
Abstract
Background
The authors present a case of cervical myelopathy and radiculopathy in the setting of multiple Klippel-Feil syndrome abnormalities treated surgically with a single-level C3–C4 anterior cervical discectomy and fusion. We discuss the clinical presentation, radiographic findings, and various treatment options for cervical spine abnormalities in Klippel-Feil syndrome.
Case Presentation
This 22-year-old female with Klippel-Feil syndrome presented with intermittent neck pain, left upper extremity weakness, and paresthesias. Preoperative MRI, CT, and X-rays of the cervical spine revealed anterolisthesis at C3/4 with unstable movement on flexion and extension imaging. In addition, there were multiple segmental fusion abnormalities including hemivertebrae and other congenital fusion abnormalities. A C3–C4 anterior cervical discectomy and fusion was performed with intervertebral disc spacer. Adequate decompression was achieved with postoperative resolution of the patient’s symptoms and improvement in neurological exam.
Conclusions
Single-level anterior cervical discectomy and fusion can be utilized for treatment of cervical myelopathy and radiculopathy in the setting of multiple congenital Klippel-Feil syndrome abnormalities.
Similar content being viewed by others


Background
Klippel-Feil syndrome (KFS) is a rare disorder characterized by the congenital fusion of cervical vertebrae [1–3] and affects anywhere from 1 in 40,000 to 50,000 live births [4, 20]. KFS is a heterogeneous condition presenting with an array of skeletal/extra-skeletal manifestations [1, 4–9] and is best known for the classical syndromic triad, found in approximately 50 % of patients, consisting of short neck, low posterior hairline, and restricted range of cervical motion [4]. Traditionally, KFS was believed to clinically manifest in adulthood due to the delayed affects of congenital vertebral fusion. However, more recently, studies have found that up to 50 % of young KFS patients experience cervical-spine-related symptoms [1, 10, 11]. Given the heterogeneity of phenotypic expression, the prevalence of KFS may in fact be higher than has previously been reported [1, 4, 7].
The abnormal fusion of cervical vertebrae predisposes those with KFS to neurologic injury due to altered spinal biomechanics, producing an increased likelihood of hypermobility, spondylolisthesis, degenerative changes, and spinal stenosis [12–14]. Early recognition and diagnosis of KFS is required in order to provide precautionary guidelines and proper nonsurgical or surgical management. Here we present a case of cervical myelopathy and radiculopathy in a 22-year-old with Klippel-Feil syndrome with hypermobility at C3/4 treated surgically with an anterior cervical discectomy and fusion.
Case presentation
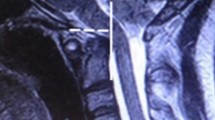
A 22-year-old female with a history of Klippel-Feil syndrome was referred to our neurosurgical clinic for evaluation of intermittent left-sided neck pain and forearm paresthesias. Over the past year and a half, she had experienced rare left upper extremity paresthesias, but her symptoms acutely worsened while walking a dog that pulled abruptly on the leash in her left hand. Following this incident, she experienced transient left upper extremity paresthesias, weakness, and occasional neck pain that worsened with leftward axial rotation of the neck. On physical examination, she was found to have a left Hoffman’s sign but was otherwise neurologically intact with full strength in all four extremities. MR imaging was obtained, which demonstrated a cervical kyphotic deformity, central canal stenosis with cord signal changes, and foraminal narrowing with right disc protrusion at the level of C3–C4 (Fig. 1). CT revealed multiple segmental abnormalities with fusion anteriorly of the atlas and the occipital condyles, along with fusions at C1–C2, C2–C3, C6–C7, C7–T1, and T1–T2. A left T1 hemivertebra, rudimentary right C7 cervical rib, and fusion of right T1 and T2 ribs were also noted (Fig. 2). Flexion and extension films showed hypermobility with approximately 4 mm of anterolisthesis of C3 on C4 (Fig. 3).

Preoperative MRI of the cervical spine without contrast demonstrates a kyphotic deformity, congenital narrowing of the spinal canal at C3–C4 and C5–C6 with compression of the thecal sac, and mild indentation of the anterior cord

Preoperative CT of the cervical spine without contrast reveals segmentation abnormalities and fusion of multiple cervical and thoracic vertebrae, including fusion of C1–C2 (dens), C2–C3, C5–C6, C6–C7, C7–T1, and T1–T2

Preoperative flexion (a) and extension (b) films reveal hypermobility at C3–C4. There is also evidence of 2-mm retrolisthesis at C5–6
Surgical technique
The patient underwent surgical treatment with an anterior cervical discectomy and fusion at C3–C4. The patient was positioned supine on the operating table and placed under general anesthesia. Traction was not utilized during the operation. The initial anterior surgical exposure was performed, undercutting the platysma in the cephalad and caudad directions to expose the underlying strap muscles medially and the sternocleidomastoid laterally. A nonlipped Cloward was used to dissect the strap muscles medially. The dissection plain was then carried downward towards the anterior longitudinal ligament, identifying the carotid artery laterally. The appropriate surgical level of C3–C4 was confirmed with intraoperative fluoroscopic imaging.
The microdissection portion of the case was performed under operative microscopy. A 15 blade was used to incise the disc space, and the disc material was removed using pituitary forceps. The superior C4 and inferior C3 cartilaginous endplates were removed with straight and upgoing curettes. A high-speed pneumatic drill was used to drill down the uncovertebral joints and posterior osteophyte. Kerrison punches assisted in decompression of the dura and complete removal of the posterior osteophyte. Exploration with a blunt nerve hook confirmed foraminal decompression bilaterally.
A VG2 size 6 lordotic allograft was malleted into the C3–C4 disc space. A size 14 skyline plate was positioned and drilled into place with four 14-mm screws, which were locked and tightened to the manufacturer’s specifications. Cam locks were used to confirm proper placement, followed by intraoperative fluoroscopic imaging (Fig. 4). The surgical field was then irrigated with bacitracin-laden solution, and a Hemovac drain was positioned and secured in place with nylon suture. Platysmal and dermal closure was achieved with interrupted 3-0 vicryl sutures, and the epidermis was closed with a 4-0 subcuticular monocryl. An Aspen collar was positioned for cervical immobilization, and the patient was extubated and transferred to the PACU in stable condition. Postoperatively, the patient was maintained in a hard collar for 6 weeks and experienced resolution of her symptoms with improvement in neurological exam. At 4 months follow-up, the patient reported resolution of all neck pain both without movement and with neck rotation. In addition, she reported resolution of the left upper extremity paresthesias and weakness. On examination, she was neurologically intact. Follow-up flexion and extension imaging displayed minimal movement at C5/6, and the patient remains asymptomatic.

Intraoperative fluoroscopic lateral view of the cervical spine demonstrates an anterior spinal fusion of C3–C4 with intervertebral disc spacer at this level
Discussion
Klippel-Feil syndrome (KFS) is a complex congenital disorder of improper fusion of at least two cervical vertebrae. The classical clinical triad of KFS, although found in 50 % or less of patients [4, 15], is comprised of a short neck, low posterior hairline, and limited range of cervical motion. Since its first description in 1912 [4], a wide range of skeletal and extra-skeletal manifestations have been reported in association with KFS, including scoliosis, cardiac abnormalities, hearing problems, split cervical cord, and Sprengel’s deformity, among others [4, 8, 16–19]. The incidence of KFS has been estimated to be anywhere from 1 in 40,000 to 50,000 live births [4, 20], with some studies suggesting a slight female predominance [13, 18, 21, 22]. While a number of genes have been described in association with KFS, the exact etiology remains unknown [20, 23].
The clinical presentations of KFS are diverse, ranging from asymptomatic [24] to signs of serious injury, such as long tract signs, sensory abnormalities, cavus feet, asymmetric reflexes, sensory abnormalities, altered cerebellar function, and pain [13]. In a study by Gray et al., 65 % of patients developed clinical symptoms before the age of 30 years old, while 20 % became symptomatic before the age of 5 [25]. Despite these findings, there have been reports of patients remaining asymptomatic for up to 40 years [24]. In a retrospective radiographic and clinical review by Samartzis et al., 33 % of patients displayed cervical-spine-related symptoms while 13.3 % were myelopathic. Interestingly, no statistical significance was noted between the presence of symptoms and cervical scoliosis or coronal cervical alignment [1]. A similar radiographic and clinical review by Guille et al. found that, among 22 KFS patients, myelopathic and radiculopathic symptoms developed at a mean age of 17.9 years, with the onset of cervical-spine-related symptoms occurring earlier in myelopathic patients (10.0 years old). Among this group, 72.7 % were noted as having cervical disc protrusions [22].
Since the original radiographic classification of KFS by Feil in 1919 [3], a wide range of radiographic findings have been reported, such as narrowing of the spinal cord, widening of the spinal canal, osteophyte or disc protrusion, ligamentum hypertrophy, spinal stenosis, subluxation, and spondylolisthesis [13, 14, 26]. The most common fused cervical levels in KFS are C2–C3 (71.0 %) followed by C5–C6 (67.7 %), C6–C7 (67.6 %), and C3–C4 (29.0 %), with the mean number of total fused segments ranging from 3.5 to 3.7 [1, 21]. Ulmer et al. also reported a 15.8 % incidence of disc herniation in adult KFS patients [15], while cervical stenosis has been found in approximately 25 %, at both fused and nonfused levels [10].
In 1995, Guille et al. reviewed the radiographic findings of 24 KFS patients at least 25 years or older and divided them into three groups based on his findings. Type I (54.5 %) consisted of a single congenitally fused cervical segment; type II (18.2 %) multiple noncontiguous, congenitally fused segments; and type III (27.3 %) multiple contiguous, congenitally fused cervical segments [22]. Other authors have utilized a similar classification scheme to evaluate the pediatric population, with the following findings: type I (25 %), type II (50 %), and type III (25 %). Axial neck symptoms are more often associated with type I fusions, while myelopathic and radicular symptoms are reportedly associated with Type II and Type III fusions [21].
MRI is the imaging modality of choice for evaluation of spinal cord abnormalities and is particularly useful for early diagnosis of KFS. MRI allows for assessment of soft tissue and provides contrast between the spinal cord and its surrounding structures. It may also reveal other spinal abnormalities such as Chiari I malformation, syringomyelia, myelomalacia, and diastematomyelia [15, 27]. In a report by Nguyen and Tyrrel, 53.8 % of patients displayed a wasp-waist sign on MRI, serving as a valuable sign for diagnosis [28]. In rare cases where MRI is contraindicated, CT myelography may be utilized. CT scan, on the other hand, provides optimal imaging of complex bony abnormalities, spinal instrumentation, and can be useful in surgical planning [27]. Other advanced imaging modalities, such as diffusion tensor imaging and fiber tracking, have been utilized in the experimental setting [29, 30].
Several authors have proposed theories behind the development of hypermobility, degenerative changes, spinal stenosis, spondylolisthesis, and neurologic injury in KFS patients, most often attributed to altered spinal biomechanics as a result of improper vertebral fusion. When compared to the control population, Pizzutillo et al. found the KFS patients exhibited increased motion across each open interspace in the upper cervical spine, predisposing one to increased spinal degeneration and neurologic injury [13]. In accordance with this biomechanical explanation, three particularly unstable fusion patterns have been described, including the following: fusion of C2–C3 with occipitalization of the atlas, a long fusion with an abnormal occipitocervical junction, and a single open space between two fused segments [4]. The patient presented in this case possesses an unstable combination of the aforementioned fusion patterns, including an abnormal occipitocervical junction with fusion of C2–C3, and a long fusion in addition to other cervical and upper thoracic abnormalities. Flexion and extension films were crucial for a thorough evaluation of the cervical spine in this case, revealing hypermobility at C3–C4. The patient’s symptoms resolved following surgery with evidence of an asymptomatic mild hypermobility at C5/6 with 3 mm of retrolisthesis on flexion and extension imaging.
Treatment approaches and timing of surgical intervention for KFS has been debated in the literature. The role of prophylactic surgery for spinal stabilization remains controversial and, as some authors claim, is not indicated in cases of hypermobility without neurological deficit [24]. In most cases, KFS patients can be treated symptomatically. A study by Theiss et al. found that 22 % of patients with congenital scoliosis and KFS developed cervical or cervical-related symptoms, with only two of those patients requiring surgery [31]. The conservative treatment of radiculopathy should be aggressive, reserving surgery for patients with refractory radiculopathy and/or myelopathy.
Surgeons should be aware of individual patient characteristics that may predispose to future neurological injury, such as a type II or type III fusion. Additionally, the risk of developing neuropathy is higher in patients with congenital cervical fusion and underlying congenital cervical stenosis [32], as noted by Theiss et al. who found a significantly greater incidence of upper extremity pain in these patients [31]. Early identification of KFS is necessary to minimize the risk for injury during routine daily activities or operative intervention. In cases of myelopathy, surgical intervention is required to potentially improve neurologic function and avoid further neurologic compromise.
Many factors must be taken into consideration when choosing a particular surgical approach including age, comorbidities, ventral vs. dorsal compression, disease focality, surgeon experience, and presence of axial pain or radiculopathy. Generally speaking, an adequate decompression of the nerve roots and spinal cord can be achieved in most cases of cervical spondylitic myelopathy using an anterior approach, with multiple discectomies being favored over corpectomy or discectomy-corpectomy hybrid approaches for multilevel disease [33]. Cervical corpectomy or laminectomy may be required for adequate decompression with extension of disease posteriorly. Discussion of specific surgical techniques for management of symptomatic KFS patients has primarily been limited to case reports [14, 32, 34–38]. In this particular case, an anterior cervical discectomy and fusion (ACDF) was chosen for treatment of single-level disease, as imaging demonstrated anterolisthesis and narrowing of the spinal canal at the level of the C3–C4 with a bulging disc. It was felt that an anterior approach would allow for adequate decompression and fusion, bearing in mind the potential for future failed arthroplasty due to abnormal congenital fusion [38].
Conclusions
Klippel-Feil syndrome (KFS) is a rare and heterogeneous condition with varying clinical manifestations. Individual patient factors should be taken into consideration when choosing a treatment approach for KFS. Various imaging modalities, including MRI, CT, and flexion/extension films of the cervical spine, are necessary for evaluation of cervical instability and extent of congenital deformity. In this particular case, a single-level ACDF was performed with success for treatment of cervical myelopathy and radiculopathy in the presence of multiple underlying congenital abnormalities.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
References
Samartzis D, Kalluri P, Herman J, Lubicky JP, Shen FH. Cervical scoliosis in the Klippel-Feil patient. Spine. 2011;36(23):E1501–8. doi:10.1097/BRS.0b013e31823145e4.
Klippel M, Feil A. Un cas d’absence des vertebres cervicales. Avec cage thoracique remontant jusqu’a la base du crane (cage thoraci- que cervicale). Nouv Iconog Salpetriere. 1912;25:223–50.
Feil A. L’absence et la diminuation des vertebres cervicales (etude cliniqueet pathogenique); le syndrome dereduction numerique cer- vicales. Theses de Paris; 1919.
Hensinger RN, Lang JE, MacEwen GD. Klippel-Feil syndrome. A constellation of associated anomalies. J Bone Joint Surg Am. 1974;56:1246–53.
Da Silva EO. Autosomal recessive Klippel-Feil syndrome. J Med Genet. 1982;19:130–4.
Juberg RC, Gershanik JJ. Cervical vertebral fusion (Klippel-Feil) syndrome with consanguineous parents. J Med Genet. 1976;13:246–9.
Van Kerckhoven MF, Fabry G. The Klippel-Feil syndrome: a constellation of deformities. Acta Orthop Belg. 1989;55:107–18.
Helmi C, Pruzansky S. Craniofacial and extracranial malformations in the Klippel-Feil syndrome. Cleft Palate J. 1980;17:65–88.
Samartzis D, Herman J, Lubicky JP, Shen FH. Sprengel’s deformity in Klippel-Feil syndrome. Spine. 2007;32(18):E512–6.
Ritterbusch JF, McGinty LD, Spar J, Orrison WW. Magnetic resonance imaging for stenosis and subluxation in Klippel-Feil syndrome. Spine. 1991;16(10 Suppl):S539–41.
Rouvreau P, Glorion C, Langlais J, Noury H, Pouliquen JC. Assessment and neurologic involvement of patients with cervical spine congenital synostosis as in Klippel-Feil syndrome: study of 19 cases. J Pediatr Orthop B. 1998;7(3):179–85.
Samartzis D, Lubicky JP, Herman J, Kalluri P, Shen FH. Symptomatic cervical disc herniation in a pediatric Klippel-Feil patient: the risk of neural injury associated with extensive congenitally fused vertebrae and a hypermobile segment. Spine. 2006;31(11):E335–8.
Pizzutillo PD, Woods M, Nicholson L, MacEwen GD. Risk factors in Klippel-Feil syndrome. Spine. 1994;19(18):2110–6.
Hall JE, Simmons ED, Danylchuk K, Barnes PD. Instability of the cervical spine and neurological involvement in Klippel-Feil syndrome. A case report. J Bone Joint Surg Am. 1990;72(3):460–2.
Ulmer JL, Elster AD, Ginsberg LE, Williams 3rd DW. Klippel-Feil syndrome: CT and MR of acquired and congenital abnormalities of cervical spine and cord. J Comput Assist Tomogr. 1993;17(2):215–24.
Samartzis D, Lubicky JP, Herman J, Shen FH. Faces of spine care: from the clinic and imaging suite. Klippel-Feil syndrome and associated abnormalities: the necessity for a multidisciplinary approach in patient management. Spine J. 2007;7(1):135–7.
Samartzis D, Lubicky JP, Herman J, Shen FH. Faces of spine care: from advanced imaging. Severe thoracic kyphoscoliosis in a Klippel-Feil patient with complete cervical spine fusion and deformity–primum non nocere. Spine J. 2006;6(6):723–4.
Thomsen MN, Schneider U, Weber M, Johannisson R, Niethard FU. Scoliosis and congenital anomalies associated with Klippel-Feil syndrome types I–III. Spine. 1997;22(4):396–401.
David KM, Copp AJ, Stevens JM, Hayward RD, Crockard HA. Split cervical spinal cord with Klippel-Feil syndrome: seven cases. Brain. 1996;119(Pt 6):1859–72.
Buonuomo PS, Macchiaiolo M, Colafati GS, Rana I, Tomà P, Gonfiantini MV, et al. Persistent neck pain in a girl: Klippel-Feil syndrome. Arch Dis Child. 2014;99(3):290–1. doi:10.1136/archdischild-2013-305203.
Samartzis D, Herman J, Lubickey JP, Shen FH. Classification of congenitally fused cervical patterns in Klippel-Feil patients. Spine. 2006;31(21):E798–804.
Guille JT, Miller A, Bowen JR, Forlin E, Caro PA. The natural history of Klippel-Feil syndrome: clinical, roentgenographic, and magnetic resonance imaging findings at adulthood. J Pediatr Orthop. 1995;15(5):617–26.
David KM, Thorogood PV, Stevens JM, Crockard HA. The dysmorphic cervical spine in Klippel-Feil syndrome: interpretations from developmental biology. Neurosurg Focus. 1999;6(6):e1.
Nagashima H, Morio Y, Teshima R. No neurological involvement for more than 40 years in Klippel-Feil syndrome with severe hypermobility of the upper cervical spine. Arch Orthop Trauma Surg. 2001;121:99–101.
Gray SW, Romaine CB, Skandalakis JE. Congenital fusion of the cervical vertebrae. Surg Gynecol Obstet. 1964;118:373–85.
Karasick D, Schweitzer ME, Vaccaro AR. The traumatized cervical spine in Klippel-Feil syndrome: imaging features. AJR Am J Roentgenol. 1998;170(1):85–8.
Laker SR, Concannon LG. Radiologic evaluation of the neck: a review of radiography, ultrasonography, computed tomography, magnetic resonance imaging, and other imaging modalities for neck pain. Phys Med Rehabil Clin N Am. 2011;22:411–28.
Nguyen VD, Tyrrel R. Klippel-Feil syndrome: patterns of bony fusion and wasp-waist sign. Skeletal Radiol. 1993;22(7):519–23.
Xiangshui M, Xiangjun C, Xiaoming Z, Qingshi Z, Yi C, Chuanqiang Q, et al. 3 T magnetic resonance diffusion tensor imaging and fibre tracking in cervical myelopathy. Clin Radiol. 2010;65(6):465–73.
Demir A, Ries M, Moonen CT, Vital JM, Dehais J, Arne P, et al. Diffusion-weighted MR imaging with apparent diffusion coefficient and apparent diffusion tensor maps in cervical spondylotic myelopathy. Radiology. 2003;229(1):37–43.
Theiss SM, Smith MD, Winter RB. The long term follow-up of patients with Klippel-Feil syndrome and congenital scoliosis. Spine. 1997;22(11):1219–22.
Prusick VR, Samberg LC, Wesolowski DP. Klippel-Feil syndrome associated with spinal stenosis. A case report. J Bone Joint Surg Am. 1985;67(1):161–4.
Shamji MF, Massicotte EM, Traynelis VC, Norvell DC, Hermsmeyer JT, Fehlings MG. Comparison of anterior surgical options for the treatment of multilevel cervical spondylotic myelopathy: a systematic review. Spine. 2013;38(22 Suppl 1):S195–209. doi:10.1097/BRS.0b013e3182a7eb27. Review.
Epstein NE, Epstein JA, Zilkha A. Traumatic myelopathy in a seventeen-year-old child with cervical spinal stenosis (without fracture or dislocation) and a C2-C3 Klippel-Feil fusion: a case report. Spine. 1984;9(4):344–7.
Herring JA, Bunnell WP. Instructional case: Klippel-Feil syndrome with neck pain. J Pediatr Orthop. 1989;9(3):343.
Holmes FC. Case report: Klippel-Feil syndrome in a cheerleader. Clin J Sport Med. 2007;17:154–6.
Matsumoto K, Wakahara K, Sumi H, Shimizu K. Central cord syndrome in patients with Klippel-Feil syndrome resulting from winter sports: report of 3 cases. Am J Sports Med. 2006;34(10):1685–9.
Papanastassiou ID, Baaj AA, Dakwar E, Eleraky M, Vrionis FD. Failure of cervical arthroplasty in a patient with adjacent segment disease associated with Klippel-Feil syndrome. Indian J Orthop. 2011;45(2):174–7. doi:10.4103/0019-5413.77139.
Acknowledgements
There was no funding source for this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AW collected the patient data and performed the primary writing of the manuscript. PD participated in the design and coordination of the study and assisted in the writing of the manuscript. AC participated in the design of the study and assisted with revisions of the manuscript. JS conceived the study and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wessell, A., DeRosa, P., Cherrick, A. et al. Cervical instability in Klippel-Feil syndrome: case report and review of the literature. Chin Neurosurg Jl 1, 6 (2015). https://doi.org/10.1186/s41016-015-0002-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41016-015-0002-7