
Abstract
Background
In the rehabilitation and sports science fields, comprehensive assessment of the response to exercise is important for accurately prescribing exercise programs. Lactate is an important energy substrate that is frequently measured in clinical practice because it provides information on aerobic capacity. Salivary lactate, which can be measured non-invasively, has recently been focused on as an alternative to blood lactate. This study aimed to determine the combined effects of body fat, body water content, and skeletal muscle mass index on peak salivary lactate levels.
Methods
Thirty-seven non-athletic males performed a squat jump exercise. Their salivary lactate levels were measured before, immediately after, and every 5 min after the exercise using a simplified device. We also assessed body composition. A linear multiple regression analysis was performed with peak salivary lactate levels as the dependent variable and body fat ratio, body water content, and the skeletal muscle mass index as independent variables.
Results
The participants’ body fat ratio (positive effect; p = 0.001) and body water content (negative effect; p = 0.035) significantly affected peak salivary lactate levels. Skeletal muscle mass index tended to positively influence salivary lactate levels (p = 0.099), albeit not significantly. The adjusted R-squared value of the model was 0.312 (p = 0.001).
Conclusions
The combined effect of body fat, body water content, and skeletal muscle mass index on peak salivary lactate levels was 31.2%. Better nutritional guidance may be effective in promoting weight loss and increasing body water content to improve aerobic capacity in the rehabilitation setting.
Similar content being viewed by others
Background
In the rehabilitation and sports science fields, comprehensive assessment of the response to exercise is important for accurately prescribing exercise programs and determining the effectiveness of training. Such responses to exercise included the metabolic [1], cardiovascular [2, 3], and respiratory [4] systems, and have been well documented in the literature. In hospitals, exercise prescriptions are commonly based on the anaerobic threshold [5] calculated from cardiopulmonary exercise testing (CPX), especially in the area of cardiac rehabilitation. Medical staff can obtain information on patients’ aerobic capacity using CPX. However, CPX systems are extremely large, expensive, and requires expertise, and so only a limited number of facilities are able to perform it. On the other hand, the point at which blood lactate (BLa) concentration increases exponentially during a graded incremental exercise test is defined as the lactate threshold (LT) and is often used in the area of sports science [6, 7]. Lactate is an important energy substrate [8, 9] that is produced by working skeletal muscle cells, circulates in the blood, and is metabolized in various tissues including the brain, heart, liver, and skeletal muscle [8, 10]. BLa is another measure of aerobic capacity [11]; as aerobic capacity improves, LT also increases. The higher LT that training provides means that energy metabolism during exercise is improved, which allows for higher endurance performance [12]. In contrast, for short-duration exercises such as squat jumps, sprints, and swimming as well as in sports in which measuring lactate during activity is difficult, it is common to evaluate aerobic capacity using peak lactate levels measured following an exercise task or trial. After the training period, if the peak lactate level is lower for the same load of exercise, aerobic capacity is considered to have improved. However, BLa measurement is slightly invasive, requiring blood sampling from the fingertip or earlobe [13, 14]. Salivary lactate (SLa) can be collected non-invasively, does not require special techniques for measurement [11], and has recently been considered an alternative method to BLa since both parameters reportedly trend in parallel during exercise. Segura et al. reported similar patterns of BLa and SLa transitions during the cycle ergometer maximal graded exercise test, which exhibited a positive correlation [15]. Santos et al. measured BLa and SLa at the 0 km point and at 6 km intervals of a 30 km run to reveal a positive correlation between BLa and SLa [11]. Moreover, Tekas et al. demonstrated a positive correlation between BLa and SLa before and after the maximum intensity Astrand treadmill test [16].
In addition to saliva, urine [17, 18] and sweat [19, 20] are also useful as specimens that can be collected non-invasively to determine lactate. However, it is difficult to obtain multiple urine samples in a short period of time, and it may not be possible to collect sufficient amounts of sweat to measure lactate levels reliably since perspiration varies greatly among individuals. Saliva-based measurements have higher clinical utility in these regards.
The greatest influence on lactate concentration is exercise intensity and working skeletal muscle cells, although other individual body characteristics may also affect lactate levels. For instance, adipocytes can produce lactate under anaerobic conditions, and the total amount of lactate produced by adipocytes is dependent on fat mass [10]. Regarding SLa, water transpiration due to exercise increases the amount of protein in the saliva [21] and may influence SLa levels. Whereas the above findings evaluate the relationship between a single physical parameter and lactate level, there have been no reports examining their combined effects in vivo. Since these multiple factors are considered to be acting simultaneously in the living body during rehabilitation, the purpose of this study was to determine the combined effects of body fat, body water content, and skeletal muscle on peak SLa levels.
Methods
Participants
A total of 37 healthy non-athletic males volunteered to participate in this observational study; their anthropometric characteristics are shown in Table 1. Informed consent was obtained from all participants after they were informed of the purpose and associated risks of this study.
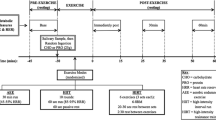
The participants were instructed to refrain from strenuous exercise the day before the trial. On the day of the trial, food intake apart from water was prohibited 1 h before the experiment. All measurements were conducted in a well-ventilated room with a temperature of 25.0 ± 1.9 °C and humidity of 52.4 ± 5.7%. Based on national regulations and guidelines, all experimental protocols were reviewed and approved by the local Ethics Committee and conformed to the recommendations of the Declaration of Helsinki.
Squat jump (SJ) exercise
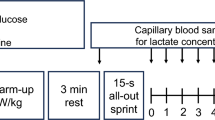
Prior to the trials, the examiner individually demonstrated and explained how to perform a standard SJ, which is often used to evaluate an athlete’s motor function for its simplicity and lack of specialized equipment [22, 23], and is also used during postoperative anterior cruciate ligament reconstruction rehabilitation [24]. Consistent with our previous studies [25, 26], a standard SJ included a squat, whereby bilateral lower limbs are spread to shoulder width, the knees flexed to 90°, with the trunk and lower legs parallel to each other, followed by a vertical jump as high as possible with the upper limbs swinging up and forward. The participants continued to repetitively perform SJs for 90 s at a constant tempo (46 bpm) guided by an electronic metronome (MA-1 SOLO METRONOME, KORG INC, Tokyo, Japan). In order to maximize their performance, the participants continued the task until the examiner signaled them to stop, without prior knowledge of the exercise duration. During the recovery phase after SJ, they rested in a sitting position.
Measurement of salivary lactate level
Lactate Pro 2 (Arkray, Kyoto, Japan) is a commercially available device for BLa measurements. It is a point-of-care device with a measurable range of 0.5–25.0 mmol/L, where values < 0.5 mmol/L are displayed as “Lo,” and values > 25.0 mmol/L are displayed as “Hi.“ We previously investigated the use of the Lactate Pro 2 for measuring SLa. The intraclass correlation coefficient between the Lactate Pro 2 and a JCA-BM 8000 automatic analyzer was 0.773, indicating substantial convergent validity [26] and validating the use of this device to measure the SLa in the current study. SLa values were measured before exercise (Pre), immediately after exercise (Post0), and every 5-min during the recovery phase (Post5–Post45). Since we aimed to measure the peak value of SLa, measurements were stopped when the value of SLa decreased five consecutive times per participant. The subjects expectorated saliva onto a clean dish just before each measurement, and SLa levels were quantified by directly placing a Lactate Pro 2 sensor on the saliva samples. The participants were instructed to brush their teeth before SJ task and rinse their mouths once with water after the SJ to remove any oral debris [16, 27]. For the safety management of the participants, heart rate (HR; Polar M200, Polar Electro Japan, Tokyo, Japan) and the Borg CR10 scale were recorded in parallel to SLa [28].
Body composition analysis
The body composition of each participant was measured using a high-precision body component analyzer (InBody 430, Inbody Japan, Tokyo, Japan) that can measure body components by bioelectrical impedance analysis, which measures the electrical resistance when small currents pass through the body [29]. The participants were instructed to stand barefoot on the device with light clothes on and grasp the handle with both hands in order to assess each body component. Body composition analyses were performed on the day of the trial, prior to the SJ exercise.
Statistical analysis
The relationship between the levels of peak SLa and body fat ratio, body water content, and SMI was modeled using linear multiple regression analysis. For body fat, the ratio of body fat mass (kg) to body weight (kg) was used. As an indicator of skeletal muscle, SMI was used rather than skeletal muscle mass to eliminate the effect of the height of each participant and was calculated by dividing the total muscle mass of the extremities by the square of the height (m). Data for which a normal distribution was confirmed were expressed as the mean ± standard deviation (SD); those that were not were expressed as the median and interquartile range (IQR). All statistical analyses were performed using the PASW Statistics software (version 26.0, SPSS, Inc., Chicago, IL, USA), and the significance threshold was set at 0.05.
Results
Peak SLa levels after squat jump exercise
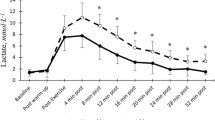
All subjects were able to complete 90 s of the SJ task at the speed of 46 bpm. Considering the data of the 37 participants, peak SLa levels were reached in 2 participants at Post0, 10 participants at Post10, 12 participants at Post15, 8 participants at Post20, 4 participants at Post25, and 1 participant at Post30. The peak SLa levels ranged from 0.7 to 7.7 mmol L, with an average value of 2.53 ± 1.49 mmol/L. The average values of the participant’s HR (123.1 ± 13.8 bpm) and Borg CR10 scale (6.8 ± 1.6) during the trial both reached maximum at Post0.
Modeling SLa using body fat ratio, body water content, and SMI
The results of multiple regression analysis are presented in Table 2. The obtained multiple regression equation was as follows: SLa peak level = 0.167 + 0.157 × Body fat ratio + (− 0.227) × Body water content + 1.190 × SMI.
The analysis was performed using a forced entry method with SLa as the dependent variable and body fat, body water content, and SMI as the independent variables. The participant’s body fat ratio (positive effect; p = 0.001) and body water content (negative effect; p = 0.035) significantly affected SLa. SMI tended to positively affect SLa (p = 0.099), albeit not significantly. Body fat ratio was observed to have the greatest influence on SLa levels. The adjusted R-squared value of the model was 0.312 (p = 0.001). The variance inflation factor was 1.174–3.562, which reflects a considerably low multicollinearity between the variables. The residuals of this model were found to be normal.
Discussion
In this investigation, we examined the combined effects of body fat ratio, body water content, and SMI on peak SLa levels after a squat jump exercise towards the clinical adoption of SLa testing in the rehabilitation setting. The importance of this study is that SLa can be measured easily and non-invasively in the clinical setting as an indicator of aerobic capacity. Our results showed that peak SLa levels can be estimated using body parameters. Clinically, this will enable better guidance for nutritional management and body composition in patients during rehabilitation.
Timing of peak SLa
BLa is known to increase immediately in response to exercise, whereas SLa increased 10–30 min after exercise in this study. Although the mechanism of this phenomenon could not be verified in the present investigation, several studies have reported similar results. Ohkuwa et al. measured BLa and SLa after 400-m and 3000-m run tests and showed that SLa peaked later than BLa [30]. Reer et al. measured BLa and SLa during a cycle ergometer test to reveal a clear delay in SLa as compared with BLa. One possible cause of this lag was considered the diffusion of lactate in the salivary glands [31].
Salivary lactate was strongly influenced by body fat ratio and body water content
The variables in this study, body fat ratio and body water content, supported the results of previous studies, whereby Jansson et al. demonstrated lactate levels of obese men (894 ± 69 µM) to be significantly higher than those of lean males (738 ± 49 µM) [32]. Particularly, white adipocytes have been reported to produce large amounts of lactate [33, 34]. Furthermore, our study indicated that for every incremental increase in body fat ratio, a 0.157 mmol/L increase in SLa level can be expected (p = 0.001), which further strengthens a positive relationship between body fat and SLa. In contrast, we found a negative relationship between SLa and body water content, whereby every incremental increase in body water content was anticipated to cause a 0.227 mmol/L decline in SLa level (p = 0.035). Whilst there are limited studies on the effect of saliva flow or secretion rate on lactate levels, an increase in total salivary proteins due to the evaporation of saliva through exercise was reported by Lindsay et al. [21]. Thus, the increase in body water and water content of saliva are proportional, and thereby results in a decrease in the lactate concentration. Regarding SMI being adopted as an index for skeletal muscles, our results suggest that SLa levels are inclined to increase by 1.190 mmol/L for every incremental increase in SMI, which is consistent with a previous study that found skeletal muscle mass and SMI to be positively correlated with BLa reduction (r = 0.71) [25]. Moreover, Santos et al. demonstrated that there was a positive correlation (r = 0.772) between the absolute values of BLa and SLa measured every 6 km in a 30-km marathon race [11]. Based on these results, we hypothesized that SMI also affects SLa and extracted it as a dependent variable. While there was a positive relationship between peak SLa and SMI, there was no significant difference (p = 0.099) observed in this study. To date, there are no reports that show the absolute value of lactate (both in blood and saliva) to be directly related to skeletal muscle mass and/or SMI. Lactate during exercise is mainly produced in the skeletal muscle and is simultaneously taken up in the working muscle, heart, brain, and liver, and in skeletal muscle, is exchanged between white-glycolytic and red-oxidative fibers depending on the physiological state [9]. Further, lactate uptake is mediated by monocarboxylate transport (MCT) proteins, and the expression of MCT isoforms depends on muscle fiber type [35]. In our study, we measured total skeletal muscle mass and calculated SMI, but did not investigate the proportion of fast and slow muscle fibers or the expression level of MCTs in individuals, and therefore, it may be necessary to add molecular biological assessments related to lactate production, consumption, transport, and skeletal muscle mass for future studies. In addition, the design of this study only allowed the assessment of the relationship between peak SLa levels and physical parameters measurable in a clinical setting, without explicit consideration of the mechanism. The next step will be to examine how body fat and body water content, which were significantly associated with SLa as independent variables in this study, are circulated in the body and released into saliva after production by exercise. Based on the results of this study, however, we believe that training guidance can be provided to patients regarding body fat and body water content in clinical practice. Specifically, body fat ratio and body water content were shown to be positively and negatively related to SLa, respectively, indicating that weight loss and proper water intake could also be effective in improving aerobic capacity.
Limitations
This study has several limitations. First, as we assessed only healthy young males it is unclear whether these results can be applied to females, as it has been reported that salivary hormone levels, ultrastructure, pH, flow rate, buffering capacity, and electrolyte levels change during the menstrual cycle [36]. In addition to sex differences, aging reduces saliva production and changes the surface tension and viscosity of saliva, which may also affect SLa levels [37]. Second, we performed measurements at 5-min intervals after observing that subjects had difficulty salivating after high-intensity SJ exercises in a pilot study. Further consideration measurement intervals are needed to ensure capture of peak SLa levels. It is also necessary to consider the absence of a consensus on stimulating saliva production, with various methods (acidic-based stimulation, chewing gum, gargling, etc.) used to date [21].
Conclusions
This study demonstrated that body fat, body water content, and SMI impacted peak SLa by 31.2%. SLa increased significantly with higher body fat and decreased significantly with higher body water content. Clinically, these findings enable more tailored nutritional advice and suggest that patients who do not show sufficient SLa decreases despite participating in a rehabilitation program may require additional advice on dietary and water consumption habits. Further studies on the mechanism by which lactate produced by skeletal muscles is released into saliva during exercise and the relationship of BLa and circulating kinetics are warranted.
Availability of data and materials
Data are available upon reasonable request, as we are analyzing this data in another study. The data that support the findings of this study are available upon request from the corresponding author.
Abbreviations
- BLa :
-
Blood lactate
- LT :
-
Lactate threshold
- SLa :
-
Salivary lactate
- SMI :
-
Skeletal muscle mass index
- SJ :
-
Squat jump
- HR :
-
Heart rate
- MCT :
-
Monocarboxylate transport
References
Costill DL. Metabolic responses during distance running. J Appl Physiol. 1970;28(3):251–5.
Stratton JR, Levy WC, Cerqueira MD, Schwartz RS, Abrass IB. Cardiovascular responses to exercise. Effects of aging and exercise training in healthy men. Circulation. 1994;89(4):1648–55.
Seals DR, Hagberg JM, Hurley BF, Ehsani AA, Holloszy JO. Endurance training in older men and women. I. Cardiovascular responses to exercise. J Appl Physiol Respir Environ Exerc Physiol. 1984;57(4):1024–9.
Goodwin GM, McCloskey DI, Mitchell JH. Cardiovascular and respiratory responses to changes in central command during isometric exercise at constant muscle tension. J Physiol. 1972;226(1):173–90.
Wasserman K, Whipp BJ, Koyl SN, Beaver WL. Anaerobic threshold and respiratory gas exchange during exercise. J Appl Physiol. 1973;35(2):236–43.
Heuberger J, Gal P, Stuurman FE, de Muinck Keizer WAS, Mejia Miranda Y, Cohen AF. Repeatability and predictive value of lactate threshold concepts in endurance sports. PLoS One. 2018;13(11):e0206846.
Feijen S, Tate A, Kuppens K, Barry LA, Struyf F. Monitoring the swimmer’s training load: a narrative review of monitoring strategies applied in research. Scand J Med Sci Sports. 2020;30(11):2037–43.
Adeva-Andany M, López-Ojén M, Funcasta-Calderón R, Ameneiros-Rodríguez E, Donapetry-García C, Vila-Altesor M, et al. Comprehensive review on lactate metabolism in human health. Mitochondrion. 2014;17:76–100.
Brooks GA. The science and translation of lactate shuttle theory. Cell Metab. 2018;27(4):757–85.
Proia P, Di Liegro CM, Schiera G, Fricano A, Di Liegro I. Lactate as a metabolite and a regulator in the central nervous system. Int J Mol Sci. 2016;17(9):1450.
Santos RV, Almeida AL, Caperuto EC, Martins E, Jr., Costa Rosa LF. Effects of a 30-km race upon salivary lactate correlation with blood lactate. Comp Biochem Physiol B Biochem Mol Biol. 2006;145(1):114–7.
Ferguson BS, Rogatzki MJ, Goodwin ML, Kane DA, Rightmire Z, Gladden LB. Lactate metabolism: historical context, prior misinterpretations, and current understanding. Eur J Appl Physiol. 2018;118(4):691–728.
Leal Junior EC, Lopes-Martins RA, Vanin AA, Baroni BM, Grosselli D, De Marchi T, et al. Effect of 830 nm low-level laser therapy in exercise-induced skeletal muscle fatigue in humans. Lasers Med Sci. 2009;24(3):425–31.
Forsyth JJ, Farrally MR. A comparison of lactate concentration in plasma collected from the toe, ear, and fingertip after a simulated rowing exercise. Br J Sports Med. 2000;34(1):35–8.
Segura R, Javierre C, Ventura JL, Lizarraga MA, Campos B, Garrido E. A new approach to the assessment of anaerobic metabolism: measurement of lactate in saliva. Br J Sports Med. 1996;30(4):305–9.
Tekus E, Kaj M, Szabo E, Szenasi NL, Kerepesi I, Figler M, et al. Comparison of blood and saliva lactate level after maximum intensity exercise. Acta Biol Hung. 2012;63 Suppl 1:89–98.
Miller AT, Jr., Miller JO, Jr. Renal excretion of lactic acid in exercise. J Appl Physiol. 1949;1(8):614–8.
McKelvie RS, Lindinger MI, Heigenhauser GJ, Sutton JR, Jones NL. Renal responses to exercise-induced lactic acidosis. Am J Physiol. 1989;257(1 Pt 2):R102–8.
Derbyshire PJ, Barr H, Davis F, Higson SP. Lactate in human sweat: a critical review of research to the present day. J Physiol Sci. 2012;62(6):429–40.
Sakharov DA, Shkurnikov MU, Vagin MY, Yashina EI, Karyakin AA, Tonevitsky AG. Relationship between lactate concentrations in active muscle sweat and whole blood. Bull Exp Biol Med. 2010;150(1):83–5.
Lindsay A, Costello JT. Realising the potential of urine and saliva as diagnostic tools in sport and exercise medicine. Sports Med. 2017;47(1):11–31.
Wisløff U, Castagna C, Helgerud J, Jones R, Hoff J. Strong correlation of maximal squat strength with sprint performance and vertical jump height in elite soccer players. Br J Sports Med. 2004;38(3):285–8.
Loturco I, Pereira LA, Moraes JE, Kitamura K, Cal Abad CC, Kobal R, et al. Jump-squat and half-squat exercises: selective influences on speed-power performance of elite rugby sevens players. PLoS One. 2017;12(1):e0170627.
Chmielewski TL, George SZ, Tillman SM, Moser MW, Lentz TA, Indelicato PA, et al. Low- versus high-intensity plyometric exercise during rehabilitation after anterior cruciate ligament reconstruction. Am J Sports Med. 2016;44(3):609–17.
Yui J, Okano S, Nishizawa H. Relationship between skeletal muscle mass and blood lactate level reduction after short squat jumps in healthy adult non-athletes. J Phys Ther Sci. 2021;33(10):717–21
Okano S, Nishizawa H, Yui J, Yokokawa Y, Koinuma M, Nakamura A. Convergent validity of a simplified device and relationship between blood lactate and salivary lactate after a vertical squat jump in healthy non-athletes. J Phys Ther Sci. 2021;33(3):187–93.
Gill SK, Price M, Costa RJ. Measurement of saliva flow rate in healthy young humans: influence of collection time and mouthrinse water temperature. Eur J Oral Sci. 2016;124(5):447–53.
Borg G. Borg’s perceived exertion and pain scales. Human Kinetics; 1998. pp. 39–43.
Taniguchi Y, Makizako H, Kiyama R, Tomioka K, Nakai Y, Kubozono T, et al. The association between osteoporosis and grip strength and skeletal muscle mass in community-dwelling older women. Int J Environ Res Public Health. 2019;16(7):1228.
Ohkuwa T, Itoh H, Yamazaki Y, Sato Y. Salivary and blood lactate after supramaximal exercise in sprinters and long-distance runners. Scand J Med Sci Sports. 1995;5(5):285–90.
Reer R, Philipp S, Marc Z, Tobias S, Detlef L, Von Duvillard SP, Braumann KM. Comparison of blood vs. saliva lactate measurements resulting from lactate minimum vs. constant load tests: 2177. Med Sci Sports Exerc. 2009;41(5):258.
Jansson PA, Larsson A, Smith U, Lönnroth P. Lactate release from the subcutaneous tissue in lean and obese men. J Clin Invest. 1994;93(1):240–6.
Petersen C, Nielsen MD, Andersen ES, Basse AL, Isidor MS, Markussen LK, et al. MCT1 and MCT4 expression and lactate flux activity increase during white and brown adipogenesis and impact adipocyte metabolism. Sci Rep. 2017;7(1):13101.
Sabater D, Arriarán S, Romero Mdel M, Agnelli S, Remesar X, Fernández-López JA, et al. Cultured 3T3L1 adipocytes dispose of excess medium glucose as lactate under abundant oxygen availability. Sci Rep. 2014;4:3663.
Coles L, Litt J, Hatta H, Bonen A. Exercise rapidly increases expression of the monocarboxylate transporters MCT1 and MCT4 in rat muscle. J Physiol. 2004;561(Pt 1):253–61.
Saibaba G, Srinivasan M, Priya Aarthy A, Silambarasan V, Archunan G. Ultrastructural and physico-chemical characterization of saliva during menstrual cycle in perspective of ovulation in human. Drug Discov Ther. 2017;11(2):91–7.
Bel’skaya LV, Sarf EA, Kosenok VK. Age and gender characteristics of the biochemical composition of saliva: correlations with the composition of blood plasma. J Oral Biol Craniofac Res. 2020;10(2):59–65.
Acknowledgements
Not applicable.
Funding
This study was supported by an Intramural Research Grant (26-6) for Neurological and Psychiatric Disorders of the National Center of Neurology and Psychiatry, and Grant-in-Aid for Scientific Research (19K12862 to HN).
Author information
Authors and Affiliations
Contributions
SO, HN, and AN designed the study and protocol. SO, HN, and JY performed the data collection, including the pilot study. The manuscript was written by SO, HN, and AN. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study protocols were reviewed and approved by the Medical Ethics Committee of Shinshu University School of Medicine (approval no. 4120). This study adhered to ethical principles under the Declaration of Helsinki. Informed consent was obtained from all participants after they were informed of the purpose and associated risks of this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Okano, S., Nishizawa, H., Yui, J. et al. Impact of body fat, body water content, and skeletal muscle mass index on peak salivary lactate levels after squat jump exercise in healthy non-athlete adult males. BMC Sports Sci Med Rehabil 14, 91 (2022). https://doi.org/10.1186/s13102-022-00482-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-022-00482-6