
Abstract
Background
Fetal alcohol syndrome (FAS) can result in cognitive dysfunction. Cognitive functions affected are subserved by few functional brain networks. Functional connectivity (FC) in these networks can be assessed with resting-state functional MRI (rs-fMRI). Alterations of FC have been reported in children and adolescents prenatally exposed to alcohol. Previous reports varied substantially regarding the exact nature of findings. The purpose of this study was to assess FC of cognition-related networks in young adults with FAS.
Methods
Cross-sectional rs-fMRI study in participants with FAS (n = 39, age: 20.9 ± 3.4 years) and healthy participants without prenatal alcohol exposure (n = 44, age: 22.2 ± 3.4 years). FC was calculated as correlation between cortical regions in ten cognition-related sub-networks. Subsequent modelling of overall FC was based on linear models comparing FC between FAS and controls. Results were subjected to a hierarchical statistical testing approach, first determining whether there is any alteration of FC in FAS in the full cognitive connectome, subsequently resolving these findings to the level of either FC within each network or between networks based on the Higher Criticism (HC) approach for detecting rare and weak effects in high-dimensional data. Finally, group differences in single connections were assessed using conventional multiple-comparison correction. In an additional exploratory analysis, dynamic FC states were assessed.
Results
Comparing FAS participants with controls, we observed altered FC of cognition-related brain regions globally, within 7 out of 10 networks, and between networks employing the HC statistic. This was most obvious in attention-related network components. Findings also spanned across subcomponents of the fronto-parietal control and default mode networks. None of the single FC alterations within these networks yielded statistical significance in the conventional high-resolution analysis. The exploratory time-resolved FC analysis did not show significant group differences of dynamic FC states.
Conclusions
FC in cognition-related networks was altered in adults with FAS. Effects were widely distributed across networks, potentially reflecting the diversity of cognitive deficits in FAS. However, no altered single connections could be determined in the most detailed analysis level. Findings were pronounced in networks in line with attentional deficits previously reported.
Similar content being viewed by others

Background
Prenatal alcohol exposure (PAE) can negatively affect a wide range of cognitive functions throughout life. These functions include general intelligence, attention, executive functions (including inhibitory control), learning and memory, language, mathematical abilities, social cognition [1, 2], and impulse control [1, 3, 4]. Deficits associated with PAE frequently persist into adulthood [5, 6]. While the term fetal alcohol spectrum disorders (FASD) generally encompasses a broad range of possible conditions related to PAE, only the full picture of characteristic physical (including growth retardation and facial abnormalities), psychological, and cognitive features is termed fetal alcohol syndrome (FAS) [2, 7, 8].
Brain activity in individual regions underlying specific cognitive functions can be assessed by functional neuroimaging with a wide range of targeted tests [9]. However, a frequent neuroscientific observation is that many higher cognitive functions, such as those negatively affected in FAS, are subserved by activity in few common sets of brain regions, i.e., functional brain networks. These include task-positive networks with overlapping definitions such as the central executive network, cognitive control network, or multiple demands network as well as networks closely interacting with them, such as the salience network and default mode network [10,11,12]. Spontaneous activity and functional connectivity within and between these networks can be examined by resting-state functional magnetic resonance imaging (rs-fMRI) [13, 14]. Static functional connectivity (FC) analysis methods identify correlated activity over a full rs-fMRI data acquisition period [14]. They have recently been supplemented by approaches for assessing dynamic or time-varying FC. Such dynamic FC analyses promise a deeper understanding of dynamic interactions of brain regions within and across these functional networks [15,16,17] in health and disease. Dynamic FC measures have been associated with differences in individual attentional performance [18, 19] and impulsivity [20, 21]. For example, altered FC dynamics have been observed in participants with attention deficit hyperactivity disorder (ADHD) [22,23,24].
Few studies have directly investigated resting-state FC within and between brain networks related to higher cognitive functions in individuals with FAS or prenatal alcohol exposure: Focusing on within-network connectivity, Fan et al. observed reduced FC in a subset of regions within the default mode, salience, ventral attention, dorsal attention, and right fronto-parietal executive control networks in children with FASD compared with non-exposed controls. These networks reflect cognitive functions typically affected in children with FASD. Networks not directly related to cognition were, however, not affected [25]. In another study with children and adolescents with FASD, Little et al. mainly described reductions of FC between core regions of the salience and fronto-parietal control networks and regions from other cognition-related networks rather than within networks [26]. In contrast, Ware et al. found lower within-network but higher between-network FC in attention-related networks in children with FASD [27]. All three studies report relatively high overall similarity of FC in cognition-related networks between exposed individuals and controls, while FC group differences had relatively small effect sizes, contrasting with the distinct clinical deficits in these individuals [25,26,27]. Further rs-fMRI and methodologically related FC studies in individuals with PAE report evidence of altered overall functional brain organization based on global graph-theoretical measures [28,29,30,31] as well as FC alterations of the default mode network [32] and within networks less directly related to cognitive control [33, 34]. No previous study has, however, explored dynamic FC in FASD. Beyond that, amid studies describing persisting cognitive deficits into adulthood [5, 6], FC has not been previously examined in adults prenatally exposed to alcohol.
The main goal of this study was therefore to examine functional connectivity in cognition-related functional brain networks in young adults with FAS and to assess whether these patterns are comparable to alterations previously observed in affected children and adolescents.
The following hypotheses should be tested:
-
Static FC in the connectome of all brain regions constituting cognition-related brain networks is altered in young adults with FAS compared with a control group without prenatal alcohol exposure (omnibus test, bi-directional effects possible).
-
Static FC within individual cognition-related brain networks is altered in FAS participants compared with controls without prenatal alcohol exposure (bi-directional effects possible).
-
Static FC between cognition-related brain networks is altered in FAS participants compared with controls without prenatal alcohol exposure (bi-directional effects possible).
In an additional exploratory analysis, we addressed dynamic interactions between cognition-related brain regions in FAS participants compared with non-exposed controls. This dynamic FC analysis [17] focused on transitions between putative FC states. Rationale of this analysis is that less stable FC states in FAS might underlie impaired impulse control (similar to reports in ADHD [22,23,24]).
Methods
The study was carried out in a research setting outside routine clinical care. Samples overlapped with previously published task-based fMRI studies on inhibitory control with joint data acquisition in a superordinate research project: a control group overlap with a task-based study in phenylketonuria [35] and a female patient and control group overlap with a task-based study in FAS [36]. There was no sample overlap with previous rs-fMRI research in FAS or FASD.
Participants
Young adult persons (n = 50) with FAS seen for regular appointments at the FAS outpatient clinic at the Children’s healthcare center Haus Walstedde (Drensteinfurt, Germany) were initially invited based on standardized primary inclusion and exclusion criteria: These primary inclusion criteria were a diagnosis of FAS made by a specialist based on the Majewski criteria [37] (see supplementary Additional_file_1.pdf: supplementary methods) [37, 38], and being 18 to 32 years of age. Primary exclusion criteria were contraindications for MRI, severe psychiatric (e.g., current symptomatic episode of major depression, bipolar disorder or schizophrenia), neurological (e.g., stroke or epilepsy) or medical (e.g., cancer) conditions, pregnancy, and severe sensory impairments. Less severe psychiatric comorbidity or symptoms in general (e.g., signs of hyperactivity or a history of adjustment disorder) as well as medication in general were not defined as primary exclusion criteria for the FAS group since they are common in individuals with a history of prenatal alcohol exposure [39]. In four participants, no fMRI data could be acquired because of claustrophobia. After data acquisition, further participants were excluded after review of potentially biasing medication, structural brain lesions, and MRI data quality control before any FC group analyses: Two participants were excluded from the analyses due to use of potentially psychoactive anti-allergic medication unrelated to FAS, which can alter rs-fMRI measurements [40]. One subject was excluded because of a callosal hypoplasia leading to structural image misregistration. Data from further 4 FAS participants were excluded because of excessive head motion (based on motion parameters, see section “Pre-processing and image quality control” for criteria). All results are based on the remaining 39 FAS participants. Current intake of the following potentially psychoactive medication was reported in the FAS group: methylphenidate or derivatives (n = 8), antipsychotics (n = 5), and antidepressants (n = 1).
The control group consisted of participants without a history of prenatal alcohol exposure. Initially, n = 52 participants were recruited by using the internal information board for employees of the Münster university hospital and mailing lists of medical students at the Münster medical faculty. Apart from general exclusion of participants with psychoactive medication in the control group, inclusion and exclusion criteria (both for initial inclusion and after data acquisition) were identical in both groups. Reasons for exclusion after data acquisition in this group were: Two participants were excluded due to use of psychoactive medication (disclosed at the study appointment). One subject was excluded because of a large frontal venous anomaly potentially biasing fMRI data [41]. One fMRI dataset was excluded because of a technical failure. Data from 4 participants were excluded because of excessive head motion (3 based on motion parameters, 1 based on visual quality indicators, see section “Pre-processing and image quality control” for criteria). We observed a statistically significant age difference between the groups with a small effect size (Table 1). We refrained from excluding further control participants in order not to compromise statistical power considering that only small age effects on FC are expected in this particular age range [42]. Finally, 44 controls were included in further analyses. Demographical data of the final sample are reported in Table 1.
Neuropsychological pre-assessment
Participants completed questionnaire-based pre-tests for handedness (Edinburgh Handedness Inventory, EHI) [43], processing speed (trail-making task, TMT) [44], and screening for severe mental comorbidity (DIA-X Stamm-Screening questionnaire, SSQ) [45]. A general intelligence estimate was calculated based on TMT results [44, 46]. Quantitative test results are presented in Table 1.
Acquisition of MRI data
MRI data were acquired at 3 Tesla (Intera with Achieva upgrade, Philips, Best, NL) using a single-channel transmit/receive head coil. FMRI data were acquired during 9:45 min of wakeful rest using gradient echo planar imaging covering the whole brain (234 functional volumes after 5 non-recorded dummy scans to allow for signal equilibration; repetition time: 2500 ms, echo time: 35 ms, 36 axial slices, spatial resolution 3.6 × 3.6 × 3.6 mm). Participants were instructed to keep their eyes open and think of nothing in particular during the rs-fMRI acquisition. T1-weighted 3D data were acquired with an inversion-prepared turbo field echo (TFE) sequence (inversion time: 411 ms, repetition time: 7.1 ms, echo time: 3.5 ms, flip angle: 9°, sagittal slices measured with 2 mm thickness, reconstructed spatial resolution by zero-filling in k-space 1.0 × 1.0 × 1.0 mm).
Analysis of MRI data
Pre-processing and image quality control
MRI data were converted to the Brain Imaging Data Structure (BIDS) [47] using in-house scripts preceding the BiDirect-BIDS-ConverteR [48, 49]. Facial features were removed from the T1-weighted anatomical data [50]. Main MRI data pre-processing was carried out using fMRIPrep [51] (version 20.0.7, RRID:SCR_016216) briefly consisting of motion estimation and correction, co-registration of fMRI and structural MRI data, estimation of noise regressors, and standard space normalization. Please consult the Supplementary Methods for further details. Subsequent actual denoising was carried out using fMRIDenoise [52] (version 0.2.1), comprising regressing out 24 head motion parameters (3 translations, 3 rotations, their 6 temporal derivatives, and their 12 quadratic terms) [53], 8 physiological noise parameters (mean physiological signals from white matter and cerebrospinal fluid, their 2 temporal derivatives, and 4 quadratic terms) [53] as well as movement spike regression based on frame-wise displacement (FD > 0.5 mm) and so-called “DVARS” (> 3) thresholds [54], temporally filtering (0.008–0.08 Hz), and, finally, smoothing the resulting standard space image with a Gaussian kernel (FWHM = 6 mm). This pre-processing leads to denoised fMRI data in a common standard space as input for further analyses.
The following steps were taken for MRI data quality control (numbers of excluded participants reported in the section “participants”): Structural MRI data were screened by a radiologist for incidental findings and major artifacts. fMRIPrep reports were reviewed for registration errors and image artifacts (including signs of strong motion artifacts in the carpet plots). Subject exclusion for excessive head motion (see section “Participants”) was based on pre-processing criteria (mean frame-wise displacement, FD > 0.3 mm or maximum FD > 5 mm or more than 20% outlier data points). FD did not differ significantly between FAS and controls. However, there was a trend towards higher mean and maximum FD in the FAS group (see Supplementary Table 1).
Static functional connectivity analysis: general approach
Functional connectivity analyses were based on a cortical atlas (“Schaefer atlas”) derived from rs-fMRI data in 1489 participants. The atlas was obtained from TemplateFlow (RRID:SCR_021876) to match the dimensions of the fmriprep outputs [55]. The atlas version with 400 parcels adopted here is the most extensively validated version of this atlas, e.g., regarding stability and correspondence with markers of brain function [56]. The individual parcels in the published atlas have been matched to 17 non-overlapping networks from a previously established atlas by Yeo et al. [57]. Ten cognition-related components out of these 17 networks were selected for further analysis: the dorsal attention network (2 sub-networks A and B), the salience / ventral attention network (2 sub-networks A and B), the mainly fronto-parietal control network (3 sub-networks A-C), and the default mode network (3 sub-networks A-C). Time-series extraction from the pre-processed fMRI data and calculation of z-transformed Pearson correlation coefficients as primary measures of FC were carried out with the Data Processing Assistant for Resting-State fMRI (DPARSF, version 5.2, RRID:SCR_002372) [58] based on Matlab 2019b (The MathWorks, Natick, MA, USA, RRID:SCR_001622). As a basis for subsequent modelling, we carried out multiple linear models (one model per pair of regions), comparing z-transformed correlation coefficients (dependent variable) among regions of interest between FAS participants and controls. The following independent variables were included in the multiple linear regression models: group (FAS vs. control, categorical), sex (categorical), age (normalized to center: 0, and standard deviation: 1), mean FD, and a constant term (intercept). Main effects of the factor group (FAS vs. controls, two-sided) are the basis of the subsequent analyses at different spatial scales. A previous analogous analysis based on multiple two-tailed two-sample t-tests, i.e., not including age, sex, and head movement with similar results has been made available in the preprint version of this article [59].
We followed a hierarchical statistical testing approach with three levels of analysis: (1) first, determining whether there is any alteration of FC in FAS participants compared with controls in the full connectome of 243 regions constituting these 10 cognition-related networks (i.e., an omnibus test) globally and subsequently aiming to resolve these findings, (2) to the level of either FC within each network or between-network connectivity, and finally (3) to individual connections.
Static functional connectivity analysis: global analysis
The omnibus test on the full connectome (main effect of group: FAS vs. control) is based on the “Higher Criticism” (HC) approach [60] in an improved version [61] implemented in Matlab (https://www.stat.cmu.edu/~jiashun/Research/software/HC/). HC statistics can be applied in order to test whether there are any non-zero effects within a large number of individual tests carried out in high-dimensional datasets. They are thus suitable to identify the existence of rare and weak effects in such data [60]. HC follows the rationale of p-value histogram analyses: Under a null-hypothesis of only zero effects in multiple parallel tests, an equal distribution of p-values is expected. Under the alternative hypothesis of existing non-zero effects, there is an excess of low p-values [62]. In simplified terms, HC statistics quantitatively test a joint hypothesis of such an excess of low p-values [60, 62]. HC has been increasingly popular for detecting effects in high-dimensional data such as in genetic [60] and economic [63] research. It has been argued that HC could be favorable for the detection of rare events compared with conventional false discovery rate (FDR) or family-wise error rate (FWE) correction methods [60]. Considering the similarly high dimensionality of FC datasets, HC has recently been applied to rs-fMRI analyses [64, 65]. Both, in this global analysis and the subsequent network-wise HC-based hypothesis tests, we used p-value histograms (main effect of group) as a plausibility check.
Static functional connectivity analysis: within-network HC analysis
Subsequently, we aimed to determine which of the 10 cognition-related networks were affected by within-network functional connectivity differences between FAS and control participants. We therefore carried out equivalent HC tests separately for these networks. Each set of tests included the full set of correlation coefficients between all regions within each network.
Static functional connectivity analysis: between-network HC analysis
For a similar analysis of between-network FC (i.e., to determine whether any between-network FC differences were present), we concatenated all parcels for each of the 10 networks separately. This resulted in a single mask for each network before time-series data extraction. The resulting correlation coefficients were assessed with an equivalent HC test.
Static functional connectivity analysis: analysis of individual connections
In a third level, we aimed to identify single between- and within-network connections exhibiting statistically significant FC differences between FAS participants and controls. Therefore, in contrast to the previously described HC-based joint hypothesis tests, we now FDR-adjusted [66] the individual hypothesis tests (main effect of group: FAS vs. control) of between- and within-network connectivity (q < 0.05), using an FDR implementation in Matlab (https://brainder.org/2011/09/05/fdr-corrected-fdr-adjusted-p-values). This was carried out separately for either all 45 between-network connections or all individual connections, and also within each separate network.
Exploratory time-resolved functional connectivity analysis
Beyond the static FC analysis, we carried out an exploratory dynamic FC analysis, using a sliding window approach with the DynamicBC toolbox (version 2.2) [67]. FC between all 243 regions in the cognition-related networks was calculated for each individual subject by Pearson linear correlation separately in overlapping windows with a length of 18 consecutive functional volumes equivalent to 45 s, similar to window lengths in previous studies [68, 69], and with a 60% overlap. The resulting time-resolved FC estimates from individual time windows were grouped by similarity (K-means cluster analysis, distance measure: correlation) in order to derive presumed FC states in the entire sample. Established methods were used to estimate the optimal number of clusters and assess the goodness of fit of the clustering solutions: (1) The optimal number of clusters (search range: 2 to 10) was estimated using the Calinski-Harabasz [70] and Davies–Bouldin [71] indices resulting in 2 clusters (see Supplementary Fig. 1). (2) Cluster-separability was estimated by a silhouette analysis. Briefly, the silhouette analysis assesses, how similar an individual element is to other elements within its own cluster compared with elements in other clusters [72]. The following summary measures describing the temporal dynamics of putative FC states were calculated for individual participants: number of transitions (NT) between connectivity states, mean dwell time (MDT) per cluster, and frequency of observing each cluster (FRC). Participants with FAS and controls were compared regarding NT and MDT using t-tests or Mann–Whitney U tests.
Statistical analysis
Statistical modelling is inherent to the FC analyses described above and is thus presented within the preceding sub-sections. Statistical tests on clinical and demographical data were carried out in SPSS (version 27.0, IBM, Armonk, NY, USA, RRID:SCR_002865).
Results
Static functional connectivity analysis: global analysis
We observed significantly altered FC of cognition-related brain regions in FAS participants compared with non-exposed controls in the global (all parcels of all 10 cognition-related networks) analysis over the entire data acquisition period. This finding is based on a joint hypothesis test (HC test statistic: 25.80, a higher value represents stronger support for an excess of low p-values in the underlying primary hypothesis tests). This joint hypothesis test aims to detect the existence of alterations within this high-dimensional dataset but which does not identify which exact connections are altered (Fig. 1). Quantitative results of FC group differences in connections between single atlas regions (Additional_file_2.csv, Additional_file_3.csv) as depicted in Fig. 1C are shared together with standardized effect size estimates (Additional_File_4.csv).

Global analysis of static functional connectivity of cognition-related brain networks. A Full atlas-based selection of 243 individual brain regions in cognition-related networks (redundant color coding for illustration of atlas resolution only). B P-value histogram of multiple individual linear models (main effect of group) comparing functional connectivity among all these brain regions between FAS patients and control participants. Under the null hypothesis of equal functional connectivity in both groups, equal numbers of p-values are expected in each histogram bin. The histogram shows an excess of low p-values. The existence of at least rare and/or weak effects visualized in the histogram is confirmed by a quantitative test of the joint hypothesis based on higher criticism statistics, following the same rationale. This means that regarding a significant number of functional connections, FAS patients differ from healthy controls. C Unthresholded matrix of connectivity group differences describing the full connectome of cognition-related brain regions. Yellow: mean z-transformed correlation coefficients relatively increased in FAS compared with controls. Blue: relatively decreased functional connectivity in FAS. Color coding of networks identical with Fig. 4. D Standardized effect size estimates (partial η2 from linear models)
Static functional connectivity analysis: within-network HC analysis
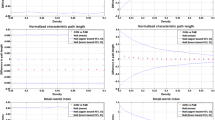
FC was altered within 7 out of 10 of these cognition-related brain networks based on the joint hypothesis tests. Based on the HC test statistic and supported by p-value histograms of tests of individual functional connections, this effect was most obvious in the salience / ventral attention A network (HC test statistic: 13.31), followed by the dorsal attention A sub-network (HC test statistic: 11.27). However, findings also spanned across sub-networks A, B, and C of the fronto-parietal control (HC test statistics: 4.02, 5.20, and 4.82) and sub-networks A, and B of the default mode (HC test statistics: 4.56 and 3.45) networks (Fig. 2). Three networks did not exhibit significant group effects: the dorsal attention B (HC test statistic: 1.00), salience/ventral attention B (HC test statistic: − 1.15), and default mode C (HC test statistic: 2.84) components (Fig. 3).

Within-network static functional connectivity differences in cognition-related brain networks. Seven (out of ten) sub-networks exhibiting altered functional connectivity in FAS patients compared with controls. First column: Overview of the networks’ overall extent. Second column: P-value histograms (different scaling reflecting different numbers of regions in each network) of multiple linear models (main effect of group) comparing functional connectivity within these sub-networks between FAS patients and control participants. Under the null hypothesis of equal functional connectivity in both groups, equal numbers of p-values are expected in each histogram bin. The histograms show an excess of low p-values, quantitatively confirmed by a test of the joint hypothesis based on higher criticism statistics. This means that FAS patients differ from healthy controls regarding at least rare and/or weak effects. Third column: Unthresholded matrices of connectivity group differences describing the full connections of cognition- related brain regions within each network. Yellow: mean z-transformed correlation coefficients relatively increased in FAS compared with controls. Blue: relatively decreased functional connectivity in FAS. Fourth column: Standardized effect size estimates (partial η2 from linear models, * single connection with significant group difference, false-discovery-rate-corrected p < 0.05 within the network but not significant when correcting across all connections). The remaining three networks without significant results are presented in Fig. 3

Within-network static functional connectivity of cognition-related brain networks (networks without significant group differences). Three (out of ten) sub-networks not exhibiting altered functional connectivity in FAS patients compared with controls. First column: Overview of the networks’ overall extent. Second column: P-value histograms of multiple linear models (main effect of group) comparing functional connectivity within these sub-networks between FAS and control participants (global null hypothesis not rejected based on HC test statistic). Third column: Unthresholded matrix of connectivity group differences describing the full connections of cognition-related brain regions within each network. Yellow: mean z-transformed correlation coefficients relatively increased in FAS compared with controls. Blue: relatively decreased functional connectivity in FAS. Fourth column: Standardized effect size estimates (partial η2 from linear models)
Static functional connectivity analysis: between-network HC analysis
A subsequent analysis revealed altered FC between cognition-related brain networks based on an equivalent joint hypothesis test (HC test statistic: 5.95). Descriptively, underlying strongest relative decreases of FC (ranking of correlation coefficient group differences) in FAS participants were observed between the salience / ventral attention B and fronto-parietal control C sub-networks. The strongest relative increases were observed between the dorsal attention B and fronto-parietal control sub-networks as well as between the default mode C sub-network and other parts of the default mode network and fronto-parietal control network (Fig. 4).

Between-network static functional connectivity of cognition-related brain networks. A 10 cognition-related networks. Each color represents an individual sub-network (network-wise concatenation of individual regions based on atlas labels). B P-value histogram of multiple linear models (main effect of group) comparing functional connectivity among these sub-networks between FAS patients and control participants. Under the null hypothesis of equal functional connectivity in both groups, equal numbers of p-values are expected in each histogram bin. The histogram shows an excess of low p-values quantitatively confirmed by a test of the joint hypothesis based on higher criticism statistics. This means that regarding a significant number of functional connections, FAS patients differ from healthy controls. C Unthresholded matrix of connectivity group differences describing the full connectome of cognition- related brain regions. Yellow: mean z-transformed correlation coefficients relatively increased in FAS compared with controls. Blue: relatively decreased functional connectivity in FAS. D Standardized effect size estimates (partial η2 from linear models)
Static functional connectivity analysis: analysis of individual connections
A single connection within the default mode B sub-network between the left dorsal prefrontal cortex and the right temporal lobe (decreased FC in FAS, difference of group-averages z-transformed correlation coefficients: − 0.210, partial η2 = 0.196) was statistically significant with FDR-adjustment within this network only (p = 0.0198), however not when adjusting (FDR) across all connections. None of the other individual FC alterations (either from the within- or between-network analysis) were statistically significant when correcting the separate tests of individual connections for multiple comparisons.
Exploratory time-resolved functional connectivity analysis
In the exploratory dynamic FC analysis, a solution consisting of two FC states was empirically derived as the optimal number of clusters across the entire sample. These two clusters representing putative FC states were only weakly separable (see silhouette values and further goodness-of-fit statistics for the clustering solutions in Supplementary Fig. 1). Both clusters differed mainly regarding (1) the relatively connectivity strength of the DMN and (2) the extent that the DMN appeared interconnected with other cognition-related brain networks. See Additional_file_1.pdf: Supplementary Fig. 2 for further details on the clusters. FAS participants did not differ significantly regarding the temporal dynamics of these FC states NT, MDT, and FRC (Table 2).
Discussion
In summary, FC was altered in adults with FAS compared to controls not exposed to alcohol prenatally both within a majority of cognition-related networks (including the salience / ventral attention networks and dorsal attention networks, as well as, to a lesser degree, the fronto-parietal control network, and the default mode network) and between these networks. These results on the global and network level are based on an HC approach, indicating that at least rare and weak group effects seem to be present [60]. HC-based findings do, however, not necessarily mean that FC is changed in a majority of connections. Group effects could not be further resolved to connections between individual regions using conventional mass-univariate testing with multiple-comparison correction. In the additional exploratory time-resolved FC analysis, altered FC dynamics in the FAS group could not be observed.
Wide distribution of group effects across networks
The wide distribution of findings across cognition-related networks is in line with the similarly wide range of cognitive deficits observed in individuals with FAS [1]. It thus suggests a rather distributed neural basis (i.e., unspecific alcohol-related damage) of such deficits rather than strongly localized alterations. A similarly wide distribution of FC alterations across networks was observed by Fan et al. in children with FASD [25]. Thus, this observation of a wide distribution spans different age groups (from childhood to young adulthood) and rs-fMRI analysis approaches. Visual interpretation of the connectivity matrices reveals different directionalities of findings: Some connections exhibited higher, and some lower FC in FAS. This bidirectionality is generally in line with a study in children with FASD by Ware et al.. They also report different directionalities of FC alterations [27]. Consequently, a simple picture of either overall increases or decreases of FC in FAS does not exist.
Group differences in attention-related networks
The observation of more obvious effects in attention- and salience-related systems compared with networks underlying other cognitive functions highlights the importance of attentional deficits in FASD [1, 73,74,75,76,77], including adults [5, 78]. However, this interpretation might be limited by the infeasibility of a direct quantitative comparison between networks as well as reverse inference [79, 80]. Our rs-fMRI findings are generally in line with previous studies suggesting a particular involvement of attentional functions and underlying neural systems in FAS when compared to other cognitive deficits: Response and activation patterns in a Go/NoGo task in a sample of young female adults overlapping with this study also provide indirect evidence of a particular importance of attentional deficits compared with inhibitory control deficits in this age group [36]. Attention-related networks were also altered in other alcohol-exposed samples studied with fMRI: Attention networks were among those altered in studies by Fan et al. [25] and Ware et al. [27]. In the latter study, FC alterations were associated with differences in attentional performance measures. The authors consequently conclude that the patterns observed (lower within-network, higher between-network FC) provide support for reduced attention network specialization and inefficiency [27]. Reduced FC between key regions of the salience network with other cognition-related networks were among the key findings by Little et al. [26]. There is further evidence of altered attention systems from magnetoencephalography [81] and diffusion tensor imaging [82].
Group differences in networks related to cognitive control
To a lesser extent, we observed altered FC in parts of the fronto-parietal control network. This network is considered a flexible hub that interacts with other processing networks in order to orchestrate performance in a wide range of cognitive tasks [83]. Changes in fronto-parietal network FC were among those also observed in younger participants with FASD [25, 26]. There is further evidence of altered activity in these networks in children with FASD from task-based fMRI studies on inhibitory control [84] and working memory [85].
Group differences in the default mode network
The default mode network (DMN), though classically reported as anti-correlated with task-positive cognitive networks [86], is considered to be involved in cognitive functions including task-switching and integration of information [87, 88]. There is evidence of regional differentiation within the DMN, with subdivisions subserving different cognitive functions [89]. Fan et al. observed altered FC in the anterior part of the DMN, discussed as subserving social perception, judgment, and self-referential processing in individuals with FASD; however, they found no changes within the posterior DMN [25]. Different from the preprint version of this analysis (i.e., not controlling for covariates in the primary models) [59], we did not find evidence of a strong predominance of group effects in either the anterior or posterior part of the DMN. Beyond that, there is further evidence of less regionally specific DMN dysfunction in FASD [32]. One single connection within the DMN was significant when correcting for multiple comparisons within the sub-network only, but not with global correction. Considering the distribution of effects within this network in comparison with the other networks, we consider this a potential outlier.
Specific aspects of the statistical approach underlying main results
The main static FC analysis applied in this study follows a hierarchical statistical approach, partially based on HC statistics. This approach addresses the general limitations of functional neuroimaging analyses in relatively infrequent disorders such as FAS: Conventional high-dimensional FC analysis methods, such as frequently used mass-univariate statistical testing, carry the risk to report only a “tip of the iceberg” of true underlying alterations due to lower than optimal statistical power. There is an increased risk of both published findings being false-positive [90, 91] or false-negative findings [90]. Further in-depth discussions on this issue have been published [91,92,93]. Consequently, statistical thresholding of mass-univariate analyses (mainly for multiple-comparison correction) might in part explain ambiguous FC results in previous studies in children with FASD [25,26,27]. Such a conventional analysis approach as applied at the most detailed analysis level in this study did not yield significant group effects regarding single connections between regions of interest in this study when correcting for multiple comparisons across all connections. There are increasing efforts to report subthreshold effects in fMRI studies in order to facilitate better interpretation of underlying patterns [94,95,96]. An example is the additional presentation of unthresholded activation or connectivity maps [95, 97]. Our hierarchical approach with HC-based joint hypothesis tests [60, 61] at the network level might help avoid these shortcomings without sacrificing information from individual connections. Compared with conventional mass-univariate fMRI analyses, it avoids selectively reporting and interpreting few selected results that would pass a multiple-comparison threshold but might not well represent the true underlying effect in a medium-power setting. The finding of group effects in HC statistics not being observed in the conventional mass-univariate analysis might indicate that substantially larger samples are desirable in future rs-fMRI studies in neurodevelopmental disorders such as FAS. This is, however, limited by the rarity of these disorders [98]. Recent work in a related field further highlights the potential specific relevance of a network-perspective and limitations of group mean comparisons at the regional perspective: Segal et al. observed that structural brain alterations in individuals with mental disorders mainly converge at the network level while effects on the regional level are sparse and heterogeneous [99]. Please see the “Methods” section for a more detailed description of the HC-based multi-level approach and underlying rationale, as well as the “Potential limitations” section for further methodical aspects.
No evidence of group differences in dynamic functional connectivity (additional exploratory analysis)
Our findings discussed so far are based on conventional static FC analyses. Clinical features typically observed in FASD include impulsivity or hyperactivity (including overlap/comorbidity with attention deficit hyperactivity disorder) [1, 3, 4]. These clinical features might suggest a potential dynamic or temporally changing nature of underlying neural disease mechanisms. This assumption is supported by dynamic FC alterations previously reported in ADHD [22,23,24]. Contrary to this assumption, we did not observe alterations of features representing non-stationarity in the exploratory time-resolved analysis of dynamical aspects of FC. In particular, compared to controls FAS participants did neither change more or less frequently between two putative FC states, nor did they remain in the different FC states for shorter or longer periods of times. Thus, we did not find evidence of altered dynamic interactions of brain regions of different networks. There is at least some evidence in children, that hyperactivity might be less severe in PAE compared with ADHD [100]. Though those findings cannot be directly translated to adult FAS participants, relatively lower hyperactivity might be the reason for the lack of dynamic FC alterations observed in our study. These findings are also generally in line with a previous rs-fMRI study reporting no alteration in regional temporal variance in less severely affected children with low levels of PAE [101].
Potential limitations
Findings of this first FC analysis in adults with PAE are restricted to young adults (ages 18–32 years) with FAS. They do not necessarily translate to other age groups. Furthermore, findings do also not necessarily translate to other gradations across the FASD spectrum. Despite greater psychopathology, attention deficits, and impulsiveness compared with controls, a recent study did not find network-based FC alterations in a population of adolescents with a wide range of PAE, i.e., less severely exposed individuals [102]. Adult participants with FAS in this sample had been diagnosed during their childhood using the Majewski criteria [37] then widely used in German-speaking countries. These criteria did not gain widespread use in other countries [38]. Although they generally reflect the full clinical picture of FAS (see also Additional_file_1.pdf: supplementary methods), disease severity cannot be exactly mapped onto newer diagnostic criteria [2]. Explicit information about the presence and quantity of maternal alcohol exposure is not available in this sample. This represents a more general limitation of FAS diagnosis both, in research and clinical care: As reflected by current clinical guidelines [8, 103,104,105], FAS can be diagnosed based on the typical clinical picture and does not require explicit knowledge about prenatal alcohol exposure. Similarly, there is a possibility of unknown sub-clinical prenatal alcohol exposure in the control group, potentially reducing the sensitivity for FC group differences. While occasional alcohol consumption has been reported in 14%, regular alcohol consumption during pregnancy has been relatively rarely reported (around 1%) in Germany [106]. Social and psychopathological characterization of the participants and their families is limited: no information about socioeconomic status is available. Socioeconomic inequalities such as parental income, educational status, or neighborhood context have been related to differences in structural brain development and to disrupted development of cognitive abilities [107]. Early SES disadvantage in childhood has been associated with altered resting-state functional connectivity of brain networks involved in cognition [108]. Children with FASD are frequently exposed to such adverse experiences when growing up [109,110,111]. In addition to the influence of prenatal alcohol exposure itself, SES might therefore pose an independent factor that could have interfered with brain development in our sample [110]. Future research is needed to highlight the effects of the additional burden imposed upon FASD subjects by socioeconomic disadvantage and the associated implications on brain structure and activity in affected individuals. Information on psychiatric comorbidity for the exclusion criteria is based on anamnestic information and a screening tool (SSQ), but not on detailed assessment within this study or on previously assigned ICD or DSM diagnostic codes. We did not include total brain volume and IQ in the statistical models of FC alterations, since both reduced IQs [1] and reduced total brain volumes [112, 113] are considered disease features of FAS with the potential for overcorrection if included as covariates [114].
Taking differences in head motion into account in rs-fMRI studies in clinical populations is a matter of ongoing critical debate [115]. Although we have taken precautions to minimize head motion, excluded participants with excessive head motion, include head motion in the analyses and even though measures did not differ significantly between groups, it cannot be excluded that parts of the results are movement-related [53, 115]. The state-of-the-art motion correction methods during data pre-processing are very similar to those showing a particularly good performance in an additional large-scale benchmarking study of rs-fMRI motion correction strategies [115]. We have also included head motion as a covariate in the main FC group analyses at the level of individual connections to further take a potential movement bias into account. This also means that connections with different distances between brain regions were modelled separately at this stage. We refrained from including global signal regression since it may confound the directionality of FC estimates and aggravate potential distance-related effects of residual head motion [115]. In this, context, it should however also be considered that motor restlessness itself is a disease feature in FAS [116].
Statistical power of the final step of the hierarchical analysis approach (resolving FC alterations to single connections between pairs of regions) is potentially limited by the high dimensionality of the underlying atlas. This notion is also supported by the distribution of effect size estimates for group differences of individual connections. This atlas resolution was chosen because it is extensively validated [56] and aims to optimally reflect the brain’s functional architecture [56, 117]. The HC-based approach was chosen here instead of averaging FC estimates to allow global and network-wise inference while maintaining the advantages of the high-resolution atlas. Findings are limited to the cortex and do not include subcortical gray matter nuclei within these networks [118, 119]. It has to be noted that there is an ongoing debate about functional network nomenclature, so that the networks described here [56] may deviate from studies using other atlases [120].
Though widely used in other research areas with high-dimensional data [60, 63], the HC statistic has only recently been introduced to fMRI [64, 65, 96]. The HC statistic primarily assumes statistically independent features, since correlations among features can lead to unbalanced p-value histograms, however without expecting peaks in the first histogram bin (low p-values). It has thus been argued that the influence of correlations among features is negligible when the underlying histograms show typical behavior [62]. In addition to the HC statistic, we therefore visually interpreted the underlying p-value histograms as a plausibility control and observed well-behaved p-value histograms in the global and within-network analysis and to a slightly lesser degree in the between-network analysis. The HC-based global hypothesis test does not directly result in p-values but in a primary decision to reject/retain the corresponding global null hypothesis. However, p-values for typical HC values have been approximated [121]. Even when using these approximated p-values, thus departing from the notion of the original HC statistic, main results would be statistically significant at the p < 0.05 level or stricter p-values.
Dynamic or time-resolved FC analysis is a promising, already widely used, yet still evolving rs-fMRI analysis method [15,16,17]. Thus, there is currently a relatively high methodological variability [15, 17]. Here, we adopted a widely used sliding window approach [17] and refrained from extensively exploring analysis settings in order to avoid false-positive findings [122]. Hence, there is a risk to miss group differences of FC dynamics which might have been uncovered with other, less well-established dynamic FC analysis approaches [15, 17, 123]. Furthermore, FC states themselves, which were estimated in the entire sample here, might be intrinsically different in both groups. This might be addressed by separate FC state estimation, however will need in the future more advanced methodology for subsequent actual group comparison. Similar to methodological heterogeneity and open methodological questions, there is still no consensus of connectivity states to be expected in a normal population. However, a relatively small number of FC states partially reflecting changing interactions of parts of the DMN, similar to those observed here (Additional_file_1.pdf: Supplementary Fig. 2) has been repeatedly reported [17, 124]. Silhouette values (Additional_file_1.pdf: Supplementary Fig. 1) indicate that clusters observed in our analysis may not be well separated. Thus, these two clusters capture dynamic FC changes as a model but might not represent truly discrete FC states in a neurobiological sense. Cluster frequencies suggest a high inter-subject variability. Despite these general limitations of this evolving methodology, we believe that our exploratory approach can be a starting point for further investigations on dynamic FC in FAS and other neurodevelopmental disorders.
Conclusions
We observed altered FC in cognition-related brain networks in young adults with FAS. Using a HC-based statistical approach, this study provides evidence of the existence of at least rare and weak effects (i.e., FC differences between participants with FAS and controls) widely distributed across a majority of these networks, potentially underlying the diversity of cognitive deficits in these individuals. Findings were pronounced in attention-related sub-networks, which is in line with substantial attentional deficits previously reported. Relevant for comparisons with previous studies is that—in contrast with network-level results—the most detailed analysis level using a more conventional mass-univariate approach did not identify significant group differences. Thus, findings could not be resolved to single functional connections. An exploratory time-resolved analysis did also not identify altered FC dynamics and could thus not explain reduced impulse control and attention deficits which have been frequently reported in FAS.
Availability of data and materials
On request to the authors, further intermediate data on a level independent from the individual participants can be shared. Due to German data protection regulations and to safeguard subject confidentiality, data on the level of individual participants cannot be made available (no participant consent for sharing these primary data).
Software and statistical algorithms used for these analyses are freely available as referenced in the “Methods” section. Further in-house code was used for individual aspects of data handling only and could be made available to other researchers on reasonable request.
Abbreviations
- ADHD:
-
Attention deficit hyperactivity disorder
- BIDS:
-
Brain Imaging Data Structure
- DMN:
-
Default mode network
- EHI:
-
Edinburgh Handedness Inventory
- FAS:
-
Fetal alcohol syndrome
- FASD:
-
Fetal alcohol spectrum disorders
- FC:
-
Functional connectivity
- FD:
-
Frame-wise displacement
- FDR:
-
False discovery rate
- fMRI:
-
Functional magnetic resonance imaging
- FRC:
-
Frequency of observing each cluster
- FWHM:
-
Full width at half maximum
- HC:
-
Higher criticism
- MDT:
-
Mean dwell time
- MRI:
-
Magnetic resonance imaging
- NT:
-
Number of transitions
- PAE:
-
Prenatal alcohol exposure
- rs-fMRI:
-
Resting-state functional magnetic resonance imaging
- SSQ:
-
Stamm-Screening questionnaire
- TFE:
-
Turbo field echo
- TMT:
-
Trail-making task
References
Davis KM, Gagnier KR, Moore TE, Todorow M. Cognitive aspects of fetal alcohol spectrum disorder. Wiley Interdiscip Rev Cogn Sci. 2013;4(1):81–92.
Popova S, Charness ME, Burd L, Crawford A, Hoyme HE, Mukherjee RAS, Riley EP, Elliott EJ. Fetal alcohol spectrum disorders. Nat Rev Dis Primers. 2023;9(1):11.
Kodituwakku P, Coriale G, Fiorentino D, Aragon AS, Kalberg WO, Buckley D, Gossage JP, Ceccanti M, May PA. Neurobehavioral characteristics of children with fetal alcohol spectrum disorders in communities from Italy: Preliminary results. Alcohol Clin Exp Res. 2006;30(9):1551–61.
Dorrie N, Focker M, Freunscht I, Hebebrand J. Fetal alcohol spectrum disorders. Eur Child Adolesc Psychiatry. 2014;23(10):863–75.
Day NL, Helsel A, Sonon K, Goldschmidt L. The association between prenatal alcohol exposure and behavior at 22 years of age. Alcohol Clin Exp Res. 2013;37(7):1171–8.
Moore EM, Riley EP. What Happens When Children with Fetal Alcohol Spectrum Disorders Become Adults? Curr Dev Disord Rep. 2015;2(3):219–27.
Wozniak JR, Riley EP, Charness ME. Clinical presentation, diagnosis, and management of fetal alcohol spectrum disorder. Lancet Neurol. 2019;18(8):760–70.
Hoyme HE, Kalberg WO, Elliott AJ, Blankenship J, Buckley D, Marais AS, Manning MA, Robinson LK, Adam MP, Abdul-Rahman O et al: Updated Clinical Guidelines for Diagnosing Fetal Alcohol Spectrum Disorders. Pediatrics 2016, 138(2).
Donald KA, Eastman E, Howells FM, Adnams C, Riley EP, Woods RP, Narr KL, Stein DJ. Neuroimaging effects of prenatal alcohol exposure on the developing human brain: a magnetic resonance imaging review. Acta Neuropsychiatr. 2015;27(5):251–69.
Niendam TA, Laird AR, Ray KL, Dean YM, Glahn DC, Carter CS. Meta-analytic evidence for a superordinate cognitive control network subserving diverse executive functions. Cogn Affect Behav Neurosci. 2012;12(2):241–68.
Menon V. Large-scale brain networks and psychopathology: a unifying triple network model. Trends Cogn Sci. 2011;15(10):483–506.
Duncan J. The multiple-demand (MD) system of the primate brain: mental programs for intelligent behaviour. Trends Cogn Sci. 2010;14(4):172–9.
Smith SM, Fox PT, Miller KL, Glahn DC, Fox PM, Mackay CE, Filippini N, Watkins KE, Toro R, Laird AR, et al. Correspondence of the brain’s functional architecture during activation and rest. Proc Natl Acad Sci U S A. 2009;106(31):13040–5.
van den Heuvel MP, Hulshoff Pol HE. Exploring the brain network: a review on resting-state fMRI functional connectivity. Eur Neuropsychopharmacol. 2010;20(8):519–34.
Iraji A, Faghiri A, Lewis N, Fu Z, Rachakonda S, Calhoun VD. Tools of the trade: estimating time-varying connectivity patterns from fMRI data. Soc Cogn Affect Neurosci. 2021;16(8):849–74.
Vidaurre D, Smith SM, Woolrich MW. Brain network dynamics are hierarchically organized in time. Proc Natl Acad Sci U S A. 2017;114(48):12827–32.
Preti MG, Bolton TA, Van De Ville D. The dynamic functional connectome: State-of-the-art and perspectives. Neuroimage. 2017;160:41–54.
Fong AHC, Yoo K, Rosenberg MD, Zhang S, Li CR, Scheinost D, Constable RT, Chun MM. Dynamic functional connectivity during task performance and rest predicts individual differences in attention across studies. Neuroimage. 2019;188:14–25.
Madhyastha TM, Askren MK, Boord P, Grabowski TJ. Dynamic connectivity at rest predicts attention task performance. Brain Connect. 2015;5(1):45–59.
Abdallah M, Farrugia N, Chirokoff V, Chanraud S. Static and dynamic aspects of cerebro-cerebellar functional connectivity are associated with self-reported measures of impulsivity: A resting-state fMRI study. Netw Neurosci. 2020;4(3):891–909.
Rafi H, Delavari F, Perroud N, Derome M, Debbane M. The continuum of attention dysfunction: Evidence from dynamic functional network connectivity analysis in neurotypical adolescents. PLoS ONE. 2023;18(1):e0279260.
Yang Y, Yang B, Zhang L, Peng G, Fang D. Dynamic Functional Connectivity Reveals Abnormal Variability in the Amygdala Subregions of Children With Attention-Deficit/Hyperactivity Disorder. Front Neurosci. 2021;15:648143.
Ahmadi M, Kazemi K, Kuc K, Cybulska-Klosowicz A, Helfroush MS, Aarabi A: Resting state dynamic functional connectivity in children with attention deficit/hyperactivity disorder. J Neural Eng 2021, 18(4).
Agoalikum E, Klugah-Brown B, Yang H, Wang P, Varshney S, Niu B, Biswal B. Differences in Disrupted Dynamic Functional Network Connectivity Among Children, Adolescents, and Adults With Attention Deficit/Hyperactivity Disorder: A Resting-State fMRI Study. Front Hum Neurosci. 2021;15:697696.
Fan J, Taylor PA, Jacobson SW, Molteno CD, Gohel S, Biswal BB, Jacobson JL, Meintjes EM. Localized reductions in resting-state functional connectivity in children with prenatal alcohol exposure. Hum Brain Mapp. 2017;38(10):5217–33.
Little G, Reynolds J, Beaulieu C. Altered Functional Connectivity Observed at Rest in Children and Adolescents Prenatally Exposed to Alcohol. Brain Connect. 2018;8(8):503–15.
Ware AL, Long X, Lebel C. Functional connectivity of the attention networks is altered and relates to neuropsychological outcomes in children with prenatal alcohol exposure. Dev Cogn Neurosci. 2021;48:100951.
Wozniak JR, Mueller BA, Mattson SN, Coles CD, Kable JA, Jones KL, Boys CJ, Lim KO, Riley EP, Sowell ER, et al. Functional connectivity abnormalities and associated cognitive deficits in fetal alcohol Spectrum disorders (FASD). Brain Imaging Behav. 2017;11(5):1432–45.
Wozniak JR, Mueller BA, Bell CJ, Muetzel RL, Hoecker HL, Boys CJ, Lim KO. Global functional connectivity abnormalities in children with fetal alcohol spectrum disorders. Alcohol Clin Exp Res. 2013;37(5):748–56.
Long X, Kar P, Gibbard B, Tortorelli C, Lebel C. The brain’s functional connectome in young children with prenatal alcohol exposure. Neuroimage Clin. 2019;24:102082.
Rodriguez CI, Vergara VM, Calhoun VD, Savage DD, Hamilton DA, Tesche CD, Stephen JM. Disruptions in global network segregation and integration in adolescents and young adults with fetal alcohol spectrum disorder. Alcohol Clin Exp Res. 2021;45(9):1775–89.
Santhanam P, Coles CD, Li Z, Li L, Lynch ME, Hu X. Default mode network dysfunction in adults with prenatal alcohol exposure. Psychiatry Res. 2011;194(3):354–62.
Wozniak JR, Mueller BA, Muetzel RL, Bell CJ, Hoecker HL, Nelson ML, Chang PN, Lim KO. Inter-hemispheric functional connectivity disruption in children with prenatal alcohol exposure. Alcohol Clin Exp Res. 2011;35(5):849–61.
Long X, Little G, Beaulieu C, Lebel C. Sensorimotor network alterations in children and youth with prenatal alcohol exposure. Hum Brain Mapp. 2018;39(5):2258–68.
Sundermann B, Garde S, Dehghan Nayyeri M, Weglage J, Rau J, Pfleiderer B, Feldmann R. Approaching altered inhibitory control in phenylketonuria: A functional MRI study with a Go-NoGo task in young female adults. Eur J Neurosci. 2020;52(8):3951–62.
Rau JMH, Sundermann B, Pfleiderer B, Dehghan-Nayyeri M, Garde S, Weglage J, Feldmann R: Inhibitory control in young adult women with fetal alcohol syndrome: Findings from a pilot functional magnetic resonance imaging study. Alcohol: Clinical and Experimental Research 2023, 47(3):600–612.
Majewski F: Untersuchungen zur Alkoholembryopathie: Thieme Stuttgart/New York; 1980.
Autti-Ramo I. Foetal alcohol syndrome–a multifaceted condition. Dev Med Child Neurol. 2002;44(2):141–4.
Famy C, Streissguth AP, Unis AS. Mental illness in adults with fetal alcohol syndrome or fetal alcohol effects. Am J Psychiatry. 1998;155(4):552–4.
van Ruitenbeek P, Vermeeren A, Mehta MA, Drexler EI, Riedel WJ. Antihistamine induced blood oxygenation level dependent response changes related to visual processes during sensori-motor performance. Hum Brain Mapp. 2014;35(7):3095–106.
Sundermann B, Pfleiderer B, Minnerup H, Berger K, Douaud G. Interaction of Developmental Venous Anomalies with Resting-State Functional MRI Measures. AJNR Am J Neuroradiol. 2018;39(12):2326–31.
Dosenbach NU, Nardos B, Cohen AL, Fair DA, Power JD, Church JA, Nelson SM, Wig GS, Vogel AC, Lessov-Schlaggar CN, et al. Prediction of individual brain maturity using fMRI. Science. 2010;329(5997):1358–61.
Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. 1971;9(1):97–113.
Oswald WD, Roth E: Der Zahlenverbindungstest (ZVT). Ein sprachfreier Intelligenz-Test zur Messung der “kognitiven Leistungsgeschwindigkeit”. , 2nd edn. Göttingen: Hogrefe; 1987.
Wittchen HU, Pfister H: DIA-X-Interviews: Manual für Screening-Verfahren und Interview; Interviewheft Längsschnittuntersuchung (DIA-X-Lifetime); Ergänzungsheft (DIA-X-Lifetime); Interviewheft Querschnittuntersuchung (DIA-X-12 Monate); Ergänzungsheft (DIA-X-12 Monate); PC-Programm zur Durchführung des Interviews (Längs- und Querschnittuntersuchung); Auswertungsprogramm. Frankfurt: Swets & Zeitlinger; 1997.
Salthouse TA. What cognitive abilities are involved in trail-making performance? Intelligence. 2011;39(4):222–32.
Gorgolewski KJ, Auer T, Calhoun VD, Craddock RC, Das S, Duff EP, Flandin G, Ghosh SS, Glatard T, Halchenko YO, et al. The brain imaging data structure, a format for organizing and describing outputs of neuroimaging experiments. Sci Data. 2016;3:160044.
Wulms N: BiDirect-BIDS-ConverteR. 2019.
Wulms N, Eppe S, Dehghan-Nayyeri M, Streeter AJ, Bonberg N, Berger K, Sundermann B, Minnerup H. The R package for DICOM to brain imaging data structure conversion. Sci Data. 2023;10(1):673.
Bischoff-Grethe A, Ozyurt IB, Busa E, Quinn BT, Fennema-Notestine C, Clark CP, Morris S, Bondi MW, Jernigan TL, Dale AM, et al. A technique for the deidentification of structural brain MR images. Hum Brain Mapp. 2007;28(9):892–903.
Esteban O, Markiewicz CJ, Blair RW, Moodie CA, Isik AI, Erramuzpe A, Kent JD, Goncalves M, DuPre E, Snyder M, et al. fMRIPrep: a robust preprocessing pipeline for functional MRI. Nat Methods. 2019;16(1):111–6.
Finc KCM, Bonna K. fMRIDenoise: automated denoising, denoising strategies comparison, and functional connectivity data quality control. 2021. https://doi.org/10.5281/zenodo.4458072.
Satterthwaite TD, Elliott MA, Gerraty RT, Ruparel K, Loughead J, Calkins ME, Eickhoff SB, Hakonarson H, Gur RC, Gur RE, et al. An improved framework for confound regression and filtering for control of motion artifact in the preprocessing of resting-state functional connectivity data. Neuroimage. 2013;64:240–56.
Power JD, Barnes KA, Snyder AZ, Schlaggar BL, Petersen SE. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. Neuroimage. 2012;59(3):2142–54.
Ciric R, Thompson WH, Lorenz R, Goncalves M, MacNicol EE, Markiewicz CJ, Halchenko YO, Ghosh SS, Gorgolewski KJ, Poldrack RA, et al. TemplateFlow: FAIR-sharing of multi-scale, multi-species brain models. Nat Methods. 2022;19(12):1568–71.
Schaefer A, Kong R, Gordon EM, Laumann TO, Zuo XN, Holmes AJ, Eickhoff SB, Yeo BTT. Local-Global Parcellation of the Human Cerebral Cortex from Intrinsic Functional Connectivity MRI. Cereb Cortex. 2018;28(9):3095–114.
Yeo BT, Krienen FM, Sepulcre J, Sabuncu MR, Lashkari D, Hollinshead M, Roffman JL, Smoller JW, Zollei L, Polimeni JR, et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol. 2011;106(3):1125–65.
Chao-Gan Y, Yu-Feng Z. DPARSF: A MATLAB Toolbox for “Pipeline” Data Analysis of Resting-State fMRI. Front Syst Neurosci. 2010;4:13.
Sundermann B, Feldmann R, Mathys C, Rau J, Garde S, Braje A, Weglage J, Pfleiderer B. Functional connectivity of cognition-related brain networks in adults with fetal alcohol syndrome. medRxiv. 2023. https://doi.org/10.1101/2023.05.18.23289319.
Donoho D, Jin J. Higher Criticism for Large-Scale Inference, Especially for Rare and Weak Effects. Stat Sci. 2015;30(1):1–25.
Donoho D, Jin J. Higher criticism for detecting sparse heterogeneous mixtures. Ann Stat. 2004;32(3):962–94.
Breheny P, Stromberg A, Lambert J: p-Value Histograms: Inference and Diagnostics. High Throughput 2018, 7(3).
Cai TT, Sun W. Large-Scale Global and Simultaneous Inference: Estimation and Testing in Very High Dimensions. Annual Review of Economics. 2017;9(1):411–39.
Gerlach AR, Karim HT, Kazan J, Aizenstein HJ, Krafty RT, Andreescu C. Networks of worry-towards a connectivity-based signature of late-life worry using higher criticism. Transl Psychiatry. 2021;11(1):550.
Wilson JD, Gerlach AR, Karim HT, Aizenstein HJ, Andreescu C. Sex matters: acute functional connectivity changes as markers of remission in late-life depression differ by sex. Mol Psychiatry. 2023. Online ahead of print. https://doi.org/10.1038/s41380-023-02158-0.
Yekutieli D, Benjamini Y. Resampling-based false discovery rate controlling multiple test procedures for correlated test statistics. J Stat Plann Inference. 1999;82(1):171–96.
Liao W, Wu GR, Xu Q, Ji GJ, Zhang Z, Zang YF, Lu G. DynamicBC: a MATLAB toolbox for dynamic brain connectome analysis. Brain Connect. 2014;4(10):780–90.
Damaraju E, Allen EA, Belger A, Ford JM, McEwen S, Mathalon DH, Mueller BA, Pearlson GD, Potkin SG, Preda A, et al. Dynamic functional connectivity analysis reveals transient states of dysconnectivity in schizophrenia. Neuroimage Clin. 2014;5:298–308.
Li J, Zhang D, Liang A, Liang B, Wang Z, Cai Y, Gao M, Gao Z, Chang S, Jiao B, et al. High transition frequencies of dynamic functional connectivity states in the creative brain. Sci Rep. 2017;7:46072.
Caliński T, Harabasz J. A dendrite method for cluster analysis. Commun Stat. 1974;3(1):1–27.
Davies DL, Bouldin DW: A Cluster Separation Measure. IEEE Transactions on Pattern Analysis and Machine Intelligence 1979, PAMI-1(2):224–227.
Rousseeuw PJ. Silhouettes: A graphical aid to the interpretation and validation of cluster analysis. J Comput Appl Math. 1987;20:53–65.
Coles CD, Platzman KA, Lynch ME, Freides D. Auditory and visual sustained attention in adolescents prenatally exposed to alcohol. Alcohol Clin Exp Res. 2002;26(2):263–71.
Gautam P, Nunez SC, Narr KL, Mattson SN, May PA, Adnams CM, Riley EP, Jones KL, Kan EC, Sowell ER. Developmental Trajectories for Visuo-Spatial Attention are Altered by Prenatal Alcohol Exposure: A Longitudinal FMRI Study. Cereb Cortex. 2015;25(12):4761–71.
Kooistra L, Crawford S, Gibbard B, Ramage B, Kaplan BJ. Differentiating attention deficits in children with fetal alcohol spectrum disorder or attention-deficit-hyperactivity disorder. Dev Med Child Neurol. 2010;52(2):205–11.
Brown RT, Coles CD, Smith IE, Platzman KA, Silverstein J, Erickson S, Falek A. Effects of prenatal alcohol exposure at school age II Attention and behavior. Neurotoxicol Teratol. 1991;13(4):369–76.
Infante MA, Moore EM, Nguyen TT, Fourligas N, Mattson SN, Riley EP. Objective assessment of ADHD core symptoms in children with heavy prenatal alcohol exposure. Physiol Behav. 2015;148:45–50.
Connor PD, Streissguth AP, Sampson PD, Bookstein FL, Barr HM. Individual differences in auditory and visual attention among fetal alcohol-affected adults. Alcohol Clin Exp Res. 1999;23(8):1395–402.
Hutzler F. Reverse inference is not a fallacy per se: cognitive processes can be inferred from functional imaging data. Neuroimage. 2014;84:1061–9.
Poldrack RA. Can cognitive processes be inferred from neuroimaging data? Trends Cogn Sci. 2006;10(2):59–63.
Candelaria-Cook FT, Schendel ME, Flynn L, Hill DE, Stephen JM. Altered Resting-State Neural Oscillations and Spectral Power in Children with Fetal Alcohol Spectrum Disorder. Alcohol Clin Exp Res. 2021;45(1):117–30.
Long X, Little G, Treit S, Beaulieu C, Gong G, Lebel C. Altered brain white matter connectome in children and adolescents with prenatal alcohol exposure. Brain Struct Funct. 2020;225(3):1123–33.
Zanto TP, Gazzaley A. Fronto-parietal network: flexible hub of cognitive control. Trends Cogn Sci. 2013;17(12):602–3.
Kodali VN, Jacobson JL, Lindinger NM, Dodge NC, Molteno CD, Meintjes EM, Jacobson SW. Differential Recruitment of Brain Regions During Response Inhibition in Children Prenatally Exposed to Alcohol. Alcohol Clin Exp Res. 2017;41(2):334–44.
Infante MA, Moore EM, Bischoff-Grethe A, Tapert SF, Mattson SN, Riley EP. Altered functional connectivity during spatial working memory in children with heavy prenatal alcohol exposure. Alcohol. 2017;64:11–21.
Fox MD, Snyder AZ, Vincent JL, Corbetta M, Van Essen DC, Raichle ME. The human brain is intrinsically organized into dynamic, anticorrelated functional networks. Proc Natl Acad Sci U S A. 2005;102(27):9673–8.
Smith V, Mitchell DJ, Duncan J. Role of the Default Mode Network in Cognitive Transitions. Cereb Cortex. 2018;28(10):3685–96.
Crittenden BM, Mitchell DJ, Duncan J. Recruitment of the default mode network during a demanding act of executive control. Elife. 2015;4:e06481.
Andrews-Hanna JR, Reidler JS, Sepulcre J, Poulin R, Buckner RL. Functional-anatomic fractionation of the brain’s default network. Neuron. 2010;65(4):550–62.
Cremers HR, Wager TD, Yarkoni T. The relation between statistical power and inference in fMRI. PLoS ONE. 2017;12(11): e0184923.
Ioannidis JP. Why most published research findings are false. PLoS Med. 2005;2(8):e124.
Yarkoni T: Big Correlations in Little Studies: Inflated fMRI Correlations Reflect Low Statistical Power-Commentary on Vul et al. (2009). Perspect Psychol Sci 2009, 4(3):294–298.
Yarkoni T, Braver TS: Cognitive Neuroscience Approaches to Individual Differences in Working Memory and Executive Control: Conceptual and Methodological Issues. In: Handbook of Individual Differences in Cognition: Attention, Memory, and Executive Control. edn. Edited by Gruszka A, Matthews G, Szymura B. New York, NY: Springer New York; 2010: 87–107.
Chen G, Taylor PA, Cox RW. Is the statistic value all we should care about in neuroimaging? Neuroimage. 2017;147:952–9.
Taylor PA, Reynolds RC, Calhoun V, Gonzalez-Castillo J, Handwerker DA, Bandettini PA, Mejia AF, Chen G. Highlight Results, Don’t Hide Them: Enhance interpretation, reduce biases and improve reproducibility. Neuroimage. 2023;274:120138.
Sundermann B, Pfleiderer B, McLeod A, Mathys C. Seeing more than the tip of the iceberg: Approaches to subthreshold effects in functional magnetic resonance imaging of the brain. PsyArXiv Preprints. 2023. https://doi.org/10.31234/osf.io/fyhst.
Gorgolewski KJ, Varoquaux G, Rivera G, Schwarz Y, Ghosh SS, Maumet C, Sochat VV, Nichols TE, Poldrack RA, Poline JB et al: NeuroVault.org: a web-based repository for collecting and sharing unthresholded statistical maps of the human brain. Front Neuroinform 2015, 9:8.
Bednarz HM, Kana RK. Advances, challenges, and promises in pediatric neuroimaging of neurodevelopmental disorders. Neurosci Biobehav Rev. 2018;90:50–69.
Segal A, Parkes L, Aquino K, Kia SM, Wolfers T, Franke B, Hoogman M, Beckmann CF, Westlye LT, Andreassen OA, et al. Regional, circuit and network heterogeneity of brain abnormalities in psychiatric disorders. Nat Neurosci. 2023;26(9):1613–29.
Glass L, Graham DM, Deweese BN, Jones KL, Riley EP, Mattson SN. Correspondence of parent report and laboratory measures of inattention and hyperactivity in children with heavy prenatal alcohol exposure. Neurotoxicol Teratol. 2014;42:43–50.
Long X, Lebel C. Evaluation of Brain Alterations and Behavior in Children With Low Levels of Prenatal Alcohol Exposure. JAMA Netw Open. 2022;5(4):e225972.
Lees B, Mewton L, Jacobus J, Valadez EA, Stapinski LA, Teesson M, Tapert SF, Squeglia LM. Association of Prenatal Alcohol Exposure With Psychological, Behavioral, and Neurodevelopmental Outcomes in Children From the Adolescent Brain Cognitive Development Study. Am J Psychiatry. 2020;177(11):1060–72.
Koehlmoos TP, Lee E, Wisdahl J, Donaldson T. Fetal alcohol spectrum disorders prevention and clinical guidelines research-workshop report. BMC Proc. 2023;17(Suppl 12):19.
Cook JL, Green CR, Lilley CM, Anderson SM, Baldwin ME, Chudley AE, Conry JL, LeBlanc N, Loock CA, Lutke J, et al. Fetal alcohol spectrum disorder: a guideline for diagnosis across the lifespan. CMAJ. 2016;188(3):191–7.
Landgraf MN, Heinen F: S3-Leitlinie Diagnose der Fetalen Alkoholspektrumstörungen. Langfassung. . AWMF-Registernummer: 022–025 2016.
Bergmann KE, Bergmann RL, Ellert U, Dudenhausen JW. Perinatale Einflussfaktoren auf die spätere Gesundheit. Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz. 2007;50(5):670–6.
Brito NH, Noble KG. Socioeconomic status and structural brain development. Front Neurosci. 2014;8:276.
Rakesh D, Zalesky A, Whittle S. Similar but distinct - Effects of different socioeconomic indicators on resting state functional connectivity: Findings from the Adolescent Brain Cognitive Development (ABCD) Study(R). Dev Cogn Neurosci. 2021;51:101005.
Lebel CA, McMorris CA, Kar P, Ritter C, Andre Q, Tortorelli C, Gibbard WB. Characterizing adverse prenatal and postnatal experiences in children. Birth Defects Res. 2019;111(12):848–58.
McLachlan K, Zhou D, Little G, Rasmussen C, Pei J, Andrew G, Reynolds JN, Beaulieu C. Current Socioeconomic Status Correlates With Brain Volumes in Healthy Children and Adolescents but Not in Children With Prenatal Alcohol Exposure. Front Hum Neurosci. 2020;14:223.
Popova S, Lange S, Shield K, Burd L, Rehm J. Prevalence of fetal alcohol spectrum disorder among special subpopulations: a systematic review and meta-analysis. Addiction. 2019;114(7):1150–72.
Lebel C, Roussotte F, Sowell ER. Imaging the impact of prenatal alcohol exposure on the structure of the developing human brain. Neuropsychol Rev. 2011;21(2):102–18.
Lebel C, Ware A: Magnetic Resonance Imaging in Fetal Alcohol Spectrum Disorder (FASD). In: Neurodevelopmental Pediatrics: Genetic and Environmental Influences. edn. Edited by Eisenstat DD, Goldowitz D, Oberlander TF, Yager JY. Cham: Springer International Publishing; 2023: 397–407.
Dennis M, Francis DJ, Cirino PT, Schachar R, Barnes MA, Fletcher JM. Why IQ is not a covariate in cognitive studies of neurodevelopmental disorders. J Int Neuropsychol Soc. 2009;15(3):331–43.
Parkes L, Fulcher B, Yucel M, Fornito A. An evaluation of the efficacy, reliability, and sensitivity of motion correction strategies for resting-state functional MRI. Neuroimage. 2018;171:415–36.
Spohr HL, Steinhausen HC. Fetal alcohol spectrum disorders and their persisting sequelae in adult life. Dtsch Arztebl Int. 2008;105(41):693–8.
Craddock RC, James GA, Holtzheimer PE 3rd, Hu XP, Mayberg HS. A whole brain fMRI atlas generated via spatially constrained spectral clustering. Hum Brain Mapp. 2012;33(8):1914–28.
Alves PN, Foulon C, Karolis V, Bzdok D, Margulies DS, Volle E. Thiebaut de Schotten M: An improved neuroanatomical model of the default-mode network reconciles previous neuroimaging and neuropathological findings. Commun Biol. 2019;2:370.
Sundermann B, Pfleiderer B. Functional connectivity profile of the human inferior frontal junction: involvement in a cognitive control network. BMC Neurosci. 2012;13:119.
Uddin LQ, Yeo BTT, Spreng RN. Towards a Universal Taxonomy of Macro-scale Functional Human Brain Networks. Brain Topogr. 2019;32(6):926–42.
Li J, Siegmund D: Higher criticism: p-values and criticism. The Annals of Statistics 2015, 43(3):1323–1350, 1328.
Carp J. On the plurality of (methodological) worlds: estimating the analytic flexibility of FMRI experiments. Front Neurosci. 2012;6:149.
Hindriks R, Adhikari MH, Murayama Y, Ganzetti M, Mantini D, Logothetis NK, Deco G. Can sliding-window correlations reveal dynamic functional connectivity in resting-state fMRI? Neuroimage. 2016;127:242–56.
Allen EA, Damaraju E, Plis SM, Erhardt EB, Eichele T, Calhoun VD. Tracking whole-brain connectivity dynamics in the resting state. Cereb Cortex. 2014;24(3):663–76.
Bell S. The write algorithm: promoting responsible artificial intelligence usage and accountability in academic writing. BMC Med. 2023;21(1):334.
Acknowledgements
We thank all participants for taking part in this study. We acknowledge the kind support of staff at the Translational Research Imaging Center (University Hospital Muenster, Clinic of Radiology). We thank Mahboobeh Dehghan Nayyeri and Niklas Wulms for assistance with BIDS data handling, and Anke McLeod for insightful discussions on the manuscript and assistance with manuscript editing. The color scheme representing networks in Figs. 1 and 4 has been inspired by Paul Tol’s guide on accessible color schemes (https://personal.sron.nl/~pault/data/colourschemes.pdf). Half-violin plots were generated with Bastian Bechtold’s Matlab plugin (https://github.com/bastibe/Violinplot-Matlab, DOI: 10.5281/zenodo.4559847). ChatGPT (GPT3.5, http://chat.openai.com/) was used for minor programming assistance (suggestions for efficient Matlab code structure) during the preparation of the revision (R1) of this manuscript in September 2023. After using this tool, the author (BS) reviewed the output and takes full responsibility for the resulting analyses in line with recommendations in a previous BMC Medicine editorial [125]. Preliminary results of this study have been presented at the 2023 annual meeting of the International Society for Magnetic Resonance in Medicine (ISMRM), program number 3336. We acknowledge support from the open access publication fund of the University of Münster.
Funding
Open Access funding enabled and organized by Projekt DEAL. Data acquisition in a subgroup of the control participants overlapped with a sister project [35] which was financially supported by Merck-Serono, Darmstadt, Germany. The sponsor had no influence on any aspects of the study including design, recruitment. We acknowledge support from the Open Access Publication Fund of the University of Muenster.
Author information
Authors and Affiliations
Contributions
BS, BP, RF, and JW conceived and designed the study. BS, RF, JR, SG, AB, and BP collected the data. BS and BP carried out main data analyses. CM, SG, AB, and JR contributed to or supervised parts of the data analysis. BS, BP, CM, RF, and JR interpreted the results. BS drafted the manuscript. All authors contributed to the manuscript for important intellectual content, approved the final manuscript and agree to take responsibility according to the journal guidelines.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of the University of Münster and the Westphalian Chamber of Physicians in Münster (reference number: 2012–314-f-s with amendment). All study procedures were carried out after obtaining written informed consent and in accordance with the Declaration of Helsinki.
Consent for publication
Participants provided informed consent for publication of study results. Consent for publication of individual data: not applicable (no individual data reported).
Competing interests
Christian Mathys: consulting and lecturing for Siemens on behalf of the employer (Evangelisches Krankenhaus Oldenburg). The other authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Document containing all supplementary methods information (rationale of the Majewski criteria for FAS, MRI data pre-processing), supplementary figures and tables (Supplementary Table 1: Group comparison of head motion; Supplementary Figure 1: Goodness-of-fit statistics for different k-means clustering solutions; Supplementary Figure 2: Connectivity matrices representing the two putative functional connectivity (FC) states in the optimal clustering solution of the time-resolved analysis)
Additional file 2.
Detailed naming of regions of interest and order key (overall and within networks)
Additional file 3.
Static functional connectivity differences (differences of z-transformed correlation coefficients averages across groups) between the full set of regions of interest as visualized in Figure 1C.
Additional file 4.
Standardized effect sizes (partial eta2) of static functional connectivity differences as visualized in Figure 1D and ordered identical to additional file 3.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sundermann, B., Feldmann, R., Mathys, C. et al. Functional connectivity of cognition-related brain networks in adults with fetal alcohol syndrome. BMC Med 21, 496 (2023). https://doi.org/10.1186/s12916-023-03208-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12916-023-03208-8