
Abstract
Background
During control mechanical ventilation (CMV), the driving pressure of the respiratory system (ΔPrs) serves as a surrogate of transpulmonary driving pressure (ΔPlung). Expiratory muscle activity that decreases end-expiratory lung volume may impair the validity of ΔPrs to reflect ΔPlung. This prospective observational study in patients with acute respiratory distress syndrome (ARDS) ventilated with proportional assist ventilation (PAV+), aimed to investigate: (1) the prevalence of elevated ΔPlung, (2) the ΔPrs-ΔPlung relationship, and (3) whether dynamic transpulmonary pressure (Plungsw) and effort indices (transdiaphragmatic and respiratory muscle pressure swings) remain within safe limits.
Methods
Thirty-one patients instrumented with esophageal and gastric catheters (n = 22) were switched from CMV to PAV+ and respiratory variables were recorded, over a maximum of 24 h. To decrease the contribution of random breaths with irregular characteristics, a 7-breath moving average technique was applied. In each patient, measurements were also analyzed per deciles of increasing lung elastance (Elung). Patients were divided into Group A, if end-inspiratory transpulmonary pressure (PLEI) increased as Elung increased, and Group B, which showed a decrease or no change in PLEI with Elung increase.
Results
In 44,836 occluded breaths, ΔPlung ≥ 12 cmH2O was infrequently observed [0.0% (0.0–16.9%) of measurements]. End-expiratory lung volume decrease, due to active expiration, was associated with underestimation of ΔPlung by ΔPrs, as suggested by a negative linear relationship between transpulmonary pressure at end-expiration (PLEE) and ΔPlung/ΔPrs. Group A included 17 and Group B 14 patients. As Elung increased, ΔPlung increased mainly due to PLEI increase in Group A, and PLEE decrease in Group B. Although ΔPrs had an area receiver operating characteristic curve (AUC) of 0.87 (95% confidence intervals 0.82–0.92, P < 0.001) for ΔPlung ≥ 12 cmH2O, this was due exclusively to Group A [0.91 (0.86–0.95), P < 0.001]. In Group B, ΔPrs showed no predictive capacity for detecting ΔPlung ≥ 12 cmH2O [0.65 (0.52–0.78), P > 0.05]. Most of the time Plungsw and effort indices remained within safe range.
Conclusion
In patients with ARDS ventilated with PAV+, injurious tidal lung stress and effort were infrequent. In the presence of expiratory muscle activity, ΔPrs underestimated ΔPlung. This phenomenon limits the usefulness of ΔPrs as a surrogate of tidal lung stress, regardless of the mode of support.
Similar content being viewed by others


Introduction
Transpulmonary driving pressure (ΔPlung) represents a direct measurement of static tidal lung stress and is proportional to lung strain, key mediators of ventilator-induced lung injury [1,2,3,4]. Despite its importance during mechanical ventilation, its clinical use remains limited due to the need for esophageal catheter insertion [5]. For this reason, during passive mechanical ventilation, the driving pressure of the respiratory system (ΔPrs), which is calculated as the difference between end-inspiratory plateau pressure (Pplat) and total positive end-expiratory pressure (PEEP), is used as a surrogate for ΔPlung. Indeed, ΔPrs can reliably predict increased ΔPlung, with high ΔPrs (≥ 15 cmH2O) being associated with elevated morbidity and mortality [2, 6,7,8].
In mechanically ventilated patients with active breathing, measurement of ΔPrs is challenging for two reasons. Firstly, Pplat calculation requires end-inspiratory occlusions during which respiratory muscle activity should be absent, which is often not the case during conventional assisted ventilation [9]. Proportional assist ventilation with load adjustable gain factors (PAV+), automatically performs end-inspiratory occlusions to measure Pplat. The interference of respiratory muscle activity with Pplat calculation is largely minimized with this mode, because the end of mechanical inflation follows the end of neural inspiration [10]. Secondly, expiratory muscle activity is often observed in critically ill patients, potentially lowering end-expiratory lung volume below the level corresponding to PEEP [11,12,13]. As a result, the relaxation of expiratory muscles contributes to tidal volume (VT) [14,15,16]. This is a reflex protective mechanism, which at increased demands, increases VT at the same end-inspiratory lung stress [14, 16]. Under these conditions ΔPrs, which assumes that the starting point of inflation is PEEP, does not account for the decrease in end-expiratory lung volume below the level corresponding to PEEP, leading to an underestimation of ΔPlung (Fig. 1 and Additional file 1: Fig. S1). Unfortunately, this later issue is largely ignored in the literature.

Effect of decreasing end-expiratory lung volume below (VEE<FRC) that corresponding to PEEP (VEE,PEEP) on calculation of driving pressure of respiratory system (ΔPrs) and lung (ΔPlung). Lung (Elung) and chest wall (Ecw) elastance were kept constant at all lung volumes. Blue and white circles denote lung and chest wall, respectively. Set values are shown using italics. The numbers between the circles represent pleural pressure (Ppl). Arrows show the magnitude of PEEP, end-inspiratory plateau pressure (Pplat), elastic recoil pressure of chest wall (Pcw) and lung (Plung), and expiratory muscle pressure (Pmusexp). Panel A shows applied pressures (cmH2O) when expiration is passive. Tidal volume (VT) is set to 500ml, Ppl at end-expiration to 4 cmH2O and Pplat to 22 cmH2O. ΔPrs = Pplat-PEEP = 12 cmH2O and respiratory system elastance (Ers) = ΔPrs/VT = 12/0.5 = 24 cmH2O/l. Ecw is set to 20% of Ers (4.8 cmH2O/l). At end-expiration, alveolar pressure (Palv) = PEEP, Pcw = Ppl = 4 cmH2O and Plung = Palv-Ppl = 6 cmH2O. Notice that Palv = Plung + Pcw. At end-inspiration Ppl increases to 6.4 cmH2O (4 + Ecw × VT = 4 + 2.4 = 6.4), Pcw = 6.4 cmH2O and Plung = Palv-Ppl = 22–6.4 = 15.6 cmH2O. ΔPlung = 15.6–6 = 9.6 cmH2O and Elung = ΔPlung/VT = 9.6/0.5 = 19.2 cmH2O/l. Panel B shows pressures when expiration is active. Because of expiratory muscle activity, VEE<FRC is set to 260 ml and therefore, compared to passive expiration, Pcw decreases by 1.2 cmH2O (Ecw × 0.26). At end-expiration, Pmusexp is set to 6.2 cmH2O and Ppl is 9 cmH2O (Ppl = Pcw + Pmusexp). Plung = Palv-Ppl = 10–9 = 1 cmH2O. Transdiaphragmatic pressure (Pdi) is deemed similar to A and begins to rise when flow is expiratory, before the full relaxation of expiratory muscles. Assuming that Pdi increases volume above VEE,PEEP by 300ml (only a portion of Pdi increases volume above VEE,PEEP), VT is 560 ml. At end-inspiration, Pplat = PEEP plus the increase in elastic recoil pressure of respiratory system due to 300 ml increase in volume above VEE,PEEP (Pplat = PEEP + 0.3 × 24 = 17.2 cmH2O). ΔPrs = Pplat-PEEP = 7.2 cmH2O and calculated Ers = 7.2/0.56 = 12.9 cmH2O/l, underestimated by 46%, because ΔPrs should be divided by 0.3 (the volume inflated above PEEP). Pcw is 5.44 cmH2O, 1.44 cmH2O higher than that at VEE,PEEP (0.3 × 4.8 = 1.44). Plung = Palv-Ppl = 17.2–5.44 = 11.76 cmH2O, ΔPlung = 11.76–1 = 10.76 cmH2O and Elung = ΔPlung/VT = 19.2 cmH2O/l, similar to that in A. See Fig. S1 in the Additional file 1 for detailed further explanation
Studies have shown that, in critically ill patients ventilated with PAV+, which via the control of breathing mechanisms permits the patients to determine VT [10], ΔPrs can be effectively maintained low [15, 17]. However, these studies did not measure ΔPlung. It is unknown whether ΔPrs reliably predicts tidal static lung stress in patients with active expiration that lowers end-expiratory lung volume below that corresponding to PEEP. The primary aim of this study was to determine the occurrence of injurious tidal lung stress, as expressed by a high ΔPlung (≥ 12 cmH2O) [18] in patients with acute respiratory distress syndrome (ARDS) ventilated with PAV+, and to elucidate the relationship between ΔPrs and ΔPlung. We hypothesize that in a given patient, the decrease in end-expiratory lung volume, secondary to expiratory muscle contraction because of increased demands, can lead to underestimation of ΔPlung by ΔPrs to an unknown extent. A secondary objective was to explore if dynamic transpulmonary pressure swings (Plungsw) and indices of respiratory effort, reflected by transdiaphragmatic (ΔPdi) and respiratory muscles pressure (Pmussw) swings, remain within a safe range. It was deemed safe to have values for Plungsw, ΔPdi, and Pmussw of less than 20, 3–12, and 3–15 cmH2O, respectively [19,20,21,22].
Methods
This prospective observational study was conducted in the medical–surgical intensive care unit (ICU) of the University Hospital of Heraklion. The study was approved by the Hospital Ethics Committee (339/09/20-03-2019), and since there was no interference with patients’ management, signed informed consent was waived.
Patients
Eligible for inclusion were intubated patients, admitted to the ICU for management of ARDS, and instrumented with esophageal and gastric catheters (NutriVent™) or only an esophageal catheter (Cooper-Surgical esophageal balloon kit) for clinical purposes. The patients were included at any time the treating physician switched them from control modes to PAV+ (Puritan-Bennett 840 ventilator, Medtronic, Boulder, CO) and estimated that they would remain on assisted mechanical ventilation for at least 24 h. The recording period was approximately 24 h, unless the patient was switched to other modes, placed on a T-piece earlier, or the recording was interrupted for procedural reasons. Patients who remained on PAV+ for less than 1 h were excluded from the analysis.
Measurements: analysis
Airflow (V′), volume and airway (Paw), esophageal (Pes), gastric (Pgas), dynamic transpulmonary (Plung = Paw-Pes), and transdiaphragmatic (Pdi = Pgas-Pes) pressures were monitored continuously. Using a customized computer program, all breaths with 300-ms end-inspiratory occlusions were identified and the beginning (zero flow) and end of inspiration (end of 300-ms occlusion) were marked. At these two points, Paw and Pes were measured and various respiratory variables, including static transpulmonary pressures and Pmussw, were calculated using standard formulas [18, 23, 24]. Plungsw and Pmussw during the breath were measured as the difference between the peak and nadir values. Expiratory muscle activity was estimated in the preceding breath by measuring the rise in Pgas (ΔPgas) during the expiratory phase [25, 26]. Each recording underwent a thorough examination to identify artifacts mainly due to esophageal peristalsis and issues related to improper balloon filling and position.
Significant expiratory muscle activity during expiration was determined by either an average ΔPgas > 1 cmH2O over the recording time or, in patients without gastric catheters, by a thorough examination of expiratory flow and Pes waveforms, which unequivocally demonstrated signs of active expiration [27]. Dynamic intrinsic PEEP (PEEPi) was calculated only in patients in whom both Pes and Pgas were available, as described previously [28].
In order to decrease the contribution of random breaths with irregular characteristics on the measured values, a seven-breath moving average (7-brMA) technique was performed and the results of this analysis are reported. Furthermore, in each patient all the artifact-free 7-brMA measurements were divided into deciles based on progressive increase in lung elastance (Elung) (Decile 1: the lowest range of Elung, Decile 10; the highest range of Elung, see Additional file 2 for reasoning of choosing Elung to characterize deciles of 7-brMA measurements). Patients were divided into two groups (A and B), depending on how their end-inspiratory transpulmonary pressure (PLEI) responded to an increase in Elung, with the assumption that expiratory muscle contraction could, as a reflex protective mechanism, prevent increases in PLEI. Group A was characterized by an increase in end-inspiratory lung stress, as measured by the PLEI, with increasing Elung, whereas patients in Group B showed a decrease or no change in PLEI.
Statistical analysis
Values are presented as median (interquartile range) or counts (percentage) unless otherwise stated. Normal distribution was checked by the Shapiro–Wilk test and comparisons within and between patients were performed by nonparametric or parametric tests, as appropriate. The diagnostic accuracy of ΔPrs in detecting ΔPlung ≥ 12 cmH2O was evaluated using the receiver operating characteristic (ROC) method [29, 30]. The effect of Elung deciles on end-expiratory transpulmonary pressure (PLEE) and ΔPgas was analyzed using a linear mixed-effect model. A similar analysis was performed to examine the effect of ΔPgas on PLEE, as well as that of PLEE on ΔPlung/ΔPrs. Regression analysis with curve estimation was performed on average values per decile between Elung and PLEE, Elung and ΔPgas, PLEE and ΔPlung/ΔPrs, and ΔPgas and PLEE and the coefficient of determination (r2) was calculated. Patients were classified into Group A if, within each patient, there was a significant linear increase in PLEI with increasing Elung. Binary logistic analysis was performed to examine if patients’ characteristics and outcomes can predict the pattern of response to changes in Elung. P < 0.05 was the statistically significant threshold. Statistical analysis was performed by using SPSS 26 software.
Results
We obtained demographic, clinical, and ventilation data from 31 patients (22 instrumented with both esophageal and gastric balloons) during a 30-month period (Table 1). Data collected during 468 h of ventilation with PAV+ were examined and a total of 44,836 artifact-free occluded breaths were analyzed.
The results of 7-brMA analysis and analysis of all occluded breaths were similar, except at high values of ΔPlung where 7-brMA analysis eliminated the sporadic high values (Additional file 2: Figs. S2, S3). Details of recorded parameters on the day of the study and the variation of ΔPlung and other respiratory variables during the recording period are shown in Additional file 2: Tables S1 and S2.
Primary outcomes
Occurrence of injurious lung stress
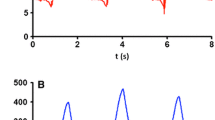
The median number of 7-brMA measurements and the percentage of these measurements where ΔPlung aligns within the range of each cmH2O, from ≤ 5 cmH2O to the maximum value is illustrated in Fig. 2. ΔPlung values ≥ 12 cmH2O were observed in 15 out of 31 patients (Additional file 3: Individual data). One patient had constantly ΔPlung ≥ 12 cmH2O, while in the remaining 14 patients, ΔPlung above and below this threshold were noted. The median (IQR) percentage of measurements with ΔPrs < 15 cmH2O and ΔPlung < 12 cmH2O is presented in Table 2.

Number of 7-breath moving average measurements (A) and % of total measurements (B) with ΔPlung within the range of each cmH2O from ≤ 5 cmH2O to maximum values. Outliers are shown by circles
The number and percentage of 7-brMA measurements where ΔPrs aligns within the range of each cmH2O, from ≤ 5 cmH2O to the maximum value is illustrated in Additional file 2: Figure S4.
Relationship between ΔP rs and ΔP lung
Twenty-one patients exhibited significant expiratory muscle activity (16 had average ΔPgas > 1 cmH2O and 5 exhibited signs of active expiration in V′ and Pes waveforms). In several of them, expiratory muscle relaxation contributed to a portion of the VT measured (Fig. 3). This led to an underestimation of ΔPlung by ΔPrs. Most patients (24/31, 77.4%) had readings of ΔPlung that exceeded ΔPrs due to this underestimation. The median number of such measurements was 332 (13–490), accounting for 31.7% (2.2–94.5%) of the total measurements. In two patients, ΔPlung always exceeded ΔPrs.

Flow and airway, esophageal, gastric, and transdiaphragmatic pressures in a patient with ARDS ventilated on PAV+ . An occluded and two, preceding and following, un-occluded breaths are shown. Notice that in all breaths inspiratory flow initially is generated only be relaxation of expiratory muscles (red areas). Thereafter, the diaphragm contracts, while expiratory muscles continue to relax (yellow areas). At the beginning of inflation of the occluded breath (zero flow) PLEE is −3.44 cmH2O and at the end of occlusion (end of blue area) PLEI is 6.48 cmH2O. The calculated ΔPlung is 9.92 cmH2O. The corresponding values of Paw are 9.62 and 13.64 cmH2O and ΔPrs is 4.02 cmH2O. Totally passive inspired volumes (integrated flow-time red area) in these three breaths are 76, 28 and 85 ml, respectively. The end of relaxation of expiratory muscles occurred when inspired volumes (sum of red and yellow areas) were 265 ml (1st breath), 247 ml (2nd breath), and 268 ml (3rd breath). Notice that before the occluded breath gastric pressure increased by 6.4 cmH2O (blue double edge arrow), indicating significant expiratory muscle activity that is able to decrease expiratory volume below that determined by PEEP. Notice also that the drop in Pgas due to expiratory muscle relaxation was 7.0 cmH2O. Observe also that at the end of occlusion Pdi returned to baseline and during occlusion the change in Pgas was negligible (0.3 cmH2O), indicating passive condition during measurements of Pplat. Tidal volume of occluded breath was 562 ml and calculated elastance of respiratory system was 7.2 cmH2O/l, while that of the lung 17.8 cmH2O. ΔPlung/ΔPrs (and Elung/Ers) was 2.5
A total of 310 deciles with progressive increases in Elung were analyzed (10 deciles per patient). When Elung increased, ΔPlung increased in all patients (Additional file 2: Table S3). There was a highly significant relationship of quadratic function (y = a + b1x + b2x2) between per decile average values of Elung and PLEE and a negative linear relationship of PLEE and ΔPlung/ΔPrs (Fig. 4). The decrease in PLEE with increasing Elung was due to expiratory muscle contraction, as reflected by a quadratic function relationship between Elung and ΔPgas (Additional File 2: Fig. S5).

Relationship between lung elastance (Elung) and transpulmonary pressure at the end of expiration (PLEE) (Left) and PLEE and ratio of driving transpulmonary pressure to that of respiratory system (ΔPlung /ΔPrs) (Right). Each circle represents the average values of these variables in each of the 10 segments characterized by increasing Elung. Blue circles: Deciles 1–3 (low Elung). Yellow circles: Deciles 4–7 (moderate Elung). Red circles: Deciles 8–10 (high Elung). Notice that the highest Elung (Decile 10) is associated with the lowest PLEE and the highest ΔPlung/ΔPrs. Observe also that at highest Elung (Decile 10) average ΔPlung is greater than ΔPrs. The number in each circle indicates the corresponding decile. Notice that PLEE begins to decrease after decile 6. This is reflected in almost constant ΔPlung/ΔPrs from decile 1 to 6
Response to increasing Elung by patient Group
Seventeen out of thirty-one patients were included in Group A and the remaining 14 were in Group B. Although with increasing Elung, ΔPlung increased similarly between groups, in Group A this increase was mainly due to a PLEI increase, while in Group B to a PLEE decrease. With increasing Elung, contrary to Group A, Group B was characterized by constant ΔPrs and Pplat, a significant decrease in PLEE, and an increase in ΔPgas (Fig. 5). The response of other variables is shown in Additional file 2: Table S4. Similar results were observed when only patients with gastric pressure measurements (n = 22) were analyzed (Additional file 2: Fig. S6). The linear mixed-effects model analysis, with PLEE as the dependent variable, Elung deciles and group category as fixed effects, and each subject as a random effect, demonstrated a significant effect (P < 0.001) of Elung on PLEE. There was no effect of group category on PLEE. Similarly, a significant effect of ΔPgas on PLEE was also observed. When ΔPlung/ΔPrs was used as the dependent variable, there was a significant effect (P < 0.001) of PLEE, as a fixed variable, but there was no significant effect of group category. Binary logistic regression showed that none of the patients’ characteristics, including age and body mass index, length of ICU stay, days on mechanical ventilation, and ICU outcome, predicted the Group classification.

Effects of a progressive increase in Elung (Decile 1: the lowest Elung; Decile 10 the highest Elung) on average respiratory variables in Group A (blue squares connected by blue lines, characterized by a linear increase in PLEI with increasing Elung) and Group B (orange squares connected by orange lines, characterized by no increase in PLEI with increasing Elung). Blue and orange dashed lines indicate standard deviation range in Groups A and B, respectively. Notice the significant interaction between groups in transpulmonary pressure at end-inspiration (PLEI) and end-expiration (PLEE), driving pressure (ΔPrs), end-inspiratory plateau pressure (Pplat), and gastric pressure increase during expiration (ΔPgas). ‡Significant interaction between Groups (Split-plot ANOVA). *Significant difference from the corresponding value of Group A. ¶Pertains to 22 patients (11 in each group)
Accuracy of ΔP rs to predict injurious ΔP lung
ROC curve analysis revealed that, although ΔPrs had high accuracy for detecting ΔPlung ≥ 12 cmH2O in the overall population, this effect was due to patients of Group A. In Group B, ΔPrs showed no predictive capacity for detecting injurious ΔPlung (Fig. 6).

Receiver operating characteristics curves (blue lines). Area under the curve (AUC) of driving pressure of respiratory system (ΔPrs) to predict transpulmonary driving pressure (ΔPlung) ≥ 12 cmH2O in all patients (A, 310 segments) and patients of Group A (B, 170 segments) and Group B (C, 140 segments). Notice that contrary to patients of Group A, in patients of Group B ΔPrs does not have a significant predictive value for ΔPlung ≥ 12 cmH2O. Values of AUC are with 95% confidence intervals, and P values pertain to the test of AUC to the guess. Best cutoff measurements based on Youden index was 11.5 cmH2O in all patients (A) and 11.8 cmH2O in patients of Group A (B)
Secondary outcomes
Dynamic transpulmonary pressure swings and effort
The median (IQR) percentage of measurements with Plungsw, inspiratory Pdi swings (ΔPdi), and Pmussw falling within a range considered optimum [19, 21, 22, 31] is presented in Table 2.
ΔPlung ≥ 12 cmH2O was associated with higher values of effort indices, VT, and Plungsw (Additional file 2: Table S5). As Elung increased, Plungsw and efforts indices significantly increased, despite significant decreases in VT (Additional file 2: Table S3).
Discussion
In this study, tidal lung stress was documented in ARDS patients during their early transmission from controlled mechanical ventilation to assisted breathing with PAV+. The main findings are as follows: (1) Half of the patients (51.6%) did not exhibit ΔPlung exceeding 12 cmH2O and in cases where it was observed, such instances were of limited duration. (2) Most of the time, Plungsw and inspiratory effort indices were within a range considered optimum. (3) A significant proportion of patients exhibited expiratory muscle recruitment and a reduction in end-expiratory lung volume, as evidenced by decreased PLEE. (4) In these patients, the relaxation of expiratory muscles contributed to VT and as a result, ΔPrs underestimated ΔPlung, making it non-suitable as an alternative for tidal static lung stress.
Certain methodological issues of the study should be discussed first. The calculation of ΔPrs during PAV+ ventilation, relies on the measurement of Pplat, by random application of short end-inspiratory occlusions. Younes et al. have shown that since with PAV+ there is a link between the end of neural and mechanical inflation, this method provides a reliable estimate of passive elastic recoil pressure of the respiratory system at the corresponding VT [10]. Indeed, we observed that Pdi at the end of occlusion had returned to baseline and in the vast majority of the patients, Pgas remained constant during the pause time, assuring passive condition (Fig. 3). In a few patients, a small increase in Pgas (0.5–< 1.5 cmH2O) was occasionally observed, leading to an overestimation of the measured Pplat and ΔPrs by this amount. This, however, did not affect the computation of the PLEI, since expiratory muscle contraction during occlusion equally elevates Paw and Pes. Secondly, consistent with earlier investigations [32,33,34], PLEE remained predominantly negative throughout the recording period in 20 out of 31 patients. While this observation might raise concerns about the precision of Pes measurements [35, 36], a recent study involving lung-injured pigs and human cadavers assessed directly pleural pressure and demonstrated that Pes accurately mirrors pleural pressure in lung regions proximal to the esophageal balloon [37]. In this study, consistently negative PLEE values were observed, whether based on pleural or esophageal pressure measurements.
Transpulmonary driving pressure, dynamic transpulmonary pressure swings, and effort indices
It has been demonstrated that keeping ΔPlung < 12 cmH2O and Plungsw < 20 cmH2O in patients with ARDS without spontaneous breathing activity is linked to improved survival [18, 38]. These thresholds have been also suggested as targets during assisted breathing [22]. We demonstrated that ΔPlung ≥ 12 cmH2O occurred rarely and for a short period of time, while in half of the patients (51.6%) such values were never observed (Table 2). Similarly, Plungsw remained within the safe range for most of the time, even when the more conservative threshold of 15 cmH2O was examined. However, it is unknown if these results, documented during PAV+ ventilation, are also applicable in conventional assisted modes. Proportional ventilation, including PAV+ and neurally adjusted ventilator assist (NAVA), allows control of breathing system to regulate VT using chemical and reflex feedback mechanisms [39, 40], that tend to naturally protect the lung from over-distension [41, 42].
While direct studies in humans are lacking, it is generally considered safe to maintain ΔPdi within the range of 3 to 12 cmH2O and Pmussw within the range of 3 to 15 cmH2O to prevent both over-assistance and under-assistance, thereby ensuring the protection of the lungs and diaphragm [21]. In our study, primary physicians, who did not have access to study data, selected a level of assistance that averaged 50%. At this average assist, which amplifies inspiratory muscle pressure by a factor of 2 [43], both ΔPdi and, to a lesser extent, Pmussw fell within the optimal ranges.
These results are in contrast to those obtained by Di Mussi et al. [44]. In their study, 16 patients transitioned from control to pressure support ventilation, with continuous monitoring of electrical activity of the diaphragm (EAdi) over a 12-h period. They observed that 50% of breaths were either over-assisted (28%) or under-assisted (22%). Notwithstanding that in the study of Di Mussi et al. [44] EAdi was used as an index of under- or over-assistance, this disparity can be attributed to the functional principles of pressure support, which, unlike PAV+, hinders the control of breathing system in regulating VT [45, 46]. The observed greater variation in Pmussw in our study (Table 2) is likely influenced by expiratory and accessory inspiratory muscle pressures, which contribute to the calculation of Pmus, as well as uncertainties related to passive chest wall properties.
Driving pressure of respiratory system and relationship to driving transpulmonary pressure
Consistent with our previous studies involving a general population of critically ill patients [15, 17], the current study showed that in ARDS patients ventilated with PAV+, ΔPrs rarely exceeded 15 cmH2O. Although in our previous studies, we postulated that ΔPrs < 15 cmH2O was associated with acceptable tidal lung stress, the current investigation challenges this assumption. We found a considerably low (11.5 cmH2O) threshold of ΔPrs for detecting ΔPlung ≥ 12 cmH2O (Fig. 6), suggesting that the calculated ΔPrs underestimated ΔPlung. These results conflict those reported recently by Perez et al. in a small ARDS patients’ cohort during pressure support ventilation [47]. In that study, ΔPrs had an excellent precision to predict ΔPlung, with a value of 15 cmH2O being identified as the best threshold for detecting ΔPlung ≥ 12 cmH2O. However, Perez et al. selectively analyzed only a few occluded breaths while patients with expiratory muscles activity were excluded. The vast majority of our patients exhibited expiratory muscle activity during expiration, limiting the applicability of the findings of Perez et al. in routine clinical practice.
The explanation why ΔPrs underestimated ΔPlung, as well as why in several measurements ΔPlung was found higher than ΔPrs lies in the effect of end-expiratory lung volume on ΔPrs calculation (Fig. 1). When analyzing all breaths, a negative linear relationship between PLEE and ΔPlung/ΔPrs was observed in 81% of patients. Additionally, by analyzing the response to Elung changes, the linear mixed-effect model analysis found a significant effect of ΔPgas on PLEE, as well as of PLEE on ΔPlung/ΔPrs. These findings indicate that in several patients, expiratory muscle contraction reduced end-expiratory lung volume, as reflected by a lower PLEE. In these patients, ΔPrs underestimated the true driving pressure of the respiratory system because it assumed that the elastic recoil pressure when volume started to enter the lungs was equal to PEEP. However, expiratory muscle activation had decreased lung volume to a lower value than that corresponding to PEEP, and the very first moment that expiratory muscles relaxed, volume started to enter the lungs as a result of an alveolar pressure lower than PEEP (Fig. 1 and 3). Obviously, underestimation of the actual respiratory system driving pressure means underestimation of the calculated respiratory system elastance. Additionally, at lung volumes well below the level determined by PEEP, not only is the actual change in ΔPrs higher than the calculated value, but the elastance of the respiratory system may also increase. In this situation, the actual ΔPrs is even higher than what is calculated assuming a linear relationship between pressure and volume during lung inflation.
Response of respiratory variables to Elung changes
As anticipated, Elung changed considerably in all patients over the observation period and ΔPlung unanimously increased at higher Elung. However, we found two distinct responses to Elung increases. One group of patients (Group A), responded with increased PLEI, which drove the increase in ΔPlung. The second group (Group B), maintained constant or even decreased the end-inspiratory lung stress (PLEI) at higher Elung, and the higher ΔPlung resulted from PLEE decrease. Gastric pressure measurements showed that the observed decrease in PLEE was accomplished by a considerable increase in expiratory muscle activity. It is of interest to note that the further decrease in PLEE and increase in ΔPgas occurred when Elung increased by 27% (Fig. 4 and Additional file 2: Fig. S5), signifying a considerable increase in ventilatory demands. This response played a pivotal role in effectively mitigating the extent of end-inspiratory lung stress associated with a specific magnitude of ΔPlung elevation. It is not clear why this different response was observed. However, in Group A, the consistently higher Elung at all deciles and the already low PLEE values at low Elung (Fig. 5) suggest that some patients could not further decrease their already low-end-expiratory lung volume. Nevertheless, the response pattern was not dependent on patients’ characteristics, total duration of mechanical ventilation, length of ICU stay, and ICU outcome.
Interestingly, in Group B patients, ΔPrs remained constant and, consequently, lacked predictive value for high ΔPlung. This underscores the importance of end-expiratory lung volume reduction below that corresponding to PEEP, as the primary determinant of ΔPlung/ΔPrs. Therefore, interpreting ΔPrs as an index of tidal lung stress should be approached with great caution. Although the ΔPrs-ΔPlung relationship was examined during PAV+, similar results should be expected during all modes of assisted mechanical ventilation, since the underestimation of ΔPlung by ΔPrs does not depend on the mode but on the ability of expiratory muscles to decrease end-expiratory lung volume below that determined by PEEP.
We cannot determine whether the distinct response to deteriorating lung elastance conferred a lung-protected benefit in one group compared to the other. Lower PLEE was associated with minimal or no increase in end-inspiratory lung stress despite ΔPlung increase (Fig. 5). However, it remains uncertain to what extent this provides protection, as decreases in end-expiratory lung volume may potentially be associated with lung injury (atelectrauma), derecruitment, and gas exchange abnormalities [48].
Limitations
This study has certain limitations that should be considered. Firstly, end-expiratory lung volume changes were not directly monitored; instead, PLEE was utilized for this purpose. However, we believe that PLEE can provide valuable insights into the direction of change. When Elung remains constant or increases, a decrease in PLEE is indicative of a reduction in end-expiratory lung volume [11]. Therefore, we feel confident that in our study, a decrease in PLEE resulted from lower end-expiratory lung volume. Secondly, this single-center study included a group of patients with ARDS, who were enrolled when the primary physician opted for PAV+ as the initial assisted mode, following judgment of safety for allowing spontaneous breathing activity. Thus, the time lag between intubation and assisted ventilation differed. However, based on clinical judgment, the patients were included at relatively early stages of recovery from ARDS, when the respiratory drive was relatively high, as evidenced by the significant proportion displaying expiratory muscle activity [45]. Nevertheless, these findings may not be generalizable to all critically ill patients, although this patient group is particularly relevant when assessing ΔPrs as a surrogate for tidal lung stress. Thirdly, this prospective observational study is subject to the inherent biases associated with patient selection and the lack of strict adherence to specific algorithms when titrating PEEP and the level of assist with PAV+ [49]. Nevertheless, this can also be considered a strength, since it allows us to capture the impact of every day clinical practice on ΔPlung and effort indices. Fourthly, since this was beyond the scope of the study, the impact of factors that influence the recruitment of expiratory muscles, such as respiratory acidosis, sedation, and diaphragmatic weakness on group response could not be assessed. Finally, the pendelluft phenomenon, which may occur in patients with high respiratory drive and unpredictably change tidal volume, was not considered.
Conclusions
Transpulmonary driving pressures and inspiratory efforts were largely maintained within a safe range during proportional assist ventilation. Contrary to existing assumptions, the respiratory system driving pressure underestimated the transpulmonary driving pressure due to expiratory muscle activity which lowers end-expiratory lung volume below that determined by PEEP. This phenomenon, which should occur regardless of the mode of support, limits the usefulness of respiratory system driving pressure as a substitute for transpulmonary driving pressure in patients with active breathing.
Abbreviations
- ΔP lung :
-
Transpulmonary driving pressure
- ΔP rs :
-
Driving pressure of the respiratory system
- P plat :
-
End-inspiratory plateau pressure
- PEEP:
-
Positive end-expiratory pressure
- V T :
-
Tidal volume
- Plungsw :
-
Transpulmonary pressure swings
- ARDS:
-
Acute respiratory distress syndrome
- V′:
-
Airflow
- Paw:
-
Airway pressure
- Pes:
-
Esophageal pressure
- Pgas:
-
Gastric pressure
- P lung (Paw-Pes):
-
Transpulmonary pressure
- Pdi (Pgas-Pes):
-
Transdiaphragmatic pressure
- Pmussw :
-
Respiratory muscles (inspiratory and expiratory) pressure swings
- ΔP gas :
-
Rise in gastric pressure during the expiratory phase
- PEEPi:
-
Dynamic intrinsic PEEP
- 7-brMA:
-
Seven-breath moving average
- E lung :
-
Lung elastance
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the receiver operating characteristic curve
- ΔPdi:
-
Inspiratory Pdi swings
- P LEI :
-
End-inspiratory transpulmonary pressure
- P LEE :
-
End-expiratory transpulmonary pressure
- CMV:
-
Control mechanical ventilation
- PAV+:
-
Proportional assist ventilation with load adjustable gain factors
- ICU:
-
Intensive care unit
References
Baedorf Kassis E, Loring SH, Talmor D. Mortality and pulmonary mechanics in relation to respiratory system and transpulmonary driving pressures in ARDS. Intensive Care Med. 2016;42(8):1206–13.
Chiumello D, Carlesso E, Brioni M, Cressoni M. Airway driving pressure and lung stress in ARDS patients. Crit Care. 2016;20(1):276.
Gattinoni L, Carlesso E, Cadringher P, Valenza F, Vagginelli F, Chiumello D. Physical and biological triggers of ventilator-induced lung injury and its prevention. Eur Respir J Suppl. 2003;47:15s–25s.
Protti A, Cressoni M, Santini A, Langer T, Mietto C, Febres D, et al. Lung stress and strain during mechanical ventilation: any safe threshold? Am J Respir Crit Care Med. 2011;183(10):1354–62.
Akoumianaki E, Maggiore SM, Valenza F, Bellani G, Jubran A, Loring SH, et al. The application of esophageal pressure measurement in patients with respiratory failure. Am J Resp Crit Care Med. 2014;189:520–31.
Amato MBP, Meade MO, Slutsky AS, Brochard L, Costa ELV, Schoenfeld DA, et al. Driving pressure and survival in the acute respiratory distress syndrome. New Engl J Med. 2015;372(8):747–55.
Roca O, Peñuelas O, Muriel A, García-De-Acilu M, Laborda C, Sacanell J, et al. Driving pressure is a risk factor for ARDS in mechanically ventilated subjects without ARDS. Respir Care. 2021;66(10):1505–13.
Laffey JG, Bellani G, Pham T, Fan E, Madotto F, Bajwa EK, et al. Potentially modifiable factors contributing to outcome from acute respiratory distress syndrome: the LUNG SAFE study. Intensive Care Med. 2016;42(12):1865–76.
Soundoulounaki S, Akoumianaki E, Kondili E, Pediaditis E, Prinianakis G, Vaporidi K, et al. Airway pressure morphology and respiratory muscle activity during end-inspiratory occlusions in pressure support ventilation. Crit Care. 2020;24(1):467.
Younes M, Webster K, Kun J, Roberts D, Masiowski B. A method for measuring passive elastance during proportional assist ventilation. Am J Respir Crit Care Med. 2001;164(1):50–60.
Baedorf Kassis E, Loring SH, Talmor D. Lung volumes and transpulmonary pressure are decreased with expiratory effort and restored with passive breathing in ARDS: a reapplication of the traditional Campbell diagram. Intensive Care Med. 2018;44(4):534–6.
Doorduin J, Roesthuis LH, Jansen D, van der Hoeven JG, van Hees HWH, Heunks LMA. Respiratory muscle effort during expiration in successful and failed weaning from mechanical ventilation. Anesthesiology. 2018;129(3):490–501.
Guervilly C, Bisbal M, Forel JM, Mechati M, Lehingue S, Bourenne J, et al. Effects of neuromuscular blockers on transpulmonary pressures in moderate to severe acute respiratory distress syndrome. Intensive Care Med. 2017;43(3):408–18.
Iscoe S. Control of abdominal muscles. Prog Neurobiol. 1998;56(4):433–506.
Georgopoulos D, Xirouchaki N, Tzanakis N, Younes M. Driving pressure during assisted mechanical ventilation: Is it controlled by patient brain? Respir Physiol Neurobiol. 2016;228:69–75.
Younes M, Remmers J. Control of tidal volume and respiratory frequency. In: Hornbein T, editor. Control of Breathing. New York: Marcel Deckker; 1981. p. 163–70.
Vaporidi K, Psarologakis C, Proklou A, Pediaditis E, Akoumianaki E, Koutsiana E, et al. Driving pressure during proportional assist ventilation: an observational study. Ann Intensive Care. 2019;9:1–9.
Chen L, Grieco DL, Beloncle F, Chen GQ, Tiribelli N, Madotto F, et al. Partition of respiratory mechanics in patients with acute respiratory distress syndrome and association with outcome: a multicentre clinical study. Intensive Care Med. 2022;48(7):888–98.
De Vries HJ, Tuinman PR, Jonkman AH, Liu L, Qiu H, Girbes ARJ, et al. Performance of noninvasive airway occlusion maneuvers to assess lung stress and diaphragm effort in mechanically ventilated critically Ill patients. Anesthesiology. 2023;138(3):274–88.
Dianti J, Tisminetzky M, Ferreyro BL, Englesakis M, Del Sorbo L, Sud S, et al. Association of positive end-expiratory pressure and lung recruitment selection strategies with mortality in acute respiratory distress syndrome a systematic review and network meta-analysis. Am J Respir Crit Care Med. 2022;205(11):1300–10.
Goligher EC, Dres M, Patel BK, Sahetya SK, Beitler JR, Telias I, et al. Lung- And diaphragm-protective ventilation. Am J Respir Crit Care Med. 2020;202(7):950–61.
De Vries HJ, Jonkman AH, De Grooth HJ, Duitman JW, Girbes ARJ, Ottenheijm CAC, et al. Lung- and diaphragm-protective ventilation by titrating inspiratory support to diaphragm effort: a randomized clinical trial. Crit Care Med. 2022;50(2):192–203.
Georgopoulos D, Mitrouska I, Bshouty Z, Webster K, Patakas D, Younes M. Respiratory response to CO2 during pressure-support ventilation in conscious normal humans. Am J Respir Crit Care Med. 1997;156(1):146–54.
Ceorgopoulos D, Mitrouska I, Webster K, Bshouty Z, Younes M. Effects of inspiratory muscle unloading on the response of respiratory motor output to CO2. Am J Respir Crit Care Med. 1997;155(6):2000–9.
Parthasarathy S, Jubran A, Tobin MJ. Cycling of inspiratory and expiratory muscle groups with the ventilator in airflow limitation. Am J Respir Crit Care Med. 1998;158:1471–8.
Parthasarathy S, Jubran A, Laghi F, Tobin MJ. Sternomastoid, rib cage, and expiratory muscle activity during weaning failure. J Appl Physiol. 2007;103(1):140–7.
Georgopoulos D, Prinianakis G, Kondili E. Bedside waveforms interpretation as a tool to identify patient-ventilator asynchronies. Intensive Care Med. 2006;32:34–47.
Lessard MR, Lofaso F, Brochard L. Expiratory muscle activity increases intrinsic positive end-expiratory pressure independently of dynamic hyperinflation in mechanically ventilated patients. Am J Respir Crit Care Med. 1995;151:562–9.
Swets JA. Measuring the accuracy of diagnostic systems. Science. 1988;240(4857):1285–93.
Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3(1):32–5.
Dianti J, Fard S, Wong J, Chan TCY, Del Sorbo L, Fan E, et al. Strategies for lung- and diaphragm-protective ventilation in acute hypoxemic respiratory failure: a physiological trial. Crit Care. 2022;26(1):1–10.
Talmor D, Sarge T, Malhotra A, O’Donnell CR, Ritz R, Lisbon A, et al. Mechanical ventilation guided by esophageal pressure in acute lung injury. New Engl J Med. 2008;359(20):2095–104.
Talmor D, Sarge T, O’Donnell CR, Ritz R, Malhotra A, Lisbon A, et al. Esophageal and transpulmonary pressures in acute respiratory failure. Crit Care Med. 2006;34(5):1389–94.
Loring SH, O’Donnell CR, Behazin N, Malhotra A, Sarge T, Ritz R, et al. Esophageal pressures in acute lung injury: do they represent artifact or useful information about transpulmonary pressure, chest wall mechanics, and lung stress? J Appl Physiol. 2010;108:515–22.
De Chazal I, Hubmayr RD. Novel aspects of pulmonary mechanics in intensive care. Br J Anaesth. 2003;91(1):81–91.
Hager DN, Brower RG. Customizing lung-protective mechanical ventilation strategies. Crit Care Med. 2006;34(5):1554–5.
Yoshida T, Amato MBP, Grieco DL, Chen L, Lima CAS, Roldan R, et al. Esophageal manometry and regional transpulmonary pressure in lung injury. Am J Respir Crit Care Med. 2018;197(8):1018–26.
Chiu LC, Hu HC, Hung CY, Chang CH, Tsai FC, Yang CT, et al. Dynamic driving pressure associated mortality in acute respiratory distress syndrome with extracorporeal membrane oxygenation. Ann Intensive Care. 2017;7(1):1–9.
Grasselli G, Beck J, Mirabella L, Pesenti A, Slutsky AS, Sinderby C. Assessment of patient-ventilator breath contribution during neurally adjusted ventilatory assist. Intensive Care Med. 2012;38(7):1224–32.
Schmidt M, Kindler F, Cecchini J, Poitou T, Morawiec E, Persichini R, et al. Neurally adjusted ventilatory assist and proportional assist ventilation both improve patient-ventilator interaction. Crit Care. 2015;19:56.
Euler C. Brainstem mechanisms for generation and control of breathing pattern. In: Handbook of Physiology. The Respiratory System. American Physiological Society Press, Bethesda; 1986. p 1–68.
Clark FJ, von Euler C. On the regulation of depth and rate of breathing. J Physiol. 1972;222(2):267–95.
Younes M. Proportional assist ventilation, a new approach to ventilatory support. Theory Am Rev Respir Dis. 1992;145(1):114–20.
Di Mussi R, Spadaro S, Volta CA, Bartolomeo N, Trerotoli P, Staffieri F, et al. Continuous assessment of neuro-ventilatory drive during 12 h of pressure support ventilation in critically ill patients. Crit Care. 2020;24(1):1–11.
Vaporidi K, Akoumianaki E, Telias I, Goligher EC, Brochard L, Georgopoulos D. Respiratory drive in critically Ill patients. Pathophysiology and clinical implications. Am J Respir Crit Care Med. 2020;201(1):20–32.
Akoumianaki E, Vaporidi K, Georgopoulos D. The injurious effects of elevated or nonelevated respiratory rate during mechanical ventilation. Am J Respir Crit Care Med. 2019;199(2):149–57.
Pérez J, Dorado JH, Accoce M, Plotnikow GA. Airway and transpulmonary driving pressure by end-inspiratory holds during pressure support ventilation. Respir Care. 2023;68(11):1483–92.
Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013;369(22):2126–36.
Xirouchaki N, Kondili E, Vaporidi K, Xirouchakis G, Klimathianaki M, Gavriilidis G, et al. Proportional assist ventilation with load-adjustable gain factors in critically ill patients: Comparison with pressure support. Intensive Care Med. 2008;34(11):2026–34.
Author information
Authors and Affiliations
Contributions
DG conceived the study. VS and EA conducted data collection. VS, EA, DG, KV, and EK conducted data analysis. DG drafted the manuscript first version. ES developed and validated the computer program for identifications of occluded breaths. All authors critically revised and approved the final version to be published.
Corresponding author
Ethics declarations
Competing interests
DG, EA, and KV received lecture fee from Medtronic. The other authors declare no competing interests. Medtronic was not involved in any aspect of the design or conduct of the study, the data analysis, or the manuscript preparation and presentation.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Figure S1.
Additional file 2.
Supplementary Methods, Results, Figures, Tables and References.
Additional file 3.
Individual data of Transpulmonary driving pressure over time.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Stamatopoulou, V., Akoumianaki, E., Vaporidi, K. et al. Driving pressure of respiratory system and lung stress in mechanically ventilated patients with active breathing. Crit Care 28, 19 (2024). https://doi.org/10.1186/s13054-024-04797-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-024-04797-3