
Abstract
Background
Immunocompromised (IC) patients are at higher risk of severe SARS-CoV-2 infection, morbidity, and mortality compared to the general population. They should be prioritized for primary prevention through vaccination. This study aimed to evaluate the efficacy of COVID-19 mRNA vaccines in IC patients through a systematic review and meta-analysis approach.
Method
PubMed-MEDLINE, Scopus, and Web of Science were searched for original articles reporting the immunogenicity of two doses of mRNA COVID-19 vaccines in adult patients with IC condition between June 1, 2020 and September 1, 2021. Meta-analysis was performed using either random or fixed effect according to the heterogeneity of the studies. Subgroup analysis was performed to identify potential sources of heterogeneity.
Results
A total of 26 studies on 3207 IC patients and 1726 healthy individuals were included. The risk of seroconversion in IC patients was 48% lower than those in controls (RR = 0.52 [0.42, 0.65]). IC patients with autoimmune conditions were 54%, and patients with malignancy were 42% more likely to have positive seroconversion than transplant recipients (P < 0.01). Subgroup meta-analysis based on the type of malignancy, revealed significantly higher proportion of positive seroconversion in solid organ compared to hematologic malignancies (RR = 0.88 [0.85, 0.92] vs. 0.61 [0.44, 0.86], P = 0.03). Subgroup meta-analysis based on type of transplantation (kidney vs. others) showed no statistically significant between-group difference of seroconversion (P = 0.55).
Conclusions
IC patients, especially transplant recipients, developed lower immunogenicity with two-dose of COVID-19 mRNA vaccines. Among patients with IC, those with autoimmune conditions and solid organ malignancies are mostly benefited from COVID-19 vaccination. Findings from this meta-analysis could aid healthcare policymakers in making decisions regarding the importance of the booster dose or more strict personal protections in the IC patients.
Similar content being viewed by others

Introduction
Immunocompromised (IC) patients include individuals with over-activation or suppression of the immune system due to primary disease or treatment regimens [1]. The most common conditions in this group are malignancies, inherited or acquired immunodeficiency diseases, autoimmune diseases, transplant recipients, and other conditions requiring long-term corticosteroid [1]. IC conditions are estimated to affect approximately 2.7% of United States adults [2]. Such patients are at higher risk of severe SARS-CoV-2 infection, extended hospitalization, intensive care admission, and mortality compared to the general population [3,4,5,6,7]. Besides, prolonged viral shedding and potential sources of novel SARS-CoV-2 variants in this population are also of particular importance [8,9,10]. Thus, IC patients should be prioritized for primary prevention through Coronavirus infectious disease 2019 (COVID-19) vaccination.
Global efforts have been taken to develop SARS-CoV-2 vaccines since the initiation of the current COVID-19 pandemic. The mRNA vaccines (i.e., mRNA-1273 and BNT162b2) are the most commonly approved vaccines worldwide which are utilized in different clinical trials on a global scale [11]. The overall efficacy and safety of COVID-19 vaccines in phase III trials were promising [12], sparking global hope toward ending the current outbreak. However, the application of COVID-19 vaccines in patients with impaired immune systems remains an ongoing subject of debate as they were excluded from the original trials [13, 14]. Due to either the primary disease or the immunosuppressive treatments, IC patients are more likely to show a weak or suboptimal immune response to COVID-19 vaccines, given previous studies on influenza vaccines [15]. Hence, real-world statistics regarding the efficacy of COVID-19 vaccines are required to provide physicians a better insight towards decision-making in this group of high-risk patients.
This study aimed to systematically review the literature and analyze the pooled effectiveness of COVID-19 vaccination in IC patients compared to healthy controls using meta-analysis. We also assessed the efficacy of mRNA vaccines in IC patients based on their etiological factors, including malignancy, transplantation, and autoimmune diseases.
Methods and materials
Protocol and literature search
This systematic review and meta-analysis study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
PubMed-MEDLINE, Scopus, and Web of Science were searched for original articles reporting the efficacy in adult patients with IC conditions between June 1, 2020 and September 1, 2021. The search terms were as follows: ((COVID-19) OR (SARS-CoV-2) OR (novel coronavirus)) AND ((vaccine) OR (vaccination)) OR (vaccinated)) AND ((immunocompromised) OR (immunosuppressed) OR (corticosteroid) OR (chemotherapy) OR (cancer) OR (malignancy) OR (rheumatologic disease) OR (immunodeficiency) OR (autoimmune) OR (AIDS) OR (HIV) OR (transplant)).
The references of the selected articles were further screened to search for potentially relevant articles. Two reviewers independently performed the literature search, and any disagreement regarding study inclusion was resolved by consensus. The authors were not blinded to the authors, institutions, or journals while selecting studies or extracting data. EndNote version ×9 was used for literature management.
Eligibility criteria
Studies investigating the immunogenicity of COVID-19 mRNA vaccination in IC patients were eligible for inclusion. The included studies met the following criteria. (1) Population: studies on IC patients with a sample size ≥ 30 participants and control group of healthy individuals. IC patients included patients with solid organ or hematologic malignancies who receive chemotherapy, patients with inherited or acquired immunodeficiency diseases, patients with autoimmune or rheumatologic diseases, patients with other conditions (i.e., asthma) receiving long-term corticosteroid, and transplant recipients. (2) Intervention: mRNA COVID-19 vaccination. (3) Study design: all retrospective and prospective studies, as well as clinical trials with a healthy control group, were included. (4) Outcomes: the main outcome of this study was seroconversion in IC patients using anti-SARS-CoV-2 spike IgG after the second dose of COVID-19 mRNA vaccines. The subgroup analysis was performed to determine the efficacy of COVID-19 mRNA vaccines in different groups of patients based on the etiology of the IC condition.
The exclusion criteria were as follows: (1) reviews and editorials; (2) case reports or case series < 30 patients; (3) partially overlapping patient cohorts; (4) articles not written in English; (5) single-arm studies or with a non-healthy control group; and (6) non-human studies. Two reviewers independently reviewed the literature in consensus.
Data collection
Eligible studies were evaluated by two experts independently. The following data were extracted from each included publication: author, date of publications, country of origin, study design, study sample size, the definition of IC conditions, inclusion and exclusion criteria, the number of IC patients, variables matched, the proportion of male, mean age, duration of disease, type and etiology of the immunodeficiency and its proportion to the total population, type of vaccination, and efficacy of the vaccination.
Any conflicts in data extraction were discussed or consulted by a third expert and resolved.
Quality assessment
National Institutes of Health (NIH) quality assessment tool [16] was used to evaluate the included studies. The scores of 11–14, 6–10, and 0–5 were considered good, fair, and poor quality, respectively. Moreover, the studies were evaluated in terms of methodology by two experts independently; any conflict of opinion was discussed or referred to a third expert and resolved.
Statistical analyses
STATA version 16 for Windows (Stata Corp, College Station, Texas) was utilized for the meta-analysis. At least three studies in each group were required to synthesize the data on outcomes. The heterogeneity of studies was measured using I2 or Q test. A fixed model was employed if the heterogeneity of studies was below 40% and a random effect model in case of heterogeneity above 40%. Effect measures were calculated as relative risk (RR), but relative risk reduction (RRR; 1-RR) values were reported in the results section for better interpretation. Also, based on the heterogeneity of studies, either meta-regression analysis or subgroup analysis was performed for potential moderators. Moreover, funnel plot asymmetry and the Eggers test were used to assess publication bias. In case of significant publication bias, the adjustment was performed for the effect size using the trim-and-fill method. A P-value less than 0.05 was considered statistically significant.
Results
Study selection
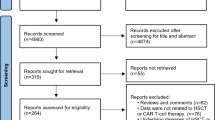
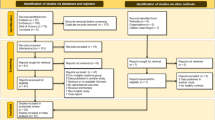
The study selection flowchart is presented in Fig. 1. The literature search, after removing duplicates, resulted in 2093 studies, of which 1992 were considered irrelevant following title and abstract screening. Of the remaining 101, a further 75 were removed according to the exclusion criteria. Therefore, in total, 26 studies [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42] were eligible for the meta-analysis of seroconversion after the second dose of the vaccine.

The PRISMA 2009 flow diagram of the study
Characteristics of included studies
Characteristics of the included studies are provided in Table 1. All 26 included studies on 3207 IC patients and 1726 healthy controls showed that 65.8% IC patients and 99.2% healthy controls had seropositive IgG tests following the second dose of COVID-19 mRNA vaccines. All of the studies were conducted in 2021. Sample sizes, from which relevant data were available for extraction, varied from 40 to 807. Participants’ mean age ranged from 42 to 71.4 years. The majority of the studies [19, 21, 24,25,26, 28, 30,31,32,33,34,35, 37,38,39,40,41,42] had a prospective cohort design (n = 18). Five studies [18, 20, 22, 23, 29] had a retrospective cohort design and three [17, 27, 36] were cross-sectional.
Seroconversion in immunocompromised patients vs. controls
Meta-analysis of 26 studies (I2 = 99.10%) revealed that positive seroconversion risk in IC patients were 48% lower than healthy controls. (RRR = 0.48; 95% CI 0.35, 0.58; P < 0.01). Subgroup meta-analysis based on the type of IC (i.e., autoimmune, transplant, and malignancy), revealed a statistically significant between-group difference (P < 0.01) (Fig. 2). When comparing each two subtypes of immunodeficiency, the results showed that IC patients due to transplant were less likely to develop positive seroconversion than IC patients due to autoimmune disorder (P < 0.01) as well as IC patients due to malignancy (P < 0.01). There was no statistically significant difference in seroconversion between IC patients with an autoimmune disorder and those with malignancy (P = 0.19).

Meta-analysis of seroconversion in immunocompromised patients vs controls, based on type of immunodeficiency
Seroconversion in patients with autoimmune disease vs. controls
Four [21, 22, 35, 38] of the included studies were conducted on IC patients with autoimmune immunodeficiency. Although the proportion of positive seroconversion in these patients was lower than the controls, the pooled analysis showed no statistically significant difference in relative risk reduction of seroconversion between two groups (RRR = 0.13; 95% CI − 0.01, 0.25; P = 0.07) (Fig. 2).
Seroconversion in patients with malignancy vs. controls
Meta-analysis of 9 studies [17, 19, 24, 25, 27, 29, 31, 32, 34] (I2 = 97.92) revealed IC patients with malignancy were 0.25 times less likely to seroconvert than healthy controls (RRR = 0.25; 95% CI 0.11, 0.37; P < 0.01). Subgroup meta-analysis was conducted based on type of malignancy (hematologic vs. solid organ). Four [24, 25, 29, 34] of the studies were on patients with hematologic malignancy and three [17, 19, 31] were on patients with solid organ malignancy. The relative risk reduction of seroconversion among IC patients with hematologic malignancies was significantly higher than those with solid organ malignancies (RRR = 0.29; 95% CI 0.14, 0.56 vs. RRR = 0.12; 95% CI 0.08, 0.15; P = 0.03) (Fig. 3).

Meta-analysis of seroconversion in immunocompromised patients with malignancy vs controls, based on type of malignancy
Seroconversion in transplant recipients vs. controls
Of the included studies, 13 [18, 20, 23, 26, 28, 30, 33, 36, 37, 39,40,41,42] were on IC patients due to transplantation (including kidney transplant, heart, lung, and liver). The meta-analysis of the 13 studies (I2 = 94.67%) showed transplant recipients were 67% less likely to develop seroconversion than controls (RRR = 0.67; 95% CI 0.53, 0.76; P < 0.01). Seven [20, 23, 26, 28, 39, 40, 42] of the included studies were on patients with kidney transplant, and the remaining [18, 30, 33, 36, 37, 41] were on patients with different transplants; none of which with more than three studies to be separated in the subgroup analysis. Hence, a subgroup meta-analysis was conducted based on the type of transplantation (kidney vs. others (including heart, lung, and liver)). The analysis did not reveal any statistically significant difference in relative risk of seroconversion in patients with kidney transplant compared to other types of transplants (RRR = 0.70, 95% CI 0.53, 0.80) vs. RRR = 0.22; 95% CI 0.34, 0.79; P = 0.55) (Fig. 4).

Meta-analysis of seroconversion in transplant patients vs controls, based on type of transplant
Quality assessment of included studies
Quality assessment of the included studies is presented in Additional file 1: Table S1. The majority of the studies (n = 18) [17,18,19, 22,23,24, 26, 28, 29, 31, 32, 34, 35, 38,39,40,41,42] were of good quality and 8 [20, 21, 25, 27, 30, 33, 36, 37] had fair quality.
Publication bias
Funnel plot for seroconversion was asymmetrical and Egger test showed statistically significant evidence of publication bias (P < 0.01, z = − 9.09). Trim-and-fill method was used to adjust the effect size (pooled estimate = 0.87; 95% CI 0.85, 0.88; number of studies = 84) (Fig. 5).

Funnel plot a and trim-and-fill funnel plot b for meta-analysis of seroconversion in patients with immunodeficiency
Discussion
Immunodeficiency comprises a wide range of disorders from primary (e.g., congenital) to numerous secondary conditions acquired consequently to a disease process or its treatment (e.g., human immunodeficiency virus (HIV) infection, radiation therapy, and immunosuppressive medications) [43]. Although inconclusive, it has been shown that IC patients might be at a higher risk of severe COVID-19 [44, 45]. On the other hand, a limited number of studies revealed reduced vaccine efficacy of vaccines in IC patients [46]. Nevertheless, data are limited on the efficacy of COVID-19 vaccines in this critical group of patients.
In this meta-analysis on the immunogenicity of COVID-19 mRNA vaccines in IC patients, we found a lower risk of positive seroconversion in this group of patients compared to healthy controls. In addition, subgroup analysis revealed a significantly lower risk of positive seroconversion in transplant recipients than patients with autoimmune disorder or malignancy. Intriguingly, COVID-19 mRNA vaccines seem to achieve lower efficacy in patients with hematologic malignancies compared to solid organs.
The controls were all healthy individuals, and a lower risk of positive seroconversion might not be surprising as observed with the administration of previous vaccines (e.g., Influenza vaccine) [47]. However, it does not undermine the importance of vaccines in IC patients, as evidence highlights that the immune response after vaccines is more robust than that of natural SARS-CoV-2 infection [48, 49]. It can also imply the importance of booster dose administration in this group of patients. As per recent Center for Disease Control and Prevention (CDC) guidelines, patients with moderately to severely compromised immune systems are recommended to receive an additional dose of COVID-19 mRNA vaccine [50]. Furthermore, studies have shown the promotion of immune response in transplant recipients receiving the third dose of mRNA vaccines, namely mRNA-1273 (Moderna) and BNT162b2 (Pfizer-BioNTech) [51, 52]. However, a dichotomous view toward the booster dose seems insufficient since the degree and etiology of immunosuppression tend to be two important factors regarding immune response and the need for an additional dose [53]. Whether a booster dose is necessarily associated with an enhanced immune response is also a matter of debate. There is evidence that initial post-vaccine antibody titer was predictive of response to booster, and some IC patients will never mount an antibody response [54], and a more restricted personal protection is highly recommended even after vaccination [55].
Interestingly, our analysis revealed significantly lower relative risk of positive seroconversion in patients with transplant compared to patients with autoimmune disorders or malignancies. A study by Evison et al. on the efficacy of the Influenza vaccine, showed that the vaccine response rate was higher among patients with HIV and patients who received dialysis compared to renal transplant recipients and patients with a rheumatologic disease [56]. This can be justified by the fact that treatment regimens may be an important contributing factor. Mycophenolate mofetil has been shown to accompany less immune response compared to a regimen consisting of prednisone, cyclosporine, and azathioprine [57,58,59]. These drugs, which are used to prevent allograft rejection, interfere with T and B cell activation and proliferation, leading to the impediment of antibody generation [60]. Although we did not find any significant difference between kidney transplant and other organ transplant recipients, transplant recipients seem to be more vulnerable to vaccine failures in general, and special attention should be directed toward this group of patients. Studies proposed some approaches to increase the immunogenicity of vaccines in transplant recipients, such as modulation of immunosuppression, adjuvants, intradermal injection, high antigen doses, and booster administration [60].
Hematologic diseases are believed to have the highest level of immunosuppression among malignancies [61]. This group of patients also has 3- to 4-fold higher rates of severe/critical COVID-19 disease and mortality [62, 63]. Hematologic malignancies are associated with immune dysfunction with alterations in both innate and adaptive immunity [64]. Cytopenia, B/plasma cells reduction, hypogammaglobulinemia, and anti-cancer therapy are among the underlying cause of immunodeficiency in these patients [65]; thus, a lower vaccine efficacy might be observed consequently, which is consistent with our findings of the lower immunogenicity of mRNA vaccines in patients with hematologic malignancies.
Although the included four studies demonstrated no statistically significant difference in relative risk of seroconversion between autoimmune disease and control, it still should be interpreted with caution because of limited sample sizes and strong heterogeneity. Autoimmune diseases are a group of heterogenous diseases treated by numerous drugs. For instance, a study of 27 subjects with systemic-onset juvenile idiopathic arthritis (sJIA) found no significant difference between the efficacy of the influenza vaccine in sJIA patients and healthy controls [66]. They also showed that the duration of tocilizumab administration did not impact the response to the vaccine. Also, another recent study showed that although short-term corticosteroid therapy reduces reactogenicity of the first dose of ChAdOx1 nCoV-19, it does not weaken its immunogenicity [67]. On the other hand, a preliminary report (preprint) shows that methotrexate might hamper humoral and cellular immune response to COVID-19 mRNA vaccines [68]. Conspicuously enough, more in-depth investigations are needed in this scope.
It is also worth mentioning that there are numerous approaches to assessing of immune response after vaccine administration which are related to anti-SARS-COV-2 recombinant spike, receptor binding domain, or neutralizing IgG or total antibodies [53]. We included articles with the main outcome of anti-SARS-CoV-2 spike IgG level; however, seropositivity may not necessarily show protection against SARS-CoV-2 [54], and routine assessment of COVID-19 vaccine responses is not recommended [54].
Another important aspect of vaccine immunogenicity can be rendered by T-cell response. T-cell response seems to be achieved efficiently after the second dose of either BNT162b2 mRNA or ChAdOx1 nCoV-19 vaccines [69]. The T-cell response should also be prioritized besides the induction of neutralizing antibodies. T cells are an indispensable part of immune response with the presence of subprotective antibody titers in IC patients [70]; e.g., patients with agammaglobulinemia tend to conquer COVID-19 showing the importance of cellular immune response when there is inefficient humoral response [71,72,73]. However, there is a lack of data regarding T-cell response in IC patients, and more studies are indeed needed.
We confined this meta-analysis to mRNA vaccines due to limited studies on other COVID-19 vaccine types and to reduce heterogeneity. However, a study by Boekel et al. on the development of antibody in patients with autoimmune diseases did not show any significant difference between immunogenicity induced by an mRNA vaccine (BNT162b2) and a viral vector type (ChAdOx1 nCoV-19) [74]. It has also been shown that inactivated COVID-19 vaccine (CoronaVac) can induce an immune response in patients with immune-mediated disease; still, the titer of antibody is associated with age and type of immunosuppressive therapy [75].
This study indeed has some limitations. There was a lack of data regarding HIV and other primary immunodeficiency disorders, and they are not included in this meta-analysis. Furthermore, we included studies with both retrospective and prospective designs, which may reduce the level of evidence. One of the major limitations of this review was the high heterogeneity of the studies. This could be explained by the different quantitative methods used in the studies, different measurement kits and cutoff points to determine a positive seroconversion. Moreover, ethnicity, different types of mRNA vaccines, and study design (i.e., retrospective or prospective) could have been the potential sources of heterogeneity. Further assessment and studies are required in this field.
Conclusion
The risk of positive seroconversion in IC patients was almost half of those in healthy individuals. However, IC conditions due to autoimmune disorders did not lower the risk of positive seroconversion, but more comprehensive investigations are needed. Among IC conditions, transplant recipients induced the lowest immunogenicity with a 67% lower risk of seroconversion than healthy individuals. Besides, we found that vaccination among IC patients with hematological malignancy induced a lower risk of seroconversion than those among IC patients with solid organ malignancy. Findings from this meta-analysis could aid healthcare policymakers in making decisions regarding the importance of the booster dose or more strict personal protections in the IC patients.
Availability of data and materials
The authors stated that all information provided in this article could be shared.
Abbreviations
- IC:
-
Immunocompromised
- COVID-19:
-
Coronavirus infectious disease 2019
- HIV:
-
Human immunodeficiency virus
References
Covid-19 vaccines for moderately to severely immunocompromised people: centers for disease control and prevention. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/immuno.html. Accessed 7 Sept 2021.
Harpaz R, Dahl RM, Dooling KL. Prevalence of immunosuppression among US adults, 2013. JAMA. 2016;316(23):2547–8.
Abkhoo A, Shaker E, Mehrabinejad M-M, Azadbakht J, Sadighi N, Salahshour F. Factors predicting outcome in intensive care unit-admitted COVID-19 patients: using clinical, laboratory, and radiologic characteristics. Crit Care Res Pract. 2021. https://doi.org/10.1155/2021/9941570.
Dumortier J, Duvoux C, Roux O, Altieri M, Barraud H, Besch C, et al. Covid-19 in liver transplant recipients: the French SOT COVID registry. Clin Res Hepatol Gastroenterol. 2021;45(4): 101639.
Liang W, Guan W, Chen R, Wang W, Li J, Xu K, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21(3):335–7.
Alhumaid S, Al Mutair A, Al Alawi Z, Al Salman K, Al Dossary N, Omar A, et al. Clinical features and prognostic factors of intensive and non-intensive 1014 COVID-19 patients: an experience cohort from Alahsa, Saudi Arabia. Eur J Med Res. 2021;26(1):1–13.
SeyedAlinaghi S, Abbasian L, Solduzian M, Yazdi NA, Jafari F, Adibimehr A, et al. Predictors of the prolonged recovery period in COVID-19 patients: a cross-sectional study. Eur J Med Res. 2021;26(1):1–10.
Hensley MK, Bain WG, Jacobs J, Nambulli S, Parikh U, Cillo A, et al. Intractable COVID-19 and prolonged SARS-CoV-2 replication in a CAR-T-cell therapy recipient: a case study. Clin Infect Dis. 2021. https://doi.org/10.1093/cid/ciab072.
Aydillo T, Gonzalez-Reiche AS, Aslam S, van de Guchte A, Khan Z, Obla A, et al. Shedding of viable SARS-CoV-2 after immunosuppressive therapy for cancer. N Engl J Med. 2020;383(26):2586–8.
Avanzato VA, Matson MJ, Seifert SN, Pryce R, Williamson BN, Anzick SL, et al. Case study: prolonged infectious SARS-CoV-2 shedding from an asymptomatic immunocompromised individual with cancer. Cell. 2020;183(7):1901-12 e9.
Addeo A, Shah PK, Bordry N, Hudson RD, Albracht B, Di Marco M, et al. Immunogenicity of SARS-CoV-2 messenger RNA vaccines in patients with cancer. Cancer Cell. 2021;39(8):1091–8.
Cheng H, Peng Z, Luo W, Si S, Mo M, Zhou H, et al. Efficacy and safety of COVID-19 vaccines in phase III trials: a meta-analysis. Vaccines. 2021;9(6):582.
Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020. https://doi.org/10.1056/NEJMoa2034577.
Baden LR, El Sahly HM, Essink B, Kotloff K, Frey S, Novak R, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med. 2021;384(5):403–16.
Natori Y, Humar A, Lipton J, Kim D, Ashton P, Hoschler K, et al. A pilot randomized trial of adjuvanted influenza vaccine in adult allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transplant. 2017;52(7):1016–21.
National Heart L, Institute B. Study Quality Assessment Tools. 2019. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed 7 Sept 2021.
Agbarya A, Sarel I, Ziv-Baran T, Agranat S, Schwartz O, Shai A, et al. Efficacy of the mRNA-based BNT162b2 COVID-19 vaccine in patients with solid malignancies treated with anti-neoplastic drugs. Cancers. 2021. https://doi.org/10.3390/cancers13164191.
Cao J, Liu X, Muthukumar A, Gagan J, Jones P, Zu Y. Poor Humoral Response in Solid Organ Transplant Recipients following Complete mRNA SARS-CoV-2 Vaccination. Clin Chem. 2021. https://doi.org/10.1093/clinchem/hvab149.
Eliakim-Raz N, Massarweh A, Stemmer A, Stemmer SM. Durability of response to SARS-CoV-2 BNT162b2 vaccination in patients on active anticancer treatment. JAMA Oncol. 2021. https://doi.org/10.1001/jamaoncol.2021.4390.
Firket L, Descy J, Seidel L, Bonvoisin C, Bouquegneau A, Grosch S, et al. Serological response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients depends on prior exposure to SARS-CoV-2. Am J Transplant. 2021. https://doi.org/10.1111/ajt.16726.
Furer V, Eviatar T, Zisman D, Peleg H, Paran D, Levartovsky D, et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: a multicentre study. Ann Rheum Dis. 2021. https://doi.org/10.1136/annrheumdis-2021-220647.
Geisen UM, Berner DK, Tran F, Sümbül M, Vullriede L, Ciripoi M, et al. Immunogenicity and safety of anti-SARS-CoV-2 mRNA vaccines in patients with chronic inflammatory conditions and immunosuppressive therapy in a monocentric cohort. Ann Rheum Dis. 2021. https://doi.org/10.1136/annrheumdis-2021-220272.
Grupper A, Rabinowich L, Schwartz D, Schwartz IF, Ben-Yehoyada M, Shashar M, et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am J Transplant. 2021;21(8):2719–26.
Herishanu Y, Avivi I, Aharon A, Shefer G, Levi S, Bronstein Y, et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Blood. 2021;137(23):3165–73.
Herzog Tzarfati K, Gutwein O, Apel A, Rahimi-Levene N, Sadovnik M, Harel L, et al. BNT162b2 COVID-19 vaccine is significantly less effective in patients with hematologic malignancies. Am J Hematol. 2021. https://doi.org/10.1002/ajh.26284.
Hod T, Ben-David A, Olmer L, Levy I, Ghinea R, Mor E, et al. Humoral Response of Renal Transplant Recipients to the BNT162b2 SARS-CoV-2 mRNA Vaccine Using Both RBD IgG and Neutralizing Antibodies. Transplantation. 2021. https://doi.org/10.1097/TP.0000000000003889.
Iacono D, Cerbone L, Palombi L, Cavalieri E, Sperduti I, Cocchiara RA, et al. Serological response to COVID-19 vaccination in patients with cancer older than 80 years. J Geriatr Oncol. 2021. https://doi.org/10.1016/j.jgo.2021.06.002.
Korth J, Jahn M, Dorsch O, Anastasiou OE, Sorge-Hadicke B, Eisenberger U, et al. Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses Basel. 2021. https://doi.org/10.3390/v13050756.
Malard F, Gaugler B, Gozlan J, Bouquet L, Fofana D, Siblany L, et al. Weak immunogenicity of SARS-CoV-2 vaccine in patients with hematologic malignancies. Blood Cancer J. 2021. https://doi.org/10.1038/s41408-021-00534-z.
Marinaki S, Adamopoulos S, Degiannis D, Roussos S, Pavlopoulou ID, Hatzakis A, et al. Immunogenicity of SARS-CoV-2 BNT162b2 vaccine in solid organ transplant recipients. Am J Transplant. 2021;21(8):2913–5.
Massarweh A, Eliakim-Raz N, Stemmer A, Levy-Barda A, Yust-Katz S, Zer A, et al. Evaluation of seropositivity following BNT162b2 messenger RNA vaccination for SARS-CoV-2 in patients undergoing treatment for cancer. JAMA Oncol. 2021. https://doi.org/10.1001/jamaoncol.2021.2155.
Monin L, Laing AG, Munoz-Ruiz M, McKenzie DR, Del Barrio ID, Alaguthurai T, et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: interim analysis of a prospective observational study. Lancet Oncol. 2021;22(6):765–78.
Peled Y, Ram E, Lavee J, Sternik L, Segev A, Wieder-Finesod A, et al. BNT162b2 vaccination in heart transplant recipients: clinical experience and antibody response. J Heart Lung Transplant. 2021;40(8):759–62.
Pimpinelli F, Marchesi F, Piaggio G, Giannarelli D, Papa E, Falcucci P, et al. Fifth-week immunogenicity and safety of anti-SARS-CoV-2 BNT162b2 vaccine in patients with multiple myeloma and myeloproliferative malignancies on active treatment: preliminary data from a single institution. J Hematol Oncol. 2021;14(1):81.
Prendecki M, Clarke C, Edwards H, McIntyre S, Mortimer P, Gleeson S, et al. Humoral and T-cell responses to SARS-CoV-2 vaccination in patients receiving immunosuppression. Ann Rheum Dis. 2021. https://doi.org/10.1136/annrheumdis-2021-220626.
Rabinowich L, Grupper A, Baruch R, Ben-Yehoyada M, Halperin T, Turner D, et al. Low immunogenicity to SARS-CoV-2 vaccination among liver transplant recipients. J Hepatol. 2021;75(2):435–8.
Rashidi-Alavijeh J, Frey A, Passenberg M, Korth J, Zmudzinski J, Anastasiou OE, et al. Humoral response to SARS-Cov-2 vaccination in liver transplant recipients-a single-center experience. Vaccines. 2021. https://doi.org/10.3390/vaccines9070738.
Reuken PA, Andreas N, Grunert PC, Glöckner S, Kamradt T, Stallmach A. T cell response after SARS-CoV-2 vaccination in immunocompromised patients with inflammatory bowel disease. J Crohn Colitis. 2021. https://doi.org/10.1093/ecco-jcc/jjab147.
Rincon-Arevalo H, Choi M, Stefanski AL, Halleck F, Weber U, Szelinski F, et al. Impaired humoral immunity to SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients and dialysis patients. Sci Immunol. 2021. https://doi.org/10.1126/sciimmunol.abj1031.
Sattler A, Schrezenmeier E, Weber UA, Potekhin A, Bachmann F, Straub-Hohenbleicher H, et al. Impaired humoral and cellular immunity after SARS-CoV-2 BNT162b2 (tozinameran) prime-boost vaccination in kidney transplant recipients. J Clin Invest. 2021. https://doi.org/10.1172/JCI150175.
Schramm R, Costard-Jackle A, Rivinius R, Fischer B, Muller B, Boeken U, et al. Poor humoral and T-cell response to two-dose SARS-CoV-2 messenger RNA vaccine BNT162b2 in cardiothoracic transplant recipients. Clin Res Cardiol. 2021;110(8):1142–9.
Stumpf J, Siepmann T, Lindner T, Karger C, Schwöbel J, Anders L, et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: a prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg Health Eur. 2021. https://doi.org/10.1016/j.lanepe.2021.100178.
Duly K, Farraye FA, Bhat S. COVID-19 vaccine use in immunocompromised patients: a commentary on evidence and recommendations. Am J Health-Syst Pharm. 2021. https://doi.org/10.1093/ajhp/zxab344.
Fung M, Babik JM. COVID-19 in immunocompromised hosts: what we know so far. Clin Infect Dis. 2021;72(2):340–50.
Salahshour F, Mehrabinejad M-M, Toosi MN, Gity M, Ghanaati H, Shakiba M, et al. Clinical and chest CT features as a predictive tool for COVID-19 clinical progress: introducing a novel semi-quantitative scoring system. Eur Radiol. 2021. https://doi.org/10.1007/s00330-020-07623-w.
Prevention CfDCa. Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Approved or Authorized in the United States 2021. https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html. Accessed 7 Sept 2021.
Felldin M, Studahl M, Svennerholm B, Friman V. The antibody response to pandemic H1N1 2009 influenza vaccine in adult organ transplant patients. Transpl Int. 2012;25(2):166–71.
Altawalah H. Antibody responses to natural SARS-CoV-2 infection or after COVID-19 vaccination. Vaccines. 2021;9(8):910.
Greaney AJ, Loes AN, Gentles LE, Crawford KHD, Starr TN, Malone KD, et al. Antibodies elicited by mRNA-1273 vaccination bind more broadly to the receptor binding domain than do those from SARS-CoV-2 infection. Sci Transl Med. 2021. https://doi.org/10.1126/scitranslmed.abi9915.
Control CfD, Prevention. COVID-19 vaccines for moderately to severely immunocompromised people. 2021. Accessed 7 Sept 2021.
Hall VG, Ferreira VH, Ku T, Ierullo M, Majchrzak-Kita B, Chaparro C, et al. Randomized trial of a third dose of mRNA-1273 vaccine in transplant recipients. N Engl J Med. 2021. https://doi.org/10.1056/NEJMc2111462.
Del Bello A, Abravanel F, Marion O, Couat C, Esposito L, Lavayssière L, et al. Efficiency of a boost with a third dose of anti-SARS-CoV-2 messenger RNA-based vaccines in solid organ transplant recipients. Am J Transplant. 2021. https://doi.org/10.1111/ajt.16775.
Lee AR, Wong SY, Chai LYA, Lee SC, Lee M, Muthiah MD, et al. Efficacy of COVID-19 vaccines in immunocompromised patients: a systematic review and meta-analysis. medRxiv. 2021;31:143.
Haidar G, Agha M, Lukanski A, Linstrum K, Troyan R, Bilderback A, et al. Immunogenicity of COVID-19 vaccination in immunocompromised patients: an observational, prospective cohort study interim analysis. medRxiv. 2021;72:340.
Tabatabaeizadeh S-A. Airborne transmission of COVID-19 and the role of face mask to prevent it: a systematic review and meta-analysis. Eur J Med Res. 2021;26(1):1–6.
Evison J, Farese S, Seitz M, Uehlinger DE, Furrer H, Mühlemann K. Randomized, double-blind comparative trial of subunit and virosomal influenza vaccines for immunocompromised patients. Clin Infect Dis. 2009;48(10):1402–12.
Cavdar C, Sayan M, Sifil A, Artuk C, Yilmaz N, Bahar H, et al. The comparison of antibody response to influenza vaccination in continuous ambulatory peritoneal dialysis, hemodialysis and renal transplantation patients. Scand J Urol Nephrol. 2003;37(1):71–6.
Smith KG, Isbel NM, Catton MG, Leydon JA, Becker GJ, Walker RG. Suppression of the humoral immune response by mycophenolate mofetil. Nephrol Dial Transplant. 1998;13(1):160–4.
Scharpé J, Evenepoel P, Maes B, Bammens B, Claes K, Osterhaus A, et al. Influenza vaccination is efficacious and safe in renal transplant recipients. Am J Transplant. 2008;8(2):332–7.
Caillard S, Thaunat O. COVID-19 vaccination in kidney transplant recipients. Nat Rev Nephrol. 2021. https://doi.org/10.1038/s41581-021-00491-7.
Chemaly RF, Ghosh S, Bodey GP, Rohatgi N, Safdar A, Keating MJ, et al. Respiratory viral infections in adults with hematologic malignancies and human stem cell transplantation recipients: a retrospective study at a major cancer center. Medicine. 2006;85(5):278–87.
Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052–9.
Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–42.
Atkins S, He F. Chemotherapy and beyond: infections in the era of old and new treatments for hematologic malignancies. Infect Dis Clin. 2019;33(2):289–309.
Dhodapkar MV, Dhodapkar KM, Ahmed R. Viral immunity and vaccines in hematologic malignancies: implications for COVID-19. Blood Cancer Discov. 2021;2(1):9.
Shinoki T, Hara R, Kaneko U, Miyamae T, Imagawa T, Mori M, et al. Safety and response to influenza vaccine in patients with systemic-onset juvenile idiopathic arthritis receiving tocilizumab. Mod Rheumatol. 2012;22(6):871–6.
Yang J, Ko JH, Baek JY, Hong J, Ha S, Lee B, et al. Effects of short-term corticosteroid use on reactogenicity and immunogenicity of the first dose of ChAdOx1 nCoV-19 vaccine. Front Immunol. 2021;12: 744206.
Haberman RH, Herati RS, Simon D, Samanovic M, Blank RB, Tuen M, et al. Methotrexate hampers immunogenicity to BNT162b2 mRNA COVID-19 vaccine in immune-mediated inflammatory disease. medRxiv. 2021;26:593.
Prendecki M, Clarke C, Edwards H, McIntyre S, Mortimer P, Gleeson S, et al. Humoral and T-cell responses to SARS-CoV-2 vaccination in patients receiving immunosuppression. Ann Rheum Dis. 2021;80(10):1322–9.
McMahan K, Yu J, Mercado NB, Loos C, Tostanoski LH, Chandrashekar A, et al. Correlates of protection against SARS-CoV-2 in rhesus macaques. Nature. 2021;590(7847):630–4.
Quinti I, Lougaris V, Milito C, Cinetto F, Pecoraro A, Mezzaroma I, et al. A possible role for B cells in COVID-19? Lesson from patients with agammaglobulinemia. J Allergy Clin Immunol. 2020;146(1):211–3.
Soresina A, Moratto D, Chiarini M, Paolillo C, Baresi G, Focà E, et al. Two X-linked agammaglobulinemia patients develop pneumonia as COVID-19 manifestation but recover. Pediatr Allergy Immunol. 2020;31(5):565–9.
Breathnach AS, Duncan CJA, El Bouzidi K, Hanrath AT, Payne BAI, Randell PA, et al. Prior COVID-19 protects against reinfection, even in the absence of detectable antibodies. J Infect. 2021;83(2):237–79.
Boekel L, Steenhuis M, Hooijberg F, Besten YR, van Kempen ZL, Kummer LY, et al. Antibody development after COVID-19 vaccination in patients with autoimmune diseases in the Netherlands: a substudy of data from two prospective cohort studies. Lancet Rheumatol. 2021. https://doi.org/10.1016/S2665-9913(21)00222-8.
Seyahi E, Bakhdiyarli G, Oztas M, Kuskucu MA, Tok Y, Sut N, et al. Antibody response to inactivated COVID-19 vaccine (CoronaVac) in immune-mediated diseases: a controlled study among hospital workers and elderly. Rheumatol Int. 2021. https://doi.org/10.1007/s00296-021-04910-7.
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
The conception and design of the study: MM, HD, SS, NR; acquisition of data: MM, AH, AA, MS, MT; drafting the article: MM, FM, MT; revising it critically for important intellectual content: SS, MM, NR, HD; final approval of the version to be submitted: NR, SS. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that there is no conflict of interest regarding the publication of this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Table S1. Quality assessment using NIH tool.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mehrabi Nejad, MM., Moosaie, F., Dehghanbanadaki, H. et al. Immunogenicity of COVID-19 mRNA vaccines in immunocompromised patients: a systematic review and meta-analysis. Eur J Med Res 27, 23 (2022). https://doi.org/10.1186/s40001-022-00648-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-022-00648-5