
Abstract
Background
Chronic lung diseases are characterized by impaired lung function. Given that many diseases have shared clinical symptoms and pathogenesis, identifying shared pathogenesis can help the design of preventive and therapeutic strategies. This study aimed to evaluate the proteins and pathways of chronic obstructive pulmonary disease (COPD), asthma, idiopathic pulmonary fibrosis (IPF), and mustard lung disease (MLD).
Methods and results
After collecting the data and determining the gene list of each disease, gene expression changes were examined in comparison to healthy individuals. Protein–protein interaction (PPI) and pathway enrichment analysis were used to evaluate genes and shared pathways of the four diseases. There were 22 shared genes, including ACTB, AHSG, ALB, APO, A1, APO C3, FTH1, GAPDH, GC, GSTP1, HP, HSPB1, IGKC, KRT10, KRT9, LCN1, PSMA2, RBP4, 100A8, S100A9, TF, and UBE2N. The major biological pathways in which these genes are involved are inflammatory pathways. Some of these genes activate different pathways in each disease, leading to the induction or inhibition of inflammation.
Conclusion
Identification of the genes and shared pathways of diseases can contribute to identifying pathogenesis pathways and designing preventive and therapeutic strategies.
Similar content being viewed by others


Introduction
Lung is a basic organ regulating and maintaining the function of the respiratory tract [1, 2]. Recent data have shown that respiratory disorders affect many people in the USA (35 million people, most of whom deal with asthma and chronic obstructive pulmonary disease (COPD)). This disorder leads to various diseases in patients, which are associated with many deaths [3]. A rise in the mortality of patients due to respiratory disorders is a major global challenge that necessitates the identification of the pathogenesis of diseases and the use of preventive and therapeutic strategies [4].
There is a wide range of chronic lung diseases which overlap in terms of clinical symptoms and are difficult to distinguish [5]. In addition, disease pathogenesis is multifactorial, and the main cause of chronic lung disease has not yet been identified. Some chronic lung diseases, including COPD, asthma, idiopathic pulmonary fibrosis (IPF), and mustard lung disease (MLD) have shared clinical symptoms such as mucus secretion, cough, impaired lung function, and dyspnea.
Recent evidence suggests that inflammation is shared in all the four mentioned diseases, leading to disease progression. The chemotaxis of immune cells and their cytokine production are the other factors in the pathogenesis of diseases [1, 6,7,8]. However, in COPD and MLD, inflammation stimulates the immune system and coagulation factors’ secretion, which ultimately causes coagulation in patients [9, 10]. Inflammation in asthma causes T cells to differentiate into T helper2 (Th2), and eventually produces a series of cytokines, including IL-5 and IL-13, which lead to mucus production and secretion in patients [11]. In IPF, inflammation leads to TGF-β production, a cytokine that causes pulmonary fibrosis in patients [12].
Protein–protein interaction (PPI) handles a wide range of genes and proteins and creates a network between them in cellular communication [13]. In fact, gene ontology (GO) shows the molecular pathways, cellular functions, and biological processes of each gene and protein in a disease. In other words, PPI depicts the network created between genes and proteins, as well as the commonalities between them in cellular communication [14,15,16].
Lung involvement is a shared pathogenesis and identical genes and molecular pathways are involved in the pathogenesis of the four diseases. Gene study has been evaluated individually in chronic lung diseases, and no study has assessed the expression of shared genes and proteins in several diseases. Thus, the present study evaluated the association between genes and shared proteins in COPD, asthma, IPF, and MLD. Biological pathways, cellular components, and molecular functions of proteins were also examined.
Materials and methods
Data collection
PubMed, Scopus, ISI Web of Science, and Cochrane databases were used to collect the data. All relevant studies were extracted and evaluated. Only case–control studies were included. Protein expression changes (increase or decrease) were measured compared to the control group. All the proteins were selected from proteomics studies. After data extraction, duplicates and missing data were deleted.
After identifying the relevant articles and extracting the studied genes, dysregulation was found in the expression of 13,940 genes in COPD, 2700 genes in asthma, 6686 genes in IPF, and 104 genes in MLD. A list of all the genes with fold change, p-value, and FDR is presented in Supplementary S1. For some genes, p-value, fold change, or FDR were not reported. After removal of duplicates, 6,348 genes in COPD, 1,597 genes in asthma, 5,272 genes in IPF, and 76 genes in MLD had up- or down-regulation. Then, using Genes Set, enrichment pathways involved in GO were identified (Fig. 1). The pathways with the highest score in which more genes were involved were then selected (Fig. 2).

Workflow of data collection and analysis of genes and pathways

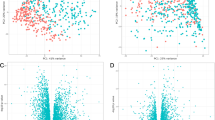
Scheme of total protein in COPD, asthma, IPF, and MLD
Based on the screened studies, proteins identified as having different expressions under varying processing conditions within each study were also considered. The studies included COPD (n = 49), asthma (n = 23), IPF (n = 25), and MLD (n = 6). Furthermore, some studies only listed the proteins that showed expression changes without indicating the extent of these changes. Therefore, in this study, no threshold level for protein expression variations was established.
Protein Interaction Network
To draw the protein interaction network, all the data were combined in a database; then, https://string-db.org/ was used for analysis. Physical and molecular interactions between proteins were identified and extracted. Finally, all data, networks and relationships between proteins were entered to Cytoscape (https://cytoscape.org/). Finally, the hub genes with the highest degree were identified using network analyzer packages.
Shared gene and pathway analysis
Shared genes of the mentioned diseases were examined. Diseases were also classified into three and two groups, and the shared genes were evaluated. Also, enrichment analysis was performed for the diseases individually and together (Figs. 3 and 4).

Scheme of the number proteins shared by the diseases. A number of proteins between MLD, asthma and IPF, B number of proteins between COPD, asthma and IPF, C number of proteins between COPD, asthma and MLD, D number of proteins between IPF, COPD and MLD

Scheme of 22 proteins shared by COPD, asthma, IPF and MLD. The nodes' size and color indicate the number of interactions they have with other proteins. Hence, a node with a larger size and a redder color indicates more interactions and points with other proteins, whereas a smaller and greener indicate a lower degree of that node
Enrichment analysis
FunRich (http://www.funrich.org) was used to evaluate the gene ontology enrichments of the listed genes. These data were used to evaluate biological and molecular similarities of the genes.
Results
This study examined shared genes and their associated biological pathways among four chronic lung diseases (COPD, IPF, asthma, and MLD) using PPI networks and enrichment analysis. In addition, changes in gene expression in each disease were identified separately. The role of genes in cellular metabolism and the biological processes involved in lung pathogenesis were also investigated.
Similarity analysis for disease genes
The genes shared by the diseases were examined. For this purpose, genes shared by the diseases were studied in two and three groups. In the ternary group, there were 763, 24, 24, and 39 genes shared by COPD-asthma-IPF, COPD-asthma-MLD, asthma-IPF-MLD and IPF-MLD-COPD, respectively. Genes shared between the three diseases are shown in a Venn diagram (Fig. 3). In the pair groups, there were 815, 3475, 55, 1346, 26, and 42 genes shared between COPD-asthma, COPD-IPF, COPD-MLD, asthma-IPF, asthma-MLD and IPF-MLD, respectively. Moreover, 22 genes were shared by the four diseases (Fig. 4). Table 1 lists these 22 genes along with their up- or down-regulation in each disease. Using Enrichr, interactions between unique proteins in each disease were designed. Further evaluations showed that the GRB2 gene in both COPD and MLD and the ESR1 and IRF7 genes in asthma and IPF had the highest association with the other genes, respectively (Supplementary file S2). The names of unique proteins in each disease, along with their interaction information with other proteins, are reported in Supplementary file S3.
Gene ontology and enrichment analysis
Gene enrichment analysis is a method for analyzing molecular and biological processes between diseases. In addition, gene ontology evaluates biological processes, cellular components, and molecular functions using the FunRich software. This tool identifies GO and biological pathways between shared disease genes. P-value < 0.05 was considered as a standard metric for high-score biological pathways.
Evaluation of hub proteins
The PPI network was determined using STRING. Then, using Cytoscape, the molecular pathways and interactions between the shared genes were drawn. The PPI network derived from the shared genes was displayed as nodes and edges based on the degree of importance and interactions. The genes with a high score were selected as the hub. These hub genes can be known as biomarkers, based on which preventive and therapeutic strategies can be designed (Fig. 5).

Scheme of shared proteins in diseases. A proteins shared by COPD, asthma and IPF, B proteins shared by COPD, asthma and MLD, C proteins shared by COPD, IPF and MLD, D proteins shared by IPF, asthma, and MLD. The size and color of the nodes correspond to the number of interactions they have with other proteins. Thus, a node with a larger size and a redder color indicates more interactions and scores with other proteins, whereas a smaller size and a greener color indicate a lower degree of that node
Shared biological process and Reactome pathway
With a more detailed evaluation, most of the genes and molecular pathways involved in GO and the biological process were identified. The main biological processes included neutrophil degranulation, innate immune response, post-translational protein modification, and retina homeostasis, while the main Reactome pathways included neutrophil degranulation, platelet degranulation, post-translational protein phosphorylation, and retinoid metabolism and transport (Table 2).
Discussion
Lung disorders are among the most shared diseases and are characterized by impaired lung function. There is a wide range of lung diseases whose clinical symptoms overlap; therefore, it is difficult to distinguish them from one another [17]. Shared genes or pathways that can be used to treat these diseases had not previously been identified [18]. In this study, we first examined the genes and pathways shared by four chronic diseases (COPD, IPF, asthma, and MLD). Based on the systems biology approach and using enrichment analysis, we examined the genes and biological pathways shared by the cited disorders. In this section, we first evaluate the biological pathways, in which 22 genes shared by the four diseases are involved, and then assess the shared biological pathways in triplicate.
Haptoglobin (HP) is a factor involved in hemoglobin metabolism. It has also been shown to be involved in the pathogenesis of chronic lung diseases. CD163 is known as the HP receptor. The interaction between HP and CD163 increases the expression of heme oxygenase-1 (HO-1), which reduces inflammation and oxidative stress [19]. CD163 has also been shown to differentiate macrophage type 2 (M2) which, in turn, decreases inflammation in COPD. Considering the role of the MAPK / cAMP / PI3K / AKT pathway in M2 differentiation, CD163 probably causes M2 differentiation by activating this pathway [20]. In asthma patients, the interaction between HDAC8 / Gal3 increases the CD163 expression; therefore, given the role of CD163 in M2 differentiation, and the role of M2 cells in Th2 differentiation, CD163 in asthma can be considered as a target for the targeted therapy route [21].
S100 A8 / A9 was another factor shared by the four diseases. In COPD, S100A8 plays a cyto-protective role. In other words, PKA / cAMP prevents inflammation and the production of reactive species oxygen (ROS). In COPD, S100A8 is dephosphorylated and degraded by SYVN1, which eventually leads to the apoptosis of lung cells [22]. Some studies have reported that S100A8 activates NF-KB through MUC5AC expression, which ultimately increases NLRP3 activation and inflammatory cytokines’ production [23]. Therefore, S100A8 acts as a double-edged sword in COPD. Identifying the pathways involved in pathogenesis and treatment can be effective for designing treatments.
In IPF, an increase in S100A8 triggers inflammatory cytokines’ production by activating TLR4. Moreover, in asthma, it causes inflammation by activating the PI3K / AKT / MAPK / NF-kB pathway [24]. In asthma, the SERPINB3 / B4 complex increases S100A8 production and inflammation by activating P38 / MAPK. S100A8; in addition to causing inflammation through molecular pathways, it can raise the production of complement C3, which is a component of the inflammatory system [25]. This study found that S100A8 / A9 expression was higher in all four diseases compared to controls; since this protein is involved in inflammation and cellular protection, identifying pathways that lead to cellular protection of S100A8 / A9 against inflammation can be a therapeutic route.
C3 increases cell survival by activating the mTOR pathway. In COPD, an increase in C3 leads to CD46 expression. CD46 activates STAT1 and, eventually, BCL-2 by forming a complex with CD3. BCL-2 expression prevents cell apoptosis. In addition, C3 expression in COPD increases the apoptosis of cytotoxic TCD8 cells, which prevents inflammation [26]. C3 expression is increased in COPD patients; therefore, C3 targeting can be a good treatment strategy. In asthma, an increase in C3 leads to innate lymphoid cell chemotaxis (ILC2), which ultimately raises the production of IL-4 and IL-13 and causes inflammation. C3 also increases the expression of CCL2 and CCL5 chemokines by activating the ERK1,2 / MAPK pathway. The expression of these chemokines leads to mast cell chemotaxis and inflammation. On the other hand, adenosine reduces the chemotaxis of mast cells to inflammation site by inhibiting ERK1,2 / MAPK [27, 28].
In IPF, C3 produces IL-17, which eventually causes pulmonary fibrosis through TGF-β / P38 / MAPK. C3 also causes pulmonary fibrosis due to MUC5B expression. Furthermore, TGF-β has been shown to inhibit C3 by inhibiting CD46 and CD55. Therefore, TGF-β, despite causing pulmonary fibrosis in IPF, can prevent inflammation and pulmonary fibrosis in patients by reducing C3 production [29,30,31]. MLD have also been found to cause C3 inflammation and disease progression and, ultimately, it reduces patient survival [32]. Since C3 expression is decreased in asthma, IPF, and MLD, identifying pathways that reduce its expression can be effective in treatment.
Apolipoprotein A1 (APO A1) is another factor with a dual role; it plays an effective role in the progression and prevention of lung damage due to inflammation by regulating different pathways. In COPD, APOA1 reduces ROS production by NADPH oxidase and NOX3 expression [33]. It also inhibits apoptosis in lung cells by inhibiting NF-κB and Caspase8. In asthma, APO A1 expression inhibits inflammation by inhibiting ERK / NF-κB. It also prevents lung damage and dysfunction by expressing Lipoxin A4 (LXA4) [33, 34]. Moreover, it reduces the chemotaxis of neutrophils to the inflammation site by lowering the VCAM-1 and CXCL5 expression. Ultimately, it decreases TGF-β production [35]. Decreased TGF-β can reduce Th2 differentiation and produce IL-4 and IL-13. In IPF, APO A1 lowers the TGF-β production. TGF-β causes pulmonary fibrosis in patients through the ERK / MAPK pathway. It also reduces M2 differentiation and TGF-β production by decreasing the IL-4 production [36, 37]. Since APOA1 has an anti-inflammatory role and, in this study, its expression had increased in some diseases, identifying the pathways leading to its increased expression can contribute to designing therapeutic methods to prevent inflammation.
CD74 is known as transferrin receptor (TF). TF is involved in the regulation of inflammation and ROS production due to iron metabolism. In COPD, CD74 inhibits macrophage migration inhibitory factor (MIF) expression. MIF generates ROS via the ASK1 / P38 / XOR pathway [38]. CD74 hinders lung cell apoptosis by inhibiting P53 and activating the ERK / MAPK / AKT pathway [38]. Inhibition of MIF expression by reducing NF-κB inhibition and M2 cell differentiation alleviates inflammation [39]. In asthma, MIF induces CCl2, CXCR2, and CXCR4 expression through the ERK / MAPK / P38 / Rho A GTPase pathway. The expression of this chemokine causes the chemotaxis of immune cells and inflammation in patients [40].
Heat shock protein (HSP) has been shown to inhibit MIF. In COPD, increased HSP expression inhibits JNK / NF-κB and prevents inflammation. HSP has also been shown to increase inflammation through the TLR4 / MAPK / NF-kB pathway [41]. Activation of the MMK3 / P38 / NF-kB / Rel A pathway also raises the HSP expression [42]. In asthma, HMGB1 expression induces HSP expression through the TLR4 / MYD88 / NF-kB pathway, which eventually produces IL-4 and IL-13. The generation of these cytokines leads to Th2 differentiation and disease progression [43, 44]. Other studies have reported that HSP induces immune cell chemotaxis and inflammation through the ERK / MAPK pathway. In IPF, HSP produces TGF-β, which causes epithelial mesenchymal transition (EMT) and pulmonary fibrosis through SMAD / P38 / ERK / MAPK [45]. HSP also activates HFL-1 after binding to LRP-1 and eventually produces TGF-β [46].
In mustard victims, as in IPF, HSP causes inflammation through TGF-β and activation of P38 / MAPK pathway [47]. CD74 is a TF receptor, and this protein along with HSP played a dual role in pathogenesis; moreover, the findings of the present study have shown that their expression has variations. Therefore, identifying the pathways that reduce inflammation via HSP and CD47 can contribute to therapeutic designs.
In addition to shared genes, several genes were observed in disease alone and were evaluated under the influence of molecular mechanisms involved in pathogenesis.
Growth factor receptor-bound protein 2 (GRB2)
GRB2 is a gene expressed on many cells. It binds to several receptors through its domains, including EGFR and FGFR, and regulates many cellular molecular processes. Studies have shown that in COPD GRB2, by activating the PI3K / AKT pathway, it increases the BCL-2 expression and prevents the apoptosis of airway epithelial cells (AECs) [48]. By activating inflammatory cells, it also induces inflammatory reactions in patients. GRB2 has been shown to produce IL-1, IL-6 and TNF-α through MAPK signaling. The production of these cytokines stimulates monocytes and neutrophils and generates inflammatory mediators. GRB2 also produces MMPs and stimulates inflammatory responses in AECs by generating VEGF and activating the MAPK / ERK pathway [48, 49].
The role of GRB2 in the pathogenesis of IPF varies. Accordingly, it has been determined that GRB2 is located downstream of the TGF-β receptor and activates the Raf / MEK / ER1 / 2 pathway. Activation of this pathway leads to the proliferation of fibroblast cells. The activation of the said pathway also stimulates the production of MMPs and the proliferation of collagen cells, which cause fibroblast cells to proliferate [50].
Thus, although GRB2 is involved in both diseases, its downstream pathways differ in each disease, a finding that can help the design of treatment strategies.
Estrogen receptor 1 (ESR1)
ESR1 was identified as the gene most closely associated with other genes in asthma. ESR1 in asthma regulates the proliferation and remodeling of airway smooth muscle (ASM). The results revealed that ESR1 produces TNF-α and activates PDFG. These factors lead to the production of MMPs and prevent the activation of their inhibitors (TIMPs) [51]. Based on the literature, ESR1 produces TNF-α by activating the NF-κB pathway. The generation of these factors leads to extracellular matrix (ECM) stimulation, which increases the remodeling of ASM. Therefore, the regulation of ESR1 expression in patients can be a therapeutic route to prevent the progression of the disease through targeted therapy [51].
Interferon Regulatory Factor 7 (IRF7)
To date, no study has been conducted on the molecular mechanism of IRF7 in MLD patients. However, its expression has been shown to decline in these patients compared with healthy individuals. IRF7 is known to suppress inflammation. It reduces the production of inflammatory mediators by suppressing the NF-κB pathway. Thus, since inflammation is an inflammatory mechanism in MLD, the regulation of IRF7 expression can be a suitable treatment route [52, 53].
Conclusion
The genes and pathways shared by COPD, asthma, IPF, and MLD were investigated. The results showed 22 shared genes involved in many pathways, including lipid metabolism, post-translational protein modification, platelet degranulation, etc. However, most genes were involved in stimulating the immune system and causing inflammation. The dysregulation of proteins can activate signaling pathways and release inflammatory mediators. Still, some of these genes were shown to act as double-edged swords as they both induce and inhibit inflammation. Given that these genes activate different pathways in the cited diseases, identifying the factors and their downstream pathways can be effective in designing preventive and therapeutic strategies.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Soriano JB, Abajobir AA, Abate KH, Abera SF, Agrawal A, Ahmed MB, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706.
Schiller HB, Montoro DT, Simon LM, Rawlins EL, Meyer KB, Strunz M, et al. The Human Lung Cell Atlas: A High-Resolution Reference Map of the Human Lung in Health and Disease. Am J Respir Cell Mol Biol. 2019;61(1):31–41.
Chuchalin AG, Khaltaev N, Antonov NS, Galkin DV, Manakov LG, Antonini P, et al. Chronic respiratory diseases and risk factors in 12 regions of the Russian Federation. Int J Chron Obstruct Pulmon Dis. 2014;9:963.
Obeidat Me, Nie Y, Chen V, Shannon CP, Andiappan AK, Lee B, et al. Network-based analysis reveals novel gene signatures in peripheral blood of patients with chronic obstructive pulmonary disease. Respir Res. 2017;18(1):1–11.
Reddel HK, Bateman ED, Becker A, Boulet L-P, Cruz AA, Drazen JM, et al. A summary of the new GINA strategy: a roadmap to asthma control. Eur Respir J. 2015;46(3):622–39.
Duck A, Pigram L, Errhalt P, Ahmed D, Chaudhuri N. IPF Care: a support program for patients with idiopathic pulmonary fibrosis treated with pirfenidone in Europe. Adv Ther. 2015;32(2):87–107.
Vestbo J, Hurd SS, Agustí AG, Jones PW, Vogelmeier C, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–65.
Karimi A, Hashemian SMR. Cytokine storm in COVID-19 and the treatment simulacrum. Biomedical and Biotechnology Research Journal (BBRJ). 2020;4(5):41.
White CW, Rancourt RC, Veress LA. Sulfur mustard inhalation: mechanisms of injury, alteration of coagulation, and fibrinolytic therapy. Ann N Y Acad Sci. 2016;1378(1):87.
Sabit R, Thomas P, Shale DJ, Collins P, Linnane SJ. The effects of hypoxia on markers of coagulation and systemic inflammation in patients with COPD. Chest. 2010;138(1):47–51.
Wolterink RGK, KleinJan A, van Nimwegen M, Bergen I, de Bruijn M, Levani Y, et al. Pulmonary innate lymphoid cells are major producers of IL-5 and IL-13 in murine models of allergic asthma. Eur J Immunol. 2012;42(5):1106–16.
Corbel M, Belleguic C, Boichot E, Lagente V. Involvement of gelatinases (MMP-2 and MMP-9) in the development of airway inflammation and pulmonary fibrosis. Cell Biol Toxicol. 2002;18(1):51–61.
Karabekmez ME, Kirdar B. A novel topological centrality measure capturing biologically important proteins. Mol BioSyst. 2016;12(2):666–73.
Barabási A-L, Gulbahce N, Loscalzo J. Network medicine: a network-based approach to human disease. Nat Rev Genet. 2011;12(1):56–68.
Ghiassian SD, Menche J, Barabási A-L. A DIseAse MOdule Detection (DIAMOnD) algorithm derived from a systematic analysis of connectivity patterns of disease proteins in the human interactome. PLoS Comput Biol. 2015;11(4): e1004120.
Mobarakeh ZT, Hasanzadeh E, Farzin A, Goodarzi A, Farahani MS, Shirian S, Mahmoodi N, Zamani N, Karimi A, Ai J. Enhanced sciatic nerve regeneration with fibrin scaffold containing human endometrial stem cells and insulin encapsulated chitosan particles: An in vivo study. Injury. 2023;54(6):1462–72.
Murray LA, Grainge C, Wark PA, Knight DA. Use of biologics to treat acute exacerbations and manage disease in asthma. COPD and IPF Pharmacology & therapeutics. 2017;169:1–12.
Rahman MR, Islam T, Zaman T, Shahjaman M, Karim MR, Huq F, et al. Identification of molecular signatures and pathways to identify novel therapeutic targets in Alzheimer’s disease: Insights from a systems biomedicine perspective. Genomics. 2020;112(2):1290–9.
Thomsen JH, Etzerodt A, Svendsen P, Moestrup SK. The haptoglobin-CD163-heme oxygenase-1 pathway for hemoglobin scavenging. Oxid Med Cell longev. 2013;2013:523652.
Chen Z, Wu H, Shi R, Fan W, Zhang J, Su W, et al. miRNAomics analysis reveals the promoting effects of cigarette smoke extract-treated Beas-2B-derived exosomes on macrophage polarization. Biochem Biophys Res Commun. 2021;572:157–63.
Li ML, Su XM, Ren Y, Zhao X, Kong LF, Kang J. HDAC8 inhibitor attenuates airway responses to antigen stimulus through synchronously suppressing galectin-3 expression and reducing macrophage-2 polarization. Respir Res. 2020;21(1):1–14.
Lin C-R, Bahmed K, Criner GJ, Marchetti N, Tuder RM, Kelsen S, et al. S100A8 protects human primary alveolar type II cells against injury and emphysema. Am J Respir Cell Mol Biol. 2019;60(3):299–307.
Kim K, Kim HJ, Binas B, Kang JH, Chung IY. Inflammatory mediators ATP and S100A12 activate the NLRP3 inflammasome to induce MUC5AC production in airway epithelial cells. Biochem Biophys Res Commun. 2018;503(2):657–64.
Da Hye Kim AG, Lee J-S, Yang EJ, Kashif A, Hong MH, Kim G, et al. Suppressive effects of S100A8 and S100A9 on neutrophil apoptosis by cytokine release of human bronchial epithelial cells in asthma. Int J Med Sci. 2020;17(4):498.
Sivaprasad U, Kinker KG, Ericksen MB, Lindsey M, Gibson AM, Bass SA, et al. SERPINB3/B4 contributes to early inflammation and barrier dysfunction in an experimental murine model of atopic dermatitis. J Investig Dermatol. 2015;135(1):160–9.
Akhavan S, Tutunchi S, Malmir A, Ajorlou P, Jalili A, Panahi G. Molecular study of the proliferation process of beta cells derived from pluripotent stem cells. Mol Biol Rep. 2022Feb;49(2):1429–36.
Gour N, Smole U, Yong H-M, Lewkowich IP, Yao N, Singh A, et al. C3a is required for ILC2 function in allergic airway inflammation. Mucosal Immunol. 2018;11(6):1653–62.
Arizmendi N, Kulka M. Adenosine activates Gαs proteins and inhibits C3a-induced activation of human mast cells. Biochem Pharmacol. 2018;156:157–67.
Cipolla E, Fisher AJ, Gu H, Mickler EA, Agarwal M, Wilke CA, et al. IL-17A deficiency mitigates bleomycin-induced complement activation during lung fibrosis. FASEB J. 2017;31(12):5543–56.
Gu H, Mickler EA, Cummings OW, Sandusky GE, Weber DJ, Gracon A, et al. Crosstalk between TGF-β1 and complement activation augments epithelial injury in pulmonary fibrosis. FASEB J. 2014;28(10):4223–34.
Sheikh M, Rahimi PO. The prevalence of AKI in Iranian children with CHD; A Systematic Review and Meta-analysis. Int J Adv Res Biol Sci. 2022;9(5):58–64.
Riahi-Zanjani B, Mahmoudi M. Immunological and hematological complications of sulfur mustard poisoning. Basic and clinical toxicology of mustard compounds: Springer; 2015. p. 273–89.
Nita-Lazar A, Goodlett DR. Targeted proteomics: Bench to bedside. J Proteomics. 2018;189:III–V.
Park SW, Lee E, Lee EJ, Kim H, Bae DJ, Han S, et al. Apolipoprotein A1 potentiates lipoxin A4 synthesis and recovery of allergen-induced disrupted tight junctions in the airway epithelium. Clin Exp Allergy. 2013;43(8):914–27.
Dai C, Yao X, Keeran KJ, Zywicke GJ, Qu X, Yu Z-X, et al. Apolipoprotein AI attenuates ovalbumin-induced neutrophilic airway inflammation via a granulocyte colony–stimulating factor–dependent mechanism. Am J Respir Cell Mol Biol. 2012;47(2):186–95.
Baek AR, Lee JM, Seo HJ, Park JS, Lee JH, Park SW, et al. Apolipoprotein A1 Inhibits TGF-β1–Induced Epithelial-to-Mesenchymal Transition of Alveolar Epithelial Cells. Tuberc Respir Dis. 2016;79(3):143–52.
Song X, Shi Y, You J, Wang Z, Xie L, Zhang C, et al. D-4F, an apolipoprotein AI mimetic, suppresses IL-4 induced macrophage alternative activation and pro-fibrotic TGF-β1 expression. Pharm Biol. 2019;57(1):470–6.
Fallica J, Varela L, Johnston L, Kim B, Serebreni L, Wang L, et al. Macrophage Migration Inhibitory Factor: A Novel Inhibitor of Apoptosis Signal-Regulating Kinase 1–p38–Xanthine Oxidoreductase-Dependent Cigarette Smoke-Induced Apoptosis. Am J Respir Cell Mol Biol. 2016;54(4):504–14.
Russell KE, Chung KF, Clarke CJ, Durham AL, Mallia P, Footitt J, et al. The MIF antagonist ISO-1 attenuates corticosteroid-insensitive inflammation and airways hyperresponsiveness in an ozone-induced model of COPD. PLoS One. 2016;11(1):e0146102.
Fan H, Hall P, Santos LL, Gregory JL, Fingerle-Rowson G, Bucala R, et al. Macrophage migration inhibitory factor and CD74 regulate macrophage chemotactic responses via MAPK and Rho GTPase. J Immunol. 2011;186(8):4915–24.
Rumora L, Somborac-Bačura A, Hlapčić I, Hulina-Tomašković A, Rajković MG. Cigarette smoke and extracellular Hsp70 induce secretion of ATP and differential activation of NLRP3 inflammasome in monocytic and bronchial epithelial cells. Cytokine. 2020;135:155220.
Kang Y, Wang F, Lu Z, Ying H, Zhang H, Ding W, et al. MAPK kinase 3 potentiates Chlamydia HSP60-induced inflammatory response through distinct activation of NF-κB. J Immunol. 2013;191(1):386–94.
Zhang YX, Chen JJ, Nabu S, Yeung QSY, Li Y, Tan JH, et al. The pregnancy outcome of mosaic embryo transfer: a prospective multicenter study and meta-analysis. Genes. 2020;11(9):973.
Rahmani F, Safavi P, Fathollahpour A, TanhayeKalateSabz F, Tajzadeh P, Arefnezhad M, et al. The interplay between non-coding RNAs and Wnt/β-catenin signaling pathway in urinary tract cancers: from tumorigenesis to metastasis. EXCLI J. 2022;21:1273–84.
Li X, Yu H, Liang L, Bi Z, Wang Y, Gao S, et al. Myricetin ameliorates bleomycin-induced pulmonary fibrosis in mice by inhibiting TGF-β signaling via targeting HSP90β. Biochem Pharmacol. 2020;178:114097.
Dong H, Luo L, Zou M, Huang C, Wan X, Hu Y, et al. Blockade of extracellular heat shock protein 90α by 1G6-D7 attenuates pulmonary fibrosis through inhibiting ERK signaling. Am J Physiol Lung Cell Mol Physiol. 2017;313(6):L1006–15.
Solopov P, Colunga Biancatelli RM, Marinova M, Dimitropoulou C, Catravas JD. The HSP90 inhibitor, AUY-922, ameliorates the development of nitrogen mustard-induced pulmonary fibrosis and lung dysfunction in mice. Int J Mol Sci. 2020;21(13):4740.
Tan Y, Qiao Y, Chen Z, Liu J, Guo Y, Tran T, et al. FGF2, an Immunomodulatory Factor in Asthma and Chronic Obstructive Pulmonary Disease (COPD). Front Cell Dev Biol. 2020;8:223.
Rahmani F, Zandigohar M, Safavi P, Behzadi M, Ghorbani Z, Payazdan M, et al. The Interplay between Noncoding RNAs and p21 Signaling in Gastrointestinal Cancer: From Tumorigenesis to Metastasis. Curr Pharm Des. 2023;29(10):766–76.
Sheikh M, Ostadrahimi P, Salarzaei M, Parooie F. Cardiac complications in pregnancy: a systematic review and meta-analysis of diagnostic accuracy of BNP and N-terminal pro-BNP. Cardiol Ther. 2021Dec;10:501–14.
Ambhore NS, Kalidhindi RSR, Pabelick CM, Hawse JR, Prakash YS, Sathish V. Differential estrogen-receptor activation regulates extracellular matrix deposition in human airway smooth muscle remodeling via NF-κB pathway. FASEB J. 2019;33(12):13935–50.
Mohammad Mohsenimajd A, Alikhani M, Mehdi Naghizadeh M, Ghazanfari T. Two dimensional proteomic analysis of serum shows immunological proteins exclusively expressed in sulfur mustard exposed patients with long term pulmonary complications. Int immunopharmacol. 2020;88:106857.
Sweeney SE, Corr M, Kimbler TB. Role of interferon regulatory factor 7 in serum-transfer arthritis: regulation of interferon-β production. Arthritis Rheum. 2012;64(4):1046–56.
Acknowledgements
We wish to thank all our colleagues at Baqiyatallah University of Medical Sciences.
Funding
The authors declare that no fund, grant, or other support was received during the drafting of this paper.
Author information
Authors and Affiliations
Contributions
M.A and BF. N. conceived the manuscript and revised it. H.R, BF. N. and M.A were involved in data extraction, analysis, and design strategy search. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rezaeeyan, H., Nobakht M. Gh, B.F. & Arabfard, M. A computational approach for the identification of key genes and biological pathways of chronic lung diseases: a systems biology approach. BMC Med Genomics 16, 159 (2023). https://doi.org/10.1186/s12920-023-01596-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12920-023-01596-7