
Abstract
Purpose
The risk of death after traumatic injury in developed trauma systems is at an all-time low. Among ‘major trauma’ patients (injury severity score, ISS > 15), the risk of dying is less than 10%. This group contains critical polytrauma patients (ISS 50–75), with high risks of death. We hypothesized that the reduction in trauma mortality was driven by reduction in moderate injury severity and that death from critical polytrauma remained persistently high.
Methods
A 20-year retrospective analysis ending December 2021 of a Level-1 trauma center’s registry was performed on all trauma patients admitted with ISS > 15. Patients’ demographics, injury severity and outcomes were collected. Multivariate logistic regression analysis was performed. Mortality was examined for the entire study group and separately for the subset of critical polytrauma patients (ISS 50–75).
Results
A total of 8462 severely injured (ISS > 15) trauma patients were identified during the 20-year period. Of these 238 (2.8%) were critical polytrauma patients (ISS 50–75). ISS > 15 mortality decreased from 11.3 to 9.4% over the study period (Adjusted OR 0.98, 0.97–0.99). ISS 50–75 mortality did not change significantly (46.2–60.0%), adjusted OR 0.96, 0.92–1.00).
Conclusion
The improvement in trauma mortality over the past 20 years has not been experienced equally. The ISS50-75 critical polytrauma mortality is a practical group to capture. It could be a group for deeper study and reporting to drive improvement.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Background
The outcomes of major trauma patients have continued to improve since organized trauma care began [1, 2]. For practical and statistical reasons, the major trauma population has often been described as an injury severity score (ISS) of greater than 15 [3, 4]. Outcome measures in trauma care span crude mortality rate to detailed functional outcomes [2, 5, 6]. Developed trauma systems now routinely report very low mortality rates in major trauma, which definition in some countries extended to include ISS > 12 [7].
ISS, the sum of three squared numbers, is not a continuous scale and mortality does not rise monotonically throughout the spectrum of ISS but with a series of stepwise increases. This yields natural groups with similar mortality [4]. These subgroups allow for comparison between systems [8]. Although in few studies, ISS 50–75 has been demonstrated as a potential practical group of for monitoring the most critically injured patients [4, 8], a small proportion of the overall major trauma population, whose outcomes may be obscured improvements in outcomes of less severely injured patients. By definition, these groups, apart from some non-survivable single system injuries with ISS of 75, uniformly consist of poly-trauma patients with Abbreviated Injury Scale greater than two in at least two body regions [4]. We hypothesized that the reduction in mortality rate since the organization of the trauma service in a Level-1 trauma center’s population was driven by improvements in the less severely injured population, with a persistently high mortality rate among ISS 50–75 poly-trauma group.
Methods
The John Hunter Hospital is a level 1 trauma center located in New South Wales (NSW), Australia. It is the highest volume trauma center in the state of NSW. It cared for 513 ISS > 15 major trauma patients in 2019 [9]. The trauma center is the referral center for major trauma for approximately 1.1 million people. Since 2002 all patients with ISS > 15 have been collected in a trauma registry.
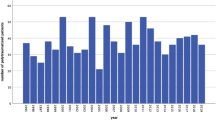
Data were extracted from the prospectively maintained trauma database for the entire period between January 1, 2002 and December 31, 2021. Data extracted were age, sex, blunt or penetrating mechanism, presentation type (transfer vs direct), ISS, date of injury and in-hospital mortality. Ethical approval was granted by the Hunter New England Human Research Ethics Committee with reference AU202105-03 (see Fig. 1).

Number of and mortality of ISS > 15 patients over the study period
Data were analyzed using Stata 17 (StataCorp. 2022. Stata Statistical Software: Release 17. College Station, TX: StataCorp LP.). Continuous data were presented as median (IQR) and categorical data as counts and proportions. Comparison between groups was with the Kruskal–Wallis test. Binary logistic regression was used to control for age, sex, injury mechanism, and interhospital transfer, and to measure interactions between variables. They were reported as odds ratios and 95% confidence intervals. Male sex was used as the reference group in the regression. Age was inserted as an indicator categorical variable, given its non-linear influence on risk of death with a threshold of 55 years of age in keeping with TRISS. Date of injury was divided into calendar year and inserted into the model as an ordinal variable over the study period. Mechanism of injury and transfer status were also included as indicator variables. Proportions were compared using Fisher’s exact test. Statistical significance was set at 5%. We used the STROBE cohort checklist when writing the manuscript [10].

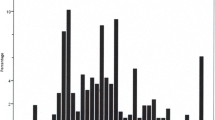
Number of and mortality of ISS 50–75 patients over the study period
Results
There were 8,462 patients with ISS > 15 (median ISS: 20, IQR: 17–26) during the 20-year study period of whom were 72.1% male and 27.8% were female with an overall mortality of 11.1%. There were 238 patients with an ISS 50–75 (12 patients/year, 2.8% of the total ISS > 15 population, median ISS: 57, IQR: 50–66, mean ISS: 58) of whom 74.3% were male and 25.6 were female with a mortality of 51.7% (Table 1). The mean age increased over the study period (0.5 years/year, p < 0.001). The overall ISS > 15 mortality rate improved over the study period (adjusted OR 0.98, 0.97–0.99) (Fig. 1). The mortality rate in the ISS 50–75 group did not improve significantly (adjusted OR 0.96, 0.91–1.00) (Fig. 2). Age was a significant confounder for overall mortality (adjusted OR 2.44, 2.12–2.81) but was not significant for the ISS 50–75 group (adjusted OR 1.15, 0.64–2.07) (Table 2).
Discussion
We hypothesized that despite our proven improvement in trauma system performance, that ISS 50–75 polytrauma mortality would remain unchanged. Overall trauma mortality fell over the study period with no significant change in ISS 50–75 mortality. This supports our hypothesis that the fall in overall trauma mortality is predominantly driven by the improvement in outcomes of less severely injured patients. We demonstrated the critical trauma population is small enough to be comprehensively audit and reflect on (one patient per month, on average) (see Table 2).
The risk of death from injury continues to fall in developed trauma systems. Quality improvement methodology in trauma uses two disparate methodologies. Preventable mortality review examines death that were statistically predicted to survive [11]. Epidemiological reporting relies on the total event rate, in this case mortality, being a measure of system performance [12]. For the latter to allow benchmarking, standardized reporting must occur. The use of a universally collected scoring system (AIS and thus ISS) allows for extraction of large data sets from long time period without retrospectively collecting physiological parameters, such as in the Revised Trauma Score (RTS) [13] and Trauma Injury Severity score (TRISS) [14]. It also avoids the complication of relying on admission GCS and respiratory rate in a population commonly intubated, sedated, and ventilated in the pre-hospital phase [15].
Reporting of trauma system performance within the ISS 50–75 poly-trauma population is sporadic. At our state level, ISS 40–75 is reported [9]. ISS 40–75 is a much larger more heterogeneous group; there is a 20% reduction in mortality rate between ISS 40 and ISS 50 (Table 3) [8]. Our 20-year ISS 50–75 mortality of 53% lags behind retrospective data from Wurm et al. with a reported mortality rate of 36% (95% CI 26–46) over the period of 2000 to 2005 among 88 patient with an ISS of 50–75 [16]. This is higher performance during a much shorter study period compared to our data. Their group was slightly less severely injured with a mean ISS of 56.8 vs 59.0, and having most of their patients (75%) in the less severely injured, ISS 50–60 range. Candefjord et al. reported ISS 50–75 as a relevant group for comparison but did not report raw mortality [17]. We reconfirmed that age is a significant cofactor in overall ISS > 15 mortality; however, this is driven by less severely injured patients with the ISS 50–75 group suffering no significant influence from age. This could make ISS 50–75 mortality a robust and practical comparator of trauma centers rather that requiring the reporting of risk-adjusted mortality which requires granular data analysis.
This study was performed at a single center, albeit the largest volume in the state. Despite this, there was still considerable variability given the smaller number of cases. This may limit the usefulness of ISS 50–75 mortality as a reporting measure for trauma centers and limits the statistical power of the subgroup. There may be a true improvement in this group that has not been detected due to the high variability year-on-year, and small number of these severely injured patients over time. The injuries were almost exclusively blunt trauma given the low rates of stabbings and firearm-related injuries in Australia [18]. The performance of pre-hospital systems was incompletely measured with no ability to capture pre-hospital deaths in this dataset; this has been studied previously by our group. In this one year prospective study of all traumatic deaths, a majority of deaths occurred in the pre-hospital setting, most of these deaths were from central nervous system causes [19]. Centers with shorter pre-hospital times may experience more in-hospital deaths, biasing their ISS 50–75 results. This dataset is limited in its lack of physiological and early treatment data, and comprehensive adjustment for medical comorbidities as confounders for mortality. Outcome data are limited to only in-hospital mortality, rather than more nuanced measures of functional outcome [20].
The ‘critical polytrauma’ group represents the most severely injured patients a trauma system cares for. Despite representing only 3% of all major trauma patients, they represent 11% of all major trauma deaths. The sample is practical to capture with approximately 11 patients per year in a single trauma center—representing a group that could be extensively studied to identify opportunities for improvement in a mature trauma system. The reduction in mortality in the major trauma population is disproportionately driven by a reduction in less severely injured patients. Critical polytrauma mortality did not improve significantly, despite an overall improvement in mortality.
References
Jenkins DH, Winchell RJ, Coimbra R, Rotondo MF, Weireter LJ, Bulger EM, et al. Position statement of the american college of surgeons committee on trauma on the National Academies of Sciences, Engineering and Medicine Report, A National Trauma Care System: Integrating Military and Civilian Trauma Systems to Achieve Zero Preventable Deaths After Injury. J Trauma Acute Care Surg. 2016;81(5):819–23.
Coccolini F, Kluger Y, Moore EE, Maier RV, Coimbra R, Ordoñez C, et al. Trauma quality indicators: internationally approved core factors for trauma management quality evaluation. World J Emerg Surg. 2021;16(1):1–10.
Roden-Foreman JW, Rapier NR, Foreman ML, Zagel AL, Sexton KW, Beck WC, et al. Rethinking the definition of major trauma: The need for trauma intervention outperforms Injury Severity Score and Revised Trauma Score in 38 adult and pediatric trauma centers. J Trauma Acute Care Surg. 2019;87(3):658–65.
Copes WS, Champion HR, Sacco WJ, Lawnick MM, Keast SL, Bain LW. The injury severity score revisited. J Trauma. 1988;28(1):69–77.
Wanner JP, deRoon-Cassini T, Kodadek L, Brasel K. Development of a trauma-specific quality-of-life measurement. J Trauma Acute Care Surg. 2015;79(2):275–81.
Livingston DH, La Bagnara S, Sieck D, Yonclas P, Castellano C, Cho C, et al. The Center for Trauma Survivorship: Addressing the great unmet need for posttrauma center care. J Trauma and Acute Care Surg. 2020;89(5):940–6.
Gomez D, Sarrami P, Singh H, Balogh ZJ, Dinh M, Hsu J. External benchmarking of trauma services in New South Wales: Risk-adjusted mortality after moderate to severe injury from 2012 to 2016. Injury. 2019;50(1):178–85.
Rozenfeld M, Radomislensky I, Freedman L, Givon A, Novikov I, Peleg K. ISS groups: are we speaking the same language? Inj Prev. 2014;20(5):330–5.
Institute of Trauma and Injury Management. Major Trauma in NSW:2018–19 2020. https://aci.health.nsw.gov.au/__data/assets/pdf_file/0018/601092/Major-Trauma-in-NSW_-2018-19.-A-Report-from-the-NSW-Trauma-Registry-final.pdf. Accessed 11 July 2021.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10): e296.
MacKenzie EJ. Review of evidence regarding trauma system effectiveness resulting from panel studies. J Trauma. 1999;47(3 Suppl):S34-41.
Chiara O, Cimbanassi S, Pitidis A, Vesconi S. Preventable trauma deaths: from panel review to population based-studies. World J Emerg Surg. 2006;1:12.
Champion HR, Sacco WJ, Copes WS, Gann DS, Gennarelli TA, Flanagan ME. A revision of the Trauma Score. J Trauma. 1989;29(5):623–9.
Champion HR, Copes WS, Sacco WJ, Lawnick MM, Keast SL, Bain LW Jr, et al. The Major Trauma Outcome Study: establishing national norms for trauma care. J Trauma. 1990;30(11):1356–65.
Bendinelli C, Ku D, King KL, Nebauer S, Balogh ZJ. Trauma patients with prehospital Glasgow Coma Scale less than nine: not a homogenous group. Eur J Trauma Emerg Surg. 2020;46(4):873–8.
Wurm S, Rose M, von Ruden C, Woltmann A, Buhren V. Severe polytrauma with an ISS >/= 50. Z Orthop Unfall. 2012;150(3):296–301.
Candefjord S, Asker L, Caragounis EC. Mortality of trauma patients treated at trauma centers compared to non-trauma centers in Sweden: a retrospective study. Eur J Trauma Emerg Surg. 2020;48:525–36.
Warren K-RJ, Morrey C, Oppy A, Pirpiris M, Balogh ZJ. The overview of the Australian trauma system. OTA Int. 2019;2(S1):e018.
Evans JA, van Wessem KJ, McDougall D, Lee KA, Lyons T, Balogh ZJ. Epidemiology of traumatic deaths: comprehensive population-based assessment. World J Surg. 2010;34(1):158–63.
Sakran JV, Ezzeddine H, Schwab CW, Bonne S, Brasel KJ, Burd RS, et al. Proceedings from the consensus conference on trauma patient-reported outcome measures. J Am Coll Surg. 2020;230(5):819–35.
Acknowledgements
We thank Natasha Weaver for her invaluable statistical advice.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. BMH is a PhD student at the University of Newcastle and a recipient of the Australian Orthopaedic Association PhD pathway scholarship.
Author information
Authors and Affiliations
Contributions
BMH: literature search, study design, data collection, data analysis, data interpretation, writing. NE: literature search, study design, critical revision. KLK: study design, data collection. ZJB: conceptualization, supervision, study design, data interpretation, critical revision.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hardy, B.M., Enninghorst, N., King, K.L. et al. The most critically injured polytrauma patient mortality: should it be a measurement of trauma system performance?. Eur J Trauma Emerg Surg 50, 115–119 (2024). https://doi.org/10.1007/s00068-022-02073-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-022-02073-z