
Abstract
Purpose
To identify MRI-detected anatomical risk factors for non-contact anterior cruciate ligament (ACL) injuries across genders.
Methods
A retrospective analysis was performed on 141 ACL-reconstructed patients (35 females, 106 males) and 142 controls (37 females, 105 males) from January 2020 to April 2022. Inclusion criteria were primary non-contact ACL injuries. The tibial plateau slope, lateral femoral condyle index, Insall-Salvati index, and patellar tendon angle were measured, using binary logistic regression for gender-specific risk evaluation.
Results
Increased lateral tibial plateau slope, reduced intercondylar notch width index, lateral femoral condyle index, and patellar tendon angle correlated with ACL injuries in both genders. The Insall-Salvati index was a significant risk factor in females but not in males.
Conclusion
This study identifies the lateral tibial plateau slope, notch width index, lateral femoral condyle index, and patellar tendon angle at near-extension as risk factors for ACL injuries in both genders, with the Insall-Salvati index also implicated in females.
Similar content being viewed by others


Introduction
Anterior cruciate ligament (ACL) injuries are frequently encountered in sports activities [1, 2], with non-contact ACL injuries—occurring without any collision with another person or object—making up 95% of ACL injuries in ball sports [3]. Such injuries are notably common among young athletes, with prevalence rates as high as 3.7% in certain athletic cohorts [4], and female athletes face higher risks, including hormone levels, muscle strength, and anatomical factors [4]. ACL ruptures lead to instability in the knee, and despite reconstructive efforts, the complete prevention of osteoarthritis remains elusive [5]. Consequently, there is a significant interest in exploring the risk factors for ACL injuries to better identify those at risk and enhance prevention efforts.
Studies have been conducted on factors associated with ACL injuries, such as the link between ACL injuries and the tibial plateau slope (TPS), but these studies often present divergent outcomes [6, 7]. Similarly, debates exist regarding whether the shape of the lateral femoral condyle plays a role in ACL injuries [8, 9]. Additionally, the ACL is subjected to increased shearing forces under the patellar tendon when the knee is extended [10, 11], highlighting the importance of examining the relationship between the patellar tendon angle and the patellar index (Insall-Salvati index) in the context of ACL injuries. Moreover, while many anatomical studies overlook gender differences, a handful suggest that the lateral tibial plateau slope (LTPS) correlates with ACL injuries in females but not in males [12], indicating a potential oversight in studies that do not differentiate by gender due to anatomical variances. Thus, this study aims to elucidate the relationship between gender-specific anatomical characteristics and non-contact ACL injuries. Recognizing the challenges in altering gender and anatomical factors, understanding their associated risks can contribute to targeted screening and preventative strategies for athletes, as well as aid in preventing reinjury after ACL reconstruction. Therefore, this research employs magnetic resonance imaging (MRI) to investigate the anatomical risk factors for non-contact ACL injuries across different genders, with a focus on the tibiofemoral joint and patella.
Methods
A retrospective study was performed on consecutive non-contact ACL reconstruction patients at our institution from January 2020 to April 2022. Inclusion criteria were primary non-contact ACL injuries, focusing on injuries typically due to overexertion or poor sports techniques [13, 14]. Exclusion criteria included: contact ACL injuries, other ligament injuries, skeletal dysplasia, knee fractures, osteoarthritis, prior knee surgeries, incomplete imaging data, and serious systemic diseases. The control group comprised patients without knee injuries, matched by age and gender, who underwent lower limb MRI due to discomfort around the knee joint but had no abnormalities on imaging.
MRI scans were performed using a 1.5 T scanner and a dedicated knee joint coil array (with the scan parameters set as follows: axial T1 phase with a repetition time of 4400ms and echo time of 30ms, sagittal T1 phase with a repetition time of 420ms and echo time of 13ms, and sagittal T2 phase with a repetition time of 3600ms and echo time of 100ms). Slices were set at a thickness of 3 mm, covering the entire anatomical structure between the proximal patella and the distal tibial tuberosity.
Anatomical parameters were measured based on previous studies [15], summarized as follows: Two circles were drawn on the tibia, one tangent to the anterior, posterior, and proximal edges of the tibia, and the other tangent to the anterior and posterior edges. The line connecting the centers of the two circles was defined as the longitudinal axis of the tibia, and similarly, the longitudinal axis of the femur was determined. The radii of the lateral condylar flexion circle (LCFCR) and the lateral condylar extension circle (LCECR) were determined based on the curvature of the lateral femoral condyle during flexion and extension, approximated to two circles, to estimate the shape of the lateral femoral condyle. The lateral femoral condyle index (LFCI) was measured by dividing the radius of the flexion circle by the radius of the extension circle, as described by Hodel, S et al. [16]. Measurements of the medial slopes of the tibial plateau (MTPS) and lateral slopes of the tibial plateau were conducted. The notch width index (NWI) was calculated as the ratio of the notch width to the width across both condyles. The Insall-Salvati index was measured as the length of the patellar tendon over the length of the patella, and the patellar tendon angle was defined as the angle between the patella and the tibia shaft. The measurement methods are illustrated in Fig. 1.

a: Determination of the tibial longitudinal axis; b: Determination of the femoral longitudinal axis; c: Calculation of the LFCI; d:LTPS; e:MTPS; f: NWI; g: Insall-Salvati index; h: Patellar tendon angle
Ethics approval
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Suzhou University, with the ethical review number: JD-HG-2023-41. As this study is an anonymous retrospective study and data analysis, it is not subject to the restrictions of patient informed consent.
Statistical methods
Data analysis employed regression modeling, using binary logistic models for males and females to evaluate the association between ACL injuries and anatomical factors, with ACL status (0 = normal; 1 = injured) as the dependent variable. Receiver operating characteristic (ROC) curve analysis assessed sensitivity and specificity, identifying optimal cutoff values. Analyses were conducted with SPSS 26.0, considering P < 0.05 as statistically significant.
Results
Patient selection
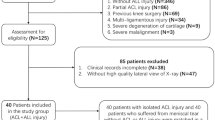
Of 189 patients undergoing primary ACL reconstruction, 48 were excluded due to: additional ligament injuries or subsequent ACL rupture (11), contact injuries or fracture history (16), osteoarthritis (10), incomplete MRI data (8), open growth plates (1), missing knee x-rays (1), and ankylosing spondylitis (1). This resulted in 141 patients with ACL injuries (35 females, 106 males) and 142 controls (37 females, 105 males) included. An independent samples T-test showed no significant age difference between groups (31.9 ± 10.1 vs. 33.4 ± 9.9 years, P = 0.268) (Fig. 2).

Flowchart of patient selection for this study
Binary logistic analysis
The LTPS significantly correlated with ACL injuries in both genders (males P < 0.001, females P = 0.022). Similarly, the NWI was significantly associated with ACL injuries (females P = 0.032, males P < 0.001), as was the LFCI (males P < 0.001, females P = 0.008). The Insall-Salvati index demonstrated significance in females (P = 0.001) but not in males (P = 0.601) (Table 1).
Considering the patellar tendon angle’s dependence on the knee’s flexion-extension angle [11], we could only measure the patellar tendon angle at the knee flexion-extension angle during MRI imaging. The knee joint angle during imaging is generally in a near-extended position as standard, and patients were divided into two groups based on the knee flexion-extension angle: 0–20° and above 20°. The 0–20° group was taken as the standard for binary logistic regression analysis. The results for both men and women were consistent, showing that the angle of the patellar tendon when the knee flexion-extension angle was 0–20° had significant implications for ACL injuries (males P = 0.009, females P = 0.013) (Table 2).
ROC curve analysis
ROC curve analysis for LPTS showed a higher cutoff for females (9.24) than males (6.22), with the males ROC area slightly exceeding the female’s. The LFCI cutoffs were close, at 0.567 for males and 0.551 for females, with the males curve area at 0.737, surpassing the female’s 0.696(Fig. 3).
The NWI’s ROC area was 0.728 for males and 0.700 for females, indicating high sensitivity and specificity, with females having a lower cutoff (0.268) than male(0.283).
The patellar index was significant for females, showing a large ROC area of 0.747 and a cutoff value of 1.218 (Table 3).
With a knee flexion angle < 20°, the patellar tendon angle’s significance varied, having a larger area for females (0.685) than males(0.622). The cutoff was 34.840 for male and 33.095 for females, highlighting gender differences in measurements (Fig. 3).

a: ROC curves for males LTPS, LFCI, and NWI. b: ROC curves for females LTPS, LFCI, NWI, and patellar index. c: ROC curve for males patellar tendon angle; d: ROC curve for females knee patellar tendon angle
Discussion
The most important finding of this study was that the LTPS is an anatomical risk factor for non-contact ACL injuries across genders. The role of the LTPS as a risk factor for ACL injuries has been debated in prior research. Dare et al., in a case-control study, discovered that an increased tibial plateau slope is associated with a heightened risk of ACL injuries [17]. Beynnon et al. observed that an increased tibial plateau slope elevates the risk of non-contact ACL injuries in females, yet they found no such correlation in males [12]. However, research by Hashemi et al. showed that the impact of the tibial plateau slope on ACL injuries shows no gender differences [18]. Our study corroborates that the LTPS is a risk factor in both genders. It also found that the cutoff value for the LTPS in males (6.22°) is significantly lower than in females (9.24°). In addition, the OR value was 1.293 for males and 1.275 for females, with the latter slightly higher. The average tibial plateau slope was 6.094° for males and 6.428° for females, suggesting that males may be more susceptible to the influence of the lateral tibial plateau slope.Increased LTPS may lead to increased anterior translation of the tibia, thereby increasing the tension on the ACL and making it more prone to injury.
The study confirmed the NWI as a significant risk factor for ACL injuries in both genders. Research by Prior et al. indicates that a smaller α angle and NWI are linked to increased ACL injury risks [7, 19, 20]. A narrower intercondylar notch, reflected by a smaller α angle, may cause ACL impingement, elevating injury chances [21]. Nonetheless, using visual inspection to classify the intercondylar notch shape could introduce inaccuracies. In Volkan Kızılgöz et al.‘s study on the impact of the intercondylar notch index on ACL injuries, both males and females were categorized, and statistically significant findings were observed. The cutoff value for males was 0.26, while for females, it was 0.27 [22]. Our study results indicate a significant association between NWI and ACL injuries, with OR of 0.767 for males and 0.807 for females. Additionally, the cutoff values were 0.283 for males and 0.268 for females. These findings suggest that the influence of NWI is more pronounced in males, as indicated by both the OR and cutoff values.
Another finding of this study is the association between the LFCI, which reflects the sphericity of the lateral femoral condyle [23], and ACL injuries. An increased LFCI indicates a deeper posterior condyle, associated with knee rotational instability, thus leading to ACL injuries [24]. The predictive value of the lateral femoral condyle morphology for ACL injuries remains a subject of debate. Hodel et al., in 2019, identified the morphology of the lateral condyle as one of the risk factors for ACL injuries [16]. However, Emma K et al.‘s study in 2022, analyzing both genders together and separately, did not find LFCI to be an independent predictor of ACL injury risk [8]. Neunghan Jeon et al.‘s 2022 study reiterated the increase in LFCI as a risk factor for ACL injury in females [9], but the measurements were based on knee X-rays rather than MRI, significantly influenced by the patient’s positioning. Our study identified LFCI as a common risk factor for ACL injuries, with cutoff values of 0.567 and 0.551 for males and females, respectively. The OR for females was 1.244, whereas for males, it was 1.147, indicating that the impact of LFCI on ACL injuries is more pronounced in females.
This study is the first to identify the patellar tendon angle at near knee extension (< 20°) as a predictor for ACL injuries. The ROC curve area was 0.685 for females and 0.622 for males. Additionally, the cutoff value for the patellar tendon angle was 33.095 for females and 34.840 for males. Moreover, the OR value for females was lower than for males (0.894 vs. 0.944), suggesting that changes in the patellar tendon angle have a greater protective effect against ACL injuries in females. The impact of the patellar tendon angle on ACL injuries might be due to the maximum shearing force exerted on the ACL when the knee is near extension [11], which decreases as the knee flexes further, reducing the anterior translation of the tibia caused by quadriceps contraction. Furthermore, the study identified the Insall-Salvati index as a risk factor for ACL injuries in females. Females have higher incidence of patella alta and patellar instability than males, which could highlight the significance of the patellar index in females ACL injuries [25]. This study also found that the average value of the Insall-Salvati index in females was significantly higher than in males. A. J. Degnan et al.’ study on the association between ACL injuries and patella alta in children aged 8–18 showed that ACL tears are associated with increased Insall-Salvati values [26]. Compared to those with normal patellar positioning, individuals with patella alta require greater knee flexion for patellar contact with the trochlea, creating contact stress between the femoral condyles and the patella. In certain situations, such as knee torsion, eversion, inversion, flexion, and extension, to prevent additional contact stress between the femoral condyles and the patella, a relative brief translation between the femur and tibia will increase. This translational change may subject the ACL to greater stress, thus increasing the risk of tears [27].
Clinical relevance
This study conducted a comprehensive analysis separately for males and females, identifying various anatomical risk factors related to ACL injuries with certain gender differences and distinct cutoff values. Notably, this study is the first to find that the patellar tendon angle is related to ACL injuries in both male and female patients. Furthermore, the Insall-Salvati index has been identified as a risk factor for ACL injuries in females. These findings can contribute to targeted screening and preventative strategies for athletes, as well as aid in preventing reinjury after ACL reconstruction.
Limitations
The study’s limitations include its single-institution subject pool, potentially limiting broader applicability. Despite using age and gender-matched controls, other variables like body metrics and activity levels were not controlled. The retrospective nature also introduces potential bias. Selection bias might be present due to the lack of clear explanation of patient inclusion and exclusion criteria, as well as the use of MRI in the control group. However, the study aimed to include consecutive patients meeting the criteria, and the use of MRI in the control group was necessary to ensure accurate measurements of anatomical factors. The matching process was based on age and gender, which are two critical factors influencing ACL injury risk, but a propensity score matching analysis was not performed due to the limited sample size. While suggesting clinical relevance for the patellar tendon angle in near-extension, a dynamic analysis might offer deeper insights. Additionally, the sample size was relatively limited, and a power analysis was not performed during the study design phase, which may affect the interpretation of the results. Despite these limitations, the study provides valuable insights into the gender-specific anatomical risk factors for ACL injuries, and the findings can serve as a foundation for future research and clinical applications.
Conclusion
This study identifies the lateral tibial plateau slope, notch width index, lateral femoral condyle index, and patellar tendon angle at near-extension as risk factors for ACL injuries in both genders, with the Insall-Salvati index also implicated in females. These findings emphasize the complex role of common anatomical features in gender-specific ACL injury risk.
Data availability
The data were available from corresponding author upon reasonable request.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- TPS:
-
Tibial plateau slope
- LTPS:
-
Lateral tibial plateau slope
- MTPS:
-
Medial tibial plateau slope
- MRI:
-
Magnetic Resonance Imaging
- LCFCR:
-
Lateral condylar flexion circle radius
- LCECR:
-
Lateral condylar extension circle radius
- LFCI:
-
Lateral femoral condyle index
- NWI:
-
Notch width index
- ROC:
-
Receiver operating characteristic
References
Montalvo AM, Schneider DK, Yut L et al. What’s my risk of sustaining an ACL injury while playing sports? A systematic review with meta-analysis[J]. Br J Sports Med 2019 53(16). 1003–1210.1136/bjsports-2016-096274.
Bram JT, Magee LC, Mehta NN, et al. Anterior Cruciate Ligament Injury incidence in adolescent athletes: a systematic review and Meta-analysis[J]. Am J Sports Med. 2021;49(7):1962–72. https://doi.org/10.1177/0363546520959619.
Chia L, De Oliveira Silva D, Whalan M et al. Non-contact anterior cruciate ligament Injury Epidemiology in Team-Ball sports: a systematic review with Meta-analysis by sex, Age, Sport, participation level, and exposure Type[J].Sports Med.2022. 52(10). 2447–6710.1007/s40279-022-01697-w.
Gornitzky AL, Lott A, Yellin JL et al. Sport-specific yearly risk and incidence of anterior cruciate ligament tears in High School athletes: a systematic review and Meta-analysis[J]. Am J Sports Med 2016 44(10). 2716–23.https://doi.org/10.1177/0363546515617742.
Monk AP, Davies LJ, Hopewell S et al. Surgical versus conservative interventions for treating anterior cruciate ligament injuries[J]. Cochrane Database Syst Rev 2016 4(4). Cd011166.https://doi.org/10.1002/14651858.CD011166.pub2.
Blanke F, Kiapour AM, Haenle M et al. Risk of Noncontact Anterior Cruciate Ligament injuries is not Associated with Slope and Concavity of the Tibial Plateau in recreational Alpine skiers: a magnetic resonance imaging-based case-control study of 121 Patients[J]. Am J Sports Med 2016 44(6). 1508–14.https://doi.org/10.1177/0363546516632332.
Shen L, Jin ZG, Dong QR et al. Anatomical risk factors of Anterior Cruciate Ligament Injury[J].Chin Med J (Engl).2018. 131(24). 2960–7.https://doi.org/10.4103/0366-6999.247207.
Nowak EK, Beaulieu ML, Beynnon BD et al. The lateral femoral Condyle Index is not a risk factor for primary noncontact Anterior Cruciate Ligament Injury[J]. Am J Sports Med 2022 50(1). 85–9210.1177/03635465211057271.
Jeon N, Choi NH, Hwangbo BH et al. An increased lateral femoral condyle ratio in addition to increased posterior tibial slope and narrower Notch Index is a risk factor for female Anterior Cruciate Ligament Injury[J].Arthroscopy.2022. 38(5). 1597–60410.1016/j.arthro.2021.10.022.
Englander ZA, Lau BC, Wittstein JR et al. Patellar tendon orientation and strain are predictors of ACL strain in vivo during a single-Leg Jump[J]. Orthop J Sports Med 2021 9(3). 2325967121991054.https://doi.org/10.1177/2325967121991054.
Englander ZA, Cutcliffe HC, Utturkar GM et al. In vivo assessment of the interaction of patellar tendon tibial shaft angle and anterior cruciate ligament elongation during flexion[J].J Biomech.2019. 90. 123–710.1016/j.jbiomech.2019.04.034.
Beynnon BD, Hall JS, Sturnick DR et al. Increased slope of the lateral tibial plateau subchondral bone is associated with greater risk of noncontact ACL injury in females but not in males: a prospective cohort study with a nested, matched case-control analysis[J]. Am J Sports Med 2014 42(5). 1039–48.https://doi.org/10.1177/0363546514523721.
Alentorn-Geli E, Myer GD, Silvers HJ et al. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: mechanisms of injury and underlying risk factors[J]. Knee Surg Sports Traumatol Arthrosc 2009 17(7). 705–29.https://doi.org/10.1007/s00167-009-0813-1.
Yu B. and W E Garrett mechanisms of non-contact ACL injuries[J].Br J sports Med.2007. 41 suppl 1(suppl 1). i47-51.https://doi.org/10.1136/bjsm.2007.037192.
Lipps DB, Wilson AM, Ashton-Miller JA, et al. Evaluation of different methods for measuring lateral tibial slope using magnetic resonance imaging[J]. Am J Sports Med. 2012;40(12):2731–6. https://doi.org/10.1177/0363546512461749.
Hodel S, Kabelitz M, Tondelli T et al. Introducing the lateral femoral Condyle Index as a risk factor for Anterior Cruciate Ligament Injury[J]. Am J Sports Med 2019 47(10). 2420–6.https://doi.org/10.1177/0363546519858612.
Dare DM, Fabricant PD, McCarthy MM, et al. Increased lateral tibial slope is a risk factor for Pediatric Anterior Cruciate Ligament Injury: an MRI-Based case-control study of 152 Patients[J]. Am J Sports Med. 2015;43(7):1632–9. https://doi.org/10.1177/0363546515579182.
Hashemi J, Chandrashekar N, Mansouri H et al. Shallow medial tibial plateau and steep medial and lateral tibial slopes: new risk factors for anterior cruciate ligament injuries[J]. Am J Sports Med 2010 38(1). 54–62.https://doi.org/10.1177/0363546509349055.
Fernández-Jaén T, López-Alcorocho JM, Rodriguez-Iñigo E, et al. The importance of the Intercondylar Notch in Anterior Cruciate Ligament Tears[J]. Orthop J Sports Med. 2015;3(8):2325967115597882. https://doi.org/10.1177/2325967115597882.
Misir A, Uzun E, Sayer G et al. Anatomic factors Associated with the development of an anterior cruciate ligament rerupture in men: a case-control Study[J]. Am J Sports Med 2022 50(12). 3228–35.https://doi.org/10.1177/03635465221120378.
Park HS, Ahn C, Fung DT et al. A knee-specific finite element analysis of the human anterior cruciate ligament impingement against the femoral intercondylar notch[J]. J Biomech 2010 43(10). 2039–42.https://doi.org/10.1016/j.jbiomech.2010.03.015.
Kızılgöz V, Sivrioğlu AK, Ulusoy GR et al. Analysis of the risk factors for anterior cruciate ligament injury: an investigation of structural tendencies[J]. Clin Imaging 2018 50. 20–3010.1016/j.clinimag.2017.12.004.
Micicoi G, Jacquet C, Khakha R, et al. Femoral and tibial bony risk factors for anterior cruciate ligament injuries are Present in more than 50% of healthy Individuals[J]. Am J Sports Med. 2021;49(14):3816–24. https://doi.org/10.1177/03635465211050421.
Pfeiffer TR, Burnham JM, Hughes JD et al. An increased lateral femoral condyle ratio is a risk factor for Anterior Cruciate Ligament Injury[J].J Bone Joint Surg Am.2018. 100(10). 857–64.https://doi.org/10.2106/jbjs.17.01011.
Balcarek P, Jung K, Ammon J et al. Anatomy of lateral patellar instability: trochlear dysplasia and tibial tubercle-trochlear groove distance is more pronounced in women who dislocate the patella[J]. Am J Sports Med 2010 38(11). 2320–7.https://doi.org/10.1177/0363546510373887.
Degnan AJ, Maldjian C, Adam RJ et al. Comparison of Insall-Salvati ratios in children with an acute anterior cruciate ligament tear and a matched control population[J]. AJR Am J Roentgenol 2015 204(1). 161–6.https://doi.org/10.2214/ajr.13.12435.
Akgün AS. and M Agirman associations between Anterior Cruciate Ligament Injuries and Patella Alta and Trochlear Dysplasia in adults using magnetic resonance Imaging[J].J Knee Surg.2021. 34(11). 1220–610.1055/s-0040-1702198.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
XJ: first author, collected the data, wrote the first draft of the manuscript, and revised it. XW:co-first authors,analyzed and interpreted the data. YM: corresponding author, agreed to be accountable for allaspects of the work, thereby ensuring that questions related to the accuracyor integrity of any part of the work are appropriately investigated and alsoresolved the final approval of the version to be published. WX revised the article critically for important intellectualcontent. CS collected the relevant information of patients. LL analyzed andinterpreted the data.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by our Institutional Ethics Committee and the study complies with all ethical guidelines.This study received ethical approval from the Ethics Committee of the Second Affiliated Hospital of Soochow University, under the ethical review number JD-HG-2023-41. In accordance with the ethical review process conducted by the Institutional Ethics Committee, it has been determined that the requirement for informed consent from participants is waived. This waiver of informed consent is justified based on the retrospective and anonymous nature of the study design, which involves the analysis of pre-existing data without directly involving or identifying individual participants.The decision to waive informed consent was made by the Institutional Ethics Committee to facilitate the conduct of the study while upholding ethical principles and protecting the rights and confidentiality of the participants. The waiver of informed consent was granted to streamline the research process and mitigate any potential risks to participants, considering that their identities are not disclosed, and their participation is not required for the study.The Institutional Ethics Committee of the Second Affiliated Hospital of Soochow University, being the overseeing body responsible for ensuring the ethical conduct of research, has thus provided explicit approval for the waiver of informed consent in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Jin, X., Wu, X., Xu, W. et al. Gender differences in the impact of anatomical factors on non-contact anterior cruciate ligament injuries: a magnetic resonance study. BMC Musculoskelet Disord 25, 264 (2024). https://doi.org/10.1186/s12891-024-07390-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-024-07390-5