
Abstract
Background
Glucose monitoring is vital for glycemic control in patients with diabetes mellitus (DM). Continuous glucose monitoring (CGM) measures whole-day glucose levels. Hemoglobin A1c (HbA1c) is a vital outcome predictor in patients with DM.
Methods
This study investigated the relationship between HbA1c and CGM, which remained unclear hitherto. Data of patients with DM (n = 91) who received CGM and HbA1c testing (1–3 months before and after CGM) were retrospectively analyzed. Diurnal and nocturnal glucose, highest CGM data (10%, 25%, and 50%), mean amplitude of glycemic excursions (MAGE), percent coefficient of variation (%CV), and continuous overlapping net glycemic action were compared with HbA1c values before and after CGM.
Results
The CGM results were significantly correlated with HbA1c values measured 1 (r = 0.69) and 2 (r = 0.39) months after CGM and 1 month (r = 0.35) before CGM. However, glucose levels recorded in CGM did not correlate with the HbA1c values 3 months after and 2–3 months before CGM. MAGE and %CV were strongly correlated with HbA1c values 1 and 2 months after CGM, respectively. Diurnal blood glucose levels were significantly correlated with HbA1c values 1–2 months before and 1 month after CGM. The nocturnal blood glucose levels were significantly correlated with HbA1c values 1–3 months before and 1–2 months after CGM.
Conclusions
CGM can predict HbA1c values within 1 month after CGM in patients with DM.
Similar content being viewed by others

Introduction
Clinical investigations have illustrated the correlation of hemoglobin A1c (HbA1c) values with both microvascular and macrovascular complications in patients with diabetes mellitus (DM) [1, 2]. Strict glycemic treatment plays a crucial role in preventing the development and progression of long-term complications associated with DM. HbA1c values are associated with blood glucose levels over the lifetime of red blood cells (approximately 120 days) and are the current gold standard for clinical monitoring of glycemic control in DM [3, 4]. A study reported a strong correlation between HbA1c values and mean blood glucose levels by using the 7-point blood glucose profiles [5]. Accordingly, HbA1c values were hypothesized to represent relatively long-term glycemic status in patients with DM [6]. The International Diabetes Federation and American Diabetes Association have reported that the HbA1c value < 7.0% is a target for improving DM control [7, 8]. However, intensive treatment of DM is accompanied by hypoglycemia. Severe hypoglycemia may be a critical cause of morbidity. Furthermore, the optimal strategy for monitoring HbA1c values in patients with DM is not well established.
Glucose monitoring is a crucial aspect of DM control. The current accessibility of continuous glucose monitoring (CGM) systems is considered a valuable development in the management of DM. CGM enables the recording of various glucose data, including glucose excursions, patterns, and trends, and timepoints of the associated changes, in an attempt to optimize glycemic control [9, 10]. Recent meta-analyses have revealed that CGM system-based blood glucose monitoring is more effective for glycemic control in patients of type 1 and 2 DM than self-monitoring of blood glucose [11,12,13]. However, approved CGM systems demonstrate suboptimal accuracy [14,15,16]. In this study, we investigated the relationship between CGM system results and HbA1c values and evaluated which time points of HbA1c values were related to CGM as well as CGM parameters correlated with glycemic control in patients with DM.
Materials and methods
Study population
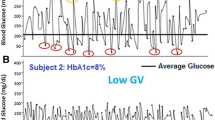
We retrospectively analyzed data of patients with DM who received CGM. CGM was performed using iPro2 (Medtronic, Northridge, CA, USA) for 5 days and 24-h CGM data were extracted from the first or second day of glucose monitoring. In total, 91 patients with DM received CGM, of which 27 (30%) had type 1 DM and 64 (70%) had type 2 DM. The age, body height, and weight, comorbidity, and history of medications of each participant were recorded. HbA1c values were measured using Sebia Capillarys 2 Flex Piercing (Sebia Electrophoresis, France). This capillary electrophoresis-based HbA1c assay had good analytical performances and a high correlation to other high-performing assays [17]. The HbA1c data were collected from 3 months before and 3 months after CGM. Very high (> 400 mg/dL) and very low (< 40 mg/dL) blood glucose levels were recorded through CGM, and patients with anemia were excluded. The blood glucose levels recorded from 0600 to 2200 represented diurnal blood glucose, and those from 2200 to 0600 represented nocturnal blood glucose levels. The whole-day, diurnal, and nocturnal glucose levels during CGM were calculated based on the average of the highest 10% (CGMH10%), 25% (CGMH25%), and 50% (CGMH50%) or all data (CGM100%). The mean amplitude of glycemic excursions (MAGE), classical standard deviation (SD), continuous overlapping net glycemic action (CONGA), and calculated coefficient of variation (CV) were calculated using Glycemic Variability Analyzer Program 1.1 (MATLAB 2010b; MathWorks, USA).
Statistical analysis
Continuous variables are expressed as mean ± SD and were compared using the Student t-test. Categorical variables were reported as frequencies and compared using the χ2 or Fisher exact test if at least one cell had an expected cell count of < 5. A two-tailed P < 0.05 was considered statistically significant. A linear correlation was used to correlate the measured parameters. All statistical analyses were performed on SigmaPlot (version 12.3). The correlations among the HbA1c at different time points and were compared using the cocor package (https://comparingcorrelations.org/) [18].
Results
Of the 91 patients with DM who received CGM, 9 patients with markedly elevated or very low blood glucose levels were excluded; of the remaining patients, 23 and 59 were diagnosed as having type 1 and 2 DM, respectively (Table 1). Patients with type 1 DM were younger and taller than patients with type 2 DM. The duration of DM was 15.3 ± 8.8 years. The mean C-peptide level among the 23 patients with type 1 DM was 0.2 ± 0.14 ng/mL. However, only 27 patients with type 2 DM have C-peptide data, and the mean level was 2.39 ± 2.08 ng/mL. Among these 82 DM patients, 23 had diabetic retinopathy, 22 had diabetic nephropathy, and 30 had diabetic neuropathy. Of these 82 patients, 67 patients adjusted their treatment during the study period. Forty patients increased the dosage of insulin, 17 decreased the dosage of insulin, 6 increased non-insulin anti-diabetic drugs, and 4 decreased non-insulin anti-diabetic drugs. Among the 82 DM patients enrolled in our study, 74 patients have checked HbA1c levels more than twice, and these HbA1c levels were evaluated in correlation with the CGM at different time points. Table 2 illustrates that the blood glucose levels (CGM100%) measured through CGM were significantly correlated with HbA1c values measured 1 (r = 0.69) and 2 (r = 0.39) months after CGM and 1–3 months (r = 0.35) before CGM. The HbA1c values 1 month after CGM was significantly correlated with the highest 10% (CGMH10%, r = 0.72), 25% (CGMH25%, r = 0.74), and 50% (CGMH50%, r = 0.73) measured from CGM. The CGMH50% of blood glucose levels was significant with HbA1c values 3 months before and 1 month after CGM, but not with HbA1c values 1–2 months before and 2–3 months after CGM. However, the CGMH10% and CGMH25% of blood glucose levels during CGM did not correspond to HbA1c values measured 13 months before and 2–3 months after CGM. The diurnal blood glucose levels were significantly correlated with HbA1c values 1 and 2 months before and 1 month after CGM. The nocturnal blood glucose levels were significantly correlated with HbA1c values 1–3 months before and 1–2 months after CGM.
Table 3 illustrates that the blood glucose levels (CGM100%) measured through CGM were significantly correlated with HbA1c values measured 1 (r = 0.71) and 2 (r = 0.44) months after CGM and 1 month (r = 0.35) before CGM in the treatment-adjusted group. The HbA1c values 1 month after CGM was significantly correlated with the highest 10% (CGMH10%, r = 0.70), 25% (CGMH25%, r = 0.73), and 50% (CGMH50%, r = 0.73) measured from CGM. The diurnal blood glucose levels were significantly correlated with HbA1c values 1 month before and 1 month after CGM. The nocturnal blood glucose levels were significantly correlated with HbA1c values 1–3 months before and 1–2 months after CGM.
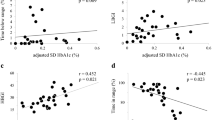
Table 4 displays the glycemic variation of patients with type 1 and 2 DM over 3 months before and 3 months after CGM. The mean, SD, MAGE, CONGA, and CV values were calculated for each patient. Table 5 displays the relationship between HbA1c and glycemic variation, including SD, percent CV (%CV), MAGE, and CONGA. Overall, the SD and MAGE were significantly correlated to HbA1c values in the next 1 month, and the %CV was significantly correlated to HbA1c values 2 months after CGM. The %CV was significantly correlated with the HbA1c values 2 months after CGM in patients with type 1 DM. In patients with type 2 DM, the SD and MAGE were significantly correlated to HbA1c values 1 month after CGM and the %CV was significantly correlated with HbA1c values 2 months after CGM.
Discussion
The goal of DM treatment is to prevent chronic complications [19, 20]. Glucose monitoring is crucial in DM control. HbA1c assay is recommended as the optimal approach to monitoring DM glycemic control [21] and is used globally as the basis of adjustment in treatment guidelines [22,23,24]. A study reported a strong correlation between HbA1c values and mean blood glucose levels using 7-point blood glucose profiles [5]. However, the optimal strategy for monitoring HbA1c values was not clear because the relationship between DM control and HbA1c values in intensive glucose monitoring is not well established. CGM could provide more blood glucose data and contribute to the improvement in DM management, as demonstrated by the significant lowering of HbA1c values in patients with DM [25,26,27,28]. However, studies have noted strong correlations between CGM interstitial glucose and venous plasma or capillary glucose levels [29,30,31]. Studies have reported a less than the acceptable correlation between CGM interstitial glucose results and venous plasma or capillary glucose levels [32, 33]. In this study, we determined that CGM may correlate well with HbA1c values over 3 months before and 3 months after CGM. The CGM was most closely related to HbA1c values in the next month after CGM when measured based on the interstitial glucose levels every 5 min for 5 days. This phenomenon was also observed with patients who have an adjustment of treatment, which means that CGM quickly corresponds to the adjustment of treatment, and seems to be closely associated with the HbA1c values one month after CGM.
Sharp and Rainbow have demonstrated that CGM was strongly correlated with HbA1c values at the time of insertion [34]. Saladri et al. also identified a correlation between the area under the glucose curve of CGM and HbA1c values in patients with type 1 DM [35]. Furthermore, Nathan et al. extensively analyzed CGM and identified a strong correlation between the mean glucose measured by CGM and HbA1c values [31]. Glucose variability may be a factor in DM complications [36]. An acute increase in blood glucose can produce significant alterations in normal homeostasis, leading to endothelial dysfunction and inflammation, among other effects [37]. A study indicated that MAGE was not correlated to HbA1c values [38]. In this study, we determined that MAGE was poorly associated with HbA1c values at several time points but was significantly correlated with the HbA1c values 1 month after CGM, particularly in patients with type 2 DM. Furthermore, CGM is vital in improving glucose variability to achieve strict glycemic control.
Several factors may alter the relationship between the mean blood glucose levels and HbA1c values. For instance, variable red cell turnover may be affected by hyperglycemia [39]. Moreover, glycation rates may differ among individuals at the same mean blood glucose levels [40]. Notably, the negative correlation between measured mean glucose levels and HbA1c values 3 months after CGM may also suggest an improvement in the mean glucose levels after the intervention based on the CGM results.
In conclusion, the association of CGM results with HbA1c values 1 month after monitoring was positive. Furthermore, CGM could record glucose variability and is a reliable tool to assess glycemic state and improve DM management.
Limitations
The limitations of this study should be considered. First, the r value in our study is relatively low compared with previous studies [18, 41]. This difference may be due to the small sample in each group in this single-center study. Second, HbA1c reflects the average blood glucose of 3 months, and the collected dynamic blood glucose data is the blood glucose data of a certain day. A larger sample size will be needed to further explore the relationship between the two. Third, the CGM data were retrospectively collected from the medical history, and HbA1c data were not integrated.
Availability of data and materials
The data used to support the findings of this study are available from the corresponding authors upon request.
References
Diabetes Control and Complications Trial Research Group, Nathan DM, Genuth S, Lachin J, Cleary P, Crofford O, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86.
Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321:405–12.
Nathan DM, Singer DE, Hurxthal K, Goodson JD. The clinical information value of the glycosylated hemoglobin assay. N Engl J Med. 1984;310:341–6.
Tahara Y, Shima K. The response of GHb to stepwise plasma glucose change over time in diabetic patients. Diabetes Care. 1993;16:1313–4.
Rohlfing CL, Wiedmeyer HM, Little RR, England JD, Tennill A, Goldstein DE. Defining the relationship between plasma glucose and HbA1c. Diabetes Care. 2002;25:275–8.
Koenig RJ, Peterson CM, Jones RL, Saudek C, Lehrman M, Cerami A. Correlation of glucose regulation and hemoglobin AIc in diabetes mellitus. N Engl J Med. 1976;295:417–20.
International Diabetes Federation Guideline Development Group. Global guideline for type 2 diabetes. Diabetes Res Clin Pract. 2014;104:1–52.
American Diabetes Association. 6. Glycemic targets. Diabetes Care. 2017;40:S48–56.
Buckingham B. Clinical overview of continuous glucose monitoring. J Diabetes Sci Technol. 2008;2:300–6.
Blevins TC. Professional continuous glucose monitoring in clinical practice 2010. J Diabetes Sci Technol. 2010;4:440–56.
Poolsup N, Suksomboon N, Kyaw AM. Systematic review and meta-analysis of the effectiveness of continuous glucose monitoring(CGM) on glucose control in diabetes. Diabetol Metab Syndr. 2013;5:39.
Szypowska A, Ramotowska A, Dzygalo K, Golicki D. Beneficial effect of real-time continuous glucose monitoring system on glycemic control in type 1 diabetic patients: systematic review and meta-analysis of randomized trials. Eur J Endocrinol. 2012;166:567–74.
Chetty VT, Almulla A, Odueyungbo A, Thabane L. The effect of continuous subcutaneous glucose monitoring (CGMS) versus intermittent whole blood finger-stick glucose monitoring (SBGM) on hemoglobin A1c (HBA1c) levels in Type I diabetic patients: a systematic review. Diabetes Res Clin Pract. 2008;81:79–87.
Jacobs B, Phan K, Bertheau L, Dogbey G, Schwartz F, Shubrook J. Continuous glucose monitoring system in a rural intensive care unit: a pilot study evaluating accuracy and acceptance. J Diabetes Sci Technol. 2010;4:636–44.
McGarraugh GV, Clarke WL, Kovatchev BP. Comparison of the clinical information provided by the FreeStyle Navigator continuous interstitial glucose monitor versus traditional blood glucose readings. Diabetes Technol Ther. 2010;12:365–71.
Mazze RS, Strock E, Borgman S, Wesley D, Stout P, Racchini J. Evaluating the accuracy, reliability, and clinical applicability of continuous glucose monitoring (CGM): is CGM ready for real time? Diabetes Technol Ther. 2009;11:11–8.
Jaisson S, Leroy N, Meurice J, Guillard E, Gillery P. First evaluation of Capillarys 2 Flex Piercing® (Sebia) as a new analyzer for HbA1c assay by capillary electrophoresis. Clin Chem Lab Med. 2012;50(10):1769–75.
Hu Y, Shen Y, Yan R, Li F, Ding B, Wang H, et al. Relationship between estimated glycosylated hemoglobin using flash glucose monitoring and actual measured glycosylated hemoglobin in a Chinese population. Diabetes Ther. 2020;11:2019–27.
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837–53.
DCCT Study Group. The Effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86.
WHO Guidelines Approved by the Guidelines Review Committee. Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus: abbreviated report of a WHO consultation. Geneva: World Health Organization; 2011.
American Diabetes Association. Standards of medical care in diabetes–2007. Diabetes Care. 2007;30(Suppl 1):S4–41.
European Diabetes Policy Group. A desktop guide to Type 2 diabetes mellitus. Diabet Med. 1999;16:716–30.
Nathan DM, Buse JB, Davidson MB, Heine RJ, Holman RR, Sherwin R, et al. A consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia. 2006;49:1711–21.
Bailey TS, Zisser HC, Garg SK. Reduction in hemoglobin A1c with real-time continuous glucose monitoring: results from a 12-week observational study. Diabetes Technol Ther. 2007;9:203–10.
Danne T, de Valk HW, Kracht T, Walte K, Geldmacher R, Sölter L, et al. Reducing glycaemic variability in type 1 diabetes self-management with a continuous glucose monitoring system based on wired enzyme technology. Diabetologia. 2009;52:1496–503.
Deiss D, Bolinder J, Riveline JP, Battelino T, Bosi E, Tubiana-Rufi N, et al. Improved glycemic control in poorly controlled patients with type 1 diabetes using real-time continuous glucose monitoring. Diabetes Care. 2006;29:2730–2.
Carlson AL, Mullen DM, Bergenstal RM. Clinical use of continuous glucose monitoring in adults with type 2 diabetes. Diabetes Technol Ther. 2017;19(S2):S4–11.
Djakouré-Platonoff C, Radermercker R, Reach G, Slama G, Selam JI. Accuracy of continuous glucose monitoring system in inpatient and outpatient conditions. Diabetes Metab. 2003;29(2 Pt 1):159–62.
Clarke WL, Anderson S, Farhy L, Breton M, Gonder-Frederick L, Cox D, et al. Evaluating the clinical accuracy of two continuous glucose sensors using continuous glucose-error grid analysis. Diabetes Care. 2005;28:2412–7.
Nathan DM, Turgeon H, Regan S. Relationship between glycated haemoglobin levels and mean glucose levels over time. Diabetologia. 2007;50:2239–44.
Baek YH, Jin HY, Lee KA, Kang SM, Kim WJ, Kim MG, et al. The correlation and accuracy of glucose levels between interstitial fluid and venous plasma by continuous glucose monitoring system. Korean Diabetes J. 2010;34:350–8.
Scuffi C. Interstitium versus blood equilibrium in glucose concentration and its impact on subcutaneous continuous glucose monitoring systems. Eur Endocrinol. 2014;10:36–42.
Sharp P, Rainbow S. Continuous glucose monitoring and haemoglobin A(1c). Ann Clin Biochem. 2002;39:516–7.
Salardi S, Zucchini S, Santoni R, Ragni L, Gualandi S, Cicognani A, et al. The glucose area under the profiles obtained with continuous glucose monitoring system relationships with HbA(lc) in pediatric type 1 diabetic patients. Diabetes Care. 2002;25:1840–4.
Ceriello A, Ihnat MA. “Glycaemic variability”: a new therapeutic challenge in diabetes and the critical care setting. Diabet Med. 2010;27:862–7.
Ceriello A. Postprandial hyperglycemia and diabetes complications: is it time to treat? Diabetes. 2005;54:1–7.
Hajime M, Okada Y, Mori H, Otsuka T, Kawaguchi M, Miyazaki M, et al. Twenty-four-hour variations in blood glucose level in Japanese type 2 diabetes patients based on continuous glucose monitoring. J Diabetes Investig. 2018;9:75–82.
Virtue MA, Furne JK, Nuttall FQ, Levitt MD. Relationship between GHb concentration and erythrocyte survival determined from breath carbon monoxide concentration. Diabetes Care. 2004;27:931–5.
Gould BJ, Davie SJ, Yudkin JS. Investigation of the mechanism underlying the variability of glycated haemoglobin in non-diabetic subjects not related to glycaemia. Clin Chim Acta. 1997;260:49–64.
Nathan DM, Kuenen J, Borg R, Zheng H, Schoenfeld D, Heine RJ, et al. Translating the A1C assay into estimated average glucose values. Diabetes Care. 2008;31:1473–8.
Acknowledgements
This study was financed by the Ministry of Science and Technology (MOST 107-2314-B-038-097-MY2, MOST 107-2314-B-038 -099 -MY3, MOST108-2314-B-038-042 and MOST109-2314-B038-098), Taipei Medical University (TMU109-AE1-B26) and from Taipei Medical University-Wan Fang Hospital (105swf02, 106-eva-06, and 107-wf-eva-13).
Funding
The present work was supported by Grants from the Ministry of Science and Technology (MOST 107-2314-B-038-097-MY2, MOST 107-2314-B-038-099-MY3, MOST108-2314-B-038-042 and MOST109-2314-B038-098), Taipei Medical University (TMU109-AE1-B26) and Taipei Medical University-Wan Fang Hospital (105swf02, 106-eva-06, and 107-wf-eva-13).
Author information
Authors and Affiliations
Contributions
Conception or design: TIL, YJC. Acquisition, analysis, or interpretation of data: JHH, YKL, TWL, HWL. Drafting the work or revising: JHH, YKL, TWL, HWL, YMC, YCH. Final approval of the manuscript: JHH, YKL, TWL, HWL, YMC, YCH, TIL, YJC. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This retrospective study was approved by the Taipei Medical University-Joint Institutional Review Board (TMU-JIRB; approval number: N202001006). The requirement for obtaining informed consent was waived by the TMU-JIRB due to the retrospective nature of the investigation.
Consent for publication
Not applicable.
Competing interests
This paper does not have a conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huang, JH., Lin, YK., Lee, TW. et al. Correlation between short- and mid-term hemoglobin A1c and glycemic control determined by continuous glucose monitoring. Diabetol Metab Syndr 13, 94 (2021). https://doi.org/10.1186/s13098-021-00714-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-021-00714-8