
Abstract
Objective
In this study, we investigated the relationship between sarcopenia and fatty liver in middle-aged and elderly patients diagnosed with type 2 diabetes mellitus (T2DM) to provide a theoretical foundation for the prevention and treatment of sarcopenia.
Methods
A total of 282 patients diagnosed with T2DM aged 50 and older and were admitted to the Endocrinology Department of Xin Medical University First Affiliated Hospital between December 2021 and February 2023, were selected. Body mass index (BMI), and limb and trunk muscle mass of the patients were measured, and data were collected. Patients were grouped based on the sarcopenia diagnostic criteria. All study participants underwent the same physical examinations and laboratory tests. The relationship between the onset of sarcopenia and fatty liver in middle-aged and elderly patients diagnosed with T2DM was then investigated using statistical analysis.
Results
Comparing the sarcopenia group to the non-sarcopenia group revealed statistically significant variations in gender, BMI, fatty liver prevalence rate, uric acid (UA), alanine aminotransferase (ALT), blood glucose, blood lipid associated indicators, and limb skeletal muscle content. There were, however, no statistically significant differences in age, disease duration, hypertension, smoking, or alcohol intake. There was a positive correlation between BMI, UA, fasting c-peptide, and Appendicular Skeletal Muscle Index (ASMI). Higher levels of BMI, ASMI, and UA were identified as protective variables against sarcopenia by multifactorial logistic regression analysis.
Conclusion
Higher levels of BMI, ASMI, and UA can greatly reduce skeletal muscle atrophy in patients with T2DM. Patients with a fatty liver may be less vulnerable to sarcopenia. There is little evidence, however, that a fatty liver works as a preventive factor against sarcopenia.
Similar content being viewed by others

Introduction
Diabetes is a chronic systemic disease. Between 2013 and 2018, the prevalence of diagnosed diabetes among adults in China increased significantly [1]. Diabetes is widely assumed to be caused by a reduction in the insulin sensitivity of various tissues and organs throughout the body, or by a decrease in endogenous insulin secretion [2]. The number of patients with T2DM is growing annually, making it a global public health concern. Diabetes affects around 38.1% of the middle-aged and elderly population, according to research [3].
Prolonged hyperglycemia in diabetes often lead to an increased incidence of fatty liver disease [4]. Non-alcoholic fatty liver disease (NAFLD) is a form of metabolic liver disease that is closely linked to insulin resistance and genetics [5, 6]. In China, it has become the leading cause of increasingly severe chronic liver disease [7]. A meta-analysis of 1 832,125 patients identified the prevalence of Non-alcoholic fatty liver disease (NAFLD) in T2DM as 65.04%, respectively [8].
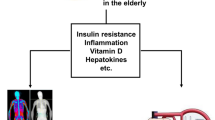
Insulin resistance in T2DM may exacerbate the condition of hyperglycemia, leading to a decrease in skeletal muscle mass and function, which is associated with sarcopenia, also known as muscle wasting [9]. Sarcopenia is a chronic metabolic disease characterized by a reduction in muscular strength and mass [10]. It is a disorder that progressively worsens and is frequently associated with other chronic diseases, such as T2DM, metabolic syndrome, cardiovascular disease, and other chronic conditions [11]. The prevalence of sarcopenia in the community ranged from 5.5 to 25.7% when using the AWGS2014 diagnostic criteria, with males having a higher prevalence than females. The prevalence of sarcopenia in Asia ranged from 7.3 to 12.0% [12]. Studies have revealed that muscle mass declines as glycated hemoglobin (HbA1c) levels rise, indicating a link between the beginning of sarcopenia and T2DM [13]. One study found that people with diabetes were 73% more likely to develop sarcopenia [14]. Additionally, patients with sarcopenia have an increased risk of developing osteoporosis [15]. Consequently, middle-aged people and the elderly with sarcopenia are more prone to falls and fractures, resulting in a significant reduction in their quality of life. Some may even become dependent on others for everyday activities, and sarcopenia becomes a major contributor to disability and mortality [16, 17].
There is currently no conclusive evidence indicating the link between sarcopenia and fatty liver in patients with diabetes. The purpose of this study is to examine the relationship between muscle wasting and fatty liver in middle-aged individuals and the elderly with T2DM, to provide a theoretical basis for the prevention and treatment of sarcopenia.
Research Content and Methods.
Study participants
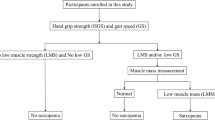
Participants in this study were all patients diagnosed with T2DM admitted to the Endocrinology Department of Xin Medical University First Affiliated Hospital between December 2021 and February 2023, aged 50 years or older. The participants were then divided into the sarcopenia group/case group and the non-sarcopenia group/control group based on the 2019 diagnostic criteria for muscle wasting developed by the Asian Working Group for Sarcopenia [12]. This study was approved by the local ethics (approval no. K202311021) committee on November 10th, 2021. All participants provided signed written informed consent.
Inclusion criteria
-
(1)
Aged 50 years and above, both males and females.
-
(2)
Meet the diagnostic criteria for diabetes published in 1999 by the World Health Organization (WHO) [15].
-
(3)
Participants free of mental diseases and competent to undertake the essential tasks of the study.
-
(4)
Those who comprehended the experiment and agreed to participate.
Exclusion Criteria
-
(1)
Below the age of 50 years.
-
(2)
Patients with Type 1 diabetes or other special types of diabetes.
-
(3)
Patients in the acute phase of any disease or with severe chronic organ failure.
-
(4)
Damage to the liver resulting from excessive alcohol intake, viral infections, drug-induced injuries, and autoimmune disorders.
-
(5)
Long-term and current use of drugs that change bone density, signs of bone metabolism, and internal hormone levels.
-
(6)
Patients suffering from degenerative diseases such as tuberculosis and malignant tumors.
Content and methods
Data collection
General data
Name, gender, age, ethnicity, diabetes disease duration, smoking history, alcohol consumption history, history of other chronic diseases (such as hypertension, coronary artery disease (CAD), and history of thyroid disease), family history, height, weight, and so on will be recorded for all study participants. All these details were meticulously recorded.
Laboratory examination
After fasting overnight for at least 8 h, blood samples were collected from all participants in the morning following their admission. Blood samples were collected by the nurses from the endocrinology department. Tests included fasting blood glucose (FBG), postprandial blood glucose (PBG), fasting c-peptide (FCP), HbA1c, alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatinine (Cr), uric acid (UA), albumin (Alb), triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), thyroid hormones, parathyroid hormone (PTH), and other bone metabolism indicators, including serum osteocalcin (BGP), 25-hydroxyvitamin D (25(OH)D), and parathyroid hormone (PTH).
Sarcopenia examination method
Participants were required to remove their shoes and socks before having their height measured. Participants were prohibited from carrying electronic devices. Next, the participants stood on predefined positions on the Biospace InBody720 or InBody770 body composition analyzer (InBody Co., Ltd., South Korea). Before administering the test, experienced nutritionists from the First Affiliated Hospital of Xinjiang Medical University collected the general information of the patients. During the test, participants remained still. The complete measurement process took roughly one minute. The completed results were then used to compute the Appendicular Skeletal Muscle Index (ASMI). The bioelectrical impedance analysis (BIA) method was applied to measure the appendicular skeletal mass (ASM) of the limbs and the whole body using the Biospace InBody720 Body Composition Analyzer or the InBody770 Body Composition Analyzer (InBody Co., Ltd.). The ASM was calculated as the sum of lean soft tissue from the arms and legs. ASMI was calculated as follows: ASMI = ASM/height2 (kg/m2) [18]. Based on the diagnostic criteria for sarcopenia, participants were subsequently categorized into the respective groups.
Fatty liver examination method
Participants underwent abdominal ultrasonography (Canon Medical Systems, Canon, Japan) or hepatic ultrasound examinations that were conducted by experienced specialists from the ultrasound department of the First Affiliated Hospital of Xin Medical University. The results were determined based on the diagnostic criteria for fatty liver [7, 8].
Diagnostic criteria
T2DM diagnostic criteria
All patients in this study were diagnosed with T2DM, i.e., they satisfied the WHO diagnostic criteria for diabetes established in 1999: possess typical diabetes symptoms of “three highs and one low” + random blood glucose level reaching or exceeding 11.1 mmol/L; fasting blood glucose reaching or exceeding 7.0 mmol/L; oral glucose tolerance test (OGTT) or 2-hour postprandial blood glucose measuring a blood glucose level that reaches or surpasses 11.1 mmol/L. For those patients without the typical “three highs and one low” symptoms or with only a single blood glucose measurement that reaches the diagnostic criteria, a re-check on a different day was required. The diagnosis was confirmed if the results were consistent with the criteria.
Sarcopenia diagnostic criteria
Using the Bays’ InBody body composition analyzer (InBody Co., Ltd.), the BMI and muscle mass in the limbs and trunk of the participants were measured. The ASMI was subsequently calculated as a diagnostic indicator. The value for the sarcopenia diagnostic criteria was based on the lowest quintile of this indicator for a healthy young population of the same ethnicity and gender. The diagnostic values for sarcopenia are: for males ≤ 7.0 kg/m2, and for females ≤ 5.7 kg/m2.
Fatty liver diagnostic criteria
The following were the diagnostic criteria for NAFLD [19] : (1) Enhanced diffuse echoes in the liver of the patient (i.e., “bright liver”), with these echoes being stronger than those from the kidney. (2) The anatomy and structures of the ducts in the liver are uncertain. (3) There is a diminishing tendency in the distant field for liver echoes. Diagnosis was confirmed if two of these criteria were met.
Statistical analysis
The SPSS software (version 27.0, IBM, USA) was used for data processing and analysis. The normality of the obtained metric data was first tested using the Kolmogorov-Smirnov test method. Measurement data that fit the normal distribution were represented by mean ± standard deviation, and the independent samples t-test was used for comparison between the two groups. Measurement data that did not fit the normal distribution were represented by median and interquartile range, with the Mann-Whitney U test used for intergroup comparison analysis. Count data were represented by frequency and percentage, with comparison made using the chi-squared test. Factors affecting sarcopenia were analyzed using the multifactorial logistic regression method. The correlation between age, disease duration, BMI, and relevant laboratory markers with the ASMI was compared using Pearson’s correlation analysis. A difference was considered statistically significant if P < 0.05.
Results
Comparison of demographic data between the two groups
There were a total of 282 participants in this study (166 males and 116 females). Based on the relevant examination results and diagnostic criteria, the participants were divided into two groups: the sarcopenia group with 61 participants, representing 21.6% of the total, and the non-sarcopenia group with 221 participants, representing 78.4% of the total. As shown in Table 1, there were substantial differences between the two groups in terms of BMI, gender, and the incidence of fatty liver. Other markers, including disease duration, incidence of hypertension, smoking history, and alcohol drinking history, revealed no significant differences.
Comparison of age, ASMI, and incidence of sarcopenia between patients diagnosed with T2DM with and without fatty liver
There were 176 patients diagnosed with T2DM with fatty liver and 106 without fatty liver. As indicated in Table 2, there were statistically significant differences in the two groups in terms of BMI and incidence of sarcopenia, but no significant differences in terms of ASMI and age.
Comparison of laboratory examination indicators between patients diagnosed with T2DM with and without sarcopenia
When comparing the relevant laboratory examination markers between patients diagnosed with T2DM having sarcopenia and those without, sarcopenia was associated with worse outcomes. According to Table 3, there were statistically significant differences in the levels of fasting c-peptide, TG, ALT, UA, and limb skeletal muscle content. Other than fasting c-peptide and TG, there were no statistically significant differences between the two groups in glucose metabolism, lipid metabolism, bone metabolism, AST, Cr, and albumin.
Correlation between ASMI and various factors in patients with T2DM
According to Table 4, a positive correlation exists between BMI, UA, fasting c-peptide, and ASMI. On the contrary, there was no discernible association between ASMI and age, disease duration, TG, or ALT.
Multifactorial logistic regression analysis
The presence of sarcopenia was the dependent variable in this experiment. Age, gender, BMI, ASMI, FCP, TG, ALT, UA, and the existence of fatty liver were considered as independent variables. The logistic regression analysis revealed that BMI and ASMI may act as protective factors against sarcopenia in patients diagnosed with T2DM (as seen in Table 5).
Discussion
Current state of diabetes and its complications in Middle-aged and elderly individuals
Diabetes, being a chronic disease that can affect the overall metabolic status of the body, can result in a range of macrovascular to microvascular complications if it is not addressed properly [20, 21]. Long-term failure to control blood glucose levels efficiently can result in a variety of issues. Some of these problems are even life-threatening [22].
A meta-analysis of 1 832,125 patients identified the prevalence of Non-alcoholic fatty liver disease (NAFLD) in T2DM as 65.04%, respectively [23]. The frequency of fatty liver in populations with normal blood glucose levels ranges between 20 and 30%. However, in patients diagnosed with T2DM, the prevalence of this condition may increase to 70–80% [24, 25]. In this study, roughly 62.4% of patients had NAFLD, which is consistent with other studies [24, 25]. Patients with fatty liver have greater blood glucose levels than those with a healthy liver [26]. A meta-analysis of 1,832,125 patients believed that the prevalence of NAFLD in T2DM was 65.04% [27].
Sarcopenia is a frequent complication in middle-aged and elderly patients diagnosed with T2DM. Approximately 4.1–11.5% of Asian middle-aged and elderly populations suffer from sarcopenia [28]. Patients diagnosed with sarcopenia undergo more rapid bone degeneration and are at a greater risk for osteoporosis than the general population. This increases the probability of falls and fractures, which has a substantial effect on daily life, and could result in debilitating conditions or even death in more extreme cases [16, 17]. Regarding treatment, no specific medications are currently available. Interventions for muscle atrophy primarily include resistance training, blood flow restrictive training, nutritional supplementation, and medication. Currently, resistance training is widely recognized as the most effective intervention for treating muscle atrophy or reducing its progression. Another major treatment approach for muscle atrophy is nutritional intervention, which involves supplementing with protein, vitamin D, leucine, etc., typically in conjunction with the aforementioned exercise training programs [29]. Currently, there are no specific medications approved for treating muscle atrophy [30]. Consequently, determining the origins and triggers of sarcopenia is crucial for its prevention and control.
Relationship between gender and sarcopenia
Due to the fundamental variances between male and female endocrine systems, there are also discrepancies in their metabolic rates. The results of this study imply that gender influences the onset of sarcopenia. Notably, the incidence of sarcopenia is substantially higher in men than in women. This disparity may be explained by the fact that males and females have different hormone levels. In addition, as people age, male and female hormonal swings diverge. Androgens, or male hormones, play a crucial function in muscle protein synthesis. Consequently, a fall in testosterone levels eventually results in a loss of muscle mass [31]. The pathogenesis of muscle atrophy may be related to factors such as aging, chronic inflammation, reduced hormone levels, mitochondrial dysfunction, nutritional deficiency, and lack of physical activity, leading to a decrease in motor neurons and satellite cell numbers, and muscle loss [32]. Some hormones, including testosterone, play a role in regulating protein synthesis and breakdown processes in muscles. Aging or other factors leading to a decline in hormone levels can result in reduced muscle synthesis metabolism, leading to loss of muscle mass and strength [33]. The impact of gender on the prevalence of muscle atrophy varies in research, with inconsistent results. A systematic review and meta-analysis suggest an overall prevalence of around 10% for community-dwelling elderly individuals with muscle atrophy, with rates of 11% for males and 9% for females. In hospitalized individuals, the rates are 23% for males and 24% for females, and in nursing homes, the rates are 51% for males and 31% for females [34]. Another study indicates a higher prevalence of muscle atrophy in non-Asian populations compared to Asian populations (males: 11% vs. 10%; females: 12% vs. 9%) [35]. Different diagnostic methods and equipment may account for the disparate results obtained by different investigations. Moreover, due to the dynamic nature of hormone levels within the human body, potential errors may occur.
This study did not identify gender as an independent risk factor for sarcopenia, which was similar to a study from Japan [36].
Association between glucose metabolism and sarcopenia
T2DM has a genetic susceptibility, with potentially thousands of genetic factors contributing to disease risk, interacting in complex ways with environmental factors [37]. The mechanisms by which glucolipotoxicity affects pancreatic function have been increasingly studied this year, indicating that the glucose toxicity mechanism in pancreatic β-cells is highly complex, involving multiple aspects and pathways. Currently, oxidative stress is considered to play a crucial role in the glucotoxicity of pancreatic cells in diabetes [38]. The roles of endoplasmic reticulum stress and the loss of pancreatic β-cell differentiation phenotype in the glucotoxicity of pancreatic β-cells are relatively clear [38, 39]. Reduced insulin sensitivity is the primary cause of T2DM. Based on contemporary research [40], skeletal muscle is the largest insulin target organ in the body. Consequently, diminished insulin sensitivity not only has substantial consequences for blood glucose homeostasis, but also has a considerable effect on skeletal muscles, a situation that may prompt the onset of sarcopenia. Insulin resistance can cause hyperglycemia and an increase in insulin levels throughout the body. In these conditions, the ability of muscle cells to produce proteins is impaired. T2DM can also cause disruptions or even anomalies in mitochondrial activity, hence increasing insulin resistance and speeding the evolution of sarcopenia. According to Stephen et al., patients without sarcopenia have lower HbA1c levels than those with sarcopenia based on blood glucose and skeletal muscle index assessment [41]. Currently, the pathophysiological mechanisms of diabetic myopathy remain a widely debated topic. Widely recognized possible causes include ischemia [42], impaired mitochondrial function [43], and inflammation [44], among other factors. Specific treatments are still focused on glycemic control [45]. Acupuncture support therapy lacks specific treatment methods, so prevention is emphasized [46]. Other potential contributing variables may include insulin secretion deficiencies, mitochondrial damage, systemic metabolic abnormalities, persistent inflammation, and other diabetes-related problems [47].
Associations between other metabolic indicators and sarcopenia
Blood lipids
The modulatory effects of fatty acids and their metabolic intermediates on skeletal muscle function are supported by recent studies. A study by Gong et al. included 84 patients aged 65 and above [48]. Blood lipid measurements, the SMI, and grip strength were assessed in the study. Patients with sarcopenia had significantly higher levels of TC, TG, LDL-C, and very low-density lipoprotein than the general population or the control group. Through Pearson’s correlation analysis, it was determined that an increase in blood lipid levels accompanied a decline in muscle strength, demonstrating a negative association between the two. Wang et al. investigated the skeletal muscle mass and blood lipid levels of 2,613 patients in another study [49]. In all, 13.85% of the patients were affected by sarcopenia. The results indicated a negative correlation between the onset of sarcopenia and TG and a favorable correlation with HDL-C. In addition, patients without sarcopenia had higher average blood lipid levels than those with sarcopenia.
UA
The relationship between UA and various diseases is complex due to the dual nature of UA, which includes both oxidative and antioxidant properties. Gout, renal disease, metabolic disorders, and obesity may be precipitated by elevated UA levels in the human body. Despite this, because of its antioxidant properties, UA is essential for maintaining normal physiological functions [50, 51]. Currently, there are few studies that have investigated the relationship between sarcopenia and UA, and their results are highly variable. Based on research conducted by Beaver et al., elevated UA may lead to the onset of sarcopenia [52]. Blood UA levels that are too high can induce systemic inflammatory reactions and increased oxidative stress, hence increasing the risk of sarcopenia.
Another study indicated a negative correlation between serum UA levels and sarcopenia, irrespective of gender [53]. In contrast, UA levels were positively correlated with skeletal muscle index and grip strength. This study revealed a significant correlation between elevated UA levels and enhanced muscle hypertrophy and grip strength. Potentially, elevated serum UA levels may delay the progression of sarcopenia. Although an excessively high UA level can lead to a variety of disorders, its vital function in everyday life cannot be neglected or denied. The incidence of sarcopenia is closely associated with UA. Whether blood UA functions as a risk factor or a protective factor for sarcopenia is yet unclear. Further research with bigger sample sizes are required to rule out other confounding variables and investigate this association in greater depth.
Association between fatty liver and sarcopenia
The risk of developing sarcopenia and fatty liver is increased by T2DM. Based on previous studies [54, 55] involving patients with normal blood glucose levels, individuals with sarcopenia are at a greater risk for developing fatty liver [56, 57]. The results of a meta-analysis that assessed 1,331 relevant publications and statistically analyzed 19 of them suggested that the muscle mass of fatty liver patients was lower than that of the control group, indicating an increased risk of fatty liver in this demographic [58]. The outcomes of this study indicate that sarcopenia is strongly negatively correlated with BMI in elderly patients diagnosed with T2DM. The non-sarcopenic group revealed a greater incidence of fatty liver as compared to the sarcopenic group. However, based on logistic regression analysis, fatty liver is neither a risk factor nor a protective factor for sarcopenia. The study by Sun et al. [59] found that higher levels of UA appear to have a protective effect against sarcopenia in male participants in a study on elderly patients with T2DM aged 65 and above. In our study, we did not separately analyze participants of different genders. Instead, gender was considered as one of the independent variables in the multifactorial analysis, along with factors such as age and fasting C-peptide levels. The analysis did not reveal a protective effect of UA against sarcopenia in the participants. The correlation between uric acid and sarcopenia in different gender groups needs further exploration. Additionally, similar to the mentioned study, our study also showed a protective effect of BMI against sarcopenia.
The strength of this article lies in the consideration of indicators affecting bone metabolism, such as parathyroid hormones, blood calcium levels, and 25-hydroxyvitamin D, when designing the study population. This enriched the exploration of potential factors linking sarcopenia and fatty liver in middle-aged and elderly patients with T2DM. The study suggests that higher levels of BMI and ASMI can reduce the occurrence of sarcopenia, providing more clues for understanding the potential correlation between fatty liver and sarcopenia. However, there are some limitations to this study. Firstly, the number of subjects included in the study is relatively small, and the proportion of sarcopenia among the subjects is low. Secondly, all enrolled patients in this study were hospitalized in the endocrinology department, raising the possibility of selection bias. Additionally, the diagnosis of fatty liver relied solely on liver ultrasound examination, without further assessments such as liver fibrosis evaluation or biopsy, thus requiring further validation of the conclusions.
Conclusion
In conclusion, our investigation into hospitalized patients within the endocrinology department, following rigorous screening, thorough testing, and careful exclusion of confounding variables, has yielded data-driven insights. Significant differences were observed in gender composition, BMI, and the incidence of fatty liver between sarcopenic and non-sarcopenic groups. Furthermore, marked variations in fasting c-peptide, TG, ALT, UA, and limb skeletal muscle content were identified when comparing the two groups. Our findings suggest a positive correlation between BMI, UA, fasting c-peptide, and ASMI levels. Moreover, through multivariate logistic regression analysis, we observed that higher BMI and ASMI serve as protective factors against sarcopenia. These findings may contribute valuable insights to the understanding of the relationships between various factors and sarcopenia.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
References
Wang L, Peng W, Zhao Z et al. Prevalence and Treatment of Diabetes in China, 2013–2018 [published correction appears in JAMA. 2022;327(11):1093]. JAMA. 2021;326(24):2498–2506. https://doi.org/10.1001/jama.2021.22208.
Rahman MS, Hossain KS, Das S, et al. Role of insulin in Health and Disease: an update. Int J Mol Sci. 2021;22(12):6403. https://doi.org/10.3390/ijms22126403. Published 2021 Jun 15.
Yang W, Lu J, Weng J, China National Diabetes and Metabolic Disorders Study Group, et al. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362(12):1090–101.
Bhatt HB, Smith RJ. Fatty liver disease in diabetes mellitus. Hepatobiliary Surg Nutr. 2015;4(2):101–8. https://doi.org/10.3978/j.issn.2304-3881.2015.01.03.
Abdelmalek MF. Nonalcoholic fatty liver disease: another leap forward. Nat Rev Gastroenterol Hepatol. 2021;18(2):85–6. https://doi.org/10.1038/s41575-020-00406-0. PMID: 33420415; PMCID: PMC7791336.
Maurice J, Manousou P. Non-alcoholic fatty liver disease. Clin Med (Lond). 2018;18(3):245–50. https://doi.org/10.7861/clinmedicine.18-3-245. PMID: 29858436; PMCID: PMC6334080.
Zhou J, Zhou F, Wang W, et al. Epidemiological features of NAFLD from 1999 to 2018 in China. Hepatology. 2020;71(5):1851–64. https://doi.org/10.1002/hep.31150.
Fatty Liver disease and alcoholic Liver Disease Group of The Liver Disease Society of the Chinese Medical Association. Guideline of prevention and treatment for nonalcoholic fatty liver disease:a 2018 update. J Mod Med Health. 2018;34(5):641–9.
Chen H, Huang X, Dong M, Wen S, Zhou L, Yuan X. The Association between Sarcopenia and Diabetes: from pathophysiology mechanism to therapeutic strategy. Diabetes Metab Syndr Obes. 2023;16:1541–54. https://doi.org/10.2147/DMSO.S410834. Published 2023 May 30.
Sarcopenia. Revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. https://doi.org/10.1093/ageing/afy169.
Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M, Writing Group for the European Working Group on Sarcopenia in Older People. 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. https://doi.org/10.1093/ageing/afy169. Erratum in: Age Ageing. 2019;48(4):601. PMID: 30312372; PMCID: PMC6322506.
Asian Working Group for Sarcopenia. 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J Am Med Dir Assoc. 2020;21(3):300–307.e2. doi: 10.1016/j.jamda.2019.12.012. Epub 2020 Feb 4.
Kalyani RR, Metter EJ, Egan J, Golden SH, Ferrucci L. Hyperglycemia predicts persistently lower muscle strength with aging. Diabetes Care. 2015;38(1):82–90. doi: 10.2337/dc14-1166. Epub 2014 Nov 12. PMID: 25392294; PMCID: PMC4274779.
Remelli F, Maietti E, Abete P, et al. Prevalence of obesity and diabetes in older people with Sarcopenia defined according to EWGSOP2 and FNHI criteria. Aging Clin Exp Res. 2022;34(1):113–20. https://doi.org/10.1007/s40520-021-01949-1.
Bischoff-Ferrari HA, Orav JE, Kanis JA, et al. Comparative performance of current definitions of Sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos Int. 2015;26:2793–802.
Gorial FI, Sayyid OS, Al Obaidi SA. Prevalence of Sarcopenia in sample of Iraqi patients with type 2 diabetes mellitus: a hospital based study. Diabetes Metab Syndr. 2020 Jul-Aug;14(4):413–6. Epub 2020 Apr 17. PMID: 32344368.
Balogun S, Winzenberg T, Wills K, Scott D, Jones G, Aitken D, Callisaya ML. Prospective Associations of Low Muscle Mass and Function with 10-Year Falls Risk, Incident Fracture and Mortality in Community-Dwelling Older Adults. J Nutr Health Aging. 2017;21(7):843–848. https://doi.org/10.1007/s12603-016-0843-6. PMID: 28717816.
Heymsfield SB, Smith R, Aulet M, Bensen B, Lichtman S, Wang J, et al. Appendicular skeletal muscle mass: measurement by dual-photon absorptiometry. Am J Clin Nutr. 1990;52:214–18. https://doi.org/10.1093/ajcn/52.2.214.
Hernaez R, Lazo M, Bonekamp S, et al. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology. 2011;54(3):1082–90. https://doi.org/10.1002/hep.24452.
Davies MJ, Aroda VR, Collins BS et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2022; 65:1925.
Hemmingsen B, Lund SS, Gluud C et al. Targeting intensive glycaemic control versus targeting conventional glycaemic control for type 2 diabetes mellitus. Cochrane Database Syst Rev 2013;:CD008143.
Deng R, Cai M. Value of combining serum cystatin C, HbA1c, hs-CRP and urine microvalbumin in the diagnosis of early renal impairment in patients with type 2 diabetes. Int J Lab Med. 2017;38(03):415–7.
Lee CH, Lui DT, Lam KS. Non-alcoholic fatty liver disease and type 2 diabetes: an update. J Diabetes Investig. 2022;13(6):930–40. https://doi.org/10.1111/jdi.13756.
Butt AS, Hamid S, Haider Z, Sharif F, Salih M, Awan S, Khan AA, Akhter J. Nonalcoholic fatty liver diseases among recently diagnosed patients with diabetes Mellitus and Risk factors. Euroasian J Hepatogastroenterol. 2019 Jan-Jun;9(1):9–13. https://doi.org/10.5005/jp-journals-10018-1288. PMID: 31988860; PMCID: PMC6969327.
Younossi ZM, Golabi P, de Avila L, Paik JM, Srishord M, Fukui N, Qiu Y, Burns L, Afendy A, Nader F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi: 10.1016/j.jhep.2019.06.021. Epub 2019 Jul 4. PMID: 31279902.
Wang B, Li M, Zhao Z, et al. Glycemic measures and development and resolution of nonalcoholic fatty liver disease in nondiabetic individuals. J Clin Endocrinol Metab. 2020;105(5):dgaa112. https://doi.org/10.1210/clinem/dgaa112.
Hu XY, Li Y, Li LQ et al. Risk factors and biomarkers of non-alcoholic fatty liver disease: an observational cross-sectional population survey. BMJ Open. 2018;8(4):e019974. Published 2018 Apr 5. https://doi.org/10.1136/bmjopen-2017-019974.
Moon SW, Lee SH, Woo A, Leem AY, Lee SH, Chung KS, Kim EY, Jung JY, Kang YA, Park MS, Kim YS, Kim CO, Kim SY. Reference values of skeletal muscle area for diagnosis of Sarcopenia using chest computed tomography in Asian general population. J Cachexia Sarcopenia Muscle. 2022;13(2):955–65. Epub 2022 Feb 15. PMID: 35170229; PMCID: PMC8978009.
Papadopoulou SK, Papadimitriou K, Voulgaridou G, et al. Exercise and nutrition impact on osteoporosis and sarcopeni - the incidence of osteosarcopenia: a narrative review. Nutrients. 2021;13(12):4499. 3390 / nu13124499.
Cruz-Jentoft AJ, Sayer AA, Sarcopenia. Lancet. 2019;393(10191):2636–46. 10. 1016 / S0140-6736(19)31138-9.
Dos Santos MR, Storer TW. Testosterone treatment as a function-promoting therapy in Sarcopenia Associated with Aging and Chronic Disease. Endocrinol Metab Clin North Am. 2022;51(1):187–204. Epub 2022 Feb 8. PMID: 35216716.
Cannataro R, Carbone L, Petro JL, et al. Sarcopenia: etiology, nutritional approaches, and miRNAs. Int J Mol Sci. 2021;22(18):9724.
Nishikawa H, Fukunishi S, Asai A, et al. Pathophysiology and mechanisms of primary sarcopenia (review). Int J Mol Med. 2021;48(2):156. https://doi.org/10.3892/ijmm.2021.4989.
Papadopoulou SK, Tsintavis P, Potsaki P et al. Differences in the prevalence of sarcopenia in community-dwelling, nursing home and hospitalized individuals. A systematic review and Meta-analysis. J Nutr Health Aging, 2020, 24(1): 83–90. DOI: 10. 1007/ s12603-019-1267-x.
Shafiee G, Keshtkar A, Soltani A, et al. Prevalence of Sarcopenia in the world: a systematic review and meta-analysis of general population studies. J Diabetes Metab Disord. 2017;16:21. 1186 / s40200-017-0302-x.
Su Y, Hirayama K, Han TF, Izutsu M, Yuki M. Sarcopenia Prevalence and Risk factors among Japanese Community Dwelling older adults living in a Snow-Covered City according to EWGSOP2. J Clin Med. 2019;8(3):291. https://doi.org/10.3390/jcm8030291. Published 2019 Feb 28.
Klein BE, Klein R, Moss SE, Cruickshanks KJ. Parental history of diabetes in a population-based study. Diabetes Care. 1996;19:827.
Bensellam M, LaybuttDR. JonasJC. Themolecular mechanismsofpancreatic B-cellglucotoxicity:recent findings and future research directions. MolCell Endocrinol. 2012;364(1–2):1–27.
Kim MK, Kim HS, LeeIK et al. Endoplasmicreticulum stress andinsulinbiosynthesis:areview. ExpDiabetesRes,2012, 2012:509437.
Merz KE, Thurmond DC. Role of skeletal muscle in insulin resistance and glucose uptake. Compr Physiol. 2020;10(3):785–809.
Cleasby ME, Jamieson PM, Atherton PJ. Insulin resistance and sarcopenia: mechanistic links between common co-morbidities. J Endocrinol. 2016;229(2):R67-81. https://doi.org/10.1530/JOE-15-0533. Epub 2016 Mar 1. PMID: 26931135.
Bell DSH. Diabetic mononeuropathies and Diabetic Amyotrophy. Diabetes Ther. 2022;13(10):1715–22. https://doi.org/10.1007/s13300-022-01308-x.
Vezza T, DíazPozo P, Canet F, et al. The role of mitochondrial dynamic dysfunction in age-associated type 2 diabetes. World J Men’s Health. 2022;40(3):399–411.
Na JSD, Dittmar PC. Diabetic amyotrophy, not your typical back pain. BMJ Case Rep. 2020;13(1):e231928. https://doi.org/10.1136/bcr-2019-231928. Published 2020 Jan 9.
Shimizu Y, Kozawa J, Hayakawa T, et al. Asymptomatic Pontine Lesion and Diabetic Amyotrophy after Rapid Improvement of Poor Glycemic Control in a patient with type 1 diabetes. Intern Med. 2019;58(23):3433–9. https://doi.org/10.2169/internalmedicine.2835-19.
Long B, Koyfman A, Gottlieb M. Evaluation and management of cauda equina syndrome in the emergency department. Am J Emerg Med. 2020;38(1):143–8. https://doi.org/10.1016/j.ajem.2019.158402.
Alqallaf A, Swan P, Docherty NG. Renal insulin resistance in type 2 diabetes mellitus and progression of chronic kidney disease: potential pathogenic mechanisms. Expert Rev Endocrinol Metab. 2022;17(6):523–32. Epub 2022 Oct 6. PMID: 36203374.
Gong H, Liu Y, Lyu X, Dong L, Zhang X. Lipoprotein subfractions in patients with Sarcopenia and their relevance to skeletal muscle mass and function. Exp Gerontol. 2022;159:111668. https://doi.org/10.1016/j.exger.2021.111668. Epub 2021 Dec 23. PMID: 34954281.
Wang N, Chen M, Fang D. Relationship between serum triglyceride to high-density lipoprotein cholesterol ratio and sarcopenia occurrence rate in community-dwelling Chinese adults. Lipids Health Dis. 2020;19(1):248. https://doi.org/10.1186/s12944-020-01422-4. PMID: 33276798; PMCID: PMC7716486.
AHMADS PARVEENN et al. Attenuation of hg(II)-induced cellular and DNA damage in human blood cells byuric acid.BiochemCellBiol, 2022,100(1):45–58.
WANG M H, WU J M,JIAO H, C et al. Enterocyte synthesizes and secret suric acid as antioxidant to protect against oxidative stress via the involvement of Nrfpathway.Free RadicBiolMed,2022,179:95–108.
Beavers KM, Beavers DP, Serra MC, Bowden RG, Wilson RL. Low relative skeletal muscle mass indicative of sarcopenia is associated with elevations in serum uric acid levels: findings from NHANES III. J Nutr Health Aging. 2009;13(3):177 – 82. https://doi.org/10.1007/s12603-009-0054-5. PMID: 19262948.
Liu X, Chen X, Hu F, Xia X, Hou L, Zhang G, Peng X, Sun X, Luo S, Yue J, Dong B. Higher uric acid serum levels are associated with Sarcopenia in West China: a cross-sectional study. BMC Geriatr. 2022;22(1):121. https://doi.org/10.1186/s12877-022-02817-x. PMID: 35151263; PMCID: PMC8841067.
Lee YH, Kim SU, Song K, Park JY, Kim DY, Ahn SH, Lee BW, Kang ES, Cha BS. Han K.H. Sarcopenia is associated with significant liver fibrosis independently of obesity and insulin resistance in nonalcoholic fatty liver disease: nationwide surveys (KNHANES 2008–2011). Hepatology. 2016;63:776–86. https://doi.org/10.1002/hep.28376.
Hong HC, Hwang SY, Choi HY, Yoo HJ, Seo JA, Kim SG, Kim NH, Baik SH, Choi DS, Choi KM. Relationship between Sarcopenia and nonalcoholic fatty liver disease: the Korean sarcopenic obesity study. Hepatology. 2014;59:1772–8. https://doi.org/10.1002/hep.26716.
Zhao X, Shi X, Gu H, Zhou W, Zhang Q. Association between handgrip strength, nonalcoholic fatty liver disease, advanced hepatic fibrosis and its modifiers: Evidence from the NHANES database of the USA. J Gastroenterol Hepatol. 2023 Feb 18. https://doi.org/10.1111/jgh.16150. Epub ahead of print. PMID: 36805682.
Zhong DY, Li L, Li HJ, Ma RM, Deng YH. Study on the mechanism and molecular docking verification of buyang huanwu decoction in treating diabetic foot. World J Tradit Chin Med. 2023;9:178–90.
Cai C, Song X, Chen Y, Chen X, Yu C. Relationship between relative skeletal muscle mass and nonalcoholic fatty liver disease: a systematic review and meta-analysis. Hepatol Int. 2020;14(1):115–26. https://doi.org/10.1007/s12072-019-09964-1. Epub 2019 Jul 9. PMID: 31290072; PMCID: PMC6994447.
Sun L, Fu J, Mu Z, Duan X, Chan P, Xiu S. Association between body fat and sarcopenia in older adults with type 2 diabetes mellitus: a cross-sectional study. Front Endocrinol (Lausanne). 2023;14:1094075. https://doi.org/10.3389/fendo.2023.1094075. Published 2023 Jan 27.
Acknowledgements
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia Fund: SKL-HIDCA-2020-45.
Author information
Authors and Affiliations
Contributions
Conception and design of the research: Li Quan, Yong Fan. Acquisition of data: Fang Zhang, Li Quan, Fei Wang, Jing Xu. Analysis and interpretation of the data: Fang Zhang, Li Quan, Fei Wang. Statistical analysis: Fang Zhang, Jing XuObtaining financing: Li Quan. Writing of the manuscript: Fang Zhang, Li Quan. Critical revision of the manuscript for intellectual content: Yong Fan. All authors read and approved the final draft.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted with approval from the Ethics Committee of The first Affiliated Hospital of Xinjiang Medical University. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Li Quan and Fang Zhang contributed equally to this study.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Quan, L., Zhang, F., Xu, J. et al. Relationship between sarcopenia and fatty liver in middle-aged and elderly patients with type 2 diabetes mellitus. J Orthop Surg Res 19, 250 (2024). https://doi.org/10.1186/s13018-024-04717-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-024-04717-9