
Abstract
Background
Few studies have compared the correlation between visceral fat area (VFA) and abdominal subcutaneous fat area (SFA) with arterial stiffness (AS) in patients with type 2 diabetes (T2D). In addition, there is currently controversy regarding the correlation between VFA and SFA with AS. We aimed to investigate the relationship between VFA and SFA with AS in patients with T2D.
Methods
In this cross-sectional study, 1475 Chinese T2D patients with an average age of 52.32 ± 10.96 years were included. VFA and SFA were determined by a dual bioelectrical impedance analyzer, and AS was determined by measurement of brachial-ankle pulse wave conduction velocity (baPWV). Atherosclerosis was deemed present in study participants with baPWV values higher than 75th percentile (1781 cm/s). Independent correlations of logVFA and logSFA with AS were assessed using multiple linear regression and multivariate logistic regression.
Results
The baPWV was linked with VFA, waist circumference, and women’s SFA in a general linear correlation study (P < 0.05), but not with body mass index (P = 0.3783) or men’s SFA (P = 0.1899). In both men and women, VFA and SFA were positively correlated with AS, according to the generalized additive model (GAM). After fully adjusting for confounders, multiple linear regression analyses showed that for every 1-unit increase in logVFA, the beta coefficient of baPWV increased by 63.1 cm/s (95% CI: 18.4, 107.8) (P < 0.05). logSFA did not correlate significantly with baPWV (P = 0.125). In the multiple logistic regression analysis, the odds ratio (OR) of elevated baPWV was 1.8 (95% CI: 1.1, 3.1) (P = 0.019) per 1-unit increase in logVFA. logSFA did not correlate significantly with AS (P = 0.091). In the subgroup analysis, the correlation between logVFA and baPWV did not interact across subgroups (P-interaction > 0.05).
Conclusions
Compared with SFA, VFA had a stronger independent positive correlation with AS in Chinese T2D patients. Patients with T2D should pay more attention to monitoring VFA and lowering it to minimize cardiovascular events.
Similar content being viewed by others


Introduction
Currently, cardiovascular disease (CVD) remains the leading cause of death in patients with diabetes. Since diabetics often combine important risk factors for CVD, such as hypertension and dyslipidemia, they have a two- to four-fold increased risk of developing CVD [1]. Studies have shown that the prevalence of diabetes is increasing, reaching 10.5% of adults globally in 2021, or 536.6 million people, and this number is expected to increase by 51% by 2045 [2]. In addition, there are racial differences in genetic susceptibility to type 2 diabetes (T2D) among Chinese. Compared with Caucasians, Asian populations have a 60% increased risk of diabetes [3]. Arterial stiffness (AS) is a significant CVD event risk factor that is closely linked to the emergence and progression of diabetes complications.
Cardiovascular risk is associated with the location of abdominal fat accumulation, which is composed of two main components: the visceral fat area (VFA) and the abdominal subcutaneous fat area (SFA) [4]. The majority of earlier research, which was done on healthy populations, primarily examined the relationship between VFA and AS only and did not consider the effect of SFA on the results. The correlation between SFA and AS is currently understudied and still controversial [5,6,7,8]. In addition, the correlation of VFA and SFA with AS has been less well reported in a special population of Chinese patients with T2D, who are more prone to insulin resistance (IR), hyperinsulinemia, and abnormal accumulation of fat than healthy individuals. Although the total obesity rate of Asians is lower than that of Africans and Caucasians, Asians are more prone to VFA accumulation. A complex combination of factors, including the sedentary lifestyle of the Chinese, reduced physical activity, and specific dietary patterns (e.g., refined carbohydrates and higher saturated fats), may lead to increased AS and a higher incidence of CVD [4, 9].
Numerous studies have demonstrated that AS has a stronger correlation with abdominal obesity than with overall obesity, despite the fact that obesity is a major risk factor for CVD [10]. Adults in China with a body mass index (BMI) ≥ 28 kg/m2 are defined as overall obesity. Men with a waist circumference (WC) ≥ 90 cm and women with a WC ≥ 85 cm are defined as abdominal obesity [11]. Some studies have shown a stronger correlation between VFA and AS than BMI and WC [12, 13], while others have reported no significant correlation between BMI and WC and AS [5, 6, 10, 14]. Due to the inability of BMI and WC to differentiate body fat distribution, the aim of this study was to compare the correlation of VFA and SFA with AS in patients with T2D in order to identify the risk factors for CVD. This will provide a practical approach and theoretical foundation for T2D patients’ CVD prevention.
Materials and methods
Study design and participants
Data were collected from May 1, 2020, to January 31, 2022, for this study. Participants’ data were collected by the Metabolic Management Center (MMC) in accordance with China’s national standards at the First People’s Hospital of Changde City, Hunan Province [15]. 1665 people with diabetes, ages 18 to 80, who fulfilled the 2020 American Diabetes Association’s diagnostic criteria for the disease were included in this cross-sectional study. Diabetes mellitus is defined as fasting plasma glucose (FPG) ≥ 7.0 mmol/L, 2 h postprandial plasma glucose (PPG) ≥ 11.1 mmol/L, or glycated hemoglobin (HbA1c) ≥ 6.5% [16]. Patients with type 1 diabetes (n = 18), age < 18 years (n = 3), other types of diabetes (n = 5), malignancy (n = 10), missing baPWV data (n = 44), low ankle-brachial index (< 0.9) (n = 12), and no bioelectrical impedance analysis (BIA) measurements performed (n = 98) were among the exclusion criteria. A final total of 1475 patients aged 18 to 80 diagnosed with T2D were included.
Measurements of variables
All variables were measured and registered by trained researchers using standardized questionnaires, including sex, age, smoking (never, former, or current), alcohol consumption (never, former, or current), work status, duration of diabetes mellitus, antihyperlipidemic medication, antihypertensive medication, antihyperglycemic medication, as well as menopause status. Height and weight were measured after removing shoes; a non-elastic tape measure was used to measure the WC; and after the individual had been sitting motionless for at least five minutes, the average of the two measurements of systolic blood pressure (SBP) and diastolic blood pressure (DBP) [13]. The formula for calculating BMI was weight in kilograms divided by height in square meters. Laboratory data, including total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), FPG, fasting C peptide (FCP), and HbA1c, were measured after participants fasted overnight for at least 12 h. PPG was obtained by taking venous blood samples 2 h after the steamed bun meal and was used to assess the post-load blood glucose.
Measurement of VFA and SFA
VFA and SFA were measured by a trained physician using a dual BIA (HDS-2000 DUALSCAN; Omron Healthcare, Kyoto, Japan) after subjects had fasted for at least 12 h [17]. The gadget measures the surface impedance of the body and the torso using a bioelectrical impedance assembly, and it also includes an abdominal dimension measurement device. Four limb electrodes were clamped to the wrists and ankles to measure trunk impedance by current and voltage, and a belt containing the electrodes was wrapped along the umbilicus to measure surface impedance. The instrument automatically calculates the body fat content based on the time and intensity of the current passage.
Assessment of baPWV
In this study, we used the baPWV to show whether a patient had atherosclerosis or not [18]. The baPWV measures were taken by the technician using an automatic atherosclerosis detection instrument (model HBP-8000, Omron Healthcare (China) Co., Ltd.) while the subjects were resting in the supine position for a minimum of five minutes. The device automatically calculated the distance from the humerus to the ankle based on the subject’s height. The arm band of the automatic recording instrument was wrapped 2–3 cm above the crossbar of the elbow socket, and the ankle band was wrapped 1–2 cm above the inner ankle. The machine automatically measures the time difference between the systolic pulse waveforms. The baPWV was computed by dividing the distance between the two spots by the time difference [2, 19]. We used the average of the left and right sides of the baPWV for analysis [20]. AS was defined as an individual whose baPWV value was higher than the study’s 75th percentile (baPWV > 1781 cm/s) [4, 21, 22].
Statistical analysis
To characterize the distribution of participants’ characteristics, the study population was divided into two groups according to gender. Continuous variables were expressed as mean ± standard deviation (normal distribution) or median (quartile 1-quartile 3) (skewed distribution) and were compared between males and females using analysis of variance or the Kruskal-Wallis H test. Categorical variables were expressed as numbers (percentages), and differences between males and females were tested using the chi-square test or Fisher’s exact test. The association of VFA, SFA, BMI, and WC with baPWV was examined using Pearson’s correlation analysis. Generalized additive modeling (GAM) was used to investigate the relationships between VFA and SFA with baPWV in both men and women. In multiple linear regression and multivariate logistic regression, we transformed VFA and SFA into natural logarithms [23], and we constructed 4 models: Model 1 for adjusted age and sex; model 2 added SBP, DBP, BMI, smoking, alcohol consumption, and work status to the previous model; model 3 added HbA1c, TC, TG, HDL-C, and LDL-C to the previous model; and model 4 added FPG, PPG, FCP, glucose-lowering medication, antihypertensive medication, lipid-lowering medications, diabetes duration, logSFA (model 4 of logVFA), and logVFA (model 4 of logSFA) to the previous model. Multiple linear regression was used to describe the independent associations between logVFA and logSFA with baPWV. Multivariate logistic regression assessed the independent associations of VFA and SFA quartiles with increased AS in patients with T2D. Furthermore, we conducted interaction tests and subgroup analyses to examine the relationship between VFA and AS. Statistical analyses were performed using R version 4.2.0 and EmpowerStats version 4.0.
Results
Participants’ characteristics
A total of 1475 patients with T2D were included in this cross-sectional study for analysis; the mean age of the total population was 52.32 ± 10.96 years, of which 854 (57.90%) were male and 621 (42.10%) were female; 157 were menopausal and 464 were non-menopausal among the females. Table 1 describes the characteristics of the participants by comparing different genders. There were no significant differences in SFA, FPG, PPG, FCP, LDL-C, and use of antihypertensive medication between males and females; compared to females, males had a higher BMI, WC, VFA, DBP, TG, and a higher proportion of 47.95% with smoking, 40.73% with alcohol use, 76.76% with a job, and 14.92% with the use of lipid-lowering medication, whereas age, SBP, TC, HDL-C, duration of diabetes, baPWV, and the proportion of 83.14% with the use of glucose-lowering drugs were lower.
Correlation of logVFA and logSFA with baPWV
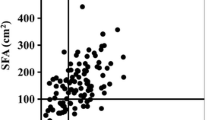
In the Pearson’s correlation analysis in Table 2, baPWV was linked to VFA, WC, and women’s SFA, but not with BMI (P = 0.3783) or men’s SFA (P = 0.1899). In Fig. 1, these relationships are displayed as scatter plots. We analyzed the correlation of VFA and SFA with baPWV by GAM, and after adjusting for all confounders (Fig. 2A with the addition of the confounder SFA and Fig. 2B with the addition of the confounder VFA), we found that VFA (Fig. 2A) and SFA (Fig. 2B) were positively correlated with baPWV in both men and women. We found in Table 3 by logistic regression modeling that for each 1-unit increase in logVFA and logSFA in model 4 fully adjusted for confounders, the beta coefficient (β) of baPWV increased by 63.1 cm/s (95% confidence interval (CI): 18.4, 107.8) (P < 0.05) and 82.4 cm/s (95% CI: -22.8, 187.5) (P = 0.125). The logVFA and logSFA quartiles were further grouped and placed as categorical variables in a logistic regression model, with the first group serving as the reference group; in Model 4, the beta coefficients of baPWV were increased by 103.0 cm/s (95% CI: 29.1, 176.9) (P for trend = 0.005) and 79.6 cm/s (95% CI: -2.7, 162.0) (P for trend = 0.195).

Scatter plots illustrate the relationship between baPWV and body fat parameters in males and females

Generalized additive modeling of the relationship between VFA (A) and SFA (B) with baPWV across sexes after adjustment for age, SBP, DBP, BMI, smoking, alcohol consumption, work status, HbA1c, TC, TG, HDL-C, LDL-C, FPG, PPG, FCP, glucose-lowering medication, antihypertensive medication, lipid-lowering medications, diabetes duration, SFA (in figure B), and VFA (in figure A)
Correlation of logVFA and logSFA with increased AS
As shown in Table 4, the risk of AS increased by 50% for each 1-unit increase in logVFA in model 4, fully adjusted by multivariable logistic regression, with an odds ratio (OR) of 1.8 (95% CI: 1.1, 3.1) for elevated baPWV (P = 0.019). The logVFA quartiles were further grouped, with the first group serving as the reference group. Results showed that in model 4, adjusted for all confounders, the OR (95% CI) for elevated baPWV was 2.2 (1.2, 3.9), 1.8 (0.9, 3.5), and 2.6 (1.2, 5.5) for groups 2, 3, and 4, respectively, compared with the reference group. The risk of increased AS was statistically significant (P for trend = 0.042). However, we found an OR of 2.4 (95% CI: 0.9, 6.9) for each 1-unit increase in logSFA for elevated baPWV, a result that was not statistically significant (P = 0.091). Furthermore, no significant correlation was found between logSFA and the risk of increased AS in model 2 (P for trend = 0.146), model 3 (P for trend = 0.242), or the fully adjusted model 4 (P for trend = 0.299), according to the results of the logSFA quartile groupings.
Subgroup analysis of logVFA and increased risk of AS
To further explore the correlation between logVFA and increased AS in different populations, we performed subgroup analyses (Fig. 3). logVFA was positively associated with the risk of increased AS in all subgroups except the DBP ≥ 90 mmHg group. We dichotomized the SFA groups, and subgroup analyses showed a positive correlation between logVFA and AS in both the low and high SFA groups. After excluding the stratification factor itself and adjusting for effect modifiers, there was no interaction between subgroups (P interaction > 0.05), and the results were stable. Although logVFA was negatively associated with an increased risk of AS at DBP ≥ 90 mmHg and positively associated at DBP < 90 mmHg, there was no interaction in this subgroup (P interaction = 0.0972).

Subgroup analyses for the association between logVFA and elevated baPWV were adjusted for age, sex, SBP, DBP, BMI, smoking, alcohol consumption, work status, HbA1c, TC, TG, HDL-C, LDL-C, FPG, PPG, FCP, glucose-lowering medication, antihypertensive medication, lipid-lowering medications, diabetes duration, and logSFA, except for the stratified variable
Discussion
In this study, the correlation between VFA and SFA with AS in patients with T2D was assessed by baPWV. This cross-sectional study showed a significant positive and dose-response relationship between VFA and baPWV in both males and females, while the dose-response relationship between SFA and baPWV was not significant in males. Furthermore, in multiple logistic regression model 1, We found that VFA and SFA were significantly positively correlated with AS when adjusting only for age and sex, but after adjusting for all confounders, the positive correlation between VFA and AS remained significant; however, the positive correlation between SFA and AS was not significant. Our study confirms a stronger, independent positive association between VFA and an increased risk of AS compared to SFA.
Abdominal fat consists of internal VFA and SFA, and abdominal obesity has a stronger correlation with AS than does total obesity [10]. However, most of the previous studies have only discussed the correlation between VFA and AS, and only a smaller number of studies have compared the correlation between VFA and SFA with AS. The sample sizes of these studies were small, and in addition, there is currently controversy regarding the correlation between SFA and AS [5,6,7,8].
The study by Ryotaro et al. included 148 T2D patients (mean age 65 ± 12 years) in China. The study showed that high VFA and low SFA are determinants of AS in patients with T2D, and high SFA protects against AS in patients with T2D. However, the study used carotid intima-media thickness (CIMT) to assess AS [7]. This is different from our results. This may be related to the different methods used in this study-like assessment of AS. Alterations in the intimal, middle, and tunica layers of the vasculature, both structurally and functionally, are linked to AS. It is controlled by elements coming from various levels of the vessel wall as well as chemicals like insulin and aldosterone in plasma [24]. Studies have shown that CIMT is mainly used as a measure of localized vascular lesions, whereas baPWV is currently used as a measure of AS [25,26,27]. A study by Amparo et al. that included 415 European Americans with an average age of 55 years old confirmed that VFA was independently associated with increased AS and was an independent predictor of CVD, while SFA and BMI did not predict CVD [5]. Another study by Melanie et al. involved 44 early T2D patients between the ages of 30 and 70. They found that VFA was an independent risk factor for arterial inflammation (a marker of early AS), whereas SFA was not. In addition, WC was not associated with arterial inflammation. The study demonstrated that, in comparison to SFA, VFA was more strongly related to early AS in T2D patients [6]. This is consistent with our findings. Studies have shown that both BMI, which assesses overall obesity, and WC, which assesses central obesity, do not correlate as strongly with AS as VFA [12, 13], and a large number of studies have reported no significant correlation between BMI and WC and AS [5, 6, 10, 14]. Furthermore, numerous previous studies have shown that the visceral adiposity index (VAI), which responds to visceral fat, is independently and positively correlated with AS [28,29,30]. In a study involving 5921 Persian adults, Zahra et al. found that among overweight men and women, as well as obese women, VFA linked better with AS than VAI, BMI, and WC [31]. The VAI, which includes lipid-related metabolic markers (TG and HDL-C) and anthropometric indices (BMI and WC), is a newly developed visceral fat index that is thought to be able to depict the distribution of fat [28], but the VFA predicts AS risk better than it. Visceral fat accumulation is more common in men and menopausal women, while subcutaneous fat accumulation is more common in women who are not menopausal [32, 33]. Through the use of general linear correlation analysis, we discovered that baPWV had a stronger association with VFA than with WC, but not with BMI. In women, baPWV is correlated with SFA, but not in men. Because of the different fat distribution in men and women, we found that VFA was significantly and positively linked with AS in both men and women by subgroup analysis. Furthermore, we performed subgroup analyses of whether women were menopausal or not, taking into account changes in hormone levels and altered lipid metabolism in women before and after menopause due to changes in hormone levels in the body [34], and it was discovered that in both menopausal and non-menopausal women, VFA was positively correlated with AS.
Our study found a stronger correlation between VFA than SFA and AS, probably because visceral adipose tissue (VAT) is composed of larger, insulin-resistant adipocytes, which are mainly distributed in the abdominal cavity organs such as the liver and heart [35]. Research has indicated that an increase in VAT also significantly increases the portal vein’s ability to transfer free fatty acids into the liver, which can lead to hepatic IR and elevated LDL-C production and release [8]. Subcutaneous adipose tissue (SAT), which is mainly distributed between the dermis and the fascia, secretes more leptin and lipocalin than VAT and promotes glucose and lipid metabolism [36]. Insulin sensitivity and glucose tolerance were observed to improve in animal trials when SAT was transplanted into the visceral cavity [37]. VAT produces pro-inflammatory cytokines, recruiting more pro-inflammatory macrophages and secreting more vasoconstrictive mediators than SAT [4, 38, 39]. Studies have shown that in people with the same BMI, the risk of CVD increases with the accumulation of visceral fat [40]. In our subgroup analysis, we found that using the Chinese diagnostic criteria for obesity, when the BMI used to diagnose overall obesity was normal (< 24 kg/m2) and when the WC used to diagnose central obesity was normal (men < 90 cm and women < 85 cm), VFA remained positively linked to AS after all confounders were excluded. Although the occurrence of CVD events is more prominent in obese T2D patients, this study found that VFA is an independent risk factor for CVD in T2D patients with normal weight. Therefore, physicians should pay attention to the monitoring of VFA in T2D patients when treating diabetes mellitus to reduce the occurrence of CVD events.
Our study does, however, have certain limitations. Firstly, because it is cross-sectional in nature, it is not possible to draw conclusions about the causal relationship between VFA and SFA with baPWV. Secondly, this study used BIA to measure VFA and SFA. A more objective assessment of the buildup of abdominal fat necessitates abdominal computed tomography or magnetic resonance imaging measurements. However, accumulating evidence has confirmed that the BIA is more cost-effective, simple to perform, and non-invasive in estimating VFA and SFA in diabetic patients [41,42,43,44]. Thirdly, recall bias cannot be completely ruled out due to this study design, but future follow-up data from MMC may provide more precise evidence. Finally, this study only included Chinese patients with T2D; more research is required to determine whether the findings apply to people of other races.
Conclusions
Our study showed that VFA was significantly positively associated with AS and stronger than SFA in patients with T2D. After adjusting for confounders, VFA remained significantly and independently positively associated with AS, whereas SFA was not significantly associated with AS. Therefore, we further emphasize the importance of monitoring and lowering VFA in patients with T2D to reduce the risk of CVD.
Data availability
The corresponding author will provide raw data supporting the conclusions of this paper without reservation upon reasonable request.
Abbreviations
- VFA:
-
Visceral fat area
- SFA:
-
Subcutaneous fat area
- AS:
-
Arterial stiffness
- T2D:
-
Type 2 diabetes
- baPWV:
-
Brachial-ankle pulse wave conduction velocity
- GAM:
-
Generalized additive model
- CI:
-
Confidence interval
- CVD:
-
Cardiovascular disease
- BIA:
-
Bioelectrical impedance analysis
- IR:
-
Insulin resistance
- BMI:
-
Body mass index
- WC:
-
Waist circumference
- MMC:
-
Metabolic Management Center
- FPG:
-
Fasting plasma glucose
- HbA1c:
-
Glycated hemoglobin
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- FCP:
-
Fasting C peptide
- PPG:
-
Postprandial plasma glucose
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- β:
-
Beta coefficient
- OR:
-
Odds ratio
- CIMT:
-
Carotid intima-media thickness
- VAT:
-
Visceral adipose tissue
- SAT:
-
Subcutaneous adipose tissue
References
Mosenzon O, Alguwaihes A, Leon JLA, Bayram F, Darmon P, Davis TME, et al. CAPTURE: a multinational, cross-sectional study of cardiovascular disease prevalence in adults with type 2 diabetes across 13 countries. Cardiovasc Diabetol. 2021;20:154.
Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119.
Wang L, Gao P, Zhang M, Huang Z, Zhang D, Deng Q, et al. Prevalence and ethnic pattern of diabetes and Prediabetes in China in 2013. JAMA. 2017;317:2515.
Koenen M, Hill MA, Cohen P, Sowers JR. Obesity, adipose tissue and vascular dysfunction. Circ Res. 2021;128:951–68.
Figueroa AL, Takx RAP, MacNabb MH, Abdelbaky A, Lavender ZR, Kaplan RS et al. Relationship Between Measures of Adiposity, Arterial Inflammation, and Subsequent Cardiovascular Events. Circ: Cardiovascular Imaging. 2016;9:e004043.
Reijrink M, De Boer SA, Spoor DS, Lefrandt JD, Lambers Heerspink HJ, Boellaard R, et al. Visceral adipose tissue volume is associated with premature atherosclerosis in early type 2 diabetes mellitus independent of traditional risk factors. Atherosclerosis. 2019;290:87–93.
Bouchi R, Takeuchi T, Akihisa M, Ohara N, Nakano Y, Nishitani R, et al. High visceral fat with low subcutaneous fat accumulation as a determinant of atherosclerosis in patients with type 2 diabetes. Cardiovasc Diabetol. 2015;14:136.
Lee JJ, Pedley A, Hoffmann U, Massaro JM, Levy D, Long MT. Visceral and Intrahepatic Fat Are Associated with cardiometabolic risk factors above other ectopic Fat depots: the Framingham Heart Study. Am J Med. 2018;131:684–e69212.
Wang Y, Zhao L, Gao L, Pan A, Xue H. Health policy and public health implications of obesity in China. Lancet Diabetes Endocrinol. 2021;9:446–61.
Kim H-L, Ahn D-W, Kim SH, Lee DS, Yoon SH, Zo J-H, et al. Association between body fat parameters and arterial stiffness. Sci Rep. 2021;11:20536.
Zhu J, Zhang Y, Wu Y, Xiang Y, Tong X, Yu Y, et al. Obesity and Dyslipidemia in Chinese adults: a cross-sectional study in Shanghai, China. Nutrients. 2022;14:2321.
Zhang J, Fang L, Qiu L, Huang L, Zhu W, Yu Y. Comparison of the ability to identify arterial stiffness between two new anthropometric indices and classical obesity indices in Chinese adults. Atherosclerosis. 2017;263:263–71.
Li G, Yao T, Wu X, Cao Z, Tu Y, Ma Y, et al. Novel and traditional anthropometric indices for identifying arterial stiffness in overweight and obese adults. Clin Nutr. 2020;39:893–900.
Xu K, Zheng Q, Shao J, Yang L, Dai Y, Zhang J, et al. Sex differences in the association between visceral adipose tissue and atherosclerosis in type 2 diabetes patients with normal bodyweight: a study in a Chinese population. J Diabetes Invest. 2023;14:92–101.
Zhang Y, Wang W, Ning G. Metabolic Management Center: an innovation project for the management of metabolic diseases and complications in China. J Diabetes. 2019;11:11–3.
American Diabetes Association. 6. Glycemic, Targets. Standards of Medical Care in Diabetes—2020. Diabetes Care. 2020;43 Supplement_1:S66–76.
Huang H, Jin J, Chen Y, Wang L, Zhong J, Chen Z, et al. Visceral fat might impact left ventricular remodeling through changes in arterial stiffness in type 2 diabetes: a cross-sectional study. Int J Cardiol. 2022;368:78–84.
Mazidi M, Kengne A-P, Katsiki N, Mikhailidis DP, Banach M. Lipid accumulation product and triglycerides/glucose index are useful predictors of insulin resistance. J Diabetes Complicat. 2018;32:266–70.
Hill MA, Yang Y, Zhang L, Sun Z, Jia G, Parrish AR, et al. Insulin resistance, cardiovascular stiffening and cardiovascular disease. Metabolism. 2021;119:154766.
Baba M, Maris M, Jianu D, Luca CT, Stoian D, Mozos I. The impact of the blood lipids levels on arterial stiffness. JCDD. 2023;10:127.
Wang S, Shi J, Peng Y, Fang Q, Mu Q, Gu W, et al. Stronger association of triglyceride glucose index than the HOMA-IR with arterial stiffness in patients with type 2 diabetes: a real-world single-centre study. Cardiovasc Diabetol. 2021;20:82.
Lu S, Li Y, Qian Z, Zhao T, Feng Z, Weng X, et al. Role of the inflammasome in insulin resistance and type 2 diabetes mellitus. Front Immunol. 2023;14:1052756.
Hayashi Y, Yokokawa H, Fukuda H, Saita M, Miyagami T, Takahashi Y, et al. Association between Visceral or Subcutaneous Fat Accumulation and B-Type Natriuretic peptide among Japanese subjects: a cross-sectional study. JCM. 2021;10:1315.
Sowers JR, Habibi J, Aroor AR, Yang Y, Lastra G, Hill MA, et al. Epithelial sodium channels in endothelial cells mediate diet-induced endothelium stiffness and impaired vascular relaxation in obese female mice. Metabolism. 2019;99:57–66.
Wu Z, Zhang H, Wang Y, Li Z, Li X, Tao L, et al. Temporal and Bidirectional Association between blood pressure variability and arterial Stiffness: Cross-lagged Cohort Study. JMIR Public Health Surveill. 2023;9:e45324.
Song Q, Ling Q, Bai J, Zhang H, Bu P, Chen F, et al. Influence of baseline arterial stiffness on effects of intensive compared with standard blood pressure control: a post hoc analysis of the STEP trial. BMC Med. 2022;20:358.
Willeit P, Tschiderer L, Allara E, Reuber K, Seekircher L, Gao L, et al. Carotid intima-media thickness progression as surrogate marker for Cardiovascular Risk: Meta-Analysis of 119 clinical trials involving 100 667 patients. Circulation. 2020;142:621–42.
Li J, Zhu J, Tan Z, Yu Y, Luo L, Zhou W, et al. Visceral adiposity index is associated with arterial stiffness in hypertensive adults with normal-weight: the China H-type hypertension registry study. Nutr Metab (Lond). 2021;18:90.
Xu C, Zhao S, Yu S, Chi C, Fan X, Ji H, et al. Association between organ damage and visceral adiposity index in community-dwelling elderly Chinese population: the Northern Shanghai Study. Aging Clin Exp Res. 2021;33:2291–7.
Bagyura Z, Kiss L, Lux Á, Csobay-Novák C, Jermendy ÁL, Polgár L, et al. Association between coronary atherosclerosis and visceral adiposity index. Nutr Metabolism Cardiovasc Dis. 2020;30:796–803.
Ataee Z, Aghaee A, Sobhani SR, Ebrahimi Miandehi E, Pirzadeh P, Alinezhad-Namaghi M, et al. Evaluation of arterial stiffness and its relation to innovative anthropometric indices in persian adults. Int J Hypertens. 2023;2023:1–11.
Fried SK, Lee M-J, Karastergiou K. Shaping fat distribution: new insights into the molecular determinants of depot- and sex-dependent adipose biology: Depot- and sex-dependent adipose Biology. Obesity. 2015;23:1345–52.
Lu Y, Pechlaner R, Cai J, Yuan H, Huang Z, Yang G, et al. Trajectories of age-related arterial stiffness in Chinese men and women. J Am Coll Cardiol. 2020;75:870–80.
Ko S-H, Kim H-S. Menopause-Associated lipid metabolic disorders and foods Beneficial for Postmenopausal Women. Nutrients. 2020;12:202.
Hu W, Zhang H, Liu Z, Duan Q, Liu J, Dong Q, et al. Relationship between adipose tissue distribution and arterial stiffness in HFpEF. Nutrition. 2022;102:111726.
Kim J-M, Chung E, Cho E-S, Lee J-H, Shin S-J, Lee HS, et al. Impact of subcutaneous and visceral fat adiposity in patients with colorectal cancer. Clin Nutr. 2021;40:5631–8.
Chen P, Hou X, Hu G, Wei L, Jiao L, Wang H, et al. Abdominal subcutaneous adipose tissue: a favorable adipose depot for diabetes? Cardiovasc Diabetol. 2018;17:93.
Francisco V, Sanz MJ, Real JT, Marques P, Capuozzo M, Ait Eldjoudi D, et al. Adipokines in non-alcoholic fatty liver disease: are we on the road toward new biomarkers and therapeutic targets? Biology. 2022;11:1237.
Yang J, Li CW, Zhang JR, Qiu H, Guo XL, Wang W. Perirenal Fat Thickness is Associated with Metabolic Dysfunction-Associated fatty liver disease in type 2 diabetes Mellitus. DMSO. 2023;16:1953–65.
Agrawal S, Wang M, Klarqvist MDR, Smith K, Shin J, Dashti H, et al. Inherited basis of visceral, abdominal subcutaneous and gluteofemoral fat depots. Nat Commun. 2022;13:3771.
Ahn D-W, Jeong JB, Kang J, Kim SH, Kim JW, Kim BG, et al. Fatty liver is an independent risk factor for gallbladder polyps. WJG. 2020;26:6979–92.
Omura-Ohata Y, Son C, Makino H, Koezuka R, Tochiya M, Tamanaha T, et al. Efficacy of visceral fat estimation by dual bioelectrical impedance analysis in detecting cardiovascular risk factors in patients with type 2 diabetes. Cardiovasc Diabetol. 2019;18:137.
Gao B, Liu Y, Ding C, Liu S, Chen X, Bian X. Comparison of visceral fat area measured by CT and bioelectrical impedance analysis in Chinese patients with gastric cancer: a cross-sectional study. BMJ Open. 2020;10:e036335.
Lai C-L, Lu H-K, Huang A-C, Chu L-P, Chuang H-Y, Hsieh K-C. Bioimpedance analysis combined with sagittal abdominal diameter for abdominal subcutaneous fat measurement. Front Nutr. 2022;9:952929.
Acknowledgements
We express our gratitude to the entire team of the Department of Endocrinology and the MMC of the Changde Hospital, Xiangya School of Medicine, Central South University, for their invaluable teamwork with this work.
Funding
This study was supported by the Hunan Provincial Key Laboratory of Clinical Epidemiology (2021ZNDXLCL001) and The Science and Technology Innovation Program of Changde City. (No. [2021]67).
Author information
Authors and Affiliations
Contributions
JM, SG, and SG handled the statistical analysis, study design, and manuscript writing. The tasks of QZ, FY, and HZ included recruiting participants, gathering and analyzing data, and following up. The manuscript was read and assessed by HL and QL. The study concept was contributed by ZD who also made significant manuscript edits. Each author accepted the submitted version of the paper and made contributions to it.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Medical Ethics Committee of the Changde Hospital, Xiangya School of Medicine, Central South University (Program number YX-2023-253-01). Every member of the study endorsed an informed consent form. Every procedure used in this investigation complied with the Helsinki Declaration.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Mao, J., Gan, S., Gong, S. et al. Visceral fat area is more strongly associated with arterial stiffness than abdominal subcutaneous fat area in Chinese patients with type 2 diabetes. Diabetol Metab Syndr 16, 123 (2024). https://doi.org/10.1186/s13098-024-01356-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-024-01356-2