
Abstract
Background
While dyslipidemia has been recognized as a potential risk factor for hyperuricemia, there is currently a dearth of large-scale data specifically focused on studying the relationship between these two conditions. To address this gap, the present study analyzed a dataset of 298,891 physical examination records to investigate in greater detail the clinical classification and compositional relationship between hyperuricemia and dyslipidemia.
Methods
For this investigation, a cross-sectional research design was utilized to analyze physical examination data that was gathered from Yijishan Hospital in Wuhu, China between 2011 and 2016. Logistic regression was employed to examine the association between hyperuricemia and dyslipidemia. Furthermore, the association between hyperuricemia and dyslipidemia was evaluated based on the clinical classifications of dyslipidemia and its components.
Results
A total of 298,891 participants from China (124,886 [41.8%] females) were included in the study, with an age range of 18 to 90 years (mean [SD]: 47.76 [13.54] years). In multivariate analysis, the odds of hyperuricemia was 1.878 times higher in patients with dyslipidemia compared to those without dyslipidemia (95% confidence interval [CI]: 1.835–1.922). In the clinical classification of dyslipidemia, individuals with hypertriglyceridemia and mixed hyperlipidemia had 1.753 times (95% CI: 1.706–1.802) and 1.925 times (95% CI: 1.870–1.982) higher odds of hyperuricemia, respectively, compared to those without dyslipidemia. Among the components of dyslipidemia, the odds ratios for hyperuricemia in individuals in the fourth quartile compared to those in the first quartile were 3.744 (95% CI: 3.636–3.918) for triglycerides, 1.518 (95% CI: 1.471–1.565) for total cholesterol, and 1.775 (95% CI: 1.718 − 1.833) for non-high-density lipoprotein cholesterol.
Conclusions
Dyslipidemia has been independently linked with hyperuricemia. Moreover, the elevation of triglycerides or total cholesterol levels, including conditions such as hypertriglyceridemia and mixed hyperlipidemia, have been observed to have a positive association with the development of hyperuricemia.
Similar content being viewed by others


Introduction
Hyperuricemia is a common metabolic disorder [1] caused by excessive uric acid production from factors such as a purine-rich diet, alcohol consumption, obesity, or reduced uric acid excretion due to conditions such as renal insufficiency, diabetes, and hypertension, among others [2, 3]. The resultant increase in blood uric acid levels exceeds the normal range of the human body. In recent decades, the incidence of hyperuricemia has increased rapidly worldwide [4]. This not only adversely affects individual health [5] but also places a significant burden on medical systems globally [6].
Numerous epidemiological studies have demonstrated that unhealthy lifestyle habits, such as smoking and drinking, can increase the risk of hyperuricemia [7, 8]. Additionally, hyperuricemia has been associated with various diseases, such as dyslipidemia, obesity, hypertension, and diabetes [9,10,11,12]. Among these, dyslipidemia is a common disorder of lipoprotein metabolism in humans [13], and its main components include total cholesterol(TC), triglyceride(TG), high-density lipoprotein cholesterol(HDL-C), and low-density lipoprotein cholesterol(LDL-C) [14].
There exists ample evidence indicating a significant association between dyslipidemia and an increased risk of hyperuricemia [15]. However, the association between components of dyslipidemia and hyperuricemia remains controversial. Cross-sectional studies have found a positive association between hyperuricemia and elevated levels of TG, TC, and LDL-C, and a negative association with decreased levels of HDL-C [16,17,18]. At the same time, we found that few studies have examined the relationship between dyslipidemia and hyperuricemia from the perspective of clinical classification of dyslipidemia. From a physiological and metabolic standpoint, dyslipidemia might escalate the risk of hyperuricemia by triggering or intensifying processes such as insulin resistance, inflammatory responses, and purine metabolic disturbances [19, 20]. There could be an interplay and mutual influence among these processes, forming a complex network that collectively propels the concurrent onset and progression of dyslipidemia and hyperuricemia. Therefore, we explored the relationship between hyperuricemia and dyslipidemia from two different perspectives of clinical types and components through a large amount of data.
Materials and methods
Study population
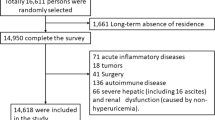
A cross-sectional study was conducted on the physical examination data of participants aged 18 to 90 from 2011 to 2016. Data provided by the First Affiliated Hospital of Wannan Medical College, Wuhu, China. In this study, subjects had to be at least 18 years of age and had no prior medical intervention for hyperuricemia. At the same time, complete data measurement and subject consent can be obtained. A total of 434,847 people participated. According to these criteria, the final physical examination data of 298,891 participants (174,005 men and 124,886 women) were included in this study.
Anthropometric and laboratory measurements
We used questionnaires to record basic anthropometric data such as age, sex, smoking, and drinking habits. Subjects were wearing light clothing and no shoes. The height measurement accuracy is 0.1 cm, and the weight measurement accuracy is 0.1 kg. Body Mass Index (BMI) is accurate to 0.01 kg/m2. We measured systolic and diastolic blood pressure using a benchtop mercury sphygmomanometer.
Venous blood was drawn from subjects in the morning on an empty stomach, and all samples were analyzed within 24 hours. Serum uric acid (SUA), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) were detected by an automatic biochemical analyzer. In addition to these measurements, non-high-density lipoprotein (non-HDL) cholesterol was calculated as the difference between TC and HDL-C.
Fasting blood glucose (FBG), alanine aminotransferase (ALT), aspartate aminotransferase (AST), blood urea nitrogen (BUN), and serum creatinine (SCR) were also measured using the same instrument. All measurements were taken by a professional doctor and checked again to confirm the accuracy of the results.
Diagnostic criteria
Hyperuricemia was defined as SUA > 420 mmol/L (male) or SUA > 360 mmol/L (female) [21, 22], which is a widely accepted diagnostic criterion. Subjects are considered to have dyslipidemia if they meet one of the following criteria at the time of examination: TC ≥ 5.2 mmol/L, TG ≥ 1.7 mmol/L, HDL-C < 1.0 mmol/L, LDL-C ≥ 3.4 mmol/L [23]. According to the clinical classification criteria [24, 25], dyslipidemia can be divided into the following four main categories: hypercholesterolemia, elevated TC level; hypertriglyceridemia, elevated TG level; mixed hyperlipidemia, TC, TG levels increased; low high-density lipoprotein cholesterol (HDL) dyslipidemia, decreased level of HDL-C.
Diabetes was defined as FBG ≥ 7.0 mmol/L [26]. Hypertension was defined as having a systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg, or currently being on treatment for hypertension [27]. According to the Chinese body mass index classification standard (WS/T 428–2013), obesity is defined as BMI ≥ 28 kg/m2.
Ethics statement
This study was approved by the Ethics Committee of Wannan Medical College. Since the subjects in this study came from people who underwent routine physical examination, only the oral and informed consent of the subjects was required with the approval of the ethics committee. Before the investigation, an oral informed consent form was provided to each subject.
Statistical analysis
All data were analyzed using IBM SPSS Statistics Version 26. Categorical variables were presented as percentages and continuous variables as mean ± standard deviation. The chi-square test and t-test were employed to compare the differences between the hyperuricemia and normal groups. Binary logistic regression analysis was conducted to examine the association between the studied parameters and hyperuricemia. In the multivariate analysis, stepwise regression was utilized to filter and adjust for covariates. To investigate the relationship between dyslipidemia parameters and hyperuricemia in detail, hyperuricemia was used as the dependent variable, while the composition and clinical type of dyslipidemia were considered independent variables. Data were tested using an asymptotic model. Model 1 was unadjusted, Model 2 was adjusted for age and sex, and Model 3 was adjusted for age, sex, smoking, drinking, obesity, hypertension, diabetes, and ALT, AST, BUN, and SCR (fully adjusted model). Results were considered significant at a p-value < 0.05.
Results
The baseline characteristics of study participants according to hyperuricemia are in Table 1. All subjects were divided into two groups. Compared with people with normal uric acid levels, the individuals in the hyperuricemia group were 5.1% higher for mean age, 9.1% higher for BMI, 6.3% higher for SBP, 5.2% higher for DBP, 5.0% higher for TC and 51.7% higher for TG. In line with these results, the rate of dyslipidemia was 52.2% higher, the rate of diabetes was 162% higher, the rate of hypertension was 77.6% higher and the rate of diabetes was 18.7% higher.
Parameters associated with hyperuricemia in the binary logistic analysis of all study participants are in Table 2. In multivariate analysis, we found that dyslipidemia (OR, 1.878; 95% CI, 1.835–1.922), obesity (OR, 1.956; 95% CI, 1.898–2.015), and hypertension (OR, 1.368; 95% CI, 1.334–1.404) were independently and positively associated with hyperuricemia.
As detailed in Table 3, in the fully adjusted model, individuals in the fourth quartile of TG (OR, 3.774; 95% CI, 3.636–3.916), TC (OR, 1.518; 95% CI, 1.471–1.565), and non-HDL (OR, 1.775; 95% CI, 1.718 − 1.833) were more likely to have hyperuricemia than those in the first quartile. Conversely, higher quartiles of HDL-C (OR, 0.676; 95% CI, 0.653-0.700) and LDL-C (OR, 0.896; 95% CI, 0.870–0.923) were associated with a lower likelihood of hyperuricemia.
The association between hyperuricemia and dyslipidemia in different clinical categories is in Table 4. In the fully adjusted model, we found significant associations between hyperuricemia and both hypertriglyceridemia (OR, 1.753; 95% CI, 1.706–1.802) and mixed hyperlipidemia (OR, 1.925; 95% CI, 1.870–1.982) in the clinical classification of dyslipidemia.
Discussion
To our knowledge, this is the most extensive cross-sectional study to date examining the relationship between hyperuricemia and various dyslipidemias. We have identified a significant correlation between dyslipidemia and hyperuricemia, particularly with hypertriglyceridemia and mixed hyperlipidemia. Elevated levels of TG and TC are significantly associated with an increased likelihood of hyperuricemia. Additionally, our analysis included non-high-density lipoprotein cholesterol, providing a more comprehensive evaluation of the dyslipidemic profiles associated with hyperuricemia.
Our results suggest that in addition to dyslipidemia, obesity, hypertension, and alcohol consumption are also significantly associated with hyperuricemia. These findings align well with observations from both cross-sectional analyses and prospective cohort studies [28,29,30,31]. Our finding that smoking and diabetes are associated with lower odds of hyperuricemia may contradict common sense. Upon examining the relevant data, we found some studies showed an inverse association between smoking and hyperuricemia, but only in women [32]. This may be because smoking causes oxidative stress, which leads to a drop in uric acid levels [33]. At the same time, the data showed that men with diabetes were less likely to develop hyperuricemia [34]. However, due to the limitations of the research method, we could not draw more specific conclusions. In addition, indicators of liver function (ALT, AST) and renal function (BUN, SCR) were positively associated with an increased likelihood of hyperuricemia [35, 36]. This may be due to food intake and the production of purine compounds, which the body breaks down in the liver, uric acid, which makes up the majority of it, is excreted through the kidneys. Elevation of these indicators indicates that the liver and kidney function of the human body is damaged, and the human body cannot decompose or excrete uric acid normally, resulting in blood uric acid in the human body exceeding the normal value [37].
A considerable body of cross-sectional epidemiological evidence indicates a significant positive association between the likelihood of hyperuricemia and levels of TG and TC, but a negative association with levels of HDL-C [15, 18, 38]. Our research also confirms this point, highlighting a noteworthy relationship where higher levels of TG are often accompanied by lower levels of HDL-C. This inverse association is in line with the established understanding that dyslipidemic profiles characterized by high TG typically present with reduced HDL-C, an indicator of altered lipid metabolism that is frequently observed in metabolic disorders. In recognizing the multifaceted nature of lipid profiles, we note the complexity in the association with total cholesterol, which is composed of HDL-C, LDL-C, and the cholesterol carried by TG in very low-density lipoprotein(VLDL). Although our current study did not delve into the intricacies of this relationship, it is an important aspect for future investigations to explore, particularly in relation to hyperuricemia. At the same time, we also found that TG is more related than other lipid components, which is consistent with the results of Hou et al. [9, 39]. Furthermore, a multicentric longitudinal study also observed that hypertriglyceridemia and low HDL-C concentrations are associated with elevated serum uric acid concentrations, further strengthening the links established in our study [20]. However, the specific mechanism of TG level and hyperuricemia has not been elucidated. Some studies have suggested that triglycerides can cause metabolic disorders of free fatty acids, accelerate the decomposition of adenosine triphosphate and lead to the increase of uric acid [9, 40]. Corroborating this, the prospective cohort study conducted by Chien and colleagues indicates an association between uric acid production and purine metabolism within the biosynthesis pathway of triglycerides [19]. Delving deeper into the mechanistic aspect, dyslipidemia can instigate the overactivity of xanthine oxidoreductase (XOR), a crucial enzyme in purine metabolism. This not only escalates the production of uric acid and reactive oxygen species (ROS), but also triggers oxidative stress. This oxidative stress could intensify the dyslipidemia, exacerbate insulin resistance, and set off a chain of metabolic changes within the body [31, 41]. Concurrently, dyslipidemia could also stimulate an inflammatory response, potentially triggering hyperuricemia, thereby providing a possible explanation for the relationship between lipid profile and uric acid levels [42].
Contrary to popular belief, our research suggests that LDL-C is inversely associated with hyperuricemia [15]. A potential explanation for this counterintuitive relationship could lie in the immunomodulatory functions of LDL-C. Studies have indicated that LDL-C may play a role in immune responses by binding to and neutralizing pathogens and toxins, which in turn could help alleviate the inflammatory responses frequently triggered by hyperuricemia [19, 20, 30]. Moreover, in our comprehensive analysis of non-HDL cholesterol, which encompasses LDL-C and VLDL-C, we observed significant associations with hyperuricemia across increasing quartiles, indicating a potential correlation between elevated non-HDL cholesterol levels and the risk of hyperuricemia [43]. While LDL-C shows a weaker inverse association with hyperuricemia compared to HDL-C, non-HDL cholesterol as a broader category might still provide additional insights into the relationship between dyslipidemia and hyperuricemia, and it should be considered in the clinical assessment of cardiovascular risk.
Most of the previous studies only focused on the relationship between dyslipidemia as a whole or individual indicator and hyperuricemia, but in this study, we found the association between different lipid diseases and hyperuricemia according to the clinical classification of dyslipidemia [24, 44]. According to the results of the study, we found that people with hypertriglyceridemia and mixed hyperlipidemia were more likely to suffer from hyperuricemia. However, people with hypercholesterolemia and low HDL-C are less likely than normal people to develop hyperuricemia. Therefore, doctors should always pay attention to the clinical risk of hyperuricemia in the first group of people.
It is worth noting that the current study has several limitations. First, this study was a cross-sectional study, and we could not determine a causal relationship between hyperuricemia and dyslipidemia. Furthermore, we lack data on factors such as diet and lifestyle that are known to have an impact on the incidence of hyperuricemia. At the same time, we also lack detailed information on uric acid or lipid-lowering drugs that might affect our results. Finally, the relationship between hyperuricemia and dyslipidemia is very complex, and further analysis is needed to more clearly explain the mechanism of influence between the two.
Conclusion
Hyperuricemia has been shown to have an independent association with dyslipidemia. Furthermore, increased levels of triglycerides or total cholesterol, which are present in conditions like hypertriglyceridemia and mixed hyperlipidemia, are positively correlated with the onset of hyperuricemia.
Data Availability
The data of participants are collected by the authors and uploaded to the database, which makes it easier for the authors to use the data in the process of analyzing data and writing manuscripts. This kind of database system can conveniently shield the data irrelevant to the experiment and effectively protect the privacy of participants. The data that support the findings of this study are available from the Health Management Center at the First Affiliated Hospital of Wannan Medical College in Wuhu, China but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the Health Management Center at the First Affiliated Hospital of Wannan Medical College in Wuhu, China. If someone wants to request the data from this study, they can contact Yufeng Wen (corresponding author).
Abbreviations
- SUA:
-
serum uric acid
- BMI:
-
body mass index
- FBG:
-
fasting blood glucose
- SBP:
-
systolic blood pressure
- DBP:
-
diastolic blood pressure
- TC:
-
total cholesterol
- TG:
-
triglycerides
- HDL-C:
-
high-density lipoprotein cholesterol
- LDL-C:
-
low-density lipoprotein cholesterol
- VLDL:
-
very low-density lipoprotein
- non-HDL:
-
non-high-density lipoprotein
- ALT:
-
alanine transaminase
- AST:
-
aspartate transaminase
- BUN:
-
blood urea nitrogen
- SCR:
-
serum creatinine
References
Zhang Y, Yu H, Chai S, Chai X, Wang L, Geng WC, Li JJ, Yue YX, Guo DS, Wang Y. Noninvasive and individual-centered monitoring of uric acid for precaution of Hyperuricemia via Optical Supramolecular Sensing. Adv Sci (Weinh). 2022;9:e2104463.
Kim SC, Neogi T, Kang EH, Liu J, Desai RJ, Zhang M, Solomon DH. Cardiovascular risks of Probenecid Versus Allopurinol in older patients with gout. J Am Coll Cardiol. 2018;71:994–1004.
Mandal AK, Mount DB. The molecular physiology of uric acid homeostasis. Annu Rev Physiol. 2015;77:323–45.
Kim Y, Choi JH, Kang J, Kim GT, Lee SG. Associations of serum retinol and alpha-tocopherol levels with uric acid concentrations: analysis of a Population-Based, nationally Representative Sample. Nutrients 2020, 12.
Song J, Jin C, Shan Z, Teng W, Li J. Prevalence and risk factors of Hyperuricemia and gout: a cross-sectional survey from 31 provinces in Mainland China. J Transl Int Med. 2022;10:134–45.
Otaki Y, Konta T, Ichikawa K, Fujimoto S, Iseki K, Moriyama T, Yamagata K, Tsuruya K, Narita I, Kondo M, et al. Possible burden of hyperuricaemia on mortality in a community-based population: a large-scale cohort study. Sci Rep. 2021;11:8999.
Nakanishi N, Yoshida H, Nakamura K, Suzuki K, Tatara K. Predictors for development of hyperuricemia: an 8-year longitudinal study in middle-aged Japanese men. Metabolism. 2001;50:621–6.
Gee Teng G, Pan A, Yuan JM, Koh WP. Cigarette Smoking and the risk of incident gout in a prospective cohort study. Arthritis Care Res (Hoboken). 2016;68:1135–42.
Hou YL, Yang XL, Wang CX, Zhi LX, Yang MJ, You CG. Hypertriglyceridemia and hyperuricemia: a retrospective study of urban residents. Lipids Health Dis. 2019;18:81.
Forman JP, Choi H, Curhan GC. Plasma uric acid level and risk for incident Hypertension among men. J Am Soc Nephrol. 2007;18:287–92.
Li LX, Dong XH, Li MF, Zhang R, Li TT, Shen J, Shen J, Bao YQ, Jia WP. Serum uric acid levels are associated with Hypertension and metabolic syndrome but not Atherosclerosis in Chinese inpatients with type 2 Diabetes. J Hypertens. 2015;33:482–90. discussion 490.
Yang C, Yang S, Feng C, Zhang C, Xu W, Zhang L, Yan Y, Deng J, Ohore OE, Li J. Associations of hyperuricemia and obesity with remission of nonalcoholic fatty Liver Disease among Chinese men: a retrospective cohort study. PLoS ONE. 2018;13:e0192396.
Pirillo A, Casula M, Olmastroni E, Norata GD, Catapano AL. Global epidemiology of dyslipidaemias. Nat Rev Cardiol. 2021;18:689–700.
Vekic J, Zeljkovic A, Stefanovic A, Jelic-Ivanovic Z, Spasojevic-Kalimanovska V. Obesity and dyslipidemia. Metabolism. 2019;92:71–81.
Peng TC, Wang CC, Kao TW, Chan JY, Yang YH, Chang YW, Chen WL. Relationship between hyperuricemia and lipid profiles in US adults. Biomed Res Int 2015, 2015:127596.
Liang J, Jiang Y, Huang Y, Song W, Li X, Huang Y, Ou J, Wei Q, Gu J. The comparison of dyslipidemia and serum uric acid in patients with gout and asymptomatic hyperuricemia: a cross-sectional study. Lipids Health Dis. 2020;19:31.
Yu Y, Huang X, Li M, Ding C, Hu L, Zhong X, Zhou W, Wang T, Zhu L, Bao H, Cheng X. Is there a nonlinear relationship between serum uric acid and lipids in a Hypertensive Population with eGFR >/=30 ml/min/1.73 m(2)? Findings from the China Hypertension Registry Study. Int J Endocrinol. 2020;2020:9725979.
Tian Y, Chen K, Xie Z, Fang Y, Wang H, Nie Y, Hu D, Mu Y. The association between serum uric acid levels, metabolic syndrome and Cardiovascular Disease in middle aged and elderly Chinese: results from the DYSlipidemia International Study. BMC Cardiovasc Disord. 2015;15:66.
Chien KL, Hsu HC, Sung FC, Su TC, Chen MF, Lee YT. Hyperuricemia as a risk factor on cardiovascular events in Taiwan: the Chin-Shan Community Cardiovascular Cohort Study. Atherosclerosis. 2005;183:147–55.
Babio N, Martinez-Gonzalez MA, Estruch R, Warnberg J, Recondo J, Ortega-Calvo M, Serra-Majem L, Corella D, Fito M, Ros E, et al. Associations between serum uric acid concentrations and metabolic syndrome and its components in the PREDIMED study. Nutr Metab Cardiovasc Dis. 2015;25:173–80.
Fang J, Alderman MH. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971–1992. National Health and Nutrition Examination Survey. JAMA. 2000;283:2404–10.
Kuwabara M. Hyperuricemia, Cardiovascular Disease, and Hypertension. Pulse (Basel). 2016;3:242–52.
Wu J, Qiu L, Cheng XQ, Xu T, Wu W, Zeng XJ, Ye YC, Guo XZ, Cheng Q, Liu Q, et al. Hyperuricemia and clustering of cardiovascular risk factors in the Chinese adult population. Sci Rep. 2017;7:5456.
Jacobson TA, Ito MK, Maki KC, Orringer CE, Bays HE, Jones PH, McKenney JM, Grundy SM, Gill EA, Wild RA, et al. National lipid association recommendations for patient-centered management of dyslipidemia: part 1–full report. J Clin Lipidol. 2015;9:129–69.
Expert Dyslipidemia P, Grundy SM. An International Atherosclerosis Society Position paper: global recommendations for the management of dyslipidemia. J Clin Lipidol. 2013;7:561–5.
Bloomgarden Z, Ning G. Journal of Diabetes: ushering in volume 10. J Diabetes. 2018;10:4–5.
Ostchega Y, Hughes JP, Zhang G, Nwankwo T, Graber J, Nguyen DT. Differences in Hypertension prevalence and Hypertension control by urbanization among adults in the United States, 2013–2018. Am J Hypertens. 2022;35:31–41.
Feig DI, Madero M, Jalal DI, Sanchez-Lozada LG, Johnson RJ. Uric acid and the origins of Hypertension. J Pediatr. 2013;162:896–902.
Ali N, Perveen R, Rahman S, Mahmood S, Rahman S, Islam S, Haque T, Sumon AH, Kathak RR, Molla NH, et al. Prevalence of hyperuricemia and the relationship between serum uric acid and obesity: a study on Bangladeshi adults. PLoS ONE. 2018;13:e0206850.
Zhang Y, Zhang M, Yu X, Wei F, Chen C, Zhang K, Feng S, Wang Y, Li WD. Association of Hypertension and hypertriglyceridemia on incident hyperuricemia: an 8-year prospective cohort study. J Transl Med. 2020;18:409.
Chen JH, Pan WH, Hsu CC, Yeh WT, Chuang SY, Chen PY, Chen HC, Chang CT, Huang WL. Impact of obesity and hypertriglyceridemia on gout development with or without hyperuricemia: a prospective study. Arthritis Care Res (Hoboken). 2013;65:133–40.
Huang XB, Zhang WQ, Tang WW, Liu Y, Ning Y, Huang C, Liu JX, Yi YJ, Xu RH, Wang TD. Prevalence and associated factors of hyperuricemia among urban adults aged 35–79 years in southwestern China: a community-based cross-sectional study. Sci Rep. 2020;10:15683.
Haj Mouhamed D, Ezzaher A, Neffati F, Douki W, Gaha L, Najjar MF. Effect of cigarette Smoking on plasma uric acid concentrations. Environ Health Prev Med. 2011;16:307–12.
Shirasawa T, Ochiai H, Yoshimoto T, Nagahama S, Watanabe A, Yoshida R, Kokaze A. Cross-sectional study of associations between normal body weight with central obesity and hyperuricemia in Japan. BMC Endocr Disorders 2020, 20.
Oku F, Hara A, Tsujiguchi H, Suzuki K, Pham KO, Suzuki F, Miyagi S, Nakamura M, Takazawa C, Sato K et al. Association between Dietary Fat Intake and Hyperuricemia in men with chronic Kidney Disease. Nutrients 2022, 14.
Deb S, Sakharkar P. A Population based study of liver function amongst adults with hyperuricemia and gout in the United States. Diseases 2021, 9.
Schlesinger N. Dietary factors and hyperuricaemia. Curr Pharm Des. 2005;11:4133–8.
Yang WX, Ma Y, Hou YL, Wang YB, You CG. Prevalence of Hyperuricemia and its correlation with serum lipids and blood glucose in Physical Examination Population in 2015–2018: a retrospective study. Clin Lab 2019, 65.
Zhang Y, Wei F, Chen C, Cai C, Zhang K, Sun N, Tian J, Shi W, Zhang M, Zang Y, et al. Higher triglyceride level predicts hyperuricemia: a prospective study of 6-year follow-up. J Clin Lipidol. 2018;12:185–92.
Balasubramanian T. Uric acid or 1-methyl uric acid in the urinary bladder increases serum glucose, insulin, true triglyceride, and total cholesterol levels in Wistar rats. ScientificWorldJournal. 2003;3:930–6.
Furuhashi M. New insights into purine metabolism in metabolic Diseases: role of xanthine oxidoreductase activity. Am J Physiol Endocrinol Metab. 2020;319:E827–34.
Davidson MH, Ballantyne CM, Jacobson TA, Bittner VA, Braun LT, Brown AS, Brown WV, Cromwell WC, Goldberg RB, McKenney JM, et al. Clinical utility of inflammatory markers and advanced lipoprotein testing: advice from an expert panel of lipid specialists. J Clin Lipidol. 2011;5:338–67.
Raja V, Aguiar C, Alsayed N, Chibber YS, ElBadawi H, Ezhov M, Hermans MP, Pandey RC, Ray KK, Tokgozoglu L, et al. Non-HDL-cholesterol in dyslipidemia: review of the state-of-the-art literature and outlook. Atherosclerosis. 2023;383:117312.
Expert Dyslipidemia Panel of the International Atherosclerosis Society Panel m. An International Atherosclerosis Society Position paper: global recommendations for the management of dyslipidemia–full report. J Clin Lipidol. 2014;8:29–60.
Acknowledgements
First of all, the authors would like to thank all the staff from the First Affiliated Hospital of Wannan Medical College who were involved in this work. Secondly, the authors would like to thank the study participants for their cooperation.
Funding
This work was supported by the Teaching Reform and Quality Improvement Plan of the Department of Education of Anhui Province-Teaching Teacher (grant number 2019jxms066); The Teaching Reform and Quality Improvement Plan of the Department of Education of Anhui Province-Teaching Team (grant number 2018jxtd153).
Author information
Authors and Affiliations
Contributions
F.Y. and M.W. wrote the main manuscript text; W.C. and R.X. prepared Tables 1, 2, 3 and 4; H.J. and S.F. conducted the experiments; C.L. and T.G. analyzed the data; J.M. and W.H. contributed to the methodology; W.Y. supervised the entire project. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research protocol has been approved by the Ethics Committee of Wannan Medical College. This study was based on data from the Health Management Center at the First Affiliated Hospital of Wannan Medical College in Wuhu, China. Since the participants in this study came to the hospital for routine physical examinations, the Medical Ethics Committee of Wannan Medical College approved that the study only needs to obtain the participant’s verbal informed consent. Therefore, this study did not have the participants’ written informed consent. Informed consent has been obtained from the participants. All methods in the current research were conducted by the Declaration of Helsinki guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fang, Y., Mei, W., Wang, C. et al. Dyslipidemia and hyperuricemia: a cross-sectional study of residents in Wuhu, China. BMC Endocr Disord 24, 2 (2024). https://doi.org/10.1186/s12902-023-01528-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12902-023-01528-7