
Abstract
Background
Pulse pressure and stroke volume variation (PPV and SVV) have been widely used in surgical patients as predictors of fluid challenge (FC) response. Several factors may affect the reliability of these indices in predicting fluid responsiveness, such as the position of the patient, the use of laparoscopy and the opening of the abdomen or the chest, combined FC characteristics, the tidal volume (Vt) and the type of anesthesia.
Methods
Systematic review and metanalysis of PPV and SVV use in surgical adult patients. The QUADAS-2 scale was used to assess the risk of bias of included studies. We adopted a metanalysis pooling of aggregate data from 5 subgroups of studies with random effects models using the common-effect inverse variance model. The area under the curve (AUC) of pooled receiving operating characteristics (ROC) curves was reported. A metaregression was performed using FC type, volume, and rate as independent variables.
Results
We selected 59 studies enrolling 2,947 patients, with a median of fluid responders of 55% (46–63). The pooled AUC for the PPV was 0.77 (0.73–0.80), with a mean threshold of 10.8 (10.6–11.0). The pooled AUC for the SVV was 0.76 (0.72–0.80), with a mean threshold of 12.1 (11.6–12.7); 19 studies (32.2%) reported the grey zone of PPV or SVV, with a median of 56% (40–62) and 57% (46–83) of patients included, respectively. In the different subgroups, the AUC and the best thresholds ranged from 0.69 and 0.81 and from 6.9 to 11.5% for the PPV, and from 0.73 to 0.79 and 9.9 to 10.8% for the SVV. A high Vt and the choice of colloids positively impacted on PPV performance, especially among patients with closed chest and abdomen, or in prone position.
Conclusion
The overall performance of PPV and SVV in operating room in predicting fluid responsiveness is moderate, ranging close to an AUC of 0.80 only some subgroups of surgical patients. The grey zone of these dynamic indices is wide and should be carefully considered during the assessment of fluid responsiveness. A high Vt and the choice of colloids for the FC are factors potentially influencing PPV reliability.
Trial Registration: PROSPERO (CRD42022379120), December 2022. https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=379120
Similar content being viewed by others
Introduction
Fluid administration in the operating room is a cornerstone of perioperative hemodynamic optimization [1,2,3,4], and its titration is obtained by adopting the fluid challenge (FC) to assess preload dependency and avoid fluid overload. In patients under mechanical ventilation, dynamic indices such as stroke volume variation (SVV) and pulse pressure variation (PPV) reliably predict the effect of FC because the fixed and repetitive inspiratory and expiratory pressure changes affect right ventricle’s preload, afterload and, hence, stroke volume (SV).
In the last decade, different aspects of the use of PPV and SVV in the operating room have been further investigated, providing clinically relevant implications. First of all, PPV and SVV reliability is affected by specific validity criteria including a tidal volume (Vt) > 8 ml/kg, a normal right ventricle’s function, the absence of heart arrythmias, an heart rate/respiratory rate ratio > 3.6 and an unimpaired respiratory mechanics [5,6,7], becoming clinically useful only below or above a grey zone of uncertainty [8]. The majority of these criteria are usually respected in the operating room, with the exception of a protective Vt, which seems to be associated with better outcomes [9] and is now suggested as standard ventilation in the operating room [10]. This is clinically meaningful, since reducing the average Vt adopted in the operating room, also the threshold adopted in the past to stratify fluid responders and non-responders (i.e. 13% [11]) may be changed.
On the contrary, in the operating room other factors associated to the type of surgery may impact a lot on PPV and SVV reliability, such as the type of anesthesia adopted, the position of the patient, the use of laparoscopy (LPS) and the opening of the abdomen or the chest.
As second, the impact of different determinants of the FC itself (i.e. the volume, the rate, the type of fluid used and the threshold to define fluid responsiveness [12,13,14]), have been further investigated and, as consequence, the value of PPV and SVV in studies adopting different types of FC may be inconsistent.
We, therefore, conducted a comprehensive systematic review and metanalysis with the primary aim of investigating the performance of PPV and SVV in different surgical setting, stratifying the patients according to chest/abdomen opening, intraoperative position, and the use of LPS.
Secondarily, we assessed the impact of other potential factors influencing the reliability of these indices in predicting fluid responsiveness in mechanically ventilated patients in the different surgical settings, specifically FC characteristics, the modality of ventilation and the type of anestestia.
Material and methods
We adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis – Protocols (PRISMA-P) guidelines [15] (Additional file 1: Table S1). The protocol of this study was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42022379120).
Data sources and search strategy
A systematic literature search was performed including PUBMED® and EMBASE® and the Cochrane Controlled Clinical trials register databases, by using the following terms: 'pulse pressure variation' OR 'stroke volume variation' OR 'fluid responsiveness' AND (surgery) OR (surgical patients) (Additional file 1: Table S2).
Articles written in English, enrolling at least 10 adult, mechanically ventilated patients undergoing elective surgery and published from 1st January 2000 until 1st March 2023 in indexed scientific journals were considered. Editorials, commentaries, letters to editor, opinion articles, reviews, and meeting abstracts were excluded. References of selected papers, review articles, commentaries, and editorials on this topic were also reviewed to identify other studies of interest missed during the primary search. When multiple publications of the same research group/center described potentially overlapping cohorts, the most recent publications were selected.
We included only those studies clearly stating the threshold for defining fluid responsiveness as SV (or its surrogates) increase above a predefined limit. Articles including data collected in the postoperative period were excluded, while data recorded in the post-operative ICU just after the end of the surgery were included. Finally, we excluded studies performed during liver transplantation, in pediatric population and during pregnancy/labor.
Data abstraction
Three couples of examiners independently performed the evaluation of titles and abstracts. The articles were then subdivided into three subgroups: “included” and “excluded” (if the two examiners agreed with the selection) or “uncertain” (in case of disagreement). In the case of “uncertain” classification, discrepancies were resolved by further examination performed by two expert authors (A.M. and M.Ce.). We used a standardized electronic spreadsheet (Microsoft Excel, V 14.4.1; Microsoft, Redmond, WA) to extract data from all included studies, recording: trial characteristics (i.e. number of centers, country), patient population (i.e. demographics, type of surgery, baseline illness severity scores), intraoperative monitoring and interventions (i.e. mechanical ventilation characteristics, monitoring technology used, FC characteristics).
Risk of bias assessment in the included studies
Assessment of risk of bias in the included studies
The QUADAS-2 scale was used to assess the risk of bias of the included studies [16]. Two expert authors (A.M. and M.Ce.) independently examined the studies using predefined criteria, which are reported in the Additional file 1: Table S4:
For each criterion, the risk of bias was judged as high (3 points), unclear (2 points) or low (1 point). If the answers to all signaling questions for a domain were “yes,” then risk of bias was judged as “low”. If any signaling question was answered “no,” the potential risk of bias was defined as indicted in Additional file 1: Table S4. The sum of these points was used to calculate the global risk of bias. Studies were included in the highest risk of bias group if the sum of the points obtained by the risk of bias and applicability judgment assessment, was higher than the median value for all the studies [17].
Statistical analysis
Descriptive analysis was carried out: the statistical unit of observation for all the selected variables was the single study and not the patient. Quantitative variables were summarized with means (standard deviations, SD) or medians (inter-quartile ranges, IQR) according to their distribution.
Patients were stratified in five main groups, according to the surgical characteristics at inclusion: (1) Patients enrolled with closed abdomen and chest; (2) Patients enrolled with closed abdomen and open chest (including sternotomy and thoracotomy); (3) Patients enrolled with open abdomen and closed chest; (4) LPS; (5) Prone position.
We adopted a metanalysis pooling of aggregate data with random effects models using the common-effect inverse variance model. The area under the curve (AUC) of pooled receiving operating characteristics (ROC) curves was reported with 95% confidence intervals (95%CI). In-between study heterogeneity was assessed with the I2 statistic. According to Higgins et al., I2 values around 25%, 50%, and 75% represented no, low, moderate, and high heterogeneity [18]. Unless stated otherwise, we considered the number of the FC performed equal to the number of patients included in the study. In the studies comparing two different surgical settings in the same population (i.e., open chest/closed chest, supine/prone etc.) data of the two subgroups of patients were separately analyzed for the purpose of the ROC curve analysis. Missing data in AUC reporting was considered an exclusion criterion from metanalysis.
For each of these five subgroups we performed a meta-regression considering the following independent variables: 1) Tidal volume (Vt) ≥ 8 ml/kg; 2) Positive end-expiratory pressure (PEEP) level (i.e., PEEP = 0 cmH2O; PEEP = 0–5 cmH2O; PEEP > 5 cmH2O); 3) total intravenous anesthesia (TIVA); 4) FC using colloids vs crystalloids; 5) volume of FC administration > 4 ml/kg; 6) rate of FC administration > 15 min).
In case of mixed populations (i.e. receving TIVA anesthesia/alogenates or undergoing LPS /laparotomy), the subgroup including at least 75% of the population was used for the final classification of the study.
The statistical analysis was performed using the software STATA® version 17 (StataCorp, College Station, TX, USA) and Medcalc (Software 8.1.1.0; Mariakerke, Belgium). For all comparisons, we considered significant p values < 0.05.
Results
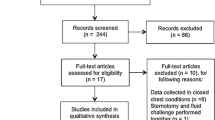
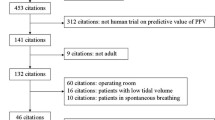
The electronic search identified 3,300 potentially relevant titles and 59 full-text manuscripts were finally selected. A detailed description of the selection process is provided in Fig. 1. Overall, the included studies enrolled 2,947 patients with a median age of 61 (55–65), and 59% (46–71) were males. The median number of patients enrolled per study was 40 (26–52), overall receiving 3,870 FCs with a median number of FCs administered of 40 (25–53) for each study and a median of fluid responders of 55% (46–63), ranging from 26.9 [19] to 91.4% [20], and colloids have been used in 41 studies (68.3%) (Table 1).

Flow of the studies
Preoperative comorbidities were reported for 2280 patients (76.1%), with cancer diagnoses being the most represented (32.7%). Surgery type was reported for 2932 patients (99.5%), with neurosurgical operations (26.4%) being the most prevalent (Additional file 1: Table S3). Seven studies (11.6%) enrolled only patients undergoing LPS, in 25 (42.4%) the patients received halogenate/opiate anesthesia, while in 23 (39.0%) TIVA and in the remaining 11 studies (18.6%) the type of anesthesia was mixed or unspecified.
Overall, the median (IQR) QUADAS-2 score of the included studies was 9 (7 -10) and 18 studies (30.5%) were classified in the subgroup with the highest risk of bias (Additional file 1: Table S5).
Overall pooled AUC of PPV and SVV in the included studies
The pooled AUC for the PPV obtained from 52 studies was 0.77 (0.73–0.80), with a mean threshold of 10.8 (10.6–11.0) (I2 = 92.2%) (Additional file 1: Table S6).
The pooled AUC for the SVV obtained from 36 studies was 0.76 (0.72–0.80), with a mean threshold of 12.1 (11.6–12.7) (I2 = 88.3%) (Additional file 1: Table S7).
Overall, 19 studies (32.2%) reported the grey zone of PPV or SVV, with a median of 56% (40–62) and 57% (46–83) of patients included in this range of uncertainty, respectively.
Pooled AUC and grey zone in the different PPV subgroups
-
1.
In the studies enrolling patients with closed chest and abdomen, the pooled AUC for PPV was 0.79 (95%CI 0.73–0.84) for a threshold of 10.9% (10.5–11.2) and a I2 of 92.7%. (Additional file 1: Figure S1); 7 studies [21,22,23,24,25,26,27] reported a median of 61.8% of patients (52–75) included in the grey zone of PPV, with a median low value of 6% (5–8) and a high value of 12% (11–17).
-
2.
In the studies enrolling patients with closed chest and open abdomen, the pooled AUC for PPV was 0.79 (95%CI 0.71–0.88) for a threshold of 11.5% (11.3–11.6) and a I2 of 88.2%. (Additional file 1: Figure S2); 6 studies [8, 25, 26, 28,29,30,31,32] reported a median of 43.5% (36–50) included in the grey zone of PPV, with a median low value of 7% (5–10) and a high value of 14% (12–25).
-
3.
In the studies enrolling patients with closed abdomen and open chest, the pooled AUC for PPV was 0.69 (95%CI 0.59–0.78) for a threshold of 6.9% (6.7–7.11) and a I2 of 68.8%. (Additional file 1: Figure S3); 1 study [33] reported 86.0% of patients included in the grey zone of PPV, with a low value of 5% and a high value of 19%.
-
4.
Studies including patients undergoing LPS showed a pooled PPV AUC of 0.74 (95%CI 0.64–0.83), with a pooled threshold of 11.3% (10.6 – 11.9) and a I2 of 60.7%. (Additional file 1: Figure S4); 1 study [34] reported 26% of patients included in the grey zone of PPV, and 2 studies [34, 35] a median low value of 6% (6–7) and a high value of 15% (9–21).
-
5.
In studies including patients in prone position, the pooled PPV AUC was 0.78 (95%CI 0.69–0.88), with a pooled threshold of 11.2% (10.9–11.5) and a I2 of 84.9%. (Additional file 1: Figure S5); 2 studies [36, 37] reported a median of 60.0% (58–62) included in the grey zone of PPV, with a median low value of 6% (5–6) and a high value of 11% (10–11),
Pooled AUC and grey zone in the different SVV subgroups
-
1.
In the studies enrolling patients with closed chest and abdomen, the pooled AUC for SVV was 0.76 (95%CI 0.69–0.82) for a threshold of 10.7% (10.4–10.9) and a I2 of 78.4%. (Additional file 1: Figure S6); 1 study [26] reported 88.5% of patients included in the grey zone of SVV, while 2 studies [30, 31] reported a median low value of 5% (3–7) and a high value of 15% (13–16).
-
2.
In the studies enrolling patients with closed chest and open abdomen, the pooled AUC for SVV was 0.79 (95%CI 0.70–0.88) for a threshold of 10.1% (9.8–10.5) and a I2 of 86.2%. (Additional file 1: Figure S7); 3 studies [28, 30, 31] reported a median of 46.0% (33.0–57.0) included in the grey zone of SVV, with a median low value of 5% (4–6) and a high value of 12% (11–15).
-
3.
In the studies enrolling patients with closed abdomen and open chest, the pooled AUC for SVV was 0.72 (95%CI 0.57–0.87) for a threshold of 10.0% (9.8–10.2) and a I2 of 85.7%. (Additional file 1: Figure S8); 1 study [33] reported 93.0% of patients included in the grey zone of SVV, with a low value of 5% and a high value of 18%.
-
4.
Studies including patients undergoing LPS showed a pooled SVV AUC of 0.78 (95%CI 0.69–0.87), with a pooled threshold of 10.8% (10.4–11.3) and a I2 of 64.4%. (Additional file 1: Figure S9); 1 study [34] reported 55.0% of patients included in the grey zone of SVV, while 3 studies [34, 35, 38] reported a median low value of 7% (3–13) and a high value of 13% (6–15).
-
5.
In studies including patients in prone position, the pooled SVV AUC was 0.73 (95%CI 0.64–0.83), with a pooled threshold of 10.2% (9.9–10.4) and a I2 of 74.9%. (Additional file 1: Figure S10); 1 study [37] reported 66% of patients included in the grey zone of SVV, with a median low value of 6% and a high value of 14%.
Data about pooled ROC and grey zones of the considered subgroups for PPV and SVV are summarized in the Table 2.
Metaregression
As shown in Table 3, the pooled AUC for PPV was positively affected by the by Vt ≥ 8 ml/kg (p < 0.001) and by the use of colloids for the FC (p < 0.001) in the group of studies with closed chest and abdomen; the Vt ≥ 8 ml/kg (p < 0.001) was also associated to increased AUC in studies enrolling prone patients. The AUCs of these subgroups are reported in the Table 4. The was no effect of any of the considered variables on the AUC of SVV.
Discussion
This systematic review and metanalysis evaluated the PPV and SVV performance in different surgical settings, updating previous papers and focusing on the role of potential factors that may be associated with better performance of the indices for predicting fluid responsiveness. Our data may be summarized as follows: (1) the overall performance of PPV and SVV in operating room in predicting fluid responsiveness is moderate, ranging close to an AUC of 0.80 only in non-LPS surgery, with closed chest, suggesting caution in the interpretation of this indices; (2) overall, the best threshold of PPV is 11%, while for the SVV is 10%. However, the minority of the studies reporting the grey zone showed that the majority of patients are patients included in this range of uncertainty, respectively; (3) a high Vt and the choice of colloids, may impact positively on PPV performance, especially among patients with closed chest and abdomen, or in prone position.
PPV and SVV have been widely investigated as indices to guide fluid administration, but also as targets of a goal-directed therapy [22]. In the operating room, most of the validity criteria affecting PPV and SVV reliability (such as low tidal volume, heart rate/respiratory rate ratio < 3.6, presence of spontaneous breathing activity, low respiratory compliance, right ventricle dysfunction) occur less frequently compared to critically ill patients. This would, in principle, improve their performance as tests for fluid responsiveness. The role of Vt has also been extensively investigated. In 2009 Marik et al. reported on an AUC of 0.93 (95% CI, 0.92–0.94) for the PPV in a small subgroup of surgical studies adopting a mean Vt > 8 ml/kg [39]. In 2011 Zhang et al. reported an AUC of 0.94 (95% CI, 0.907–0.945) for the SVV in 8 surgical studies [40], decreasing to 0.84 by excluding only one study on 20 patients [41]. Similarly, Messina et al. in 2018 reported an AUC of 0.86 for PPV (10 studies) and of 0.87 for SVV (16 studies) in surgical trials with a mean Vt of 8 ml/kg [11]. The metaregression showed that the only AUCs of the PPV in the subgroups of patients with closed chest and abdomen or in prone position were positively affected by the intraoperative use of a Vt ≥ 8 ml/kg. Although the use of an intraoperative lung-protective ventilation strategy is associated with a better outcome [9] and is now suggested as standard practice in the operating room [10], this limits the assessment of fluid responsiveness in surgical patients by means of dynamic indices and, not surprisingly, pooling data from recent studies show an overall worse performance of PPV, as compared to the past.
Accordingly to the reduced Vt, also the thresholds of PPV and SVV should be reconsidered. Our results suggest a best pooled threshold for PPV (11%) and SVV (10%) both lower than 13% proposed in the past [8]. However, these thresholds derived from ROC curve analysis may be scarcely useful in clinical practice, since it often falls within the grey zone of uncertainty. Considering the different subgroups, our results show that the range of PPV and SVV values included between the lowest 5–7% and the highest of 12–19%, should be considered with caution, suggesting the use of other functional hemodynamic tests in surgical patients for enhancing the reliability of these dynamic indices [17].
The metaregression showed that the AUC of the PPV in the subgroups of patients with closed chest and abdomen was improved by the use of colloids (p < 0.001) and, potentially, by a FC volume > 4 ml/kg (borderline effect; p = 0.05). For the SVV, these two variables showed also borderline effects (p = 0.06 and p = 0.08, respectively). Recently, it has been demonstrated that at least 4 ml/kg should be infused to effectively challenge cardiac preload [14, 42]. Accordingly, reducing FC volume would impact on the identification of fluid responders and, in turn, on AUC magnitude. Colloids are still adopted in the operating room, and their different persistence in the intravascular space may affect fluid responsiveness especially when the time of evaluation of FC is prolonged above 10 min (when the effect of a crystalloid FC fades[13]).
Strenghts and limitations
To the best of our knowledge, this is the most updated and largest metanalysis on PPV and SVV use in the operating room. Our approach considered the physiologic characteristics of the surgical patients and not the specific type of surgery. This implies that the results may be applied to different settings (i.e. the subgroup with closed chest and abdomen may include neurosurgery, vascular non-abdominal surgery and otolaryngology surgery). Moreover, the meta-regression analysis enhanced specific variables potentially affecting PPV and SVV reliability.
Regarding the limitations, despite the minority of the studies (30.5%) were classified in the subgroup with the highest risk of bias, the QUADAS-2 score, however, as any other bias score, would not perfectly fit to the design of the included studies, and it has been adapted by the authors in some domain, considering clinical of physiological variables potentially affecting FC outcome and, hence, ROC curve analysis.
Moreover, the heterogeneity of the AUCs obtained from of the analyzing data ranged from 43.5 to 88.2%, implying a significant variability in the population enrolled and data presentation. Again, this is, unfortunately, a quite common problem in the field of hemodynamic for either critically ill and surgical patients as previously shown in other papers [17, 43]. Overall, data obtained from the meta-regression should be considered with caution, due to the small number of studies included in some subgroup.
This is not a meta-analysis based on individual data and the assessment of fluid responsiveness has been evaluated by different hemodynamic tools, including echocardiography, calibrated and uncalibrated machines.
The authors state some discrepancies between the final literature search, focused on PPV and SVV use in studies assessing the performance of these variables in predicting fluid responsiveness, and the original PROSPERO registration, which includes also randomized-controlled studies adopting PVV and SVV in the context of perioperative hemodynamic optimization. After an initial screening, it was clear that these studies should have been not included in the literature search, and the string has been modified, accordingly.
Conclusions
The overall performance of PPV and SVV in operating room in predicting fluid responsiveness is moderate, ranging close to an AUC of 0.80 only for some subgroups of surgical patients, with a best threshold of 11% and 10%, respectively. Considering the different subgroups, the grey zone of these dynamic indices (from 5 to 7% and to 12 to 19%) is wide and should be carefully considered during the assessment of fluid responsiveness. A high Vt and the choice of colloids for the FC, may impact positively on the performance of the dynamic indices, especially among patients with closed chest and abdomen, or in prone position.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- FC:
-
Fluid challenge
- MV:
-
Mechanical ventilation
- SVV:
-
Stroke volume variation
- PPV:
-
Pulse pressure variation
- SV:
-
Stroke volume
- AUC:
-
Area under the curve (AUC) of pooled receiving operating characteristics (ROC) curve
- LPS:
-
Laparoscopy
- Vt:
-
Tidal volume
References
Thiele RH, Raghunathan K, Brudney CS, Lobo DN, Martin D, Senagore A, Cannesson M, Gan TJ, Mythen MM, Shaw AD, Miller TE. Perioperative quality initiative IW: American society for enhanced recovery (aser) and perioperative quality initiative (poqi) joint consensus statement on perioperative fluid management within an enhanced recovery pathway for colorectal surgery. Perioper Med. 2016;5:24.
Feldheiser A, Aziz O, Baldini G, Cox BP, Fearon KC, Feldman LS, Gan TJ, Kennedy RH, Ljungqvist O, Lobo DN, Miller T, Radtke FF, Ruiz Garces T, Schricker T, Scott MJ, Thacker JK, Ytrebo LM, Carli F. Enhanced recovery after surgery (eras) for gastrointestinal surgery, part 2: consensus statement for anaesthesia practice. Acta Anaesthesiol Scand. 2016;60:289–334.
Makaryus R, Miller TE, Gan TJ. Current concepts of fluid management in enhanced recovery pathways. Br J Anaesth. 2018;120:376–83.
Navarro LH, Bloomstone JA, Auler JO Jr, Cannesson M, Rocca GD, Gan TJ, Kinsky M, Magder S, Miller TE, Mythen M, Perel A, Reuter DA, Pinsky MR, Kramer GC. Perioperative fluid therapy: a statement from the international fluid optimization group. Perioper Med. 2015;4:3.
Biais M, Ehrmann S, Mari A, Conte B, Mahjoub Y, Desebbe O, Pottecher J, Lakhal K, Benzekri-Lefevre D, Molinari N, Boulain T, Lefrant JY, Muller L, AzuRea G. Clinical relevance of pulse pressure variations for predicting fluid responsiveness in mechanically ventilated intensive care unit patients: the grey zone approach. Crit Care. 2014;18:587.
Mahjoub Y, Lejeune V, Muller L, Perbet S, Zieleskiewicz L, Bart F, Veber B, Paugam-Burtz C, Jaber S, Ayham A, Zogheib E, Lasocki S, Vieillard-Baron A, Quintard H, Joannes-Boyau O, Plantefeve G, Montravers P, Duperret S, Lakhdari M, Ammenouche N, Lorne E, Slama M, Dupont H. Evaluation of pulse pressure variation validity criteria in critically ill patients: a prospective observational multicentre point-prevalence study. Br J Anaesth. 2014;112:681–5.
De Backer D, Heenen S, Piagnerelli M, Koch M, Vincent JL. Pulse pressure variations to predict fluid responsiveness: influence of tidal volume. Intensive Care Med. 2005;31:517–23.
Cannesson M, Le Manach Y, Hofer CK, Goarin JP, Lehot JJ, Vallet B, Tavernier B. Assessing the diagnostic accuracy of pulse pressure variations for the prediction of fluid responsiveness: a “gray zone” approach. Anesthesiology. 2011;115:231–41.
Futier E, Constantin JM, Paugam-Burtz C, Pascal J, Eurin M, Neuschwander A, Marret E, Beaussier M, Gutton C, Lefrant JY, Allaouchiche B. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Eng J Med. 2013;369(5):428–37.
Eikermann M, Kurth T. Apply protective mechanical ventilation in the operating room in an individualized approach to perioperative respiratory care. Anesthesiology. 2015;123:12–4.
Messina A, Pelaia C, Bruni A, Garofalo E, Bonicolini E, Longhini F, Dellara E, Saderi L, Romagnoli S, Sotgiu G, Cecconi M, Navalesi P. Fluid challenge during anesthesia: a systematic review and meta-analysis. Anesth Analg. 2018;127:1353–64.
Messina A, Sotgiu G, Saderi L, Cammarota G, Capuano L, Colombo D, Bennett V, Payen D, Navalesi P, Cecconi M. Does the definition of fluid responsiveness affect passive leg raising reliability? A methodological ancillary analysis from a multicentric study. Minerva Anestesiol. 2021;88(4):272–81.
Messina A, Palandri C, De Rosa S, Danzi V, Bonaldi E, Montagnini C, Baino S, Villa F, Sala F, Zito P, Negri K, Della Corte F, Cammarota G, Saderi L, Sotgiu G, Monge Garcia MI, Cecconi M. Pharmacodynamic analysis of a fluid challenge with 4 ml kg(− 1) over 10 or 20 min: a multicenter cross-over randomized clinical trial. J Clin Monit Comput. 2022;36:1193–203.
Barthelemy R, Kindermans M, Delval P, Collet M, Gaugain S, Cecconi M, Mebazaa A, Chousterman BG. Accuracy of cumulative volumes of fluid challenge to assess fluid responsiveness in critically ill patients with acute circulatory failure: a pharmacodynamic approach. Br J Anaesth. 2022;128:236–43.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. BMJ. 2009;339:b2535.
Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA, Bossuyt PM. Group Q–Quadas-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155:529–36.
Messina A, Dell’Anna A, Baggiani M, Torrini F, Maresca GM, Bennett V, Saderi L, Sotgiu G, Antonelli M, Cecconi M. Functional hemodynamic tests: a systematic review and a metanalysis on the reliability of the end-expiratory occlusion test and of the mini-fluid challenge in predicting fluid responsiveness. Crit Care. 2019;23:264.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–58.
de Courson H, Chauvet J, Le Gall L, Georges D, Boyer P, Verchere E, Nouette-Gaulain K, Biais M. Utility of changes in end-tidal carbon dioxide after volume expansion to assess fluid responsiveness in the operating room: a prospective observational study. Br J Anaesth. 2020;125:672–9.
Bubenek-Turconi SI, Hendy A, Baila S, Dragan A, Chioncel O, Valeanu L, Morosanu B, Iliescu VA. The value of a superior vena cava collapsibility index measured with a miniaturized transoesophageal monoplane continuous echocardiography probe to predict fluid responsiveness compared to stroke volume variations in open major vascular surgery: a prospective cohort study. J Clin Monit Comput. 2020;34:491–9.
Joosten A, Boudart C, Vincent JL, Vanden Eynden F, Barvais L, Van Obbergh L, Rinehart J, Desebbe O. Ability of a new smartphone pulse pressure variation and cardiac output application to predict fluid responsiveness in patients undergoing cardiac surgery. Anesth Analg. 2019;128:1145–51.
Biais M, de Courson H, Lanchon R, Pereira B, Bardonneau G, Griton M, Sesay M, Nouette-Gaulain K. Mini-fluid challenge of 100 ml of crystalloid predicts fluid responsiveness in the operating room. Anesthesiology. 2017;127:450–6.
Biais M, Lanchon R, Sesay M, Le Gall L, Pereira B, Futier E, Nouette-Gaulain K. Changes in stroke volume induced by lung recruitment maneuver predict fluid responsiveness in mechanically ventilated patients in the operating room. Anesthesiology. 2017;126:260–7.
Shen J, Dai S, Tao X, Chen X, Xu L. Corrected flow time and respirophasic variation in blood flow peak velocity of radial artery predict fluid responsiveness in gynecological surgical patients with mechanical ventilation. BMC Anesthesiol. 2022;22:299.
Nordstrom J, Hallsjo-Sander C, Shore R, Bjorne H. Stroke volume optimization in elective bowel surgery: a comparison between pulse power wave analysis (lidcorapid) and oesophageal doppler (cardioq). Br J Anaesth. 2013;110:374–80.
Messina A, Montagnini C, Cammarota G, De Rosa S, Giuliani F, Muratore L, Della Corte F, Navalesi P, Cecconi M. Tidal volume challenge to predict fluid responsiveness in the operating room: an observational study. Eur J Anaesthesiol. 2019;36:583–91.
Biais M, Larghi M, Henriot J, de Courson H, Sesay M, Nouette-Gaulain K. End-expiratory occlusion test predicts fluid responsiveness in patients with protective ventilation in the operating room. Anesth Analg. 2017;125:1889–95.
De Broca B, Garnier J, Fischer MO, Archange T, Marc J, Abou-Arab O, Dupont H, Lorne E, Guinot PG. Stroke volume changes induced by a recruitment maneuver predict fluid responsiveness in patients with protective ventilation in the operating theater. Medicine. 2016;95:e4259.
Kimura A, Suehiro K, Juri T, Tanaka K, Mori T. Changes in corrected carotid flow time induced by recruitment maneuver predict fluid responsiveness in patients undergoing general anesthesia. J Clin Monit Comput. 2022;36:1069–77.
Messina A, Lionetti G, Foti L, Bellotti E, Marcomini N, Cammarota G, Bennett V, Saderi L, Sotgiu G, Della Corte F, Protti A, Monge Garcia MI, Romagnoli S, Cecconi M. Mini fluid challenge and end-expiratory occlusion test to assess fluid responsiveness in the operating room (maneuver study): a multicentre cohort study. Eur J Anaesthesiol. 2021;38:422–31.
Weil G, Motamed C, Eghiaian A, Monnet X, Suria S. Comparison of proaqt/pulsioflex. Anaesth Crit Care Pain Med. 2019;38:153–9.
Weil G, Motamed C, Monnet X, Eghiaian A, Le Maho AL. End-expiratory occlusion test to predict fluid responsiveness is not suitable for laparotomic surgery. Anesth Analg. 2020;130:151–8.
Kimura A, Suehiro K, Juri T, Fujimoto Y, Yoshida H, Tanaka K, Mori T, Nishikawa K. Hemodynamic changes via the lung recruitment maneuver can predict fluid responsiveness in stroke volume and arterial pressure during one-lung ventilation. Anesth Analg. 2021;133:44–52.
Jun JH, Chung RK, Baik HJ, Chung MH, Hyeon JS, Lee YG, Park SH. The tidal volume challenge improves the reliability of dynamic preload indices during robot-assisted laparoscopic surgery in the trendelenburg position with lung-protective ventilation. BMC Anesthesiol. 2019;19:142.
Zlicar M, Novak-Jankovic V, Blagus R, Cecconi M. Predictive values of pulse pressure variation and stroke volume variation for fluid responsiveness in patients with pneumoperitoneum. J Clin Monit Comput. 2018;32:825–32.
Kim DH, Shin S, Kim JY, Kim SH, Jo M, Choi YS. Pulse pressure variation and pleth variability index as predictors of fluid responsiveness in patients undergoing spinal surgery in the prone position. Ther Clin Risk Manag. 2018;14:1175–83.
Lee CT, Lee TS, Chiu CT, Teng HC, Cheng HL, Wu CY. Mini-fluid challenge test predicts stroke volume and arterial pressure fluid responsiveness during spine surgery in prone position: a stard-compliant diagnostic accuracy study. Medicine. 2020;99:e19031.
Guinot PG, de Broca B, Bernard E, Abou Arab O, Lorne E, Dupont H. Respiratory stroke volume variation assessed by oesophageal doppler monitoring predicts fluid responsiveness during laparoscopy. Br J Anaesth. 2014;112:660–4.
Marik PE, Cavallazzi R, Vasu T, Hirani A. Dynamic changes in arterial waveform derived variables and fluid responsiveness in mechanically ventilated patients: a systematic review of the literature. Crit Care Med. 2009;37:2642–7.
Zhang Z, Lu B, Sheng X, Jin N. Accuracy of stroke volume variation in predicting fluid responsiveness: a systematic review and meta-analysis. J Anesth. 2011;25:904–16.
Zimmermann M, Feibicke T, Keyl C, Prasser C, Moritz S, Graf BM, Wiesenack C. Accuracy of stroke volume variation compared with pleth variability index to predict fluid responsiveness in mechanically ventilated patients undergoing major surgery. Eur J Anaesthesiol. 2010;27:555–61.
Aya HD, Ster IC, Fletcher N, Grounds RM, Rhodes A, Cecconi M. Pharmacodynamic analysis of a fluid challenge. Crit Care Med. 2016;44:880–91.
Messina A, Calabro L, Pugliese L, Lulja A, Sopuch A, Rosalba D, Morenghi E, Hernandez G, Monnet X, Cecconi M. Fluid challenge in critically ill patients receiving haemodynamic monitoring: a systematic review and comparison of two decades. Crit Care. 2022;26:186.
Hofer CK, Müller SM, Furrer L, Klaghofer R, Genoni M, Zollinger A. Stroke volume and pulse pressure variation for prediction of fluid responsiveness in patients undergoing off-pump coronary artery bypass grafting. Chest. 2005;128:848–54.
Preisman S, Kogan S, Berkenstadt H, Perel A. Predicting fluid responsiveness in patients undergoing cardiac surgery: functional haemodynamic parameters including the respiratory systolic variation test and static preload indicators. Br J Anaesth. 2005;95:746–55.
Cannesson M, Attof Y, Rosamel P, Desebbe O, Joseph P, Metton O, Bastien O, Lehot JJ. Respiratory variations in pulse oximetry plethysmographic waveform amplitude to predict fluid responsiveness in the operating room. Anesthesiology. 2007;106:1105–11.
Lee JH, Kim JT, Yoon SZ, Lim YJ, Jeon Y, Bahk JH, Kim CS. Evaluation of corrected flow time in oesophageal doppler as a predictor of fluid responsiveness. Br J Anaesth. 2007;99:343–8.
Cannesson M, Slieker J, Desebbe O, Bauer C, Chiari P, Henaine R, Lehot JJ. The ability of a novel algorithm for automatic estimation of the respiratory variations in arterial pulse pressure to monitor fluid responsiveness in the operating room. Anesthesia Analgesia. 2008;106:1195–200.
Messina A, Romano SM, Bonicolini E, Colombo D, Cammarota G, Chiostri M, Della Corte F, Navalesi P, Payen D, Romagnoli S. Cardiac cycle efficiency and dicrotic pressure variations: new parameters for fluid therapy: an observational study. Eur J Anaesthesiol. 2017;34:755–63.
Cannesson M, Desebbe O, Rosamel P, Delannoy B, Robin J, Bastien O, Lehot JJ. Pleth variability index to monitor the respiratory variations in the pulse oximeter plethysmographic waveform amplitude and predict fluid responsiveness in the operating theatre. Br J Anaesth. 2008;101:200–6.
Min JJ, Kim TK, Lee JH, Park J, Cho HS, Kim WS, Lee YT. Evaluation of augmented pulse pressure variation using the valsalva manoeuvre as a predictor of fluid responsiveness under open-chest conditions: a prospective observational study. Eur J Anaesthesiol. 2017;34:254–61.
Cannesson M, Musard H, Desebbe O, Boucau C, Simon R, Hénaine R, Lehot JJ. The ability of stroke volume variations obtained with vigileo/flotrac system to monitor fluid responsiveness in mechanically ventilated patients. Anesth Analg. 2009;108:513–7.
Jeong DM, Ahn HJ, Park HW, Yang M, Kim JA, Park J. Stroke volume variation and pulse pressure variation are not useful for predicting fluid responsiveness in thoracic surgery. Anesth Analg. 2017;125:1158–65.
Derichard A, Robin E, Tavernier B, Costecalde M, Fleyfel M, Onimus J, Lebuffe G, Chambon JP, Vallet B. Automated pulse pressure and stroke volume variations from radial artery: evaluation during major abdominal surgery. Br J Anaesth. 2009;103:678–84.
Min JJ, Lee JH, Hong KY, Choi SJ. Utility of stroke volume variation measured using non-invasive bioreactance as a predictor of fluid responsiveness in the prone position. J Clin Monit Comput. 2017;31:397–405.
de Waal EE, Rex S, Kruitwagen CL, Kalkman CJ, Buhre WF. Dynamic preload indicators fail to predict fluid responsiveness in open-chest conditions. Crit Care Med. 2009;37:510–5.
Biais M, Bernard O, Ha JC, Degryse C, Sztark F. Abilities of pulse pressure variations and stroke volume variations to predict fluid responsiveness in prone position during scoliosis surgery. Br J Anaesth. 2010;104:407–13.
Suehiro K, Okutani R. Stroke volume variation as a predictor of fluid responsiveness in patients undergoing one-lung ventilation. J Cardiothorac Vasc Anesth. 2010;24:772–5.
Lee JH, Jeon Y, Bahk JH, Gil NS, Hong DM, Kim JH, Kim HJ. Pulse pressure variation as a predictor of fluid responsiveness during one-lung ventilation for lung surgery using thoracotomy: randomised controlled study. Eur J Anaesthesiol. 2011;28:39–44.
Høiseth L, Hoff IE, Skare O, Kirkebøen KA, Landsverk SA. Photoplethysmographic and pulse pressure variations during abdominal surgery. Acta Anaesthesiol Scand. 2011;55:1221–30.
Biais M, Stecken L, Ottolenghi L, Roullet S, Quinart A, Masson F, Sztark F. The ability of pulse pressure variations obtained with cnap™ device to predict fluid responsiveness in the operating room. Anesth Analg. 2011;113:523–8.
Ali A, Abdullah T, Sabanci PA, Dogan L, Orhan-Sungur M, Akinci IO. Comparison of ability of pulse pressure variation to predict fluid responsiveness in prone and supine position: an observational study. J Clin Monit Comput. 2019;33:573–80.
Suehiro K, Okutani R. Influence of tidal volume for stroke volume variation to predict fluid responsiveness in patients undergoing one-lung ventilation. J Anesth. 2011;25:777–80.
Vistisen ST, Berg JM, Boekel MF, Modestini M, Bergman R, Jainandunsing JS, Mariani MA, Scheeren TWL. Using extra systoles and the micro-fluid challenge to predict fluid responsiveness during cardiac surgery. J Clin Monit Comput. 2019;33:777–86.
Høiseth L, Hoff IE, Myre K, Landsverk SA, Kirkebøen KA. Dynamic variables of fluid responsiveness during pneumoperitoneum and laparoscopic surgery. Acta Anaesthesiol Scand. 2012;56:777–86.
Ali A, Aygun E, Abdullah T, Bolsoy-Deveci S, Orhan-Sungur M, Canbaz M, Ozkan Akinci I. A challenge with 5 cmh2o of positive end-expiratory pressure predicts fluid responsiveness in neurosurgery patients with protective ventilation: an observational study. Minerva Anestesiol. 2019;85:1184–92.
Kim KM, Gwak MS, Choi SJ, Kim MH, Park MH, Heo BY. Pulse pressure variation and stroke volume variation to predict fluid responsiveness in patients undergoing carotid endarterectomy. Korean J Anesthesiol. 2013;65:237–43.
Ali A, Dorman Y, Abdullah T, Yasa C, Orhan-Sungur M, Akinci IO, Ergin-Ozcan P. Ability of mini-fluid challenge to predict fluid responsiveness in obese patients undergoing surgery in the prone position. Minerva Anestesiol. 2019;85:981–8.
Seo H, Kong YG, Jin SJ, Chin JH, Kim HY, Lee YK, Hwang JH, Kim YK. Dynamic arterial elastance in predicting arterial pressure increase after fluid challenge during robot-assisted laparoscopic prostatectomy: a prospective observational study. Medicine. 2015;94:e1794.
Berger K, Francony G, Bouzat P, Halle C, Genty C, Oddoux M, Gay E, Albaladejo P, Payen JF. Prone position affects stroke volume variation performance in predicting fluid responsiveness in neurosurgical patients. Minerva Anestesiol. 2015;81:628–35.
Watanabe R, Suehiro K, Mukai A, Tanaka K, Yamada T, Mori T, Nishikawa K. Changes in stroke volume induced by lung recruitment maneuver can predict fluid responsiveness during intraoperative lung-protective ventilation in prone position. BMC Anesthesiol. 2021;21:303.
Tusman G, Groisman I, Maidana GA, Scandurra A, Arca JM, Bohm SH, Suarez-Sipmann F. The sensitivity and specificity of pulmonary carbon dioxide elimination for noninvasive assessment of fluid responsiveness. Anesth Analg. 2016;122:1404–11.
Montenij LJ, Sonneveld JP, Nierich AP, Buhre WF, de Waal EE. Diagnostic accuracy of stroke volume variation measured with uncalibrated arterial waveform analysis for the prediction of fluid responsiveness in patients with impaired left ventricular function: a prospective, observational study. J Clin Monit Comput. 2016;30:481–6.
Flick M, Sand U, Bergholz A, Kouz K, Reiter B, Flotzinger D, Saugel B, Kubitz JC. Right ventricular and pulmonary artery pulse pressure variation and systolic pressure variation for the prediction of fluid responsiveness: an interventional study in coronary artery bypass surgery patients. J Clin Monit Comput. 2022;36:1817–25.
Acknowledgements
Not applicable.
Funding
This work was partially supported by “Ricerca Corrente” funding from Italian Ministry of Health to IRCCS Humanitas Research Hospital.
Author information
Authors and Affiliations
Contributions
AM and MCe conceived and designed the study; AM and EM performed the data analysis; MCa, LC, GL, DB, GMM and AB performed data extraction and helped in data analysis; LF, MA and MSC helped in drafting the article and revising it critically for important intellectual content. All the authors approved the final version to be published and agreed to be accountable for all aspects of the work thereby ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Prof. Michelle Chew is a Critical Care journal editor and received travel reimbursements and speaker fees from Edwards Lifesciences and from AOP Health. Dr. Messina received travel expenses and registration for meetings, congresses, and courses and lecture fees from Vygon, Phlips, Edwards; Prof. Cecconi is a consultant for Edwards Lifesciences.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Supplementray Tables and Figures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Messina, A., Caporale, M., Calabrò, L. et al. Reliability of pulse pressure and stroke volume variation in assessing fluid responsiveness in the operating room: a metanalysis and a metaregression. Crit Care 27, 431 (2023). https://doi.org/10.1186/s13054-023-04706-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-023-04706-0