
Abstract
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) is one of the most important nosocomial pathogens and is also emerging in Turkish hospitals. The aim of this study was to determine the antimicrobial susceptibility profiles of MRSA isolated from Turkish hospitals.
Materials and methods
A total of 397 MRSA strains isolated from 12 hospitals in Turkey were included to present study. Antimicrobial susceptibilities were tested using agar dilution method. Presence of ermA, ermB, ermC, msrA, tetM, tetK, linA and aac-aph genes were studied by PCR.
Results
All strains were susceptible to vancomycin and linezolid. The susceptibility rates for fusidic acid, lincomycin, erythromycin, tetracyclin, gentamycin, kanamycin, and, ciprofloxacin were 91.9%, 41.1%, 27.2%, 11.8%, 8.5%, 8.3% and 6.8%, respectively. Lincomycin inactivation was positive for 3 isolates. Of 225 erythromycin resistant isolates 48 had ermA, 20 had ermC, and 128 had ermA-C. PCR was negative for 15 strains. Of 3 isolates with lincomycin inactivation one had linA and msrA. Of 358 gentamycin resistant isolates 334 had aac-aph and 24 were negatives. Among 350 tetracyclin resistant isolates 314 had tetM. Of 36 tetM negative isolates 10 had tetK.
Conclusion
MRSA isolates from Turkish hospitals were multiresistant to antimicrobials. Quinolone and gentamycin resistance levels were high and macrolide and lincosamide resistance were relatively low. Susceptibility rates for fusidic asid were high. Linezolide and vancomycin resistance are not emerged. The most common resistance genes were ermA, tetM and aac-aph. Evolution of antimicrobial susceptibilities and resistance genes profiles of MRSA isolates should be surveyed at regional and national level for accurate treatment of patients and to control dissemination of resistance genes.
Similar content being viewed by others

Introduction
Staphylococci are important infection agents that cause hospital and community acquired infections. These bacteria have ability to adapt themselves to difficult conditions and successful clones have capacity of epidemic and pandemic dissemination [1]. Increasing resistance problem in staphylococci became an important public health problem. In 1944 when penicillin became available for use the susceptibility rate of Staphylococcus aureus to penicillin was >94% which became <5% recently [2]. Methicillin resistance appeared and started to disseminate from 1980 and became one of the major problem in hospital infections. Methicillin resistance is due to acquisition of a transpeptidase, PBP2a, involved in cell wall synthesis that has low affinity for beta lactam antibiotics which rends bacteria resistant to all beta lactam antibiotics. Treatment of infections due to methicillin resistant S. aureus (MRSA) causes problems due to restricted number of choices [1]. Especially from 2003, when vancomycin resistant S. aureus emerged it became urgent to search new treatment possibilities for these bacteria [3]. In addition emergence and dissemination of community MRSA isolates forced to evaluate empiric treatment options in consideration with changing resistance profiles of these bacteria. MRSA strains do not affect only human but also infect farm animals and pets [4]. Although development of new antibiotics reduced dramatically recently, some antibiotics like daptomycin, linezolid and tigecyclin could be commercialized lately [1].
In the present study susceptibilities of 397 MRSA isolated from 12 centers in Turkey to linezolid, fusidic acid, kanamycin, gentamycin, erythromycin, lincomycin, tetracyclin, vancomycin and ciprofloxacin were tested by agar dilution method and presence known resistance genes were verified by PCR using specific primers.
Materials and methods
A total of 12 centers from 11 cities participated to the present study and sent MRSA isolates to Aydın where susceptibility testing and molecular studies were done at ADU BILTEM Epidemiology Unit. Methicillin resistance was confirmed by cefoxitin disc method. A total of 397 MRSA isolates were collected from hospitalized patients between 2006-2008, from Aydın (15 isolates), İzmir(2 centres 17 and 22 isolates), Afyon (32), Manisa (23), Van (42), Trabzon (54), Samsun (51), Ankara (31), Konya (28), Istanbul (55), and Edirne (36).
Determination of antimicrobial susceptibilities
Agar dilution method
Antibiotics tested were linezolid, fusidic acid, kanamycin, gentamycin, erythromycin, lincomycin, tetracyclin, vancomycin and ciprofloxacin. Erythromycin and fusidic acid were from Koçak Farma (Tekirdağ, Türkiye), kanamycin, tetracyclin and vancomycin were purchased from Sigma, and commercial injectable preparations were used for the remaining antimicrobials. Agar dilution method was used as described previously [5]. Shortly plates were prepared with serial dilution from 64 or 128 mg/L antibiotic concentrations. Inoculum with 5X104 bacteria was placed onto agar using multipoint inoculator. After 16-20 h incubation at 37°C the lowest concentration that inhibits bacterial growth was accepted as MIC. Reference strain S. aureus RN4220 was included to each run.
Gots test
All lincomycin resistant isolates were tested by Gots’ test for presence of resistance by antibiotic inactivation. For this purpose to 19 ml agar at 50-60°C 19 ml BHI (Brain Heart infusion) agar 0,5 mg/L clindamycin and 1 ml overnight broth of Micrococcus luteus ATCC9341 were added, mixed and poured to petri dish and left for solidification. The MRSA isolates were inoculated as small round onto agar. On one plate approximately 20 MRSA isolates were inoculated. After 24 h incubation at 37°C plates were left 24 h at room temperature. Growth of indicator bacteria in the round of tested bacteria was accepted as positive which showed presence of resistance mechanism by inactivation [6].
Determination of resistance mechanisms
DNA extraction
DNA extraction was done using Instagen Matrix (BioRad) as recommended by manufacturer. Shortly 1-2 colonies were homogenized in 1 ml of distillated water and centrifuged at 10000 rpm for 1 minute. Supernatant were discarded and pellet was homogenized with 100 μl of instagen matrix. After incubation at 55′C during 15-30 min the mixture was vortexed and incubated at 95′C during 8 min. Lysate were centrifuged and 2 μl of supernatant were used as DNA for PCR reactions.
PCR
Erythromycin, lincomycin, gentamycin and tetracyclin resistant MRSA isolates were tested for the presence of msrA, ermA, ermB, ermC, linA, linB, aac-aph, tetM and tetK genes by PCR using specific primers. List of the primers and PCR conditions are shown in Table 1[7]-[11].
Results
Susceptibilities to antibiotics
MICs and resistance was evaluated using CLSI criteria [12]. All 397 MRSA isolates tested were found to be susceptible to vancomycin and linezolid. Only 8 of 397 MRSA isolates were susceptible to all antibiotics tested. In Table 2 MIC50 and MIC90 of the isolates are shown for each antibiotic tested. The number of resistant isolates to erythromycin, lincomycin, tetracyclin, gentamycin, fusidik acid, ciprofloxacin and kanamycin were 225 (%56.7), 168 (%42.3), 350 (%88.2), 358 (%90.2), 32 (%8.1), 366 (%92.2), and 363 (%91.4), respectively (Table 3). Distribution of resistance levels for the antibiotics for each centre is shown at Table 4.
Resistance mechanisms
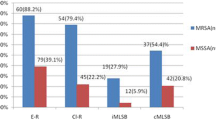
Of 225 erythromycin resistant MRSA isolates 48 carried ermA, 20 carried ermC, 1 carried both ermA and ermB, 1 carried both ermB and ermC, 128 carried both ermA and ermC, 2 carried ermA, ermB and ermC, 2 carried msrA, 2 carried msrA and ermA, 1 had msrA and ermB, 4 had msrA, ermA and ermC, 1 had msrA and ermC genes. A total of 15 isolates were negatives for all erythromycin resistance genes tested. Among MRSA isolates 64 were intermediate resistant to erythromycin. Of these isolates 36 were positive for ermA, 1 isolate had both ermA and ermC, and 1 isolate was positive for msrA. All remaining 26 isolates were negatives for the genes tested. Among 168 lincomycin resistant isolates 9 had ermA, 17 had ermC, 1 had both ermA and ermB, 1 had both ermB and ermC, 124 had both ermA and ermC, 4 had msrA, ermA and ermC, 2 had ermA, ermB and ermC, 1 had linA and msrA, 1 had ermC and msrA genes found and 8 isolates were negative by PCR for the genes tested. All lincomycin resistant isolates were tested for clindamycin inactivation by Gots’ test and 3 isolates were found to be positive for inactivation. Of these 3 isolates one carried linA gene responsible for lincosamide inactivation and also msrA gene, but remaining 2 isolates were negatives for both linA and linB genes.
Among macrolide resistant isolates the most frequently encountered gene was ermA (185 isolates) folloved by ermC (157 isolates), msrA (10 isolates) and ermB (9 isolates).
A total of 358 isolates were resistant to gentamycin and 334 of these isolates were positive for aac-aph gene and remaining 24 isolates were negative for this gene.
It was found that 350 of 397 isolates were resistant to tetracyclin. Of these 350 isolates 314 carried tetM gene and 36 did not carry this gene. Among tetM negative 36 isolates 10 had tetK gene and remaining 26 isolates were negative both tetM and tetK. Distribution of resistance genes among resistant isolates are shown in Table 5. Among macrolide resistance isolates the most common gene combination was ermA-ermC. Among tetracyclin and gentamycin resistant isolates the most common resistant genes were tetM and aac-aph, respectively.
Discussion
Antibiotic resistance became an important public health problem in Turkey as it is in whole world. Restriction of beta lactam use in MRSA isolates required use of other types of antibiotics for the treatment of infections due to MRSA isolates so survey of susceptibilities of MRSA isolates for antibiotics other than beta lactams became very important.
Our study is the largest study done in Turkey which evaluates both phenotypic and genotypic aspect of antimicrobial resistance among MRSA. A study done in Harran University, Urfa at 2004 indicated that erythromycin, clindamycin, gentamycin and ciprofloxacin resistant among MRSA isolates 63%, 50%, 81% and 25%, respectively [13]. Other study done at Manisa, at 2007 evaluated resistance of MRSA isolated from 1998 to 2002 [14]. It was shown that erythromycin resistance decreased from 59.5% to 51%, clindamycin resistance increased from 28.4% to 41.5%, tetracyclin resistance increased from 57.6% to 88%, and gentamycin resistance from 28.4% to% 87.5, ciprofloxacin resistance from 34.1% to 92.2%. Our study confirmed the tendency for increase in the resistance level of ciprofloxacin, tetracyclin and gentamycin. Sarıbas et al. investigated macrolide resistance genes among MRSA isolates and showed that macrolide resistance level was 29.9% and 86% of the resistant isolates carried ermA gene [15]. Sarıbaş et al. found resistance level lower than our study and other studies from Turkey however resistance gene profile was similar with 86% of ermA gene but in our study more than 50% of ermA positive isolates also carried ermC gene. Gül et al. evaluated erythromycin resistance rate among MRSA isolated between 2003′2006 and found resistance rate as 84.9% [16]. Of resistant isolates 37.7% had ermA 26.6% had ermC and 18.6% had both ermA and ermC[16]. Aktaş et al. studied 22 erythromycin resistant MRSA isolated in Istanbul and found thet the most frequent genotype was presence of both ermA and ermC 40.9(%) followed by ermC (18.2%) [17]. Ardıç et al. also found among 28 erythromycin resistant MRSA that presence of both ermA and ermC was the most frequent genotype [18].
In the world among erythromycin resistant MRSA isolates ermA was the most frequent gene in France (57.6%) [10], Colombia (78.5%) [19] and Malesia (52.8%) [20] but in Greece which is neighbour of Turkey ermC (96.5%) [21] found to be the most frequent gene.
In our study the most frequent mechanism of macrolide resistance among MRSA isolates found to be presence of methylase. Presence of methylase may confer inducible lincomycin resistance which should be taken in consideration for treatment design. The dominant genes among tetracyclin and aminoglycoside resistant isolates were tetM and aac-aph, respectively.
The dissemination of resistance was also analysed at regional level. İsolates from Istanbul had lower tetracycline resistance than other regions. MRSA isolates from Van had higher macrolide resistance rates than other regions. Ciprofloxacin resistance rates were very high in all centers and the lowest rate was in Trabzon with 74% and highest rates were in Aydın, Ankara and İzmirwith 100%. Tetracyclin resistance was lowest in Istanbul with 52.7% and highest in Ankara with 100%. Fusidic acid resistance rates were relatively low. All isolates from Ankara, Aydın and Manisa were susceptible to fusidic acid, and highest resistance rate was in Afyon with 21.7%. Erythromycin resistance was lowest at Van with 4.7% and highest at Konya with 89.3%. At the same time Konya was the center where the resistance rate differences were the highest between erythromycin and lincomycin. Resistance rates were the lowest in Afyon and Samsun with <50%. Lincomycin resistance rate was 46.2%. Resistance to gentamycin was lowest in Trabzon with 68.5% and highest in Istanbul with 96.3%.
In our study the most common gentamycin resistance gene was aac-aph gene (96%). Ardıç et al. studied with 17 gentamycin resistant MRSA isolates from Istanbul at 2006 and found 16 of 17 (94,1%) isolate carried aac-aph gene [22]. A study from Iran, neighbour state of Turkey, showed that isolates from Tehran aac-aph gene was the most common gene among gentamycin resistant S. aureus (83%) [23]. Tetracyclin resistance gene tetM was 90% positive among tetracyclin resistant isolates which were only 49% among resistant isolates from Malesia [20].
Conclusion
Our study is one of the largest epidemiological study done in Turkey. These multi-centre data of resistance level and mechanism of resistance of MRSA isolates will be important for future surveillance studies to determine the evolution of resistance levels and mechanisms at national and regional level. Also our results and follow up studies may constitute a database for empirical treatment of infections due to MRSA. Our multicentre study showed that isolates from 12 centres from Turkey had multiple resistances. Quinolone and gentamycin resistance found to be very high. Fusidic acid resistance was low and erythromycin and lincomycin susceptibility found to be relatively high. This study indicated that resistance to linezolid and vancomycin resistance is not emerged among MRSA isolates from Turkish hospitals.
Authors' contributions
AYÇ, AGS, SAC, GB, HG, MÖ, MTO, NK, NÖ, OA, SÖ and UA participated of collection and identification of MRSA isolates. MIC testing and genetic studies were done by ÖY and BB, and manuscript draft was prepared by ÖY and BB. All authors read and approved the final manuscript.
References
Gould IM, David MZ, Esposito S, Garau J, Lina G, Mazzei T, Peters G: New insights into meticillin-resistant Staphylococcus aureus (MRSA) pathogenesis, treatment and resistance. Int J Antimicrob Agents. 2012, 39 (2): 96-104. 10.1016/j.ijantimicag.2011.09.028.
Neu HC: The crisis in antibiotic resistance. Science. 1992, 257: 1064-1068. 10.1126/science.257.5073.1064.
Bozdogan B, Ednie L, Credito K, Kosowska K, Appelbaum PC: Derivatives of a vancomycin-resistant Staphylococcus aureus strain isolated at Hershey Medical Center. Antimicrob Agents Chemother. 2004, 48 (12): 4762-4765. 10.1128/AAC.48.12.4762-4765.2004.
Türkyılmaz S, Tekbıyık S, Oryasin E, Bozdogan B: Molecular Epidemiology and Antimicrobial Resistance Mechanisms of Methicillin-Resistant Staphylococcus aureus Isolated from Bovine Milk. Zoonoses Public Health. 2010, 57: 197-203. 10.1111/j.1863-2378.2009.01257.x.
Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard-Ninth Edition. 2012, Clinical and Laboratory Standards Institute, CLSI document M29-A3 ISBN 1-56238-784-7,
Gots JS: The detection of penicillinase production properties of microorganisms. Science. 1945, 102: 309-10.1126/science.102.2647.309.
Sutcliffe J, Grebe T, Tait-Kamradt A, Wondrack L: Detection of erythromycin-resistant determinants by PCR. Antimicrob Agents Chemother. 1996, 40: 2562-2566.
Kao SJ, You I, Clewell DB, Donabedian SM, Zervos MJ, Petrin J, Shaw KJ, Chow JW: Detection of the high-level aminoglycoside resistance gene aph(2")-Ib in Enterococcus faecium. Antimicrob Agents Chemother. 2000, 44: 2876-2879. 10.1128/AAC.44.10.2876-2879.2000.
Warsa UC, Nonoyama M, Ida T, Okamoto R, Okubo T, Shimauchi C, Kuga A, Inoue M: Detection of tet(K) and tet(M) in Staphylococcus aureus of Asian countries by the polymerase chain reaction. J Antibiot. 1996, 49: 1127-1132. 10.7164/antibiotics.49.1127.
Lina G, Quaglia A, Reverdy ME, Leclercq R, Vandenesch F, Etienne J: Distribution of genes encoding resistance to macrolides, lincosamides, and streptogramins among staphylococci. Antimicrob Agents Chemother. 1999, 43: 1062-1066.
Bozdogan B, Berrezouga L, Kuo MS, Yurek DA, Farley KA, Stockman BJ, Leclercq R: A new resistance gene, linB, conferring resistance to lincosamides by nucleotidylation in Enterococcus faecium HM1025. Antimicrob Agents Chemother. 1999, 43: 925-929.
Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically, 6th ed. Approved standard M7-A6. 2003, Clinical and Laboratory Standards Institute, Wayne, PA
Sırmatel F, Yıldız Zeyrek F, Erkmen O: Antibiotic resistance in nosocomial Staphylococcus strains with broth microdilution method. ANKEM Derg. 2004, 18: 200-204.
Kurutepe S, Sürücüoülu S, Gazi H, Teker A, Özbakkaloğlu B: Antibiotic resistance rates of methicillin resistant and susceptible Staphylococcus aureus strains. Turk J Infect. 2007, 21: 187-191.
Sarıbaş Z, Tunçkanat F, Özçakır O, Ercis S: Investigation of macrolide-lincosamide-streptogramin B (MLS(B)) and telithromycin resistance in clinical strains of staphylococci. Mikrobiyol Bul. 2010, 44: 177-186.
Gul HC, Kilic A, Guclu AU, Bedir O, Orhon M, Basustaoglu AC: Macrolide-lincosamide-streptogramin B resistant phenotypes and genotypes for methicillin-resistant Staphylococcus aureus in Turkey, from 2003 to 2006. Pol J Microbiol. 2008, 57: 307-312.
Aktas Z, Aridogan A, Kayacan CB, Aydin D: Resistance to macrolide, lincosamide and streptogramin antibiotics in staphylococci isolated in Istanbul, Turkey. J Microbiol. 2007, 45: 286-290.
Ardic N, Ozyurt M, Sareyyupoglu B, Haznedaroglu T: Investigation of erythromycin and tetracycline resistance genes in methicillin-resistant staphylococci. Int J Antimicrob Agents. 2005, 26: 213-218. 10.1016/j.ijantimicag.2005.06.013.
Reyes J, Hidalgo M, Díaz L, Rincón S, Moreno J, Vanegas N, Castañeda E, Arias CA: Characterization of macrolide resistance in Gram-positive cocci from Colombian hospitals: a countrywide surveillance. Int J Infect Dis. 2007, 11: 329-336. 10.1016/j.ijid.2006.09.005.
Lim KT, Hanifah YA, Yusof MYM, Thong KL: ermA, ermC, tetM and tetK are essential for erythromycin and tetracycline resistance among methicillin-resistant Staphylococcus aureus strains isolated from a tertiary hospital in Malaysia. Indian J Med Microb. 2012, 30: 203-207. 10.4103/0255-0857.96693.
Spiliopoulou I, Petinaki E, Papandreou P, Dimitracopoulos G: erm(C) is the predominant genetic determinant for the expression of resistance to macrolides among methicillin-resistant Staphylococcus aureus clinical isolates in Greece. J Antimicrob Chemother. 2004, 53: 814-817. 10.1093/jac/dkh197.
Ardic N, Sareyyupoglu B, Ozyurt M, Haznedaroglu T, Ilga U: Investigation of aminoglycoside modifying enzyme genes in methicillin-resistant staphylococci. Microbiol Res. 2006, 161: 49-54. 10.1016/j.micres.2005.05.002.
Fatholahzadeh B, Emaneini M, Feizabadi MM, Sedaghat H, Aligholi M, Taherikalani M, Jabalameli F: Characterisation of genes encoding aminoglycoside-modifying enzymes among meticillin-resistant Staphylococcus aureus isolated from two hospitals in Tehran, Iran. Int J Antimicrob Agents. 2009, 33: 264-265. 10.1016/j.ijantimicag.2008.09.018.
Acknowledgement
This study was supported by grant TPF09025 from Adnan Menderes University BAP.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interest.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Yıldız, Ö., Çoban, A.Y., Şener, A.G. et al. Antimicrobial susceptibility and resistance mechanisms of methicillin resistant Staphylococcus aureusisolated from 12 Hospitals in Turkey. Ann Clin Microbiol Antimicrob 13, 44 (2014). https://doi.org/10.1186/s12941-014-0044-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12941-014-0044-2