
Abstract
Long non-coding RNAs (lncRNAs) have been gaining importance in the field of cancer research in recent years. PRNCR1 (prostate cancer-associated non-coding RNA1) is a 12.7 kb, intron-less lncRNA found to play an oncogenic role in malignancy of diverse organs including prostate, breast, lung, oral cavity, colon and rectum. Single-nucleotide polymorphisms (SNPs) of PRNCR1 locus have been found to be associated with cancer susceptibility in different populations. In this review, an attempt has been made for the first time to summarize all sorts of available data on PRNCR1 to date from relevant databases (GeneCard, LncExpDB, Ensembl genome browser, and PubMed). As functional roles of PRNCR1, miRNA (microRNA) sponging was mostly highlighted in the pathogenesis of different cancer; in addition, an association of the lncRNA with chromatin-modifying complex to enhance androgen receptor-mediated gene transcription was reported in prostate cancer. Diagnostic and prognostic importance of PRNCR1 was found in some malignancies suggesting potency of the lncRNA to serve as a clinical biomarker. For PRNCR1 SNPs, although cancer susceptibility of the risk alleles/genotypes was reported in different populations, majorities of the findings were not replicated and underlying molecular mechanisms remained unexplored. Therapeutic implication of PRNCR1 was not studied well and future research may come up in this direction for intervening novel strategies to fight against cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Recent advances in RNA-seq data analysis reveal that around 80–85% of the human genome is actively transcribed and majority of the transcripts are non-coding RNAs (ncRNAs) (Djebali et al. 2012; Hangauer et al. 2013). Long non-coding RNAs (lncRNAs) have a standard length of > 200 nucleotides (Adhikary et al. 2019) and are similar to mRNAs in many aspects, i.e., lncRNAs like mRNAs are transcribed by RNA polymerase-II, have exon structures interrupted by introns, undergo post-transcriptional modifications like 5’capping, 3’polyadenylation, splicing and exhibit cell-type-specific, tissue-specific and developmental stage-specific expression patterns (Chernikova et al. 2016; Sun et al. 2018; Liu et al. 2016; Derrien et al. 2012; Sarropoulos et al. 2019). LncRNAs also serve as vital regulators of gene expression by modulating processes like transcription, splicing, mRNA turnover, and translation (Faust et al. 2012; He et al. 2019; Martone et al. 2020). Association of lncRNAs with disease conditions including cancer has been established and, oncogenic and tumor-suppressive lncRNAs have been designated in human malignancies (He et al. 2019). Therefore, genes encoding lncRNAs should be studied with equal priority to that of protein-coding genes for exploring molecular pathogenesis of associated disease conditions.
Prostate cancer-associated non-coding RNA1 (PRNCR1) is an intron-less lncRNA known to play oncogenic role in prostate cancer (Chung et al. 2011). The role of PRNCR1 has also been reported in the malignancy of other organs (Pang et al. 2019; Cheng et al. 2018) and in addition, single-nucleotide polymorphisms (SNPs) of the gene have been found to be associated with cancer susceptibilities (Sattarifard et al. 2017; Li et al. 2013, 2016a). Thus, PRNCR1 seems to be an important lncRNA to be explored in more detail in different aspects of human malignancy and for this, a review work summarizing the available data will be helpful which is lacking altogether to the best of our knowledge. On the aforesaid backdrop, the present study attempts to summarize available information of PRNCR1 from published literature with special emphasis on its role in the pathogenesis of human cancers and its potential diagnostic, prognostic, as well as therapeutic values for associated disease conditions.
Genomic locus and biogenesis
PRNCR1 is localized in chromosomal 8q24.21 region (GRCh38/hg38) which is a part of 8q24 gene desert of human genome (Chung et al. 2011; Huppi et al. 2012). Besides PRNCR1, 8q24 also contains other lncRNA genes like prostate cancer-associated transcript 1 (PCAT1), cancer-associated region long non-coding RNA-5 (CARLo-5), plasmacytoma variant translocation-1 (PVT1), etc. and protein-coding genes like POU Class 5 Homeobox 1B (POU5F1B) and MYC (Huppi et al. 2012; Kim et al. 2014). Chromosome 8q24 was found to undergo frequent genetic alterations like amplification, deletion, translocation and viral-integration in different cancers (Huppi et al. 2012). In cervical cancer, the 8q24.21 region harboring PRNCR1 locus was reported as a preferred site for integration of the human papillomavirus (HPV) genome (Bodelon et al, 2016). PRNCR1 gene is intron-less, consists of a single exon of approximately 12.7 kb and occupies a position overlapping with PCAT1 locus in a sense direction (GRCh38.p13) (Fig. 1). In addition to PRNCR1, CARLo-5 and POU5F1B loci also overlap with PCAT1 locus in antisense and sense directions, respectively. Total 4 transcript variants of PRNCR1 have been reported with following transcript IDs; URS00009C6066_9606 (12,727 nucleotides), URS0000759F81_9606 (12,722 nucleotides), URS0000E9A964_9606 (12,722 nucleotides) and URS0001BCD7EB_9606 (12,721 nucleotides) (GeneCards, http://www.genecards.org). In addition to minute difference in length, PRNCR1 transcripts show variation at 5’ and 3’ end sequences. PRNCR1 promoter is not well defined although the gene locus has five enhancer elements having binding sites for transcription factors (GeneCards, http://www.genecards.org). Thus, transcriptional regulation of PRNCR1 is not well characterized. However, the chromosomal 8q24 region harbors MYC super-enhancer elements that involve long-range transcriptional regulation of the host gene as well as of adjacent loci (Lancho and Herranz 2018). Long-range physical interaction of MYC enhancer was established with the promoter of CARLo-5 locus leading to transcriptional up-regulation of the latter (Kim et al. 2014); such probability for transcriptional regulation of PRNCR1 has not been tested in any investigation to date.

Schematic view of human chromosomal 8 q24.21 region harboring PCAT/PRNCR1 locus and adjacent genes loci. Exons are represented as boxes and introns as connecting lines in transcripts. TSS transcription start site, TFBS transcription factor binding site
Gene expression profile under normal and diseased conditions
Expression profile of PRNCR1 in normal body tissue of adult and developmental stages in human was downloaded from LncExpDB (https://bigd.big.ac.cn/lncexpdb) (Li et al. 2021a). PRNCR1 is expressed about ubiquitously in majority of organs of human body (Fig. 2A) (Project ID, E-MTAB-2836; source, EBI ArrayExpress), suggesting importance of the lncRNA in normal physiological functioning. In addition to endometrium, prostate and appendix, comparatively higher PRNCR1 level was also found in spleen and lymph node than other organs; this indicated an association of the lncRNA in host’s immune response which was also evident from its (PRNCR1) differential expression pattern in peripheral blood lymphocyte in response to HIV, HCV, HBV infections (GSE125686), and in primary lung epithelium in response to SARS-CoV-2 infection (GSE147507) compared to normal control (Fig. 2B). However, functional link of PRNCR1 with host’s immunity is not explored to date, although role of the lncRNA has been reported in activation of androgen receptor which is also expressed in immune cells and involved in development and regulation of innate as well as adaptive immune responses (Yang et al. 2013; Lai et al. 2012). Furthermore, a significant association of the PRNCR1 variant (rs1456315) with the susceptibility of osteoarthritis, an immune response related disease was also found in a Chinese population (Wang et al. 2018).

Summarized view on expression pattern of PRNCR1 in human body. PRNCR1 expression levels in normal tissue of different organs (A), in blood samples of normal and virus infected individuals (B), during development of 7 vital organ from early organogenesis to adulthood (C) and in blood exosomes of normal and diseased individuals (D). TPM transcript per million, HBV hepatitis B virus, HCV hepatitis C virus, HIV human immunodeficiency virus
During organogenesis, PRNCR1 level increased substantially in the embryonic cerebellum on the 10th week and in the embryonic heart between 9th and 13th weeks of gestation (Fig. 2C) (Project ID, E-MTAB-6814; source, EBI ArrayExpress) functional significance of which was not investigated. But, PRNCR1 through miRNA sponging was found to up-regulate the expression of HEY2 and CCND2 (Cheng et al. 2018; Ouyang et al. 2021) that were also reported to have involvement in the development of embryonic heart and cerebellum, respectively (Anderson et al. 2018; Leto et al. 2011). However, lncRNAs generally show cell type-specific expression patterns in tissue in connection to their specific biological function, i.e., LOC646329 was abundantly expressed in human radial glia cells but, a low overall expression level of the lncRNA was found in the neocortex tissue (Liu et al. 2016). Therefore in PRNCR1, detailed information on the expression pattern is warranted up to the cell type level in adult and embryonic tissues for more precise functional interpretation.
Apart from the body tissue/organ, PRNCR1 expression was also detected in blood exosomes of normal and diseased individuals (GSE100063, GSE100206) (Fig. 2D) and the phenomenon may have association with cell-to-cell communication process in endocrine manner.
Among diseased conditions, PRNCR1 was mostly studied in association with cancer and frequent over-expression of the lncRNA was found in malignant tumors of prostate (Chung et al. 2011), breast (Pang et al. 2019), oral cavity (Liu et al. 2021), etc. Molecular mechanisms associated with PRNCR1 over-expression remained unexplored; however, frequent amplification of the chromosomal 8q24.21 region harboring PRNCR1 locus in different malignancies (Raeder et al. 2013; Bhosale et al. 2017) might be a probable explanation. Furthermore, transcription factors like KDM1A, JUND, CEBPB and CREB1 having binding sites on PRNCR1 enhancer elements (Fig. 1) were over-expressed in malignant conditions (Kashyap et al. 2013; Elliott et al. 2019; Milde-Langosch et al. 2003; Fang et al, 2016) and hence might contribute significantly to the transcriptional up-regulation of the lncRNA gene.
Functional role of PRNCR1 in oncogenesis
Oncogenic impact of PRNCR1 was evident from its influence on dysregulation of vital cellular processes like epithelial–mesenchymal transition, proliferation, migration and so on in different human malignancies (Table 1). As potential mechanism of PRNCR1-mediated oncogenesis, androgen receptor (AR) regulated gene activation, modulation of key regulatory proteins of cell cycle progression and sponging of miRNA targeting mRNA of oncogenic function were mostly highlighted (Table 1, Fig. 3). So far, the interaction of five miRNAs with PRNCR1 was established experimentally in different human malignancies; PRNCR1 is found to harbor four binding sites for miR-326, three sites for miR-944, and one site each for miR-126-5p, miR-377, and miR-448 that (binding sites) remain scattered roughly along the length of the lncRNA (Fig. 3A).

Summarized information on functional mechanism of PRNCR1 in oncogenesis. A Schematic view showing interaction PRNCR1 with proteins and target miRNAs. B–D details of PRNCR1-mediated oncogenesis in prostate cancer, breast cancer, non-small cell lung carcinoma (NSCLC) and oral squamous cell carcinoma (OSCC). 1–6; PRNCR1-mediated expression of androgen responsive genes through chromatin modification via recruitment of DOT1L (DOT1-Like Histone Lysine Methyltransferase), PCGEM1 (Prostate Cancer Gene Expression Marker 1, an lncRNA) and PYGO2 (Pygopus Homolog). AR androgen receptor, ARE androgen response element, H3K4me3 trimethylation at 4th lysine residue of H3 histone. The cartoon symbols for the malignancies have been created with BioRender.com
Prostate cancer
PRNCR1 transcript was first cloned and characterized successfully as lncRNA in human prostate tissue and prostate cancer cell line (Chung et al. 2011). The investigators found PRNCR1 over-expression in prostate cancer (PCa) cells and prostatic intraepithelial neoplasia; furthermore, reduced PCa cell viability and simultaneously decreased androgen receptor (AR) trans-activation following knockdown of PRNCR1 strongly suggested its association in AR signaling pathway. In PCa, AR is aberrantly activated and serves as a master regulator for G1–S progression of cell cycle through inactivation of retinoblastoma protein, promoting G1 cyclin-dependent kinase activity, etc. (Balk and Knudsen 2008). According to Yang et al., PRNCR1 over-expression in prostate cancer causes significant enhancement of ligand-dependent and ligand-independent AR activation (Yang et al. 2013). From experimental evidences, the authors propose that PRNCR1 interacts with AR bound to androgen response element (ARE) and mediates its (AR) methylation via recruitment of DOT1-like histone H3K79 methyltransferase (DOT1L); prostate cancer gene expression marker 1 (PCGEM1, a lncRNA) binds to methylated AR and recruits pygopus family PHD finger 2 (PYGO2) which recognizes active chromatin mark (H3K4me3) leading to selective looping of AR-bound enhancer (ARE) with promoter of the target gene and its transcriptional activation (Fig. 3B). The authors also highlighted importance of PRNCR1 in ligand-independent aberrant activation of full length and truncated AR in castration resistant prostate cancer (CRPC); following sh-RNA mediated knock-down of PRNCR1 and also PCGEM1, they found reduced growth of CRPC cells in tumor xenograft. On contrary, Prensner et al. did not find any evidence for PRNCR1 to interact with AR in prostate cancer and therefore failed to establish this lncRNA as a component of AR signaling pathway (Prensner et al. 2014). The discrepancies might be due to differences in prostatic lesions used with respect to tumor stage, Gleason scores, ethnicity of the patients, etc. and methodological details employed by the investigators (Yang et al. 2013 and Prensner et al. 2014).
Breast cancer
In breast cancer (BC), consistent over-expression of PRNCR1 was found in primary breast tumor compared to adjacent normal tissue (Pang et al. 2019; Abdollahzadeh et al. 2020; Guo et al. 2019; Ouyang et al. 2021). PRNCR1 knockdown led to apoptosis induction and suppression of tumor associated phenotypes like proliferation, migration, invasion and epithelial to mesenchymal transition in BC cells (Pang et al. 2019). As molecular mechanism of tumorigenesis, the role of PRNCR1 in modulating functional state or expression level of some key cell cycle regulator proteins was highlighted. From the evidence of knockdown experiment in BC cell line, PRNCR1 was predicted to involve in maintenance of CHK1/2 proteins in dephosphorylated and AKT in phosphorylated forms, and thus keeping the former in inactive and the latter in active states to augment cell cycle progression (Fig. 3C). However, the candidate phosphatase and kinase serving as functional mediators of PRNCR1 activity need to be identified for better understanding of the disease pathogenesis. Very recently in BC cell line, PRNCR1 was found to bind with miR-377 competitively and up-regulate the expression of its (miRNA) natural target CCND2 (Ouyang et al. 2021); CCND2 over-expression was also correlated with aberrant activation of MEK/MAPK pathway leading to accelerated cell cycle progression and suppression of apoptosis in BC cells, and thus was speculated to contribute to the breast tumor growth. On the contrary, significantly reduced expression of CCND2 was frequently reported in primary breast tumors compared to adjacent normal tissue and promoter hyper-methylation was highlighted as a potential mechanism of gene inactivation (Fischer et al. 2002; Evron et al. 2001; Truong et al. 2015). Moreover, in another study dealing with the TCGA dataset, promoter hyper-methylation of CCND2 and associated reduced gene expression in breast tumor was found to be associated with poor patient prognosis (Hung et al. 2018). Therefore, in breast cancer, the role of CCND2 as a downstream oncogenic effector of PRNCR1 seems to be a matter of scientific debate and the findings (Ouyang et al. 2021) of in vitro experimental system that lacks tumor micro-environment altogether needs to be replicated in primary breast tumors for the validation purpose.
Non-small cell lung cancer
Non-small cell lung cancer (NSCLC) accounts for more than 80% of lung cancer (Ettinger et al. 2012). In NSCLC, PRNCR1 was found to act as competitive endogenous RNA (ceRNA) for mir-126-5p and mir-448 (Fig. 3D) (Guo et al. 2020; Cheng et al. 2018). Experimental evidences showed that mir-126-5p and mir-448 inhibited cell proliferation, migration, invasion and epithelial to mesenchymal transition (EMT) in NSCLC through attenuating MTDH (metadherin) and HEY2 (Hairy and enhancer of split-related with YRPW motif protein 2) mRNAs, respectively. MTDH is a cell adhesion molecule frequently over-expressed in primary NSCLC tumors (Zhang et al. 2018; Guo et al. 2020). Oncogenic impact of MTDH may be exerted through several signaling pathways like Wnt/β-catenin, MAPK, PI3K/AKT, etc. (Wang et al. 2016) that are actively involved in cell cycle progression (Vadlakonda et al. 2013) and deregulation of which has been often reported in NSCLC (Akiri et al. 2009; Ciuffreda et al. 2014). Additionally, therapeutic agent like evodiamine was also used to suppress proliferation and induce apoptosis in human NSCLC cells successfully through blocking MTDH expression (Zou et al. 2015). However, the oncogenic role of MTDH in NSCLC was contradicted in only one investigation (Yao et al. 2014); the discrepancy might be due to racial and ethnic differences in the patient population and/or differences in clinical stages and grades of tumors included in the study from that of other investigations (Zhang et al. 2018; Guo et al. 2020). HEY2 is a transcription factor of bHLH (basic helix–loop–helix) family and a direct target of notch signaling pathway (Fischer et al. 2004). Alteration of notch pathway was noted in NSCLC (Lee et al. 2008) and over-expression of HEY2 was also found in tumor tissue compared to adjacent normal (Westhoff et al. 2009). Therefore, in NSCLC, PRNCR1 influenced deregulation of miR-126-5p/MTDH and miR-448/HEY2 networks by sponging its target miRNAs and this might contribute significantly to the process of tumorigenesis through associated signaling pathways.
Oral squamous cell carcinoma
In oral squamous cell carcinoma (OSCC) and tongue squamous cell carcinoma (TSCC), the most common type of OSCC, PRNCR1 over-expression was reported in primary tumors as well as in cancer cell lines (Liu et al. 2021; Lin et al. 2020). Following PRNCR1 knockdown reduced tumor phenotypes of cancer cells like proliferation, migration, and invasion suggested the association of the lncRNA in disease pathogenesis. Moreover after PRNCR1 knockdown, TSCC cells also showed increased apoptosis in vitro and reduced growth in tumor xenograft (Lin et al. 2020).
In oral cancer, PRNCR1 was found to exert its oncogenic impact through sponging target miRNAs (Fig. 3E). miR-326 was reported as a downstream target of PRNCR1 in OSCC cells leading to the up-regulated expression of Fascin actin-bundling protein-1 (FSCN-1) (Liu et al. 2021); in OSCC, FSCN-1 was over-expressed and found to mediate the activation of positive cell cycle regulators like AKT, ERK and JNK (Alam et al. 2012). miR-326 was found to have lethal effect on OSCC cells (Lindenbergh-van der Plas et al. 2013) and over-expression of FSCN-1 was shown to be associated with poor patient outcome (Chen et al. 2019). Thus, over-expression of miR-326 and subsequent down-regulation of FSCN-1 in oral tumor seemed to be an effective strategy of disease management and this might be achieved through targeting PRNCR1 by novel therapeutic measures. In TSCC cells, PRNCR1 was found to attenuate mir-944 and thereby up-regulate expression of HOXB5 (Lin et al. 2020), a transcription factor over-expressed in head and neck tumors; also in oral cells, HOXB5 was found to involve in the transcriptional up-regulation of EGFR and thereby mediate the activation of AKT/Wnt/β-catenin signaling axis (Lee et al. 2020) associated with the cell cycle regulation (Vadlakonda et al. 2013). Moreover, although tumor-suppressive role of miR-944 was reported in breast and colorectal cancers (Flores-Pérez et al. 2016; Wen et al. 2017), the miRNA was found to be over-expressed and play an oncogenic role in cervical carcinoma (Park et al. 2019) and interestingly in tobacco-induced oral cancer (Peng et al. 2020). Thus, functional role of miR-944 may be oncogenic or tumor-suppressive depending upon upstream modulators (lncRNAs) and downstream target mRNAs and these seem to differ in primary oral tumors under the influence of tumor-specific microenvironment from that of cultured oral cancer cells and hence may contribute to the associated discrepant findings.
Colorectal cancer
PRNCR1 over-expression was reported in primary colorectal carcinoma (CRC) compared to adjacent noncancerous tissue (Yang et al. 2016). PRNCR1 was also over-expressed in CRC cell lines and after its (PRNCR1) knockdown, cell proliferation was inhibited through cell cycle arrest at G0/G1 phase; however, rate of apoptotic cell death remained unaffected and also no significant change was observed in cell migration and invasion properties.
PRNCR1 as potential clinical biomarker in cancer
The PRNCR1 expression level in tumor was shown to have diagnostic and prognostic importance in different human malignancies (Table 1). PRNCR1 locus also harbors many SNPs (genetic variants) some of which showed association with the disease prognosis. In addition, significant association of PRNCR1 SNPs was also reported with the cancer susceptibility in different case–control studies (Table 2).
Prostate cancer
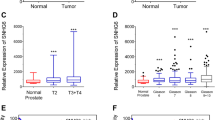
PRNCR1 expression level was not found as a significant predictor for cancer-specific mortality of patients in one investigation (Prensner et al. 2014); but the finding needs further validation as the investigators failed to establish any functional role of the lncRNA in pathogenesis of prostate cancer. Among single-nucleotide polymorphisms (SNPs) of PRNCR1, significant association of rs16901979 was found with tumor Gleason Scores in French West Indies population (Cancel-Tassin et al. 2015). In prostate cancer, Gleason Score is evaluated histopathologically to assess the disease prognosis (Egevad et al. 2002). Therefore, rs16901979 seems to have prognostic importance in prostate cancer that needs to be validated in different patient populations with an aim to develop comparatively less-invasive disease biomarker.
In a case–control study with Iranian population, significant association of PRNCR1 SNPs, rs13252298 (A/G), rs1456315 (A/G), and rs7841060 (T/G) was found with prostate cancer susceptibility, and ‘G’ was found as the risk allele (Sattarifard et al. 2017); moreover, the SNPs remained in linkage disequilibrium (LD) with another PRNCR1 variant (rs7007694, T/C), and the haplotypes GTGG (rs1456315G/ rs7007694T/rs7841060G/rs13252298G) and GTGA were found to be associated with higher disease risk compared to ATTG in the studied population. In other studies, significant association of rs1016343 (C/T) in Chinese populations (Zheng et al. 2010; Hui et al. 2014) and rs13254738 (C/A), rs16901979 (C/A), rs1016343, and rs1456315 in Japanese populations (Yamada et al. 2009; Takata et al. 2010) was reported with the risk of developing prostate cancer. Moreover, in a study conducted on patients of John Hopkins hospital, significant association of rs16901979 was found with the risk of hereditary prostate cancer, but not with risk of non-hereditary disease subtype (Sun et al. 2008). However, on the contrary, no link of the SNP (rs16901979) was established with disease risk in two independent studies on Ashkenazi Jewish and Jamaican populations (Vijai et al. 2011; Cropp et al. 2014).
Breast cancer
PRNCR1 expression level was suggested as a potential diagnostic biomarker in breast cancer (Abdollahzadeh et al. 2020). In ROC (receiver operating characteristic) curve analysis, the optimal cut-off score for PRNCR1 expression was determined with respect to maximum sensitivity and specificity in distinguishing breast tumor from adjacent non-tumor and also from clinically healthy normal tissue. Moreover in breast cancer, significant association of PRNCR1 expression level with increasing tumor size, advanced clinical stages, lymph node metastasis and poor patient survival suggested its importance as a potential prognostic biomarker (Abdollahzadeh et al. 2020; Guo et al. 2019; Ouyang et al. 2021). Interestingly, in breast tumors negative for estrogen receptor (ER) and Her2, significantly higher expression level of PRNCR1 was detected compared to tumors positive for the markers (Abdollahzadeh et al. 2020). Categorization of breast tumors based on ER, PR (progesterone receptor) and Her2 expression status (positive/negative) is a common practice to determine therapeutic modalities (Onitilo et al. 2009). Tumors negative for ER, PR and Her2 (Triple negative breast cancer) show poor response to the conventional therapies using tamoxifen or herceptin and therefore usually have worse prognosis (Al-Mahmood et al. 2018). Higher PRNCR1 level in ER and Her2-negative breast tumors raised the candidature of the lncRNA as target for novel therapeutic with an aim for better management of the disease subtype.
Oral squamous cell carcinoma
In one investigation, malignant tongue tumors were categorized as of high and low PRNCR1 levels taking the median value of the expression as a cut-off; significant association of high PRNCR1 level in tumor was found with parameters of disease progression like increased tumor size, higher clinical stage, and incidence of lymph node metastasis (Lin et al. 2020). Furthermore, significantly shorter overall survival of the patients having high PRNCR1 level in tumors than those with low expression level indicated potential of the lncRNA in predicting disease prognosis.
Colorectal cancer
In colorectal carcinoma (CRC), PRNCR1 level showed higher AUC (area under curve) value in ROC curve analysis than conventional serum based biomarker (CEA-CA199) and hence was proposed as more sensitive one for diagnosing the disease condition (Yang et al. 2016). Higher PRNCR1 expression level was significantly more frequent in tumors of large volume and this indicated possible association of the lncRNA in disease progression; however, the investigators failed to establish any association of PRNCR1 with other clinico-pathological features like tumor TNM stage and differentiation. Among PRNCR1 SNPs, risk allele (G) of rs1456315 was found to be associated with increased tumor size and poor differentiation of CRC in Chinese population (Li et al. 2013). Tumor differentiation (histologic grade) was reported as stage independent prognostic factor for patients having CRC (Alexander et al. 2005). Therefore, rs1456315 seems to have prognostic importance in CRC that needs to be validated in other patient populations and moreover functional analysis of the SNP should also be done to explore the underlying molecular mechanism.
Individual susceptibility for developing CRC was found to be influenced by PRNCR1 variants. In a Chinese population, significant association of AG genotype and G allele of rs13252298 was noted with decreased CRC risk compared to AA genotype and A allele, respectively (Li et al. 2013). In a Saudi population, rs1456315 (T/C) was linked with CRC susceptibility; minor allele ‘C’ was found as the risk allele and CC genotype, as well as CC + CT additive genotypes, showed significant association with increased disease risk (AlMutairi et al. 2019). The authors also noticed significant association of the SNP (rs1456315) with disease susceptibility in younger individuals (≤ 57 years) and females; moreover, the SNP was found to be associated in predisposing individuals for developing tumors particularly at the colon but not at the rectum. As a functional consequence of ‘T’ > ‘C’ allelic substitution of rs1456315, alteration in the secondary structure of PRNCR1 was suggested with a change in minimum free energy level (− 85.70 kcal/mol to − 85.10 kcal/mol) and base pairing probabilities (AlMutairi et al. 2019); but the finding was not validated in wet lab experiments and associated molecular pathway remained unexplored.
Gastric cancer
Prognostic importance of PRNCR1 SNP rs12682421 (G/A) was explored in gastric cancer (GC) in a Chinese population (Zhang et al. 2020); patients carrying AA genotype for the SNP was found to experience higher death incidence than those with GG and GA. However, the finding needs to be replicated before its implementation to predict patient outcome so that personalized therapeutic strategies may be designed in accordance. In bioinformatics analysis, ‘A’ allele of rs12682421 was shown to facilitate binding of PRNCR1 with glucocorticoid receptor β (GR-β) and the phenomenon was hypothesized to contribute poor prognosis of GC patients (Zhang et al. 2020). GR-β is a transcription factor that lacks glucocorticoid binding site and acts as inhibitor for transcriptional activity of its alternatively spliced isoform GR-α (Yudt et al. 2003). GR-β is pro-inflammatory in function and has been found to promote aggressive tumor phenotype (cell migration) in bladder cancer and glioma (McBeth et al. 2016; Yin et al. 2013). But the role of GR-β in the pathogenesis of GC is not well characterized and a very low/undetectable expression level of the receptor has been found in gastric tumors (Block et al. 2017). Furthermore, in existing literature, although glucocorticoid receptor was found to interact with lncRNA, such interaction was mediated competitively through DNA-binding domain of the receptor leading to inactivation of its transcriptional activity (Parsonnet et al. 2019). Therefore, in the study done by Zhang et al., bioinformatics finding for interaction of PRNCR1 with GR-β needs to be validated in wet lab experiments and potential impact of such interaction on GR-β should be assessed in functional analysis.
PRNCR1 SNPs were also studied in connection with GC susceptibility. In a Chinese population, AG genotype of rs13252298 showed significant association with increased risk of gastric cancer (GC), while CT and CC genotypes of rs7007694 (C/G/T) and GG genotype of rs1456315 (A/G/T) were associated with significantly decreased disease risk (Li et al. 2016a). In one more study with the Chinese population, G allele of PRNCR1 SNP rs16901946 (A/G) was shown to be associated with GC risk (He et al. 2017); moreover, among the carriers of risk allele, significantly increased GC susceptibility in male, individuals aged ≤ 60 years and in those having Helicobacter pylori infection suggested potential interaction of the SNP genotypes with gender, age, and bacterial infection toward predisposition to the disease. In Korean population, TT genotype of rs1016343 was found to be associated with significantly decreased risk of GC negative for lymph node metastasis (LNM) in < 60-year-old subjects (Hong et al. 2019). The study also found significant association of GG genotype of rs13252298 with higher risk of intestinal-type GC which is more frequently linked to dietary and environmental factors than diffuse-type GC in which genetic contribution is mostly highlighted (Hu et al. 2012). In addition, when GC subtypes were considered together and age-stratified, the study found significant association of the SNP genotype (GG, rs13252298) with higher GC risk of tumor stage III and positive LNM in subjects of ≥ 60 years (Hong et al. 2019).
Lung cancer
Among PRNCR1 SNPs, rs13252298 and rs1456315 were found to influence the susceptibility of lung cancer (LC) and non-small cell lung cancer (NSCLC) in a Chinese northeast population (Li et al. 2021b). Surprisingly the authors did not find significant interaction of the SNPs with cigarette smoking and the variants were found to be associated with the disease susceptibility (LC & NSCLC) of females only but not in males. NSCLC incidence was also reported among never smokers especially females and the disease subset was considered to have a unique genetic predisposition (Devesa et al. 2005; Santoro et al. 2011) to which PRNCR1 SNPs seemed to have a significant contribution.
Considering diagnostic and prognostic importance of PRNCR1 expression level in tumor, sensitivity and specificity scores should be evaluated more extensively before introducing the criteria in routine clinical practice for associated malignant conditions. The associations of PRNCR1 SNPs with cancer susceptibility in different populations need to be replicated so that the information can be explored as components of disease risk prediction models that may be useful to identify individuals at elevated risk (Wen et al. 2016; Hosono et al. 2016). However, some PRNCR1 variants also showed association for decreased susceptibility to certain malignancies and this might be due to genetic variability specific to the ethnicity of the studied population and differential interaction of SNP genotypes with disease-specific risk factors. Similarly, genetic variants of other oncogenic lncRNAs like PCAT1 and MALAT1 were also found to be associated with decreased susceptibilities to bladder and lung cancers, respectively (Lin et al. 2017; Chen et al. 2021a). PRNCR1 SNPs are located in exon-1 and are non-coding as the gene encodes for an lncRNA. But, allelic variations at SNP site seemed to affect the secondary structure of PRNCR1 (AlMutairi et al. 2019). In lncRNAs like MALAT1, HOTAIR, SRA and MEG3, secondary structure was reported to play vital functional role (Brown et al. 2012; Somarowthu et al. 2015; Novikova et al. 2012; Zhang et al. 2010). Moreover, in lncRNA, allelic variations of exonic SNP might contribute to loss/gain of miRNA target site (Miao et al. 2018) and the role of PRNCR1 as a miRNA sponge is well established (Cheng et al. 2018; Ouyang et al. 2021; Guo et al. 2020). Therefore, in PRNCR1, impact of the SNPs in connection to all possible functional aspects of the lncRNA need to be analyzed in details to explore the molecular basis for association of the variants with cancer susceptibility.
Therapeutic importance of PRNCR1
Frequent over-expression of PRNCR1 in malignancies and its association with adverse tumor phenotypes and poor patient outcome suggested importance of the lncRNA as a potential target for novel cancer therapeutics (Guo et al. 2019; Abdollahzadeh et al. 2020; Lin et al. 2020; Yang et al. 2016). Oncogenic lncRNAs are commonly targeted at post-transcriptional level by RNA interference (RNAi), antisense oligonucleotides (ASOs) and morpholino ASOs (block RNA function sterically) for therapeutic purpose; however, CRISPR/Cas9-mediated transcriptional silencing of gene locus is also considered as an important strategy (Arun et al. 2018).
In cell line-based experiments, PRNCR1 was knocked down post-transcriptionally by siRNA in breast cancer (Pang et al. 2019) and by ASO in colorectal cancer (Yang et al. 2016). In oral cancer, siRNA-mediated knock-down of PRNCR1 was successfully accomplished in vitro as well as in vivo system, but restricted to the xenograft tumor model only (Lin et al. 2020). However, xenograft tumors, as developed from cultured human cancer cell line, may not have representative histological architecture and cellular complexity of native primary tumors (Becher and Holland 2006). Thus, as a prerequisite of clinical trials, therapeutic strategies targeting PRNCR1 need to be tested in extensive pre-clinical studies involving chemical carcinogen-induced or genetically engineered animal models. But, the PRNCR1 locus is found in human only and absence of the gene ortholog in other mammalian species may be a limiting factor for its animal model experimentation. For other oncogenic lncRNAs like DANCR, LINC01296, MALAT1, etc., detailed preclinical research on siRNA/ASO-based techniques was also done in addition to in vitro studies, indicating prospects of the strategy for clinical trials (Chen et al. 2021b).
The interaction of PRNCR1 with its target miRNAs and proteins (AR, DOT1L, etc.) can be blocked sterically by morpholino ASOs (chemically modified and unable to induce RNAse H activity) designed against specific secondary/tertiary structures of the lncRNA involved at interaction interfaces. Morpholino ASOs can be used to block disease-specific function of an lncRNA (i.e., interaction with one miRNA) leaving other functions unaffected (Lennox and Behlke 2016; Arun et al. 2018); hence, the strategy seems to be superior over others that target the entire lncRNA for transcriptional silencing or degradation. Morpholino ASOs were used successfully to block lncRNAs like Cyrano, NATs (natural antisense transcripts) etc. (Lennox and Behlke 2016); for implementation of the strategy against PRNCR1, detailed information on secondary/tertiary structure of the lncRNA determined using advanced tools like SHAPE (Selective 2′ Hydroxyl Acylation analyzed by Primer Extension) and PARIS (Psoralen Analysis of RNA Interactions and Structures), is needed as an essential prerequisite.
Transcriptional silencing of lncRNA can be achieved by CRISPR/Cas9 method. In one study, CRISPR interference (CRISPRi) libraries have been developed to inactivate promoters of 16,401 lncRNA genes loci across the human genome (Liu et al. 2017). Investigators validated the efficiency of the method in suppression of major oncogenic lncRNA loci like MINCR, PVT1, DANCR, LINC00467, etc. in human cancer cell lines and also assessed the impact on cellular phenotypes. However, PRNCR1 promoter is not well characterized and this may restrict the successful designing of single guide RNA (sgRNA) for CRISPR/Cas9-mediated knockdown of the lncRNA locus.
Conclusion and future perspectives
As oncogenic lncRNA, although over-expression of PRNCR1 has been found in malignancies of different organs, the underlying molecular mechanism remains largely unexplored. Impact of PRNCR1 on aggressive tumor phenotypes like cell proliferation, migration and invasion should be studied in more details to identify and characterize associated signaling pathways. Ligand-independent activation of androgen receptor (AR) was frequently reported in castration resistant prostate cancer (CRPC) (Hu et al. 2009; Li et al. 2016b) and the conflicting result was available on role of PRNCR1 in this connection (Yang et al. 2013; Prensner et al. 2014). CRPC is an aggressive disease subtype with worse prognosis and attempts for improvement of disease outcome by novel therapeutics targeting the AR have been reported (Chiin and Attard 2013; Narayanan 2020). Apart from prostate cancer, aberrant AR activation was also reported in gastric carcinoma, hepatocellular carcinoma, and some subtype of breast cancer (Zhang et al. 2014; Jiang et al. 2014; Ni et al. 2011). Therefore, extensive research is warranted to explore the role of PRNCR1 in AR signaling pathway with an aim to design novel strategies for the associated malignant conditions. Detail investigation is also warranted regarding discrepant findings on target miRNA and downstream oncogenic effectors of PRNCR1 in OSCC, breast cancer and NSCLC, respectively. Moreover, the functional role of PRNCR1 in pathogenesis of CRC is needed to explore in more details for identification and characterization of associated molecular pathways. Recently, lncRNAs are emerging as novel tumor biomarkers due to their stability in exosomes of body fluids like plasma, urine and saliva (Li et al. 2015; Berrondo et al. 2016; Tang et al. 2013). Tumor cells have a tendency to release more exosomes and hence peripheral blood of cancer patients usually contains higher amount of exosomes than that of disease-free control (Melo et al. 2015). PRNCR1 level in tumor was shown to have diagnostic and prognostic importance and comparatively higher expression level of the lncRNA was also found in blood exosomes of patients of pancreatic carcinoma, hepatocellular carcinoma and colorectal cancer than that of normal control (GSE100063, GSE100206) (Fig. 2D); for clinical implication of the findings, further research is needed to analyze the lncRNA level more extensively in blood as well as other body fluids of diseased and normal individuals in connection with different disease parameters.
Therefore, as per available literature, PRNCR1 plays vital roles in the pathogenesis of human malignancies molecular basis of which is not fully understood; this seems to open new scope of further research for exploring all possible potentials of the lncRNA in diagnostic, prognostic and therapeutic aspects of associated disease conditions.
Availability of data and material
Not applicable.
Code availability
Not applicable.
References
Abdollahzadeh R, Mansoori Y, Azarnezhad A et al (2020) Expression and clinicopathological significance of AOC4P, PRNCR1, and PCAT1 lncRNAs in breast cancer. Pathol Res Pract 216(10):153131. https://doi.org/10.1016/j.prp.2020.153131
Adhikary J, Chakraborty S, Dalal S et al (2019) Circular PVT1: an oncogenic non-coding RNA with emerging clinical importance. J Clin Pathol 72(8):513–519. https://doi.org/10.1136/jclinpath-2019-205891
Akiri G, Cherian MM, Vijayakumar S et al (2009) Wnt pathway aberrations including autocrine Wnt activation occur at high frequency in human non-small-cell lung carcinoma. Oncogene 28(21):2163–2172. https://doi.org/10.1038/onc.2009.82
Alam H, Bhate AV, Gangadaran P et al (2012) Fascin overexpression promotes neoplastic progression in oral squamous cell carcinoma. BMC Cancer 12:32. https://doi.org/10.1186/1471-2407-12-32
Alexander D, Jhala N, Chatla C et al (2005) High-grade tumor differentiation is an indicator of poor prognosis in African Americans with colonic adenocarcinomas. Cancer 103(10):2163–2170. https://doi.org/10.1002/cncr.21021
Al-Mahmood S, Sapiezynski J, Garbuzenko OB et al (2018) Metastatic and triple-negative breast cancer: challenges and treatment options. Drug Deliv Transl Res 8(5):1483–1507. https://doi.org/10.1007/s13346-018-0551-3
AlMutairi M, Parine NR, Shaik JP et al (2019) Association between polymorphisms in PRNCR1 and risk of colorectal cancer in the Saudi population. PLoS ONE 14(9):e0220931. https://doi.org/10.1371/journal.pone.0220931
Anderson DJ, Kaplan DI, Bell KM et al (2018) NKX2-5 regulates human cardiomyogenesis via a HEY2 dependent transcriptional network. Nat Commun 9(1):1373. https://doi.org/10.1038/s41467-018-03714-x
Arun G, Diermeier SD, Spector DL (2018) Therapeutic targeting of long non-coding RNAs in cancer. Trends Mol Med 24(3):257–277. https://doi.org/10.1016/j.molmed.2018.01.001
Balk SP, Knudsen KE (2008) AR, the cell cycle, and prostate cancer. Nucl Recept Signal 6:e001. https://doi.org/10.1621/nrs.06001
Becher OJ, Holland EC (2006) Genetically engineered models have advantages over xenografts for preclinical studies. Cancer Res 66(7):3355–3358. https://doi.org/10.1158/0008-5472.CAN-05-3827 (Discussion 3358–3359)
Berrondo C, Flax J, Kucherov V et al (2016) Expression of the long non-coding RNA HOTAIR correlates with disease progression in bladder cancer and is contained in bladder cancer patient urinary exosomes. PLoS ONE 11(1):e0147236. https://doi.org/10.1371/journal.pone.0147236
Bhosale PG, Cristea S, Ambatipudi S et al (2017) Chromosomal alterations and gene expression changes associated with the progression of leukoplakia to advanced gingivobuccal cancer. Transl Oncol 10(3):396–409. https://doi.org/10.1016/j.tranon.2017.03.008
Block TS, Murphy TI, Munster PN et al (2017) Glucocorticoid receptor expression in 20 solid tumor types using immunohistochemistry assay. Cancer Manag Res 9:65. https://doi.org/10.2147/CMAR.S124475
Bodelon C, Untereiner ME, Machiela MJ et al (2016) Genomic characterization of viral integration sites in HPV-related cancers. Int J Cancer 139(9):2001–2011. https://doi.org/10.1002/ijc.30243
Brown JA, Valenstein ML, Yario TA et al (2012) Formation of triple-helical structures by the 3′-end sequences of MALAT1 and MENβ noncoding RNAs. Proc Natl Acad Sci USA 109(47):19202–19207. https://doi.org/10.1073/pnas.1217338109
Cancel-Tassin G, Romana M, Gaffory C et al (2015) Region 2 of 8q24 is associated with the risk of aggressive prostate cancer in Caribbean men of African descent from Guadeloupe (French West Indies). Asian J Androl 17(1):117. https://doi.org/10.4103/1008682X.135127
Chen Y, Tian T, Li ZY et al (2019) FSCN1 is an effective marker of poor prognosis and a potential therapeutic target in human tongue squamous cell carcinoma. Cell Death Dis 10(5):356. https://doi.org/10.1038/s41419-019-1574-5
Chen M, Cai D, Gu H et al (2021a) MALAT1 rs619586 A/G polymorphisms are associated with decreased risk of lung cancer. Medicine (baltimore) 100(12):e23716. https://doi.org/10.1097/MD.0000000000023716
Chen Y, Li Z, Chen X, Zhang S (2021b) Long non-coding RNAs: From disease code to drug role. Acta Pharm Sin B 11(2):340–354. https://doi.org/10.1016/j.apsb.2020.10.001
Cheng D, Bao C, Zhang X et al (2018) LncRNA PRNCR1 interacts with HEY2 to abolish miR-448-mediated growth inhibition in non-small cell lung cancer. Biomed Pharmacother 107:1540–15407. https://doi.org/10.1016/j.biopha.2018.08.105
Chernikova D, Managadze D, Glazko GV et al (2016) Conservation of the exon-intron structure of long intergenic non-coding RNA genes in eutherian mammals. Life (basel) 6(3):27. https://doi.org/10.3390/life6030027
Chiin AL, Attard G (2013) Improved therapeutic targeting of the androgen receptor: rational drug design improves survival in castration-resistant prostate cancer. Curr Drug Targets 14(4):408–419. https://doi.org/10.2174/1389450111314040003
Chung S, Nakagawa H, Uemura M et al (2011) Association of a novel long non-coding RNA in 8q24 with prostate cancer susceptibility. Cancer Sci 102(1):245–252. https://doi.org/10.1111/j.1349-7006.2010.01737.x
Ciuffreda L, Cesta Incani U, Steelman SL et al (2014) Signalling intermediates (MAPK and PI3K) as therapeutic targets in NSCLC. Curr Pharm Des 20(24):3944–3957. https://doi.org/10.2174/13816128113196660763
Cropp CD, Robbins CM, Sheng X et al (2014) 8q24 risk alleles and prostate cancer in African-Barbadian men. Prostate 74(16):1579–1588. https://doi.org/10.1002/pros.22871
Derrien T, Johnson R, Bussotti G et al (2012) The GENCODE v7 catalog of human long noncoding RNAs: analysis of their gene structure, evolution, and expression. Genome Res 22(9):1775–1789. https://doi.org/10.1101/gr.132159.111
Devesa SS, Bray F, Vizcaino AP et al (2005) International lung cancer trends by histologic type: male: female differences diminishing and adenocarcinoma rates rising. Int J Cancer 117(2):294–299. https://doi.org/10.1002/ijc.21183
Djebali S, Davis CA, Merkel A et al (2012) Landscape of transcription in human cells. Nature 489(7414):101–108. https://doi.org/10.1038/nature11233
Egevad L, Granfors T, Karlberg L et al (2002) Prognostic value of the Gleason score in prostate cancer. BJU Int 89(6):538–542. https://doi.org/10.1046/j.1464-410x.2002.02669.x
Elliott B, Millena AC, Matyunina L et al (2019) Essential role of JunD in cell proliferation is mediated via MYC signalling in prostate cancer cells. Cancer Lett 448:155–167. https://doi.org/10.1016/j.canlet.2019.02.005
Ettinger DS, Akerley W, Borghaei H et al (2012) Non–small cell lung cancer. J Natl Compr Cancer Netw 10(10):1236–1271. https://doi.org/10.6004/jnccn.2012.0130
Evron E, Umbricht CB, Korz D et al (2001) Loss of cyclin D2 expression in the majority of breast cancers is associated with promoter hypermethylation. Cancer Res 61(6):2782–2787 (PMID: 11289162)
Fang Z, Lin A, Chen J et al (2016) CREB1 directly activates the transcription of ribonucleotide reductase small subunit M2 and promotes the aggressiveness of human colorectal cancer. Oncotarget 7(47):78055–78068. https://doi.org/10.18632/oncotarget.12938
Faust T, Frankel A, D’Orso I (2012) Transcription control by long non-coding RNAs. Transcription 3(2):78–86. https://doi.org/10.4161/trns.19349
Fischer H, Chen J, Skoog L et al (2002) Cyclin D2 expression in familial and sporadic breast cancer. Oncol Rep 9(6):1157–1161 (PMID: 12375011)
Fischer A, Schumacher N, Maier M et al (2004) The Notch target genes Hey1 and Hey2 are required for embryonic vascular development. Genes Dev 18(8):901–911. https://doi.org/10.1101/gad.291004
Flores-Pérez A, Marchat LA, Rodríguez-Cuevas S et al (2016) Suppression of cell migration is promoted by miR-944 through targeting of SIAH1 and PTP4A1 in breast cancer cells. BMC Cancer 16:379. https://doi.org/10.1186/s12885-016-2470-3
Guo Q, Lv S, Wang B et al (2019) Long non-coding RNA PRNCR1 has an oncogenic role in breast cancer. Exp Ther Med 18(6):4547–4554. https://doi.org/10.3892/etm.2019.8152
Guo R, Hu T, Liu Y et al (2020) Long non-coding RNA PRNCR1 modulates non-small cell lung cancer cell proliferation, apoptosis, migration, invasion, and EMT through PRNCR1/miR-126–5p/MTDH axis. Biosci Rep. https://doi.org/10.1042/BSR20193153
Hangauer MJ, Vaughn IW, McManus MT (2013) Pervasive transcription of the human genome produces thousands of previously unidentified long intergenic noncoding RNAs. PLoS Genet 9(6):e1003569. https://doi.org/10.1371/journal.pgen.1003569
He BS, Sun HL, Xu T et al (2017) Association of genetic polymorphisms in the LncRNAs with gastric cancer risk in a Chinese population. J Cancer 8(4):531. https://doi.org/10.7150/jca.17519
He RZ, Luo DX, Mo YY (2019) Emerging roles of lncRNAs in the post-transcriptional regulation in cancer. Genes Dis 6(1):6–15. https://doi.org/10.1016/j.gendis.2019.01.003
Hong JH, Jin EH, Kang H et al (2019) Correlations between genetic polymorphisms in long non-coding RNA PRNCR1 and gastric cancer risk in a Korean population. Int J Mol Sci 20(13):3355. https://doi.org/10.3390/ijms20133355
Hosono S, Ito H, Oze I et al (2016) A risk prediction model for colorectal cancer using genome-wide association study-identified polymorphisms and established risk factors among Japanese: results from two independent case-control studies. Eur J Cancer Prev 25(6):500–507. https://doi.org/10.1097/CEJ.0000000000000213
Hu R, Dunn TA, Wei S et al (2009) Ligand-independent androgen receptor variants derived from splicing of cryptic exons signify hormone-refractory prostate cancer. Cancer Res 69(1):16–22. https://doi.org/10.1158/0008-5472.CAN-08-2764
Hu B, El Hajj N, Sittler S et al (2012) Gastric cancer: Classification, histology and application of molecular pathology. J Gastrointest Oncol 3(3):251. https://doi.org/10.3978/j.issn.2078-6891.2012.021
Hui J, Xu Y, Yang K et al (2014) Study of genetic variants of 8q21 and 8q24 associated with prostate cancer in Jing-Jin residents in northern China. Clin Lab 60(4):645–652. https://doi.org/10.7754/clin.lab.2013.130624
Hung CS, Wang SC, Yen YT et al (2018) Hypermethylation of CCND2 in lung and breast cancer is a potential biomarker and drug target. Int J Mol Sci 19(10):3096. https://doi.org/10.3390/ijms19103096
Huppi K, Pitt JJ, Wahlberg BM et al (2012) The 8q24 gene desert: an oasis of non-coding transcriptional activity. Front Genet 3:69. https://doi.org/10.3389/fgene.2012.00069
Jiang X, Kanda T, Nakamoto S et al (2014) Involvement of androgen receptor and glucose-regulated protein 78 kDa in human hepatocarcinogenesis. Exp Cell Res 323(2):326–336. https://doi.org/10.1016/j.yexcr.2014.02.017
Kashyap V, Ahmad S, Nilsson EM et al (2013) The lysine specific demethylase-1 (LSD1/KDM1A) regulates VEGF-A expression in prostate cancer. Mol Oncol 7(3):555–566. https://doi.org/10.1016/j.molonc.2013.01.003
Kim T, Cui R, Jeon YJ (2014) Long-range interaction and correlation between MYC enhancer and oncogenic long noncoding RNA CARLo-5. Proc Natl Acad Sci USA 111(11):4173–4178. https://doi.org/10.1073/pnas.1400350111
Lai JJ, Lai KP, Zeng W, Chuang KH, Altuwaijri S, Chang C (2012) Androgen receptor influences on body defense system via modulation of innate and adaptive immune systems: lessons from conditional AR knockout mice. Am J Pathol 181(5):1504–1512. https://doi.org/10.1016/j.ajpath.2012.07.008
Lancho O, Herranz D (2018) The MYC enhancer-ome: long-range transcriptional regulation of MYC in cancer. Trends Cancer 4(12):810–822. https://doi.org/10.1016/j.trecan.2018.10.003
Lee SM, Jung CK, Ko YH et al (2008) Expression of Notch 1 and 3 is related to inhibition of lymph node metastasis and progression in non-small cell lung carcinomas. Basic Appl Pathol 1(2):93–97. https://doi.org/10.1111/j.17559294.2008.00020.x
Lee K, Chang JW, Oh C et al (2020) HOXB5 acts as an oncogenic driver in head and neck squamous cell carcinoma via EGFR/Akt/Wnt/β-catenin signaling axis. Eur J Surg Oncol 46(6):1066–1073. https://doi.org/10.1016/j.ejso.2019.12.009
Lennox KA, Behlke MA (2016) Cellular localization of long non-coding RNAs affects silencing by RNAi more than by antisense oligonucleotides. Nucleic Acids Res 44(2):863–877. https://doi.org/10.1093/nar/gkv1206
Leto K, Bartolini A, Di Gregorio A et al (2011) Modulation of cell-cycle dynamics is required to regulate the number of cerebellar GABAergic interneurons and their rhythm of maturation. Development 138(16):3463–3472. https://doi.org/10.1242/dev.064378
Li L, Sun R, Liang Y et al (2013) Association between polymorphisms in long non-coding RNA PRNCR1 in 8q24 and risk of colorectal cancer. J Exp Clin Cancer Res 32(1):104. https://doi.org/10.1186/1756-9966-32-104
Li Q, Shao Y, Zhang X et al (2015) Plasma long noncoding RNA protected by exosomes as a potential stable biomarker for gastric cancer. Tumour Biol 36(3):2007–2012. https://doi.org/10.1007/s13277-014-2807-y
Li L, Jia F, Bai P et al (2016a) Association between polymorphisms in long non-coding RNA PRNCR1 in 8q24 and risk of gastric cancer. Tumour Biol 37(1):299–303. https://doi.org/10.1007/s13277-015-3750-2
Li H, Xie N, Chen R et al (2016b) UGT2B17 expedites progression of castration-resistant prostate cancers by promoting ligand-independent AR signalling. Cancer Res 76(22):6701–6711. https://doi.org/10.1158/0008-5472.CAN-16-1518
Li N, Cui Z, Gao M et al (2021b) Genetic polymorphisms of PRNCR1 and lung cancer risk in chinese northeast population: a case-control study and meta-analysis. DNA Cell Biol 40(1):132–144. https://doi.org/10.1089/dna.2020.6194
Li Z, Liu L, Jiang S et al (2021a) LncExpDB: an expression database of human long non-coding RNAs. Nucleic Acids Res 49(D1):D962–D968. https://doi.org/10.1093/nar/gkaa850
Lin Y, Ge Y, Wang Y et al (2017) The association of rs710886 in lncRNA PCAT1 with bladder cancer risk in a Chinese population. Gene 627:226–232. https://doi.org/10.1016/j.gene.2017.06.021
Lin C, Zou Y, Li R et al (2020) Long non-coding RNA PRNCR1 exerts oncogenic effects in tongue squamous cell carcinoma in vitro and in vivo by sponging microRNA-944 and thereby increasing HOXB5 expression. Int J Mol Med 46(1):119–130. https://doi.org/10.3892/ijmm.2020.4581
Lindenbergh-van der Plas M, Martens-de Kemp SR, de Maaker M et al (2013) Identification of lethal microRNAs specific for head and neck cancer. Clin Cancer Res 19(20):5647–5657. https://doi.org/10.1158/1078-0432.CCR-12-2295
Liu SJ, Nowakowski TJ, Pollen AA et al (2016) Single-cell analysis of long non-coding RNAs in the developing human neocortex. Genome Biol 17:67. https://doi.org/10.1186/s13059-016-0932-1
Liu SJ, Horlbeck MA, Cho SW et al (2017) CRISPRi-based genome-scale identification of functional long noncoding RNA loci in human cells. Science. https://doi.org/10.1126/science.aah7111
Liu DK, Li YJ, Tian B et al (2021) LncRNA PRNCR1 aggravates the malignancy of oral squamous cell carcinoma by regulating miR-326/FSCN1 axis. Eur Rev Med Pharmacol Sci 25(8):3226–3234. https://doi.org/10.26355/eurrev_202104_25731
Martone J, Mariani D, Santini T et al (2020) SMaRT lncRNA controls translation of a G-quadruplex-containing mRNA antagonizing the DHX36 helicase. EMBO Rep 21(6):e49942. https://doi.org/10.15252/embr.201949942
McBeth L, Nwaneri AC, Grabnar M et al (2016) Glucocorticoid receptor beta increases migration of human bladder cancer cells. Oncotarget 7(19):27313. https://doi.org/10.18632/oncotarget.8430
Melo SA, Luecke LB, Kahlert C et al (2015) Glypican-1 identifies cancer exosomes and detects early pancreatic cancer. Nature 523(7559):177–182. https://doi.org/10.1038/nature14581
Miao YR, Liu W, Zhang Q et al (2018) lncRNASNP2: an updated database of functional SNPs and mutations in human and mouse lncRNAs. Nucleic Acids Res 46(D1):D276–D280. https://doi.org/10.1093/nar/gkx1004
Milde-Langosch K, Löning T, Bamberger AM (2003) Expression of the CCAAT/ enhancer-binding proteins C/EBPalpha, C/EBPbeta and C/EBPdelta in breast cancer: correlations with clinicopathologic parameters and cell-cycle regulatory proteins. Breast Cancer Res Treat 79(2):175–185. https://doi.org/10.1023/a:1023929504884
Narayanan R (2020) Therapeutic targeting of the androgen receptor (AR) and AR variants in prostate cancer. Asian J Urol 7(3):271–283. https://doi.org/10.1016/j.ajur.2020.03.002
Ni M, Chen Y, Lim E et al (2011) Targeting androgen receptor in estrogen receptor-negative breast cancer. Cancer Cell 20(1):119–131. https://doi.org/10.1016/j.ccr.2011.05.026
Novikova IV, Hennelly SP, Sanbonmatsu KY (2012) Structural architecture of the human long non-coding RNA, steroid receptor RNA activator. Nucleic Acids Res 40(11):5034–5051. https://doi.org/10.1093/nar/gks071
Onitilo AA, Engel JM, Greenlee RT et al (2009) Breast cancer subtypes based on ER/PR and Her2 expression: comparison of clinicopathologic features and survival. Clin Med Res 7(1–2):4–13. https://doi.org/10.3121/cmr.2009.825
Ouyang J, Liu Z, Yuan X et al (2021) LncRNA PRNCR1 promotes breast cancer proliferation and inhibits apoptosis by modulating microRNA-377/CCND2/MEK/MAPK axis. Arch Med Res. https://doi.org/10.1016/j.arcmed.2021.01.007
Pang D, Hu Q, Lan X et al (2019) The novel long non-coding RNA PRNCR1-2 is involved in breast cancer cell proliferation, migration, invasion and cell cycle progression. Mol Med Rep 19(3):1824–1832. https://doi.org/10.3892/mmr.2018.9789
Park S, Kim J, Eom K et al (2019) microRNA-944 overexpression is a biomarker for poor prognosis of advanced cervical cancer. BMC Cancer 19(1):419. https://doi.org/10.1186/s12885-019-5620-6
Parsonnet NV, Lammer NC, Holmes ZE et al (2019) The glucocorticoid receptor DNA-binding domain recognizes RNA hairpin structures with high affinity. Nucleic Acids Res 47(15):8180–8192. https://doi.org/10.1093/nar/gkz486
Peng HY, Hsiao JR, Chou ST et al (2020) MiR-944/CISH mediated inflammation via STAT3 is involved in oral cancer malignance by cigarette smoking. Neoplasia 22(11):554–565. https://doi.org/10.1016/j.neo.2020.08.005
Prensner JR, Sahu A, Iyer MK et al (2014) The lncRNAs PCGEM1 and PRNCR1 are not implicated in castration resistant prostate cancer. Oncotarget 5(6):1434. https://doi.org/10.18632/oncotarget.1846
Raeder MB, Birkeland E, Trovik J et al (2013) Integrated genomic analysis of the 8q24 amplification in endometrial cancers identifies ATAD2 as essential to MYC-dependent cancers. PLoS ONE 8(2):e54873. https://doi.org/10.1371/journal.pone.0054873
Santoro IL, Ramos RP, Franceschini J et al (2011) Non-small cell lung cancer in never smokers: a clinical entity to be identified. Clinics 66(11):1873–1877. https://doi.org/10.1590/s1807-59322011001100005
Sarropoulos I, Marin R, Cardoso-Moreira M et al (2019) Developmental dynamics of lncRNAs across mammalian organs and species. Nature 571(7766):510–514. https://doi.org/10.1038/s41586-019-1341-x
Sattarifard H, Hashemi M, Hassanzarei S et al (2017) Association between genetic polymorphisms of long non-coding RNA PRNCR1 and prostate cancer risk in a sample of the Iranian population. Mol Clin Oncol 7(6):1152–1158. https://doi.org/10.3892/mco.2017.1462
Somarowthu S, Legiewicz M, Chillón I et al (2015) HOTAIR forms an intricate and modular secondary structure. Mol Cell 58(2):353–361. https://doi.org/10.1016/j.molcel.2015.03.006
Sun J, Lange EM, Isaacs SD et al (2008) Chromosome 8q24 risk variants in hereditary and non-hereditary prostate cancer patients. Prostate 68(5):489–497. https://doi.org/10.1002/pros.20695
Sun Q, Hao Q, Prasanth KV (2018) Nuclear long noncoding RNAs: key regulators of gene expression. Trends Genet 34(2):142–157. https://doi.org/10.1016/j.tig.2017.11.005
Takata R, Akamatsu S, Kubo M et al (2010) Genome-wide association study identifies five new susceptibility loci for prostate cancer in the Japanese population. Nat Genet 42(9):751–754. https://doi.org/10.1038/ng.635
Tang H, Wu Z, Zhang J et al (2013) Salivary lncRNA as a potential marker for oral squamous cell carcinoma diagnosis. Mol Med Rep 7(3):761–766. https://doi.org/10.3892/mmr.2012.1254
Truong PK, Lao TD, Doan TP et al (2015) Loss of expression of cyclin d2 by aberrant DNA methylation: a potential biomarker in vietnamese breast cancer patients. Asian Pac J Cancer Prev 16(6):2209–2213. https://doi.org/10.7314/apjcp.2015.16.6.2209
Vadlakonda L, Pasupuleti M, Pallu R (2013) Role of PI3K-AKT-mTOR and Wnt Signaling Pathways in Transition of G1-S Phase of Cell Cycle in Cancer Cells. Front Oncol 3:85. https://doi.org/10.3389/fonc.2013.00085
Vijai J, Kirchhoff T, Gallagher D et al (2011) Genetic architecture of prostate cancer in the Ashkenazi Jewish population. Br J Cancer 105(6):864–869. https://doi.org/10.1038/bjc.2011.307
Wang Z, Tang ZY, Yin Z et al (2016) Metadherin regulates epithelial–mesenchymal transition in carcinoma. Onco Targets Ther 9:2429. https://doi.org/10.2147/OTT.S104556
Wang Q, Wu Y, Li F et al (2018) Association of genetic polymorphisms in immune-related lncRNA with osteoarthritis susceptibility in Chinese Han population. Per Med 15(2):103–110. https://doi.org/10.2217/pme-2017-0072
Wen W, Shu XO, Guo X et al (2016) Prediction of breast cancer risk based on common genetic variants in women of East Asian ancestry. Breast Cancer Res 18(1):124. https://doi.org/10.1186/s13058-016-0786-1
Wen L, Li Y, Jiang Z, Zhang Y, Yang B, Han F et al (2017) miR-944 inhibits cell migration and invasion by targeting MACC1 in colorectal cancer. Oncol Rep 37(6):3415–3422. https://doi.org/10.3892/or.2017.5611
Westhoff B, Colaluca IN, D’Ario G et al (2009) Alterations of the Notch pathway in lung cancer. Proc Natl Acad Sci USA 106(52):22293–22298. https://doi.org/10.1073/pnas.0907781106
Yamada H, Penney KL, Takahashi H et al (2009) Replication of prostate cancer risk loci in a Japanese case–control association study. J Natl Cancer Inst 101(19):1330–1336. https://doi.org/10.1093/jnci/djp287
Yang L, Lin C, Jin C et al (2013) lncRNA-dependent mechanisms of androgen-receptor-regulated gene activation programs. Nature 500(7464):598–602. https://doi.org/10.1038/nature12451
Yang L, Qiu M, Xu Y et al (2016) Upregulation of long non-coding RNA PRNCR1 in colorectal cancer promotes cell proliferation and cell cycle progression. Oncol Rep 35(1):318–324. https://doi.org/10.3892/or.2015.4364
Yao Y, Gu X, Liu H et al (2014) Metadherin regulates proliferation and metastasis via actin cytoskeletal remodelling in non-small cell lung cancer. Br J Cancer 111(2):355–364. https://doi.org/10.1038/bjc.2014.267
Yin Y, Zhang X, Li Z et al (2013) Glucocorticoid receptor β regulates injury-mediated astrocyte activation and contributes to glioma pathogenesis via modulation of β-catenin/TCF transcriptional activity. Neurobiol Dis 59:165–176. https://doi.org/10.1016/j.nbd.2013.07.013
Yudt MR, Jewell CM, Bienstock RJ et al (2003) Molecular origins for the dominant negative function of human glucocorticoid receptor beta. Mol Cell Biol 23(12):4319–4330. https://doi.org/10.1128/MCB.23.12.4319-4330.2003
Zhang X, Rice K, Wang Y et al (2010) Maternally expressed gene 3 (MEG3) noncoding ribonucleic acid: isoform structure, expression, and functions. Endocrinology 151(3):939–947. https://doi.org/10.1210/en.2009-0657
Zhang BG, Du T, Ming-de Zang QC et al (2014) Androgen receptor promotes gastric cancer cell migration and invasion via AKT-phosphorylation dependent upregulation of matrix metalloproteinase 9. Oncotarget 5(21):10584. https://doi.org/10.18632/oncotarget.2513
Zhang Y, Wang Y, Wang J (2018) MicroRNA-584 inhibits cell proliferation and invasion in non-small cell lung cancer by directly targeting MTDH. Exp Ther Med 15(2):2203–2211. https://doi.org/10.3892/etm.2017.5624
Zhang Y, Wu Y, Jia Z et al (2020) Long non-coding RNA polymorphisms on 8q24 are associated with the prognosis of gastric cancer in a Chinese population. Peer J 8:e8600. https://doi.org/10.7717/peerj.8600
Zheng SL, Hsing AW, Sun J et al (2010) Association of 17 prostate cancer susceptibility loci with prostate cancer risk in Chinese men. Prostate 70(4):425–432. https://doi.org/10.1002/pros.21076
Zou Y, Qin X, Xiong H et al (2015) Apoptosis of human non-small-cell lung cancer A549 cells triggered by evodiamine through MTDH-dependent signalling pathway. Tumour Biol 36(7):5187–5193. https://doi.org/10.1007/s13277-015-3174-z
Acknowledgements
We are thankful to the Hon’ble Vice Chancellor, Presidency University Kolkata, India.
Funding
Financial support for this work was provided by the West Bengal State Govt. sponsored Presidency University FRPDF funds to Dr. Amlan Ghosh.
Author information
Authors and Affiliations
Contributions
AB (Abhishek Bardhan) collected and interpreted data and drafted the manuscript. AB (Anwesha Banerjee) did the study design and also drafted the manuscript. KB and DP did literature reviews, reviewed successive versions, and participated in their revision. AG did study design, data interpretation, and manuscript preparation. All the authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors state that they have no competing or financial interest.
Ethical approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bardhan, A., Banerjee, A., Basu, K. et al. PRNCR1: a long non-coding RNA with a pivotal oncogenic role in cancer. Hum Genet 141, 15–29 (2022). https://doi.org/10.1007/s00439-021-02396-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00439-021-02396-8