
Abstract
Background
Patients with cancer visit the emergency department often and have a high rate of admission compared to other patients. Admission rates by institution may vary widely, even after accounting for patient and hospital-specific characteristics.
Objectives
To review the variables that affect admission rates among patients with cancer in the emergency department.
Methods
We performed a secondary analysis of a prospective cohort study of patients with cancer at 18 emergency departments between March 1, 2016, and January 30, 2017, to examine differences in patient populations between hospitals with varying admission rates. We calculated the percentage admitted by hospital and used it to categorize hospitals into quartiles. We compared outcomes, patient demographics, and disease characteristics between the admission quartiles using linear or logistic regression.
Results
A total of 1075 patients were included. The median age of our sample was 64, and 51% of patients were female, 84% were white, and 13% were Black. Of the 1075 patients, 615 (57.2%) were admitted as inpatients with a range from 21.2 to 81.7% by hospital. Differences between admission quartiles were found for education, mode of arrival, and recent chemotherapy (p < 0.05). There were no significant differences among quartiles in age, gender, race, or ECOG score. We found significant difference between admission quartiles in 30-day emergency department revisits. Differences in readmission rates and mortality did not appear to be significant between the various quartiles.
Conclusions
In our study, we observed several differences among patients with cancer receiving care at hospitals with different admission rates. These included patients’ education level, mode of arrival, and whether they had received recent chemotherapy. Emergency Severity Index (ESI) score may have also contributed to admission rate variability. Further study into unmeasured factors influencing hospital admissions, such as local culture, resources, and pathways, could identify generalizable findings to reduce avoidable admissions and reduce variation among similar patients in different hospitals.
Similar content being viewed by others
Background
The number of patients with cancer is growing, driven by an increase in older adult patients with cancer. Investigators estimate that this population will grow from 15.5 million cancer survivors in 2015 to 26.1 million by 2040 [1]. In 2018 alone, patients with cancer in the United States (US) visited the emergency department (ED) approximately 4,884,000 times, representing 4.2% of all visits [2]. Hospitalizations with a principal or secondary diagnosis of cancer accounted for 10.5% of adult hospitalizations with a total cost of US $49.8 billion in 2017 [3]. In various studies, admission rates for patients with cancer in the ED are higher than for the general population, ranging from 58 to 62% while only being 16.3% for the general ED population [4,5,6,7]. Patients with cancer admitted through the ED are more acutely ill than others, with one institution reporting that 13% of patients with cancer who visited their ED were admitted to the ICU and 11% died during hospitalization [8].
In patients without cancer, condition-specific admission rates vary widely among EDs, even after adjusting for patient acuity and complexity [9,10,11,12,13,14]. Variability in admission rates has not been consistently linked to patient or hospital characteristics [15]. In an analysis of the ED component of the 2010 National Ambulatory Care Survey, whether a patient was admitted was dependent not just on their clinical factors but also on which ED evaluated them [16]. Because of this, prospective, multicenter studies to properly understand the variables that influence ED patient admission to the hospital are needed.
Founded in 2015, the National Cancer Institute (NCI) sponsored the Comprehensive Oncologic Emergencies Research Network (CONCERN) with the goal of identifying knowledge gaps and accelerating knowledge generation for patients with cancer requiring emergent care [17]. We previously described the disposition of patients with cancer in the ED to whether they received observation unit care and short stay and long stay inpatient admission [18]. Understanding the key drivers of ED admissions among patients with cancer can illuminate how to maximize healthcare quality through appropriate admissions and reducing unneeded resource utilization. Such knowledge may also improve patient comfort and satisfaction by preventing unnecessary hospital admissions and maximizing time at home, a patient-centered outcome that is increasingly noted to be important in cancer care [19]. In this secondary analysis of our prospective, multicenter observation study, we describe patient characteristics leading to inpatient admission to the hospital among patients with cancer visiting the ED [20].
Methods
Design and setting
We conducted a planned secondary analysis of the CONCERN data obtained between March 1, 2016, and January 30, 2017, to examine differences in patient populations between hospitals with varying admission rates. The percent admitted by hospital was calculated and used to categorize hospitals into quartiles. We previously published the protocol for this 18-site, prospective observational cohort study [20]. This study included adults ≥ 18 years of age with active cancer defined as (1) antineoplastic therapy within the past 12 months, (2) previously diagnosed or emergency physician-diagnosed cancer recurrence or metastasis, or (3) cancer-related symptoms. Exclusion criteria included pregnancy, incarceration, psychiatric chief complaint, chief complaint due to trauma, non-English speaking, previous enrollment in this same study, or being too ill or otherwise unable to participate in survey administration. The 18 sites were primarily urban academic EDs, all of which were affiliated with centers that provide comprehensive cancer care. Thirteen of the sites are affiliated with NCI-designated comprehensive cancer centers. Each participating site’s institutional review board approved all study procedures.
Data collection
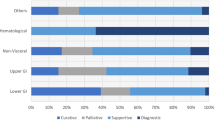
Trained research personnel approached patients in the ED, obtained informed consent, and administered the study questionnaire. Study personnel then conducted a chart review to identify patients who revisited the ED over the subsequent 30 days. Collected information included demographics, cancer type and status, medical history, current treatments and medications, functional status, symptom burden, palliative/hospice care utilization, clinical data including ED lab tests, ED disposition, hospital use/length of stay, Eastern Cooperative Group performance status (EGOG), Functional Assessment of Cancer Therapy-General Measure (FACT-G7), Condensed Memorial Symptom Assessment Scale (CMSAS), and up to four ED diagnoses using the International Statistical Classification of Diseases and Related Health Problems 10th Revision [21,22,23]. We grouped International Classification of Diseases-10 (ICD-10) codes using the Clinical Classifications Software (CCS) to explore the most common themes of conditions managed in each setting [24]. Chart review data included comorbidities sufficient to calculate the Charlson Comorbidity Index (CCI) [25].
We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines [26] and have previously published a description of the missing values and interrater reliability [27].
Outcome measures
We accessed key patient demographic and health history items (e.g., age, sex, cancer type), ED and hospital length of stay (LOS) and diagnoses, and initial ED disposition. The primary outcomes were the overall and department-specific inpatient admission rates. Secondary outcomes included the 30-day readmission rate, the 30-day ED revisit rate, and the 30-day mortality rate.
Statistical analysis
The percent of hospital admission was calculated for each center, and the EDs were grouped based on the data distribution in order to partition centers into quartiles by admission rate.
Descriptive statistics were used to characterize the demographic and clinical characteristics of the study population overall and by quartile of readmission. Characteristics between the quartiles were compared using univariate logistic regression for dichotomous variables or univariate linear regression for continuous variables. Each model included the ED to account for clustering unless small numbers prohibited clustering. Each outcome (admitted to hospital for > 24 h within 30 days, admitted to hospital for > 24 h within 30 days OR died within 30 days, return to ED within 30 days, and 30-day mortality) was compared between the quartiles using univariate logistic regression. Those with unknown mortality were set to missing prior to comparison. SAS 9.4 (SAS Institute, Inc., Cary, NC, USA) and Stata 16.1 (StataCorp LLC, College Station, TX, USA) were used in the analyses. We considered a p-value of 0.05 statistically significant for all analyses.
Results
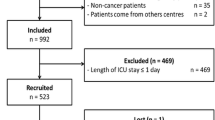
We included 1051 patients from 18 participating EDs. The median age was 64. Females comprised 51% of patients, 84% of patients were white, 13% were Black/African American, and 7% were Hispanic or Latino (see Table 2). The top five diagnoses and the percent of patients that presented with these diagnoses were (1) abdominal and pelvic pain (9.3%), (2) fever (8.1%), (3) abnormalities of breathing (7.2%), (4) nausea and vomiting (5.6%), and (5) pain in throat and chest (4.7%) [20].
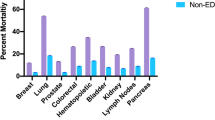
Table 1 describes the site enrollment characteristics. The total admission rate in our sample was 58.5% (n = 615) with the unadjusted admission rate among the individual EDs ranging from 21.2 to 81.7%. We partitioned the EDs into quartiles based on natural groups in the admission rate distribution. The admission rates of each quartile were Q1 21–38%, Q2 47–56%, Q3 60–66%, and Q4 69–82% (see Table 1). The baseline ED admission rate for all diagnoses (including non-cancer) at each site was collected and was Q1 30%, Q2 20%, Q3 30%, and Q4 30%. The overall readmission rate within 30 days ranged from 0 to 43.1%. There was no correlation between the initial ED admission rate and the readmission rate (Fig. 1). A minority of the centers were not NCI-designated cancer centers (n = 6) and were distributed across Q2, Q3. and Q4.

Initial admission and 30-day readmission rates by site. The shading indicates quartiles defined by initial admission: Q1 21–38% (yellow), Q2 47–56% (green), Q3 60–66% (blue), and Q4 69–82% (orange)
Patient characteristics by admission rate quartile are presented in Table 2. There were no significant differences among quartiles in age, gender, race, marital status, ECOG score, or ED arrival day. Sunday to Thursday was compared to Friday and Saturday as there is generally less outpatient follow-up available on Saturday and Sunday for patients discharged from the ED. Although the Emergency Severity Index (ESI) data was not documented in 17% (n = 42) of patients in Q1, there appeared to be a higher percentage of patients with ESI 1 and 2 in the higher admission EDs. In order to test this, we attributed all the undocumented or missing ESI data from Q1 into category ESI 1 or 2. This still showed a lower number of ESI scores of 1 or 2 present in Q1 (Q1 33.9% [n = 86], Q2 32.9% [n = 52], Q3 46% [n = 161] and Q4 66.5% [n = 208], p < 0.001). Q1 had a higher percentage of patients with a bachelor’s degree (Q1 55% [n = 137] vs. Q4 35% [n = 106], p < 0.01). Q4 had a higher rate of patients arriving by private vehicle (Q4 70% [n = 218] vs. Q1 27% [n = 69], Q2 49% [n = 77], Q3 32% [n = 111], p < 0.001) though this is difficult to analyze due to the large number of patients who either had undocumented or missing data as a mode of arrival (Q1 50% [n = 125], Q2 32% [n = 51], Q3 41% [n = 143], Q4 8% [n = 26]).
We illustrate cancer type and treatment grouped by admission quartile in Table 3. The use of traditional chemotherapy was lower in Q1 than in other groups (Q1 39% [n = 99] vs. Q2 59% [n = 83], Q3 41% [n = 142], Q4 55% [n = 171], p = 0.001) as was the use of radiotherapy (Q1 7% [n = 17] vs. Q2 14% [n = 22] vs 9% [n = 30] vs. 12% [n = 39], p = 0.004). There was no difference found between solid tumors and hematologic malignancies. Table 4 details the symptoms and symptom treatment by admission quartile. The use of long-acting opiates was higher in Q4 than in the other quartiles (Q4 13% [n = 40] vs. Q1 5% [n = 13], Q2 1% [n = 2], and Q3 6% [n = 21]. There was no significant difference in quartiles in terms of the presence of fever, pain, nausea, or shortness of breath.
We show 30-day readmission, 30-day ED revisits, and 30-day mortality by quartile in Table 5. Thirty-day ED revisits were higher in Q3 and Q4 than in Q1 and Q2 (Q4 28% [n = 88}, Q3 29% [n = 100], Q2 25% [n = 25%], Q1 23% [n = 59], p < 0.001). There was no significant difference between 30-day readmission and 30-day mortality in the different quartiles.
Discussion
In this secondary analysis of CONCERN’s prior prospective study of patients with cancer visiting EDs, we found a wide variation in admission rates among the participating sites. Various factors may have contributed to this finding. Variability in patient severity among the participating sites, as measured by ESI, may have contributed to admission rate variability. ECOG score did not appear to factor into this variation. Previous studies show that ESI predicts patient disposition in the ED, and Adler et al. previously demonstrated that ESI was predictive of patient disposition to outpatient or hospital care in this sample as well [28,29,30]. Future studies regarding ED admission rate variability could consider the use of ESI as a variable.
There were other differences in patient factors between the different admission rate quartiles in our analysis. The first was education level. Patients from Q1 EDs were more likely to have a bachelor’s degree or higher than those from Q3 and Q4 hospitals. One study showed that lower education levels in patients with cancer had an OR of 1.92 for having at least one symptomatic visit to the ED or for hospital admission [31]. In another qualitative study, physicians frequently changed management plans based on their patients’ socioeconomic status in an effort to enhance outcomes [32]. Other studies have also linked health literacy, low educational levels, and low socioeconomic status to higher ED utilization and hospital admission rates [33,34,35,36]. Perhaps patients with higher education levels are better able to advocate for themselves, or they may have access to better support at home such as home nursing or fewer barriers to access to care. Mode of transportation was also statistically significant in our study. Patients arriving by private vehicle was higher in Q4 than in the other quartiles. This may have been due to the locations of the individual hospitals in areas with high versus low utilization of public transportation or with different rates of private vehicle ownership. Unfortunately, the categories “other” and “unknown/not documented” do not allow sufficient analysis into the alternative modes of transportation such as public transportation, taxi, and rideshare, which could provide better insight into this difference.
Q4 had the highest percentage of patients receiving traditional chemotherapy. This was expected due to the high rate of complications among patients receiving traditional chemotherapy, such as infections, anemia, nausea, vomiting, and dehydration that can lead to admission [37]. Additionally, there was a higher percentage of patients using long-acting opiates at home in Q4. Patients taking long-acting opiates may have pain that is more difficult to control and fewer outpatient options available, hence requiring admission for symptom control. There also may have been unmeasured differences between study sites that led to this finding, such as opioid prescribing practices and other socioeconomic factors, such as the degree of family support.
The variability in admission rates between EDs did not appear to affect the 30-day readmission rate. There was no significant difference between the ED quartile groups in the 30-day readmission rate or the 30-day mortality rate. On the other hand, ED 30-day revisits were lower in Q1 and Q2 than in Q3 and Q4. These findings imply that a lower initial admission rate may not necessarily lead to subsequent ED visits and hospital revisits. One possible explanation for this may have been lower patient severity in the EDs with lower admission rates. It may also be due to improved outpatient algorithms or coordination of care by those respective sites in treating their patient population. These results are analogous to other studies in other patient populations that have demonstrated that variations in ED disposition generally do not impact the treatment plan nor patient outcomes [38, 39].
There are several limitations to our study. This study includes patients from mostly large, urban academic medical centers, and therefore, not all these results are generalizable to the overall population of EDs caring for patients with cancer. As this study only included patients visiting the CONCERN group EDs, some of the patients may have had ED revisits and readmissions at other hospitals outside of the study. While our dataset included the ESI and CCI, some institutions did not have all the data to compute those individual values. As such, we were unable to use these variables to risk adjust, and risk-adjust adjusting may have demonstrated variation not attributable to patient severity. Likewise, we were unable to compare admission rates based on ED diagnosis as the number of patients within each diagnosis grouping was too small to analyze [20]. Analyses of these data may have yielded further insight into differing ED practices in managing individual diagnoses. In addition, we did not have sufficient power to analyze this data set by hospital variables/characteristics. It would be interesting to determine if hospital characteristics, e.g., visit volume, rural vs urban, and academic vs non-academic, contribute to this variation. The only two standalone cancer hospitals with a closed ED in our study were in Q1 and Q2, suggesting there may have been more standardized protocols for patients at these institutions and improved coordination of care and outpatient follow-up.
Approximately, 7% of approached patients in this study were “too ill or otherwise unable to participate,” accounting for roughly 21% of ineligible patients. The exclusion of patients too ill to participate may have underestimated hospital admission rates, hospital revisit rates, readmission rates, and 30-day mortality. Past research suggests that emergency physicians vary significantly in the decisions they make for treating patients with common, low-mortality conditions such as chest pain without clear evidence of acute myocardial infarction, soft tissue infections, urinary tract infections, asthma, and COPD [40]. Meanwhile, there is little variation in treatment decisions for high-risk conditions such as confirmed acute myocardial infarction, sepsis, or kidney failure [41]. It is possible that by excluding patients too ill to participate, our study highlighted a population of patients subject to physician discretion while excluding a population with little variation in care. Non-English-speaking patients were also excluded from this study and comprised approximately 6% of those assessed for eligibility and 18% of those deemed ineligible. This may have skewed admission rates depending on the individual site’s baseline population.
Conclusions
Overall, our study showed variations in ED admission rates among the different sites in this study. Some factors that appear to have contributed to this may have been patient severity, patient education level, recent exposure to chemotherapy, and the use of long-acting opiates. There were fewer 30-day ED revisits in the lower admission rate hospitals. Differences in readmission rates and mortality were no different between EDs with high and low admission rates. Further study into the practices, cultures, and supports that allow for lower admission rates in certain EDs is warranted. Broad implementation of those practices could lead to potential benefits such as substantial cost savings for the healthcare system and increased patient satisfaction.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from CONCERN on reasonable request. https://epi.grants.cancer.gov/concern/#con.
References
Bluethmann SM, Mariotto AB, Rowland JH. Anticipating the “silver tsunami”: prevalence trajectories and comorbidity burden among older cancer survivors in the United States. Cancer Epidemiol Biomarkers Prev. 2016;25(7):1029–36.
Cairns C, Kang K, Santo L. National Hospital Ambulatory Medical Care Survey: 2018 emergency department summary tables. Available from: https://www.cdc.gov/nchs/data/nhamcs/web_tables/2018_ed_web_tables-508.pdf.
Roemer M. Cancer-Related Hospitalizations for Adults, 2017. 2021 Jan 26. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville: Agency for Healthcare Research and Quality (US); 2006. Statistical Brief #270. PMID: 33683837.
Rivera DR, Gallicchio L, Brown J, Liu B, Kyriacou DN, Shelburne N. Trends in adult cancer-related emergency department utilization: an analysis of data from the nationwide emergency department sample. JAMA Oncol. 2017;3(10): e172450.
Mayer DK, Travers D, Wyss A, Leak A, Waller A. Why do patients with cancer visit emergency departments? Results of a 2008 population study in North Carolina. J Clin Oncol. 2011;29(19):2683–8.
Vandyk AD, Harrison MB, Macartney G, Ross-White A, Stacey D. Emergency department visits for symptoms experienced by oncology patients: a systematic review. Support Care Cancer. 2012;20(8):1589–99.
Schuur JD, Venkatesh AK. The growing role of emergency departments in hospital admissions. N Engl J Med. 2012;367(5):391–3.
Elsayem AF, Merriman KW, Gonzalez CE, Yeung SC, Chaftari PS, Reyes-Gibby C, et al. Presenting symptoms in the emergency department as predictors of intensive care unit admissions and hospital mortality in a comprehensive cancer center. J Oncol Pract. 2016;12(5):e554–63.
Smulowitz PB, O’Malley AJ, McWilliams JM, Zaborski L, Landon BE. Variation in Rates of hospital admission from the emergency department among Medicare patients at the regional, hospital, and physician levels. Ann Emerg Med. 2021;78(4):474–83.
Abualenain J, Frohna WJ, Shesser R, Ding R, Smith M, Pines JM. Emergency department physician-level and hospital-level variation in admission rates. Ann Emerg Med. 2013;61(6):638–43.
Khojah I, Li S, Luo Q, Davis G, Galarraga JE, Granovsky M, et al. The relative contribution of provider and ED-level factors to variation among the top 15 reasons for ED admission. Am J Emerg Med. 2017;35(9):1291–7.
Shoff C, Caines K, Pines JM. Geographic variation in predictors of ED admission rates in U.S. Medicare fee-for-service beneficiaries. Am J Emerg Med. 2019;37(6):1078–84.
Perrin JM, Homer CJ, Berwick DM, Woolf AD, Freeman JL, Wennberg JE. Variations in rates of hospitalization of children in three urban communities. N Engl J Med. 1989;320(18):1183–7.
Mueller EL, Jacob SA, Cochrane AR, Carroll AE, Bennett WE Jr. Variation in hospital admission from the emergency department for children with cancer: a Pediatric Health Information System study. Pediatr Blood Cancer. 2020;67(6): e28140.
Venkatesh AK, Dai Y, Ross JS, Schuur JD, Capp R, Krumholz HM. Variation in US hospital emergency department admission rates by clinical condition. Med Care. 2015;53(3):237–44.
Capp R, Ross JS, Fox JP, Wang Y, Desai MM, Venkatesh AK, et al. Hospital variation in risk-standardized hospital admission rates from US EDs among adults. Am J Emerg Med. 2014;32(8):837–43.
National Cancer Institute Division of Cancer Control and Population Sciences. Comprehensive Oncologic Emergencies Research Network (CONCERN). Available from: https://epi.grants.cancer.gov/concern/. Accessed 23 Mar 2022.
Klotz AD, Caterino JM, Durham D, Felipe Rico J, Pallin DJ, Grudzen CR, et al. Observation unit use among patients with cancer following emergency department visits: results of a multicenter prospective cohort from CONCERN. Acad Emerg Med. 2022;29(2):174–83.
Gupta A, O'Callaghan CJ, Zhu L, Jonker DJ, Wong RPW, Colwell B, et al. Evaluating the time toxicity of cancer treatment in the CCTG CO.17 trial. JCO Oncol Pract. 2023;19(6):e859-e66.
Caterino JM, Adler D, Durham DD, Yeung SJ, Hudson MF, Bastani A, et al. Analysis of diagnoses, symptoms, medications, and admissions among patients with cancer presenting to emergency departments. JAMA Netw Open. 2019;2(3): e190979.
Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–55.
Yanez B, Pearman T, Lis CG, Beaumont JL, Cella D. The FACT-G7: a rapid version of the functional assessment of cancer therapy-general (FACT-G) for monitoring symptoms and concerns in oncology practice and research. Ann Oncol. 2013;24(4):1073–8.
Chang VT, Hwang SS, Kasimis B, Thaler HT. Shorter symptom assessment instruments: the Condensed Memorial Symptom Assessment Scale (CMSAS). Cancer Invest. 2004;22(4):526–36.
AHRQ. HCUP Clinical Classifications Software (CCS) for ICD-10-CM. In: Agency for Healthcare Research and Quality, editor. HCUP Clinical Classifications Software (CCS) for ICD-10-CM. Rockville: 2018. www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp.
Charlson M, TPS, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47:1245–51.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting of observational studies. Der Internist. 2008;49(6):688–93.
Adler D, Abar B, Durham DD, Bastani A, Bernstein SL, Baugh CW, et al. Validation of the Emergency Severity Index (Version 4) for the triage of adult emergency department patients with active cancer. J Emerg Med. 2019;57(3):354–61.
Wuerz RC, Milne LW, Eitel DR, Travers D, Gilboy N. Reliability and validity of a new five-level triage instrument. Acad Emerg Med Off J Soc Acad Emerg Med. 2000;7(3):236–42.
Tanabe P, Gimbel R, Yarnold PR, Kyriacou DN, Adams JG. Reliability and validity of scores on the Emergency Severity Index version 3. Acad Emerg Med. 2004;11(1):59–65.
Eitel DR, Travers DA, Rosenau AM, Gilboy N, Wuerz RC. The emergency severity index triage algorithm version 2 is reliable and valid. Acad Emerg Med. 2003;10(10):1070–80.
Siefert ML, Bonquist TM, Berry DL, Hong F. Symptom-related emergency department visits and hospital admissions during ambulatory cancer treatment. J Commun Support Oncol. 2015;13(5):188–94.
Bernheim SM, Ross JS, Krumholz HM, Bradley EH. Influence of patients’ socioeconomic status on clinical management decisions: a qualitative study. Ann Fam Med. 2008;6(1):53–9.
Williams MV, Baker DW, Parker RM, Nurss JR. Relationship of functional health literacy to patients’ knowledge of their chronic disease. A study of patients with hypertension and diabetes. Arch Intern Med. 1998;158(2):166–72.
Baker DW, Gazmararian JA, Williams MV, Scott T, Parker RM, Green D, et al. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am J Public Health. 2002;92(8):1278–83.
Olsen F, Balteskard L, Uleberg B, Jacobsen BK, Heuch I, Moen A. Impact of parents’ education on variation in hospital admissions for children: a population-based cohort study. BMJ Open. 2021;11(6): e046656.
Filc D, Davidovich N, Novack L, Balicer RD. Is socioeconomic status associated with utilization of health care services in a single-payer universal health care system? Int J Equity Health. 2014;13:115.
Pittman NM, Hopman WM, Mates M. Emergency room visits and hospital admission rates after curative chemotherapy for breast cancer. J Oncol Pract. 2015;11(2):120–5.
Admon AJ, Seymour CW, Gershengorn HB, Wunsch H, Cooke CR. Hospital-level variation in ICU admission and critical care procedures for patients hospitalized for pulmonary embolism. Chest. 2014;146(6):1452–61.
Vinson DR, Ballard DW, Huang J, Reed ME, Lin JS, Kene MV, et al. Outpatient management of emergency department patients with acute pulmonary embolism: variation, patient characteristics, and outcomes. Ann Emerg Med. 2018;72(1):62–72 e3.
Busby J, Purdy S, Hollingworth W. A systematic review of the magnitude and cause of geographic variation in unplanned hospital admission rates and length of stay for ambulatory care sensitive conditions. BMC Health Serv Res. 2015;15:324.
Sabbatini AK, Nallamothu BK, Kocher KE. Reducing variation in hospital admissions from the emergency department for low-mortality conditions may produce savings. Health Aff (Millwood). 2014;33(9):1655-63. https://doi.org/10.1377/hlthaff.2013.1318.
Acknowledgements
N/A.
Funding
None.
Author information
Authors and Affiliations
Contributions
All authors conceived the study. JFR and JMC were responsible for data acquisition. JAS performed the statistical analysis working closely with JFR, JMC, and CWB. JFR, CWB, and JAS drafted the manuscript, and all authors contributed substantially to its revision. JFR, JMC, CWB, and JAS designed the statistical analysis. JFR takes responsibility for the paper as a whole.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Each participating site’s institutional review board approved all study procedures.
Consent for publication
N/A.
Competing interests
Dr. Rico has funding from Novartis, Global Blood Therapeutics, and Daichi-Sancho. Dr. Yeung was a member of an expert panel for Celgene, Inc. Dr. Yeung had funding support from Bristol-Myers Squibb, Inc. and Depomed, Inc. (now Assertio Therapeutics, Inc.). Dr. Bischof receives funding support from Abbott, Beckman Coulter, CalciMedica, Comprehensive Research Associates, and RCE. Dr. Baugh is a speaker for Roche Diagnostics; advisor for Lucia Health Guidelines; advisory board member for Roche Diagnostics, Bristol Myers Squib, InCarda Therapeutics, Salix Pharmaceuticals, and AcelRx Pharmaceuticals; consultant/grant recipient for Visby Medical; and consultant for Torus Biosystems. The other authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rico, J.F., Caterino, J.M., Stephens, J.A. et al. Variables associated with admission rates among cancer patients presenting to emergency departments: a CONCERN group study. Emerg Cancer Care 2, 7 (2023). https://doi.org/10.1186/s44201-023-00022-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44201-023-00022-z