculoskeletal trauma. Ann R Coll Surg Engl. 2016;98:291–4.
Behrman SW, Fabian TC, Kudsk KA, et al. Improved outcome with femur fractures: early vs. delayed fixation. J Trauma. 1990;30:792–7 (discussion 797-798).
Berwin JT, Pearce O, Harries L, et al. Managing polytrauma patients. Injury. 2020;51:2091–6.
Bieler D, Paffrath T, Schmidt A, et al. Why do some trauma patients die while others survive? A matched-pair analysis based on data from Trauma Register DGU(R). Chin J Traumatol. 2020;23:224–32.
Blasius FM, Laubach M, Andruszkow H, et al. Strategies for the treatment of femoral fractures in severely injured patients: trends in over two decades from the TraumaRegister DGU((R)). Eur J Trauma Emerg Surg. 2022;48:1769–78.
Braitman LE, Rosenbaum PR. Rare outcomes, common treatments: analytic strategies using propensity scores. Ann Intern Med. 2002;137:693–5.
Charash WE, Fabian TC, Croce MA. Delayed surgical fixation of femur fractures is a risk factor for pulmonary failure independent of thoracic trauma. J Trauma. 1994;37:667–72.
D’alleyrand J-CG, O’toole RV. The evolution of damage control orthopedics: current evidence and practical applications of early appropriate care. Orthop Clin N Am. 2013;44:499–507.
Dei Giudici L, Giampaolini N, Panfighi A, et al. Orthopaedic timing in polytrauma in a second level emergency hospital. An overrated problem? Open Orthop J. 2015;9:296–302.
Dunham CM, Bosse MJ, Clancy TV, et al. Practice management guidelines for the optimal timing of long-bone fracture stabilization in polytrauma patients: the EAST Practice Management Guidelines Work Group. J Trauma-Inj Infect. 2001;50:958–67.
Feldman G, Mosheiff R, Nasrallah K, et al. Evolution of treatment of femoral shaft fracture in polytrauma: Did damage control orthopaedics improve the outcome? A retrospective study. Injury. 2021;52:1886–90.
Giannoudi M, Harwood P. Damage control resuscitation: lessons learned. Eur J Trauma Emerg Surg. 2016;42:273–82.
Giannoudis PV. Surgical priorities in damage control in polytrauma. J Bone Jt Surg Br. 2003;85:478–83.
Giannoudis PV, Giannoudi M, Stavlas P. Damage control orthopaedics: lessons learned. Injury. 2009;40(Supplement 4):S47–52.
Gonschorek O, Czermak BJ, Friedl H-P. Technik der intramedullären Stabilisierung im Rahmen der Versorgung beim Polytraumatisierten. Trauma Berufskrank. 2000;2:111–7.
Guerado E, Bertrand ML, Cano JR, et al. Damage control orthopaedics: State of the art. World J Orthop. 2019;10:1–13.
Güsgen C, Willms A, Schwab R. Damage control surgery. Trauma Berufskrank. 2021;21:147–54.
Güsgen C, Willms A, Schwab R. Damage control surgery: Bestandteil der thorakoabdominellen Notfallchirurgie. Trauma Berufskrank. 2017;19:80–7.
Haas NP, Lindner T, Bail HJ. Neues zum polytrauma. Chirurg. 2007;78:894–901.
Hafner T, Horst K, Hildebrand F. Fracture management in polytrauma. Unfallchirurgie (Heidelb). 2022;125:559–67.
Harvin JA, Harvin WH, Camp E, et al. Early femur fracture fixation is associated with a reduction in pulmonary complications and hospital charges: a decade of experience with 1,376 diaphyseal femur fractures. J Trauma Acute Care Surg. 2012;73:1442–8 (discussion 1448-1449).
Harvin JA, Kao LS, Liang MK, et al. Decreasing the use of damage control laparotomy in trauma: a quality improvement project. J Am Coll Surg. 2017;225:200–9.
Harwood PJM, Giannoudis PV, Van Griensven M, et al. Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma Inj Infect. 2005;58:446–54.
Hildebrand F, Frink M, Mommsen P, et al. Die damage-control-strategie. Trauma Berufskrankh. 2010;12:475–9.
Hogel F, Gerlach UV, Sudkamp NP, et al. Pulmonary fat embolism after reamed and unreamed nailing of femoral fractures. Injury. 2010;41:1317–22.
Horst K, Andruszkow H, Weber CD, et al. Surgical treatment strategies in pediatric trauma patients: ETC vs. DCO-an analysis of 316 pediatric trauma patients from the TraumaRegister DGU((R)). Eur J Trauma Emerg Surg. 2019;45:801–8.
Kobbe P, Micansky F, Lichte P, et al. Increased morbidity and mortality after bilateral femoral shaft fractures: Myth or reality in the era of damage control? Injury. 2013;44:221–5.
Kuhmola A, Simons T, Handolin L, et al. Surgical strategy for femoral shaft fractures in severely injured patients: A 13-year experience from a tertiary trauma centre. Injury. 2021;52:956–60.
Kuss O, Blettner M, Börgermann J. Propensity Scoreeine alternative. Methode zur Analyse von Therapieeffekten. Dtsch Arztebl Int. 2016;113:597–603.
Lalani N, Jimenez RB, Yeap B. Understanding propensity score analyses. Int J Radiat Oncol Biol Phys. 2020;107:404–7.
Lefering R. Strategies for comparative analyses of registry data. Injury. 2014;45(Suppl 3):S83-88.
Leibner E, Andreae M, Galvagno SM, et al. Damage control resuscitation. Clin Exp Emerg Med. 2020;7:5–13.
Liu XY, Jiang M, Yi CL, et al. Early intramedullary nailing for femoral fractures in patients with severe thoracic trauma: a systemic review and meta-analysis. Chin J Traumatol. 2016;19:160–3.
Moore TA, Simske NM, Vallier HA. Fracture fixation in the polytrauma patient: markers that matter. Injury. 2020;51(Suppl 2):S10–4.
Nauth A, Hildebrand F, Vallier H, et al. Polytrauma: update on basic science and clinical evidence. OTA Int. 2021;4: e116.
Nicholas B, Toth L, Van Wessem K, et al. Borderline femur fracture patients: early total care or damage control orthopaedics? ANZ J Surg. 2011;81:148–53.
Nicola R. Early total care versus damage control: current concepts in the orthopedic care of polytrauma patients. Int Sch Res Not. 2013. https://doi.org/10.1155/2013/329452.
Pape H-C, Hildebrand F, Pertschy S, et al. Changes in the management of femoral shaft fractures in polytrauma patients: from early total care to damage control orthopedic surgery. J Trauma. 2002;53:452–61 (discussion 461-462).
Pape H-C, Lefering R, Butcher N, et al. The definition of polytrauma revisited: an international consensus process and proposal of the new “Berlin definition.” J Trauma Acute Care Surg. 2014;77:780–6.
Pape H-C, Rixen D, Morley J, et al. Impact of the method of initial stabilization for femoral shaft fractures in patients with multiple injuries at risk for complications (borderline patients). Ann Surg. 2007;246:491–501.
Pape HC, Giannoudis P, Krettek C. The timing of fracture treatment in polytrauma patients: relevance of damage control orthopedic surgery. Am J Surg. 2002;183:622–9.
Pape HC, Halvachizadeh S, Leenen L, et al. Timing of major fracture care in polytrauma patients: an update on principles, parameters and strategies for 2020. Injury. 2019;50:1656–70.
Pape HC, Pfeifer R. Safe definitive orthopaedic surgery (SDS): repeated assessment for tapered application of Early Definitive Care and Damage Control? An inclusive view of recent advances in polytrauma management. Injury. 2015;46:1–3.
Pfeifer R, Kalbas Y, Coimbra R, et al. Indications and interventions of damage control orthopedic surgeries: an expert opinion survey. Eur J Trauma Emerg Surg. 2021;47:2081–92.
Rixen D, Grass G, Sauerland S, et al. Evaluation of criteria for temporary external fixation in risk-adapted damage control orthopedic surgery of femur shaft fractures in multiple trauma patients: “evidence-based medicine” versus “reality” in the trauma registry of the German Trauma Society. J Trauma. 2005;59:1375–94.
Rixen D, Steinhausen E, Sauerland S, et al. Randomized, controlled, two-arm, interventional, multicenter study on risk-adapted damage control orthopedic surgery of femur shaft fractures in multiple-trauma patients. Trials. 2016;17:47.
Rixen D, Steinhausen E, Sauerland S, et al. Protocol for a randomized controlled trial on risk adapted damage control orthopedic surgery of femur shaft fractures in multiple trauma patients. Trials. 2009;10:72.
Rondanelli AM, Gomez-Sierra MA, Ossa AA, et al. Damage control in orthopaedical and traumatology. Colomb Med (Cali). 2021;52: e4184802.
Rotondo MF, Schwab CW, Mcgonigal MD, et al. “Damage control”: an approach for improved survival in exsanguinating penetrating abdominal injury. J Trauma. 1993;35:375–82 (discussion 382-383).
Santolini E, Stella M, Divano S, et al. Optimum timing of conversion from DCO to definitive fixation in closed fractures of the lower limb: When and how? Injury. 2020. https://doi.org/10.1016/j.injury.2020.09.021.
Scalea T. What’s new in trauma in the past 10 years. Int Anesthesiol Clin Summer. 2002;40:1–17.
Steinhausen E, Lefering R, Tjardes T, et al. A risk-adapted approach is beneficial in the management of bilateral femoral shaft fractures in multiple trauma patients: an analysis based on the trauma registry of the German Trauma Society. J Trauma Acute Care Surg. 2014;76:1288–93.
Stinner DJ, Edwards D. Surgical Management of Musculoskeletal Trauma. Surg Clin N Am. 2017;97:1119–31.
Tuttle MS, Smith WR, Williams AE, et al. Safety and efficacy of damage control external fixation versus early definitive stabilization for femoral shaft fractures in the multiple-injured patient. J Trauma. 2009;67:602–5.
Volpin G, Pfeifer R, Saveski J, et al. Damage control orthopaedics in polytraumatized patients- current concepts. J Clin Orthop Trauma. 2021;12:72–82.
Wenda K, Runkel M. Systemic complications in intramedullary nailing. Orthopade. 1996;25:292–9.
Willms A, Gusgen C, Schwab R, et al. Status quo of the use of DCS concepts and outcome with focus on blunt abdominal trauma: a registry-based analysis from the TraumaRegister DGU(R). Langenbecks Arch Surg. 2022;407:805–17.
Yamamoto R, Udagawa K, Nishida Y, et al. Damage control orthopedics and decreased in-hospital mortality: A nationwide study. Injury. 2019;50:2240–6.
Funding
Open Access funding enabled and organized by Projekt DEAL. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript. No funds, grants or other support was received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
von Lübken, F., Prause, S., Lang, P. et al. Early total care or damage control orthopaedics for major fractures ? Results of propensity score matching for early definitive versus early temporary fixation based on data from the trauma registry of the German Trauma Society (TraumaRegister DGU®). Eur J Trauma Emerg Surg 49, 1933–1946 (2023). https://doi.org/10.1007/s00068-022-02215-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-022-02215-3