
Avoid common mistakes on your manuscript.
Introduction
One of the dreams of all medical chemists is to create molecules that will help mankind. The same is true for physician scientists who want those molecules to help the patient sitting in front of them. The authors of this editorial have had the privilege of working together with the medical chemist to whom this special issue is dedicated, Dr. Laurence Hurley (Fig. 1A, B).

Dr. Laurence Hurley – Colleague and Mentor. A: Dr. Hurley being welcomed by Dr. Von Hoff to the Arizona Cancer Center circa 2000. B: Dr. Hurley and his trainees (from left) Haiyong Han, Dong-Fang Shi, Vijay Gokhale, Laurence Hurley, Steve Warner
We are very fortunate to have known and worked with Dr. Hurley. He has trained so many medical chemists and motivated so many physician scientists. In the many years of working together in translational research plus the clinical experience of conducting Phase I clinical trials for more than 400 agents, these are some “enlightenments” we would like to pass on to the next generation of medical chemists. We have always been sure that Dr. Hurley was working to make a difference for patients as well as working in memory of his father who passed away from pancreatic cancer in 1975 (Fig. 2). Dr. Hurley often mentioned his father’s last words when he saw him “Laurence, this is a terrible disease, and you need to do something about it”. Dr. Hurley and other medicinal chemists like him and physician scientists are doing just that.

Harold Hurley, Dr. Laurence Hurley’s father
As we work together aiming to discover effective molecule(s), we are always seeking the best method for picking a “winner” that will be most helpful to patients. Table 1 details the time commitment for a patient to participate in a Phase I clinical trial. If one estimates a patient has an expected lifespan of 12 weeks, an average Phase I trial which requires on average 400 hours of a patient’s time will consume almost 20% of their remaining lifetime (if that new therapy does not work for that patient). Therefore, we should do everything possible to ensure a patient has the best possible chance of receiving an effective agent(s).
Methods
The estimates described here are based on experience of having taken more than 400 new agents into Phase I clinical trials, all of which were based on what was believed at the time as the best possible science. Of course, not all were eventually approved by the FDA, but many were. What have we learned that distinguishes agents that were approved from those not approved? And what does one look for to increase the chances that a new agent will eventually work for patients?
Experience-based findings
Here is a checklist of what one should look for to increase the chance that a newly discovered agent will have the greatest chance of success in the clinic.
-
A.
New Mechanism of Action Based on the Best Possible Science.
Since the majority of patients with cancer walking into an oncology clinic specializing in new therapeutics these days have a resistant tumor, it of course makes sense that a new mechanism of action is the very best way to address that resistance (e.g. avoid potential cross resistance). So one should always look for a compound produced by the medical chemist that has a purported new mechanism of action (MOA). One can easily recognize that agents with new MOA’s can change the world for patients––such as imatinib did for patients with CML [1] and PD-1 or CTLA-4 inhibitors did for patients with so many different types of cancer [2, 3]. However, one cannot take for granted that all agents with a new MOA based on published new science are appropriate to move forward into a clinical trial. Multiple authors have recently warned all of us that perhaps only 16–25% of new therapeutic science is reproducible [4, 5]. Of course, there are a multitude of reasons for some of lack of reproducibility (different cell lines, etc.). But these data give physician scientists great pause as to what they should take into the clinic!
-
B.
New Formulation of an Established Agent.
In the early days of new formulations of already approved agents, there was a great deal of skepticism that just a change in formulation could make a difference. However, the science of agent formulation such as liposomal doxorubicin [6] and the nanoparticle albumin bound paclitaxel (now referred to in the package insert as “paclitaxel protein-bound particle for injectable suspension”) [7] have certainly documented that new formulations of established agents have an excellent chance of success [if that formulation is shown to be superior in pre-clinical models (see below)].
-
C.
Tumor Growth Curves Are Fine, But Tumor Regression and 45-day Survivors Are the Best.
A typical tumor growth curve usually published for a potential new anti-cancer agent is shown in Fig. 3. Just think of how many times a clinical investigator sees this type of curve, takes the new agent into the clinic and the clinical trial result(s) are negative [8].
Fig. 3 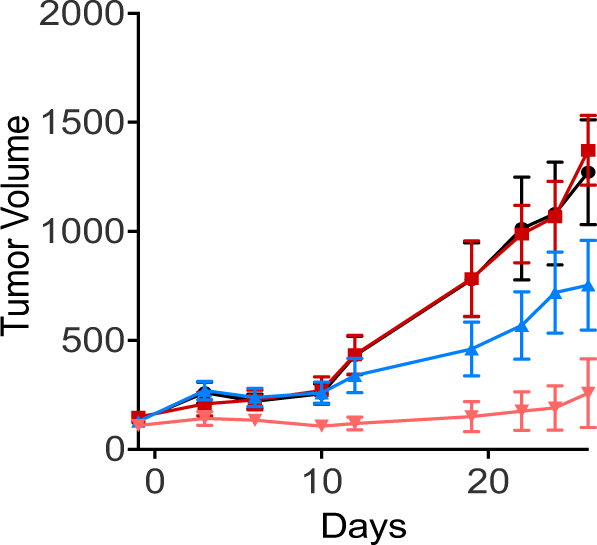
Typical growth curve often shown for a new anticancer agent. Will this be a strong predictor for success in the clinic?
This is particularly true if the pre-clinical team initiates studies with tumors ≤100 mm3 in volume. There are hundreds and hundreds of examples of these situations. Based on multiple years of translational research to bedside experience, what are the in vivo parameters most valuable in predicting success in the clinic?
In our experience, tumor regression in an animal model is a very good prognostic sign for the clinical activity of a compound (if that compound is a cytotoxic agent). That is because cytotoxic agents are generally evaluated clinically by looking for tumor shrinkage––and why not also demand that in an animal model? If the compound is not a cytotoxic agent, what else is a valuable prognostic factor for success in the clinic?
In 1983 Staquet and colleagues reviewed all the National Cancer Institute’s screening programs (on P388 leukemia and B16 melanoma) to determine what was the best prognostic factor for essential success in the clinic [9]. They found that the percentage of animals that were ≥45-day survivors in the B16 melanoma system was the best prognostic factor for activity in the clinic. In our continued use of that parameter over the years, we too have found it to be most predictive [10]. Figure 4 details an example of such a long-term survivor’s curve.
Fig. 4 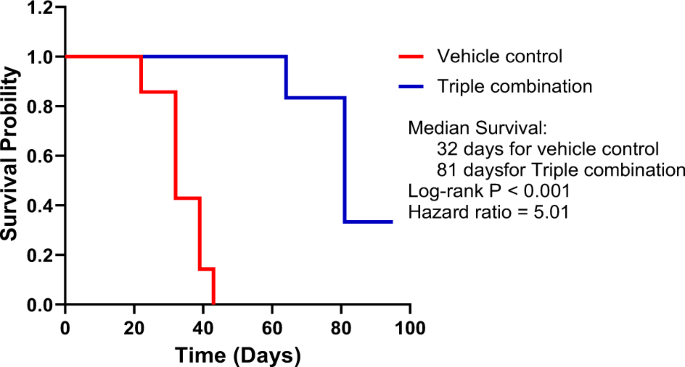
An example of significant improvement in animal survival (≥45 days) by a chemotherapy regimen. A combination of three chemotherapeutic drugs (Triple combination), nab-paclitaxel + gemcitabine + cisplatin, was tested in a patient-derived xenograft model for pancreatic cancer. This same combination showed high response rate (71%) and significant improvement in overall survival in a Phase II clinical trial in patients with advanced pancreatic cancer [11]
In Fig. 4, one can see that the experiment has been carried out to past 100 days with a substantial percentage of long term (≥45 day) survivors. This is an excellent prognostic indicator that the new agent or new combination of agents will have activity in the clinic [11].
It is important to note that in speaking with pre-clinical scientists and veterinarians they acknowledge the need to sacrifice the animals when their tumors reached a specific size (e.g., 2000 mm3), which usually happens first in control animals. However, there is no reason that the treated animals cannot be followed for survival if their tumors are still within the size parameters. Obtaining the percent of animals (with smaller tumors) that are ≥45-day survivors is very important.
-
D.
Clinical Champion.
A medicinal chemist should have a physician scientist partner. It should be one who understands the medicinal chemist’s evidence and who is an excellent teacher so he/she can give the chemist a clinical trial design which maximizes the possibility the chemist’s new molecule can eventually produce clinical activity. The clinician scientist should strive to provide the best possible design that will help patients.


Conclusion
Although the information presented above is largely experience-based, we hope these comments are helpful to the medicinal chemists (many trained by Dr. Hurley) who are laboring at the research bench to help patients. Figure 5 summarizes the points in a pyramid of success for a medicinal chemist’s best chance to have their compound/invention help patients.

Pyramid for success of a medicinal chemist’s anticancer compound/invention having significance clinical activity (approval by the FDA)
References
Druker BJ, Guilhot F, O’Brien SG, Gathmann I, Kantarjian H, Gattermann N, et al. Five-year follow-up of patients receiving imatinib for chronic myeloid leukemia. N Engl J Med. 2006;355:2408–17. https://doi.org/10.1056/NEJMoa062867.
Korman AJ, Peggs KS, Allison JP. Checkpoint blockade in cancer immunotherapy. Adv Immunol. 2006;90:297–339. https://doi.org/10.1016/s0065-2776(06)90008-x.
Peggs KS, Quezada SA, Korman AJ, Allison JP. Principles and use of anti-CTLA4 antibody in human cancer immunotherapy. Curr Opin Immunol. 2006;18:206–13. https://doi.org/10.1016/j.coi.2006.01.011.
Begley CG, Ellis LM. Raise standards for preclinical cancer research. Nature. 2012;483:531–3. https://doi.org/10.1038/483531a.
Prinz F, Schlange T, Asadullah K. Believe it or not: how much can we rely on published data on potential drug targets? Nat Rev Drug Disco. 2011;10:712 https://doi.org/10.1038/nrd3439-c1.
Muggia FM, Hainsworth JD, Jeffers S, Miller P, Groshen S, Tan M, et al. Phase II study of liposomal doxorubicin in refractory ovarian cancer: antitumor activity and toxicity modification by liposomal encapsulation. J Clin Oncol. 1997;15:987–93. https://doi.org/10.1200/jco.1997.15.3.987.
Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369:1691–703. https://doi.org/10.1056/NEJMoa1304369.
Pan E, Bogumil D, Cortessis V, Yu S, Nieva J. A systematic review of the efficacy of preclinical models of lung cancer drugs. Front Oncol. 2020;10:591 https://doi.org/10.3389/fonc.2020.00591.
Staquet MJ, Byar DP, Green SB, Rozencweig M. Clinical predictivity of transplantable tumor systems in the selection of new drugs for solid tumors: rationale for a three-stage strategy. Cancer Treat Rep. 1983;67:753–65.
Von Hoff DD Clinical Trial Designs for Approval of New Anticancer Agents. In: Figg WD, McLeod HL, editors. Handbook of Anticancer Pharmacokinetics and Pharmacodynamics. Totowa, NJ: Humana Press; 2004. p. 579–92.
Jameson GS, Borazanci E, Babiker HM, Poplin E, Niewiarowska AA, Gordon MS, et al. Response rate following albumin-bound paclitaxel plus gemcitabine plus cisplatin treatment among patients with advanced pancreatic cancer: a phase 1b/2 pilot clinical trial. JAMA Oncol. 2020;6:125–32. https://doi.org/10.1001/jamaoncol.2019.3394.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Von Hoff, D.D., Han, H. Useful preclinical clues that a proposed new therapy would work in the clinic: to make a medicinal chemist’s dreams come true. Med Chem Res 31, 1064–1067 (2022). https://doi.org/10.1007/s00044-022-02906-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00044-022-02906-x