
Abstract
Background and aims
This study aimed to investigate the association between the Dietary Inflammatory Index (DII) and dyslipidemia, as well as to evaluate the mortality risk associated with DII in participants with dyslipidemia.
Methods
Data from the National Health and Nutrition Examination Survey database were divided into dyslipidemia and non-dyslipidemia groups. The association between DII and dyslipidemia was investigated using the weighted chi-square test, weighted t-test, and weighted logistic regression. Weighted Cox proportional hazards models were used to estimate the hazard ratios and 95% confidence intervals for all-cause and cardiovascular disease-related mortality within the dyslipidemia group.
Results
A total of 17,820 participants, including 4,839 without and 12,981 with dyslipidemia were analyzed in this study. The results showed that DII was higher in the dyslipidemia group compared to the non-dyslipidemia group (1.42 ± 0.03 vs. 1.23 ± 0.04, P < 0.01). However, for energy, protein, carbohydrates, total fat, saturated fat, and iron, DII was lower in participants with dyslipidemia. Logistic regression analysis revealed a strong positive association between DII and dyslipidemia. The odds ratios for dyslipidemia from Q1 to Q4 were 1.00 (reference), 1.12 (0.96–1.31), 1.23 (1.04–1.44), and 1.33 (1.11–1.59), respectively. In participants with dyslipidemia, a high DII was associated with high all-cause and cardiovascular mortality.
Conclusion
DII was closely associated with dyslipidemia. A pro-inflammatory diet may play a role in unfavorable consequences and is linked to both all-cause mortality and cardiovascular death in patients with dyslipidemia. Participants with dyslipidemia should pay attention to their anti-inflammatory dietary patterns.
Similar content being viewed by others

Introduction
Dyslipidemia comprises a range of conditions primarily defined by elevations in lipoprotein cholesterol, including low-density lipoprotein (LDL) and non-high-density lipoprotein cholesterol, as well as elevated triglycerides (TG) [1]. In the United States, 29% and 26% of adults have elevated LDL and TG levels, respectively [2]. Early accumulation of total cholesterol (TC) increases the risk of cardiovascular diseases (CVDs) by 2–3 times [3], which is a high-risk factor for stroke and death [4]. According to the U.S. Preventive Services Task Force, CVDs account for > 25% of all deaths in the United States [5]. Dyslipidemia causes a huge health and economic burden worldwide, and medical treatment has long been committed to improving dyslipidemia [6]; however, there is a serious lack of awareness of the etiology and prevention of this disease [7].
Dyslipidemia is primarily caused by hereditary, nutritional, and systemic diseases [8, 9]. Anti-inflammatory dietary patterns (such as the Mediterranean diet [10], dash diet [11], and Nordic diet [12]) are considered to have preventive effects. Potential mechanisms include improving insulin resistance [13], altering the gut microbiome [14], reducing mucosal and systemic inflammatory responses [15], and affecting epigenetic links such as DNA methylation and acetylation [16]. Obesity is another important risk factor for dyslipidemia, which has been recognized as chronic low-grade inflammation; a high-sugar, high-fat diet leads to increased harmful metabolites and systemic inflammation, which ultimately promotes the progression of obesity [17, 18].
The Dietary Inflammatory Index (DII) is a tool used to assess the level of an individual’s dietary inflammation by scoring the pro- or anti-inflammatory levels of various diets, which helps to clarify the relationship between diet-related inflammation and various metabolic diseases [19].
Increasing attention has been paid to the important role of systemic chronic inflammation in the occurrence and development of obesity [17], metabolic syndrome [20], cardiovascular metabolic diseases [21], diabetes mellitus (DM) [22], tumors [23] and other major chronic noncommunicable diseases [24] that threaten human health. Most studies were clinical trials, limited by the number of participants and short follow-up periods. No study has analyzed the association between DII and dyslipidemia and the risk on mortality outcomes in participants with dyslipidemia in large, well followed-up public databases so far.
In this study, we compared DII between individuals with and without dyslipidemia, explored the dose relationship between DII and dyslipidemia, and investigated the association between DII and all-cause mortality and CVDs mortality in the dyslipidemia group based on the National Health and Nutrition Examination Survey (NHANES) databases.
Methods
Data extraction
NHANES is a nationwide cross-sectional survey conducted by the National Center for Health Statistics in the United States. Detailed information on the design of the continuous NHANES is available at http://www.cdc.gov/nchs/nhanes/index.htm. All study protocols were approved by the Ethics Review Board of the National Center for Health Statistics. Ethical accreditation of our study was provided by the NHANES institutional review board https://www.cdc.gov/nchs/nhanes/irba98.html (Protocol #98 − 12, Protocol #2005-06, Protocol #2011-17, Protocol #2018-01).
Data from 1999 to 2019 were gathered from the NHANES database [25]. The program uses the United States Department of Agriculture’s automated multiple-pass method (AMPM) to collect dietary information from representative participants. Participants were selected based on a national sampling design. The AMPM approach is a research-based multiple-pass approach aimed at minimizing interviewer recall regarding food consumption [26]. Five steps were designed to enhance the completeness and accuracy of food recall. Additionally, at the conclusion of the interview, the participants were asked to indicate whether their food intake on the recalled day was greater, similar, or significantly lower than their usual consumption [27]. Finally, the nutrient profiles of every food and beverage were calculated using the Food Nutrient Database for Dietary Studies.
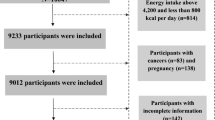
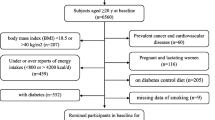
The inclusion criteria were: (1) participants at least 20 years old; (2) complete and accessible participants information; (3) complete mortality follow-up information; and (4) complete information regarding all exposure variables, outcome variables, and covariables. The collection is detailed in the flow chart (Fig. 1). Overall, 116,876 participants were included. After excluding participants without serum information (serum lipids and routine blood tests), dyslipidemia diagnosis information, DII information, and information about other covariables, including body mass index (BMI), smoking status, alcohol status, and other related diseases (hypertension, diabetes mellitus [DM], coronary artery disease [CAD], chronic heart failure [CHF], stroke, and cancer), 17,820 participants were ultimately included in our analysis.

Flow chart of the screening process for the selection of participants in NHANES (1999–2019)
Note: *diagnosis including: hypertension, DM, CAD, CHF, stroke and cancer
Exposure variable
DII was set as the exposure variable. It was calculated by adding the scores for each dietary component consumed within 24 h. We calculated DII according to the protocol described by Shivappa et al. [19]. The calculation of DII was based on a world database containing dietary intake data, as described by Shivappa et al. Robust estimates of the mean and standard deviation for each parameter were provided. The centered percentile value for each parameter was multiplied by the overall food parameter-specific inflammatory effect score. Food parameter-specific DII scores were summed to obtain the overall DII score for each individual. DII based on less than 30 food parameters reportedly maintains its predictive capacity. In the NHANES database, 28 food parameters are available, including energy, protein, carbohydrate, fiber, total fat, saturated fat, monounsaturated fatty acids (MUFA), polyunsaturated fatty acids (PUFA), cholesterol, Vitamin A, β-carotene, thiamin, riboflavin, niacin, Vitamin B6, folic acid, Vitamin B12, Vitamin C, Vitamin D, Vitamin E, magnesium, iron, zinc, selenium, caffeine, alcohol, and N3 and N6 fatty acids. By summarizing each DII score, we obtained an “overall DII score,” which is the final DII score for each topic that defines anti-and proinflammatory diets. DII is lower with an anti-inflammatory diet and higher with a pro-inflammatory one.
Outcome variable
The main outcomes were dyslipidemia status and mortality. Dyslipidemia was defined as an elevated TG (≥ 150 mg/dL) TC level (≥ 200 mg/dL or 5.18 mmol/L, LDL cholesterol ≥ 130 mg/dL or 3.37 mmol/L, or high-density lipoprotein [HDL] cholesterol < 40 mg/dL or 1.04 mmol/L in men and < 50 mg/dL or 1.30 mmol/L in women) or intake of cholesterol-lowering agents [28].
To investigate whether DII is associated with the risk of all-cause and CVD-related mortality in patients with dyslipidemia, we performed a survival analysis in the dyslipidemia group. Mortality status was determined by cross-referencing the NHANES data with the national death index records, commencing from the baseline survey date until December 31, 2019. The identification of fatalities resulting from CVDs (specifically I20–I51, I11, I13, I00–I09) was based on the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10).
Covariable
We included covariables associated with DII and dyslipidemia based on previous studies [29, 30]. The variables included age, sex, race, education, annual family income, BMI, C-reactive protein (CRP), alcohol consumption, smoking status, hypertension, DM, CAD, CHF, stroke, and cancer. The following covariables were extracted directly from the NHANES database according to participants’ self-reported data: age, sex, and race.
BMI was calculated as weight (kg) divided by height squared (m2) [31].
Hypertension was diagnosed when one of the following conditions was met [32]: (1) participant responded affirmatively to the inquiry “Have you received a definitive diagnosis of hypertension?”; (2) participant displayed a systolic blood pressure (SBP) measurement ≥ 140 mmHg and/or a diastolic blood pressure (DBP) measurement ≥ 90 mmHg; or (3) current use of antihypertensive medication.
DM was diagnosed when any of the following conditions were met [33]: (1) participant answered affirmatively to the question “Do you have a clear diagnosis of DM?”; (2) glycohemoglobin levels > 6.5%; (3) fasting plasma glucose levels ≥ 7.0 mmol/L; (4) randomly assigned blood glucose levels ≥ 11.1 mmol/L; (5) 2-hour oral glucose tolerance test levels ≥ 11.1 mmol/L; or (6) the participant was taking medications for diabetes or insulin.
CHF, CAD, cancer, and stroke were diagnosed according to the participants’ answers to the question, “Do you have a clear diagnosis of CHF/CAD/cancer/stroke?”
Education level was classified as “below high school,” “high school,” and “above high school.”
Alcohol intake was categorized as never (< 12 drinks in lifetime), former drinker (≥ 12 drinks in 1 year and consumed none in the past year, or had not consumed alcohol in the past year but drank ≥ 12 drinks in their lifetime), current mild drinker (≤ 1 drink per day for women or ≤ 2 drinks per day for men on average over the past year), current moderate drinker (≤ 2 drink per day for women or ≤ 3 drinks per day for men on average over the past year), or current heavy drinkers (> 3 drinks per day for women or > 4 drinks per day for men on average over the past year) [34].
Statistical analysis
In our study, wtdr4 year and wtdrd1 were used as weighted variables. Wtdr4 year was the sample weighting code for day-1 dietary in 1999–2002 while wtdrd1 were the sample weighting code for day-1 dietary in 2003–2019. The detail information about sample weighting code could be found on https://wwwn.cdc.gov/nchs/nhanes/search/default.aspx.
Our study conducted two sets of quartile calculations: one based on DII of all participants and the other based on the dyslipidemia subgroup. The former were labeled as Q1, Q2, Q3, and Q4, while the latter were labeled as q1, q2, q3, and q4. Three adjustment variables of the models were used for the dose-related and survival analyses. Model 1 was adjusted for age and sex; Model 2 was adjusted for age, sex, race, education, and BMI; and Model 3 was adjusted for age, sex, race, education, BMI, smoking, alcohol consumption, and comorbidities, including hypertension, DM, CAD, CHF, stroke, and cancer. All data were analyzed using R (version 4.2.3; R Foundation for Statistical Computing, Vienna, Austria) and R Studio. P < 0.05 was considered as a statistically significant. For continuous variables, the mean and standard error (SE) were used, and weighted t-tests were used for comparison. For categorical variables, we used the number of cases and weighted prevalence for description and a chi-squared test for comparison between groups.
Univariate logistic regression analyses were performed to investigate the association between dyslipidemia and DII. A multivariate logistic regression model was then used to analyze the relationship between DII and dyslipidemia after adjusting for covariables. The adjusted variables included sex, BMI, race, family income, education, comorbidities (CHF, DM, CAD, hypertension, cancer, and stroke), and smoking, and alcohol status. Dose-related analyses of DII in participants with dyslipidemia were performed using multivariate logistic regression. The outcome variable was dyslipidemia, and the control group was participants without dyslipidemia. We calculated Pfor trend to assess the association between DII and dyslipidemia, adjusted with the three aforementioned models. We conducted a subgroup analysis of age, sex, race, family income, education level, BMI, comorbidities, smoking, and alcohol consumption.
Finally, a survival analysis was performed in the subgroup of participants with dyslipidemia to reveal the association between the DII and the risk of all-cause and CVD-related mortality in these participants. Cox regression analysis was performed using DIIs of participants with dyslipidemia. The Cox proportional hazards model was used to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) for the association between concentrations and all-cause and cause-specific mortality.
Results
Baseline characteristics of participants
Overall, 17,820 participants were involved, representing a population of 117,825,860 US citizens with robust follow-up data. Table 1 shows the basic information of participants with and without dyslipidemia. Participants with dyslipidemia (12,981) accounted for approximately 72.84% of all the participants in our study. Participants with dyslipidemia exhibited higher DII (1.42 ± 0.03 vs. 1.23 ± 0.04), BMI (29.15 ± 0.11 vs. 26.24 ± 0.12 kg/m2), and blood pressure (SBP: 123.57 ± 0.27 mmHg vs. 117.51 ± 0.35 mmHg; DBP: 71.68 ± 0.22 mmHg vs. 69.42 ± 0.26 mmHg). Additionally, participants with dyslipidemia were older (50.13 ± 0.28 years vs. 40.21 ± 0.36 years), with a higher CRP (0.44 ± 0.02 mg/L vs. 0.31 ± 0.01 mg/L) and likelihood for comorbidities (hypertension, DM, CAD, CHF, stroke, and cancer). The baseline characteristics of the participants across DII quartiles are shown in Supplementary Table S1. Compared with the Q1, Q2, and Q3 groups, the Q4 group had the highest proportion of participants with dyslipidemia. The results also suggested a gradual decrease in the proportion of participants without dyslipidemia in the Q1–Q4 groups, which were 30.04%, 26.57%, 25.38%, and 23.74%, respectively. In Q4, the proportion of participants with dyslipidemia reached 76.26%, accompanied by a higher BMI of 29.10 ± 0.16 kg/m2. Furthermore, the Q4 group exhibited a higher incidence of comorbidities, including CHF, DM, stroke, and hypertension than the Q1–Q3 groups. Moreover, Q4 showed the highest CRP levels (0.52 ± 0.03 mg/L).
Comparison of DII and component of DII between the dyslipidemia and non-dyslipidemia groups
Compared to participants without dyslipidemia, those with dyslipidemia had higher scores for fiber, MUFA, PUFA, vitamins A/E/B6, thiamin, riboflavin, niacin, folic acid, magnesium, zinc, selenium, alcohol, and N-6 fatty acids. However, they had lower energy, protein, carbohydrate, total fat, saturated fat, and iron scores (Supplementary table S2).
Association between DII and dyslipidemia
The univariate logistic regression analysis is presented in Fig. 2A. DII was strongly and positively associated with dyslipidemia. The odds ratio (OR) (95% confidence interval [CI]) was estimated to be 1.06 (1.03–1.09), indicating that the odds of having dyslipidemia increased by 1.06 times for every one-unit increase in DII (P < 0.01). Age, BMI, comorbidities (CHF, DM, cancer, stroke, CAD, and hypertension), smoking status, and alcohol intake were also associated with dyslipidemia. In multivariate logistic regression analysis, after adjusting for sex, BMI, race, family income, education, comorbidities (hypertension, DM, CAD, CHF, stroke, and cancer), and smoking, and alcohol status (Fig. 2B), DII was still associated with dyslipidemia. The OR (95% CI) was 1.05 (1.02–1.08), indicating that the odds of having dyslipidemia increased by 5% for every one-unit increase in DII (P < 0.01).

Logistic regression of factors associated with dyslipidemia
Note: DII was associated with dyslipidemia in both weighted univariable logistic regression (A) and weighted multivariable logistic regression (B). The P value was calculated by weighted univariable logistic regression and multivariable logistic regression. Covariable including age, BMI, sex, race, family income, education, hypertension, DM, CAD, CHF, stroke, and cancer, smoking and alcohol intake
Dose-response analysis of DII and dyslipidemia
Multiple regression analysis was conducted across the DII quartiles to further explore the dose-response relationship between dyslipidemia and DII (Table 2). After adjusting for smoking, alcohol and comorbidities (hypertension, DM, CAD, CHF, stroke, and cancer), the OR and 95% CI from Q1 to Q4 were 1.00 (reference), 1.12 (0.96–1.31), 1.23 (1.04–1.44), and 1.33 (1.11–1.59), respectively (Pfor trend <0.01), indicating a persistent dose-response relationship between DII and dyslipidemia.
Subgroup analysis
Significant moderating effects were found in the subgroup analysis stratified by family income (Pfor interaction = 0.03). A stronger association was observed in participants with an annual family income <$20,000 than in those with annual family income >$20 000; ORs (95% CI) were 1.13 (1.07–1.20) and 1.04 (1.01–1.08), respectively. However, DII was still associated with dyslipidemia in participants with a household income >$20,000 (Pfor trend = 0.01). The association between DII and dyslipidemia was more significant in participants without comorbidities (CHF, DM, stroke, CAD, cancer) (Pfor trend <0.05). There was no significant interaction between the subgroups (Pfor interaction >0.05) (Table 3).
Survival analysis for DII with all-cause CVD-related mortality in participants with dyslipidemia
In the cohort of 12,981 participants with dyslipidemia, 2,203 all-cause deaths were observed during the follow-up period, of which 588 were related to CVDs. After adjusting for age, sex, race, education, BMI, smoking, alcohol consumption, and comorbidities (CHF, DM, stroke, CAD, hypertension, and cancer) in Model 3, DII remained highly associated with all-cause CVD-related mortality in patients with dyslipidemia. The multivariate-adjusted HRs (95% CI) for all-cause mortality from Q1 to Q4 were 1.00 (reference), 1.39 (1.20–1.62), 1.37 (1.13–1.65), 1.50 (1.24–1.82), respectively (P < 0.01). For CVD-related mortality, HRs from Q1 to Q4 were 1.00 (reference), 1.46 (1.00–2.13), 1.38 (0.94–2.01), 2.07 (1.38–3.09), respectively (P < 0.01) (Table 4).
Discussion
This study represented an initial analysis of the association between DII and dyslipidemia based on the NHANES database. These findings indicate that a proinflammatory diet is associated with dyslipidemia and that a dose-response relationship exists between DII and dyslipidemia. Additionally, survival analysis suggested that dyslipidemia with a higher DII score was positively associated with a high risk of all-cause CVD-related mortality.
Comparison with other studies
DII has been used to evaluate the inflammatory propensity for individual dietary intake. This was first proposed by Hébert et al. (2009) [35]. Tyrovolas et al. reported the relationship between DII and CVD risk factors (assessed as obesity, DM, hypertension, and hypercholesterolemia) and suggested that the CVD risk factors among participants on a proinflammatory diet were 1.37–1.50 times higher compared to those on an anti-inflammatory diet [36]. In another clinical study, DII was found to increase waist circumference and TG levels in overweight and obese women [37]. However, most of these studies were clinical studies and were limited by their small sample sizes and short follow-up periods. Hence, we investigated the association between DII and dyslipidemia based on NHANES data. Our results suggested a strong relationship between a proinflammatory diet and dyslipidemia. Subgroup analyses suggested that DII was more strongly associated with dyslipidemia in households with annual incomes <$20 000. A proinflammatory diet was also strongly associated with all-cause and cardiovascular mortality in participants with dyslipidemia.
Possible mechanisms between Dietary Inflammatory and Dyslipidemia
Our study found that DII for fiber, MUFA, PUFA, vitamin A/E, vitamin B (including B6, thiamin, riboflavin, niacin, and folic acid), magnesium, and zinc in participants with dyslipidemia were significantly higher than those in participants without dyslipidemia. Possible mechanisms are as follows.
Fiber: Previous research has demonstrated that a higher fiber content can potentially mediate the beneficial effects of risk markers associated with CVDs [38]. These effects are attributed to various mechanisms such as enhanced insulin sensitivity, decreased oxidative stress, and cytokine production [39]. Additionally, it has been found that fiber exerts anti-inflammatory properties [40].
MUFA and PUFA: Studies have found that MUFA can mitigate inflammation by modulating the production of inflammatory mediators and regulating neutrophil infiltration [41]. Potential underlying mechanisms include the reduction of endoplasmic reticulum stress [42], enhancement of vascular endothelial inflammation, and systemic inflammatory responses [43].
Vitamins A and E: Fat-soluble vitamins possess antioxidant properties [44] and can interact with lipoproteins. Their action is linked to the production of chylomicrons in the gut, which subsequently affect lipid absorption and metabolism [45, 46].
Folic acid and Vitamin B6 are essential nutrients for nucleic acid synthesis and methyl generation [47]. Vitamin B6, in particular, has been found to reduce endogenous cholesterol and lipid synthesis, while enhancing cholesterol transport to liver cells [48].
Niacin: Niacin has been extensively studied for its ability to regulate fat metabolism. It can modulate the expression of lipoproteins [49, 50], diacylglycerol acyltransferase [51], and genes related to fat metabolism [52, 53]. Niacin promotes endothelium-dependent vasodilation and reduces vascular inflammation [54].
Thiamin: Thiamin, in its bioactive form (thiamine pyrophosphate), plays a crucial role in maintaining the balance of oxidative metabolism in the body. It regulates glucose and lipid metabolism by influencing lipid peroxidation product levels and glutathione reductase activity [55].
Riboflavin: Riboflavin affects the activity of lipid-metabolizing enzymes, such as 3-hydroxy-3-methyl glutaryl coenzyme A reductase and lecithin-cholesterol acyltransferase, thereby regulating blood lipid levels [56, 57]. Additionally, studies have shown a negative association between riboflavin and the intestinal flora, suggesting a potential mechanism for regulating lipid metabolism [58].
Magnesium: Increasing magnesium intake improves chronic metabolic disorders and cardiovascular diseases by reducing low-grade inflammation [59]. This effect is believed to be mediated by the regulation of reactive oxygen species activity [60]. Furthermore, magnesium can regulate enzymes involved in liver lipid metabolism, thereby reducing blood lipid levels [60, 61].
Implication for the clinical practice
Changes in the distribution of large amounts of nutrients (such as fats), low-carbohydrate diets, and caloric restriction appear to be effective strategies for ameliorating inflammation and reducing serum lipid levels [62]. Interestingly, further analysis of nutrient composition revealed that participants with dyslipidemia scored lower on energy, protein, carbohydrate, total fat, saturated fat, and selenium levels than those without it. It is presumed that individuals with dyslipidemia have already begun to undergo dietary changes after the diagnosis. Another NHANES study reported that participants with chronic diseases such as dyslipidemia, DM, or hypertension paid more attention to the nutritional labels of foods. These individuals occasionally exhibit inappropriate dietary patterns [63]. However, participants with dyslipidemia still had higher overall DII scores than those without it. Diet should be considered as a whole, and participants should be more concerned about diet patterns than restricting or supplementing the intake of a single nutrient [64]. Research has shown that a single dietary supplement tends toward negative results in reducing mortality from CVDs and other causes [65]. Participants with CVDs are more likely to benefit from a healthy dietary pattern than from a single dietary supplement. Another efficient strategy is to implement nutritional content ratings on food packaging beyond the mere listing of calories and ingredients to comprehensively evaluate nutrition and mitigate the risk of CVDs [66].
The subgroup analysis results showed a stronger association between DII and dyslipidemia in participants with an annual family income <$20,000. It is consistent with the global trend of dyslipidemia prevalence shifting from high-income to low-income countries [67, 68]. Subgroup analysis also showed a stronger association between DII and dyslipidemia in participants without comorbidities (CHF, DM, stroke, CAD, cancer) compared to those with them. Similarly, different BMI categories did not affect the association between DII and dyslipidemia (Pfor interaction = 0.34), but for participants with a BMI of 25–30 kg/m2, an increase in DII was associated with an increase in dyslipidemia (Pfor trend = 0.02). Possible causes are associated with the comorbid dyslipidemia that participants with aforementioned chronic diseases or overweight individuals (BMI > 25 kg/m2) might have already had, thus weakening the association between DII and dyslipidemia. These results suggested that special attention should be given to the intake of anti-inflammatory diet, for individuals with fewer comorbidities, a BMI of 20–25 kg/m2, and an annual family income <$20,000, as their dietary intake had a stronger association with dyslipidemia.
Limitations
There were unavoidable limitations; therefore, the conclusions of this study should be interpreted with caution. First, as this was a cross-sectional study, a causal explanation for the relationship between DII and dyslipidemia cannot be provided. Second, data from the NHANES database were subject to memory bias and random errors. This study did not include individuals below the age of 20 years or those without serum sample, which may have resulted in data bias. Furthermore, as a result of the database’s design, some individual information among the participants could not be extracted, potentially introducing bias, such as energy intake restriction and inflammatory-related diseases. Recently, studies have reported the Energy-adjusted Dietary Inflammatory Index (E-DII) [69, 70] that aims to mitigate the bias resulting from differences in energy intake. In future research, we plan to incorporate E-DII and further validate its effectiveness in addressing this source of bias.
Conclusions
The findings of our study indicates a close association between DII and dyslipidemia, as evidenced by higher scores on certain proinflammatory diets among participants with dyslipidemia compared to those without it. Moreover, our study indicates that a pro-inflammatory diet may play a role in unfavorable consequences and is linked to both all-cause mortality and cardiovascular death in patients with dyslipidemia.
Abbreviations
- AMPM:
-
Automated Multiple Pass methods
- BMI:
-
Body Mass Index
- CAD:
-
Coronary Artery Disease
- CHF:
-
Congestive Heart Failure
- CIs:
-
Confidence Intervals
- CRP:
-
C reactive protein
- CVDs:
-
Cardiovascular Diseases
- DBP:
-
Diastolic Blood Pressure
- DII:
-
Dietary Inflammatory Index
- DM:
-
Diabetes Mellitus
- HDL:
-
High-Density Lipoprotein
- HRs:
-
Hazard ratios
- LDL:
-
Low-Density Lipoprotein
- MUFA:
-
Monounsaturated Fatty Acids
- NHANES:
-
National Health and Nutrition Examination Survey
- OR:
-
Odds Ratio
- PUFA:
-
Polyunsaturated Fatty Acids
- SBP:
-
Systolic Blood Pressure
- TC:
-
Total Cholesterol
- TG:
-
Triglycerides
References
Handelsman Y, Jellinger PS, Guerin CK, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the management of Dyslipidemia and Prevention of Cardiovascular Disease algorithm – 2020 executive Summary[J]. Endocr Pract. 2020;26(10):1196–224.
Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics–2020 update: a report from the American Heart Association. Circulation. 2020;141:e139–e596.
Alloubani A, Nimer R, Samara R. Relationship between hyperlipidemia, cardiovascular disease and stroke: a systematic review. Curr Cardiol Rev. 2021;17:e051121189015. https://doi.org/10.2174/1573403X16999201210200342
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics-2015 update: a report from the american heart association. Circulation. 2015;131:e29–322.
US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Aspirin use to prevent Cardiovascular Disease: US Preventive Services Task Force Recommendation Statement[J]. JAMA. 2022;327(16):1577.
Aggarwal R, Bhatt DL, Rodriguez F, Yeh RW, Wadhera RK. Trends in lipid concentrations and lipid control among US adults, 2007–2018. JAMA. 2022;328(8):737–45. https://doi.org/10.1001/jama.2022.12567. pii: 2795529.
Newton SL, Hoffmann AP, Yu Z, Haidermota S, Natarajan P, Honigberg MC. Management of severe and moderate hypercholesterolemia in Young Women and Men. JAMA Cardiol. 2022;7(2):227–30. https://doi.org/10.1001/jamacardio.2021.4983. pii: 2786325.
Taghizadeh E, Mardani R, Rostami D, Taghizadeh H, Bazireh H, Hayat SMG. Molecular mechanisms, prevalence, and molecular methods for familial combined hyperlipidemia disease: a review. J Cell Biochem. 2019;120(6):8891–8. https://doi.org/10.1002/jcb.28311
Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk[J]. Eur Heart J. 2020;41(1):111–88. https://doi.org/10.1016/S2213-8587
Foscolou A, Georgousopoulou E, Magriplis Eet la. The mediating role of Mediterranean diet on the association between Lp(a) levels and cardiovascular disease risk: a 10-year follow-up of the ATTICA study. Clin Biochem. 2018;60:33–7. https://doi.org/10.1016/j.clinbiochem.2018.07.011. pii: S0009-9120(18)30595-2. PubMed PMID: 30055165.
Lari A, Sohouli MH, Fatahi S, et al. The effects of the Dietary Approaches to stop hypertension (DASH) diet on metabolic risk factors in patients with chronic disease: a systematic review and meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2021;31(10):2766–78. https://doi.org/10.1016/j.numecd.2021.05.030
Adamsson V, Reumark A, Fredriksson IB, et al. Effects of a healthy Nordic diet on cardiovascular risk factors in hypercholesterolaemic subjects: a randomized controlled trial (NORDIET). J Intern Med. 2011;269(2):150–9. https://doi.org/10.1111/j.1365-2796.2010.02290.x
Festa A, D’Agostino R, Howard G, et al. Chronic subclinical inflammation as part of the insulin resistance syndrome: the insulin resistance atherosclerosis study (IRAS). Circulation. 2000;102(1):42–7. https://doi.org/10.1161/01.cir.102.1.42. PubMed PMID: 10880413.
Xu M, Lan R, Qiao L et al. Bacteroides vulgatus ameliorates lipid metabolic Disorders and modulates gut microbial composition in hyperlipidemic rats. Microbiol Spectr 2023 Jan 10:e0251722. https://doi.org/10.1128/spectrum.02517-22
Fujita K, Hayashi T, Mstsushita, et al. Obesity inflam-mation and prostate cancer [J]. J Clin Med. 2019;8:201.
Franzago M, Pilenzi L, Di Rado S, Vitacolonna E, Stuppia L. The epigenetic aging, obesity, and lifestyle. Front Cell Dev Biol. 2022; 10:985274. pii: 985274. https://doi.org/10.3389/fcell.2022.985274
Hariharan R, Odjidja EN, Scott D, et al. The dietary inflammatory index, obesity, type 2 diabetes, and cardiovascular risk factors and diseases. Obes Rev. 2022;23(1):e13349. https://doi.org/10.1111/obr.13349
De Heredia FP, Gómez-Martínez S, Marcos A. Obesity, inflammation and the immune system. Proc Nutr Soc. 2012;71(2):332-8. pii: S0029665112000092. https://doi.org/10.1017/S0029665112000092
Shivappa N, Steck SE, Hurley TG et al. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689-96. pii: S1368980013002115. https://doi.org/10.1017/S1368980013002115
Moodley A, Womersley JS, Swart PC, et al. A network analysis investigating the associations between posttraumatic stress symptoms, markers of inflammation and metabolic syndrome. J Psychiatr Res. 2023;165:105–14. https://doi.org/10.1016/j.jpsychires.2023.07.018. pii: S0022-3956(23)00368-0.
Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352:1685–95. https://doi.org/10.1056/NEJMra043430
Li T, Wang P, Wang X, et al. Inflammation and insulin resistance in Diabetic Chronic Coronary Syndrome Patients. Nutrients. 2023;15(12). https://doi.org/10.3390/nu15122808. pii: nu15122808.
Yin Q, Yang Q, Shi W et al. Mendelian Randomization Analyses of Chronic Immune-Mediated Diseases, Circulating Inflammatory Biomarkers, and Cytokines in Relation to Liver Cancer. Cancers (Basel). 2023;15(11) pii: cancers15112930. https://doi.org/10.3390/cancers15112930
Mrowietz U, Sümbül M, Gerdes S. Depression, a major comorbidity of psoriatic disease, is caused by metabolic inflammation. J Eur Acad Dermatol Venereol. 2023 May;15. https://doi.org/10.1111/jdv.19192
Centers for Disease Control and Prevention (CDC); National Center for Health Statistics (NCHS). National Health and Examination Survey Data.Available online: https://wwwn.cdc.gov/nchs/nhanes/Default.aspx(accessed on 5 Aug 2023).
Agricultural Research Service; Beltsville Human Nutrition Research Center; Food Surveys Research Group. USDA Automated Multiple-Pass Method for Dietary Recalls.Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/ampm-usda-automated-multiple-pass-method/(accessed on 5 Aug 2023).
Moshfegh AJ, Rhodes DG, Baer DJ, et al. The US Department of Agriculture Automated multiple-pass method reduces bias in the collection of energy intakes. Am J Clin Nutr. 2008;88(2):324–32. https://doi.org/10.1093/ajcn/88.2.324
Reiter-Brennan C, Osei AD, Iftekhar Uddin SM, et al. ACC/AHA lipid guidelines: personalized care to prevent cardiovascular disease. Cleve Clin J Med. 2020;87(4):231–9. https://doi.org/10.3949/ccjm.87a.19078
Zhang Y, Liu W, Zhang W, et al. Association between blood lead levels and hyperlipidemiais: results from the NHANES (1999–2018). Front Public Health. 2022;10:981749. https://doi.org/10.3389/fpubh.2022.981749. Published 2022 Sep 9.
Chen X, Zhou M, Yan H, Chen J, Wang Y, Mo X. Association of serum total 25-hydroxy-vitamin D concentration and risk of all-cause, cardiovascular and malignancies-specific mortality in patients with hyperlipidemia in the United States. Front Nutr. 2022;9:971720. Published 2022 Oct 20. https://doi.org/10.3389/fnut.2022.971720
Korhonen PE, Mikkola T, Kautiainen H, Eriksson JG. Both lean and fat body mass associate with blood pressure. Eur J Intern Med. 2021;91:40–4. https://doi.org/10.1016/j.ejim.2021.04.025
Miao H, Liu Y, Tsai TC, Schwartz J, Ji JS. Association between blood lead level and uncontrolled hypertension in the US Population (NHANES 1999–2016). J Am Heart Assoc. 2020;9(13):e015533. https://doi.org/10.1161/JAHA.119.015533
Wan Z, Guo J, Pan A, Chen C, Liu L, Liu G. Association of serum 25-Hydroxyvitamin D concentrations with all-cause and cause-specific mortality among individuals with diabetes. Diabetes Care. 2021;44(2):350–7. https://doi.org/10.2337/dc20-1485
Casagrande SS, Cowie CC. Trends in dietary intake among adults with type 2 diabetes: NHANES 1988–2012. J Hum Nutr Diet. 2017;30(4):479–89. https://doi.org/10.1111/jhn.12443
Cavicchia PP, Steck SE, Hurley TG, Hussey JR, Ma Y, Ockene IS, Hébert JR. A new dietary inflammatory index predicts interval changes in serum high-sensitivity C-reactive protein. J Nutr. 2009;139(12):2365–72. https://doi.org/10.3945/jn.109.114025. Epub 2009 Oct 28. PMID: 19864399; PMCID: PMC2777480.
Tyrovolas S, Koyanagi A, Kotsakis GA, et al. Dietary inflammatory potential is linked to cardiovascular disease risk burden in the US adult population. Int J Cardiol. 2017;240:409–13. https://doi.org/10.1016/j.ijcard.2017.04.104
Tavakoli A, Mirzababaei A, Moosavi H, Mehranfar S, Keshavarz SA, Mirzaei K. Dietary inflammatory index (DII) may be associated with hypertriglyceridemia waist circumference phenotype in overweight and obese Iranian women: a cross sectional study. BMC Res Notes. 2021;14(1):312. Published 2021 Aug 16. https://doi.org/10.1186/s13104-021-05712-7
Ma Y, Griffith JA, Chasan-Taber L, et al. Association between dietary fiber and serum C-reactive protein1–3[J]. Am J Clin Nutr. 2006;83(4):760–6. https://doi.org/10.1093/ajcn/83.4.760
Merchant AT, Pitiphat W, Franz M, Joshipura KJ. Whole-grain and fiber intakes and periodontitis risk in men. Am J Clin Nutr. 2006;83(6):1395–400. https://doi.org/10.1093/ajcn/83.6.1395
Hills RD Jr, Pontefract BA, Mishcon HR, Black CA, Sutton SC, Theberge CR. Gut microbiome: profound implications for diet and disease. Nutrients. 2019;11(7):1613. https://doi.org/10.3390/nu11071613
Farag MA, Gad MZ. Omega-9 fatty acids: potential roles in inflammation and cancer management. J Genet Eng Biotechnol. 2022;20(1):48. pii: https://doi.org/10.1186/s43141-022-00329-0. doi: 10.1186/s43141-022-00329-0.
Zheng J, Lee J, Byun J, et al. Partial replacement of high-fat diet with n-3 PUFAs enhanced beef tallow attenuates dyslipidemia and endoplasmic reticulum stress in tunicamycin-injected rats. Front Nutr. 2023;10:1155436. https://doi.org/10.3389/fnut.2023.1155436
Scoditti E, Capurso C, Capurso A, et al. Vascular effects of the Mediterranean diet-part II: role of omega-3 fatty acids and olive oil polyphenols. Vascul Pharmacol. 2014;63:127–34.
Cheng T-Y, Zhu Z, Masuda S, Morcos NC. Effects of multinutrient supplementation on antioxidant defense systems in healthy human beings. J Nutr Biochem 2001;12:388e95. Elsevier.
Reboul E. Vitamin E intestinal absorption: regulation of membrane transport across the enterocyte. IUBMB Life. 2019;71(4):416–23. https://doi.org/10.1002/iub.1955
Julve J, Martín-Campos JM, Escolà-Gil JC, Blanco-Vaca F, Chylomicrons. Advances in biology, pathology, laboratory testing, and therapeutics. Clin Chim Acta. 2016;455:134 – 48. pii: S0009-8981(16)30047-X. https://doi.org/10.1016/j.cca.2016.02.004
Li M, Li S, Chavarro JE, et al. Prepregnancy habitual intakes of total, supplemental, and food folate and risk of gestational diabetes mellitus: a prospective cohort study. Diabetes Care. 2019;42(6):1034–41. https://doi.org/10.2337/dc18-2198
Zhang Q, Zhou X, Zhang J, Li Q, Qian Z. Selenium and vitamin B6 cosupplementation improves dyslipidemia and fatty liver syndrome by SIRT1/SREBP-1c pathway in hyperlipidemic Sprague-Dawley rats induced by high-fat diet. Nutr Res. 2022;106:101–18. https://doi.org/10.1016/j.nutres.2022.06.010. pii: S0271-5317(22).
MOSELHY SS, KAMAL I H, KUMOSANI T A, et al. Possible inhibition of hydroxy methyl glutaryl CoA reductase activity by nicotinic acid and ergosterol: as targeting for hypocholesterolemic action[J]. Afr Health Sci. 2016;16(1):319–24. https://doi.org/10.4314/ahs.v16i1.42
ROMANI M, HOFER D C KATSYUBAE, et al. Niacin: an old lipid drug in a new NAD + dress[J]. J Lipid Res. 2019;60(4):741–6. https://doi.org/10.1194/jlr.S092007
HU M, CHU W C W YAMASHITAS, et al. Liver fat reduction with niacin is influenced by DGAT-2 polymorphisms in hypertriglyceridemic patients[J]. J Lipid Res. 2012;53(4):802–9. https://doi.org/10.1194/jlr.P023614
XING X K, WANG H, ZHAO L, et al. Niacin downregulates chemokine (c-c motif) ligand 2(CCL2) expression and inhibits fat synthesis in rat liver cells[J]. Trop J Pharm Res. 2020;19(5):977–82. https://doi.org/10.4314/tjpr.v19i5.10
KROON T, BACCEGA T, OLSÉN A, et al. Nicotinic acid timed to feeding reverses tissue lipid accumulation and improves glucose control in obese Zucker rats[J]. J Lipid Res. 2017;58(1):31–41. https://doi.org/10.1194/jlr.M068395
WU BJ, CHARLTON YANL, Arteriosclerosis, et al. Thromb Vascular Biology. 2010;30(5):968–75. https://doi.org/10.1161/ATVBAHA.109.201129
Ke ZJ, Gibson GE. Selective response of various brain cell types during neurodegeneration induced by mild impairment of oxidative metabolism. Neurochem Int 2004 Jul-Aug;45(2–3):361–9. pii: S0197018603002985. https://doi.org/10.1016/j.neuint.2003.09.008
Lv XC, Chen M, Huang ZR, Guo WL, Ai LZ, Bai WD, Yu XD, Liu YL, Rao PF, Ni L. Potential mechanisms underlying the ameliorative effect of Lactobacillus paracasei FZU103 on the lipid metabolism in hyperlipidemic mice fed a high-fat diet. Food Res Int. 2021;139:109956. pii: S0963-9969(20)30981-9. https://doi.org/10.1016/j.foodres.2020.109956
Yang B, Xuan S, Ruan Q, Jiang S, Cui H, Zhu L, Luo X, Jin J, Zhao Z. UPLC/Q-TOF-MS/MS-based metabolomics revealed the lipid-lowering effect of Ilicis Rotundae Cortex on high-fat diet induced hyperlipidemia rats. J Ethnopharmacol. 2020;256:112784. pii: S0378-8741(19)34981-5. https://doi.org/10.1016/j.jep.2020.112784
Wang Z, Cai Z, Ferrari MW, Liu Y, Li C, Zhang T, Lyu G. The v between gut microbiota and serum Metabolomic in Elderly patients with chronic heart failure. Mediators Inflamm. 2021;2021:5587428. https://doi.org/10.1155/2021/5587428
Song Y, Ridker PM, Manson JE, Cook NR, Buring JE, Liu S. Magnesium intake, C-reactive protein, and the prevalence of metabolic syndrome in middle-aged and older U.S. women. Diabetes Care. 2005;28(6):1438-44. pii: 28/6/1438. https://doi.org/10.2337/diacare.28.6.1438
Mak IT, Kramer JH, Chen X, Chmielinska JJ, Spurney CF, Weglicki WB. Mg supplementation attenuates ritonavir-induced hyperlipidemia, oxidative stress, and cardiac dysfunction in rats. Am J Physiol Regul Integr Comp Physiol. 2013;305(10):R1102-11. pii: ajpregu.00268.2013. https://doi.org/10.1152/ajpregu.00268.2013
Lupo MG, Biancorosso N, Brilli E, Tarantino G, Adorni MP, Vivian G, Salvalaio M, Dall’Acqua S, Sut S, Neutel C, Chen H, Bressan A, Faggin E, Rattazzi M, Ferri N. Cholesterol-Lowering Action of a Novel Nutraceutical Combination in Uremic Rats: Insights into the Molecular Mechanism in a Hepatoma Cell Line. Nutrients. 2020;12(2) pii: nu12020436.
Luna-Castillo KP, Olivares-Ochoa XC, Hernández-Ruiz RG, et al. The Effect of Dietary Interventions on Hypertriglyceridemia: from Public Health to Molecular Nutrition Evidence[J]. Nutrients. 2022;14(5):1104. https://doi.org/10.3390/nu14051104
Post RE, Mainous AG 3rd, Diaz VA, Matheson EM, Everett CJ. Use of the nutrition facts label in chronic disease management: results from the National Health and Nutrition Examination Survey. J Am Diet Assoc. 2010;110(4):628–32. https://doi.org/10.1016/j.jada.2009.12.015
Jacobs DR Jr, Tapsell LC. Food, not nutrients, is the fundamental unit in nutrition. Nutr Rev. 2007;65(10):439–50. https://doi.org/10.1111/j.1753-4887.2007.tb00269
Greenberg ER, Baron JA, Karagas MR, et al. Mortality associated with low plasma concentration of beta carotene and the effect of oral supplementation. JAMA. 1996;275(9):699–703. https://doi.org/10.1001/jama.1996.03530330043027
Egnell M, Boutron I, Péneau S, et al. Impact of the nutri-score front-of-pack nutrition label on purchasing intentions of individuals with chronic diseases: results of a randomised trial. BMJ Open. 2022;12(8):e058139. https://doi.org/10.1136/bmjopen-2021-058139
NCD Risk Factor Collaboration (NCD-RisC). Repositioning of the global epicentre of non-optimal cholesterol. Nature. 2020;582(7810):73–7. https://doi.org/10.1038/s41586-020-2338-1
Bowry AD, Lewey J, Dugani SB, Choudhry NK. The Burden of Cardiovascular Disease in Low- and Middle-Income Countries: Epidemiology and Management. Can J Cardiol. 2015;31(9):1151–9. https://doi.org/10.1016/j.cjca.2015.06.028
Silva ARC, Guandalini VR, Pereira TSS et al. Association between Dietary Inflammatory Index and Gastric Adenocarcinoma: A Multicenter Case-Control Study in Brazil. Nutrients. 2023;15(13):2867. Published 2023 Jun 24. https://doi.org/10.3390/nu15132867
Wang L, Wang X, Sun M, et al. Oral health and 10-year cardiovascular risk in US adults: mediating role of inflammatory diet and vitamin D. Clin Oral Investig. 2023;27(7):3405–13. https://doi.org/10.1007/s00784-023-05097-w
Acknowledgements
Thanks to Zhang Jing (Shanghai Tongren Hospital) for his work on the NHANES database. His outstanding work makes it easier for us to explore the NHANES database.
Funding
This work was supported by National Natural Science Foundation of China (82174130;82274262), and Program of Shanghai Municipal Health Commission (202240053).
Author information
Authors and Affiliations
Contributions
Xiaozhe Chen, Bo Lu, Chunlei Hou, Xunjie Zhou conceived the ideas and design of the study. Xiaozhe Chen, and Chunlei Hou collected data from NEHANES. Lei Yao, Jianhua Li, and Xunjie Zhou analyzed the data. Mingtai Gui, Lei Yao, and Xiaozhe Chen drafted the manuscript. Deyu Fu and Mingzhu Wang revised the final version of the manuscript and supervised the study. Xiaozhe Chen and Chunlei Hou contributed equally to this study and share the first authorship. Bo Lu and Deyu Fu share the correspondence. All authors have read and approved the final version of the manuscript for publication.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the National Centre for Health Statistics Research Ethics Review Board.
Consent for publication
All individuals signed an informed consent form.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, X., Hou, C., Yao, L. et al. Dietary inflammation index is associated with dyslipidemia: evidence from national health and nutrition examination survey, 1999–2019. Lipids Health Dis 22, 149 (2023). https://doi.org/10.1186/s12944-023-01914-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-023-01914-z