
Abstract
Background
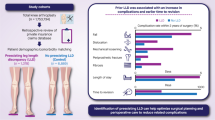
Leg length discrepancy (LLD) is one of the troublesome complications of total hip arthroplasty (THA). Previously, several risk factors have been suggested, but they were subjected to their inherent limitations. By controlling confounding variables, we hypothesized that known risk factors be re-evaluated and novel ones be discovered. This study aimed to analyze the independent risk factors for LLD after primary THA in patients with non-traumatic osteonecrosis of the femoral head (ONFH).
Methods
We retrospectively reviewed patients with non-traumatic ONFH who underwent unilateral THA between 2014 and 2021. All patients were operated by one senior surgeon using a single implant. Demographic data, surgical parameters, and radiological findings (pre-operative LLD, Dorr classification, and femoral neck resection) were analyzed to identify the risk factors of ≥ 5 mm post-operative LLD based on radiological measurement and to calculate odds ratios by logistic regression analysis. Post hoc power analysis demonstrated that the number of analyzed patients was sufficient with 80% power.
Results
One hundred and eighty-six patients were analyzed, including 96 females, with a mean age of 58.8 years at the time of initial THA. The average post-operative LLD was 1.2 ± 2.9 mm in the control group and 9.7 ± 3.2 mm in the LLD group, respectively. The LLD group tended to have minimal pre-operative LLD than the control group (-3.2 ± 5.1 mm vs. -7.9 ± 5.8 mm p = 2.38 × 10− 8). No significant difference was found between the groups in age, gender, body mass index, femoral cortical index, and implant size.
Conclusion
Mild pre-operative LLD is associated with an increased risk of post-operative LLD after primary THA in patients with ONFH. Thus, surgeons should recognize pre-operative LLD to achieve an optimal outcome and must inform patients about the risk of developing LLD.
Similar content being viewed by others


Introduction
As the longevity of total hip arthroplasty (THA) implants has been continuously increasing, [1] so has the number of patients who underwent THA [2]. Leg length discrepancy (LLD) after THA has been not uncommonly reported. Perceived post-operative LLD-impaired patients’ function [3], limping [4], and patient dissatisfaction [5], leading to legal issues [6, 7].
To prevent this complication, several previous studies have elucidated the possible risk factors for post-operative LLD. Brumat et al. and Lim et al. suggested that the shape of the proximal femur and post-operative LLD were related [8, 9]. In revision THA, Kennedy et al. revealed that body mass index (BMI) was positively related to the risk of developing post-operative LLD [10]. Furthermore, Kishimoto et al. interestingly suggested that surgeon volume was associated with the risk of post-operative LLD [11]. However, these studies were limited to numerous pre-operative diagnoses, various types of cemented and cementless femoral stems, and several surgeons participating in the studies. Thus, it is hard to know how much these factors affect the outcome of surgery.
Osteonecrosis of the femoral head (ONFH) is a prevalent indication of THA [12]. Patients diagnosed with ONFH typically presented with a younger age and relatively mild deformity of the proximal femur, making this cohort more sensitive to LLD. Consequently, a thorough understanding of postoperative LLD and its associated risk factors in ONFH patients undergoing THA is essential for optimizing surgical outcomes and enhancing the overall quality of patient care.
We hypothesized that by controlling the confounding variables, previously reported possible risk factors might be re-evaluated and novel risk factors could be discovered. The aim of this study was to evaluate the risk factors of post-operative LLD (1) by controlling pre-operative diagnosis for THA, (2) by using the same THA implant, and (3) by performing the surgery with a single senior surgeon.
Methods
Study design
This was a retrospective observational study that followed STROBE guideline [13]. Upon Institutional Review Board approval, we conducted a study on a cohort of patients with uni-lateral non-traumatic osteonecrosis of the femoral head who had primary THA with a single stem design. We included patients who received primary THA with the studied implant in a tertiary referral hospital from July 2014 to Oct 2020. Patients were excluded if they had a history of previous hip replacement on the contralateral hip, had the contralateral hip replacement within 6 months, and had severe osteoarthritis on the contralateral hip joint, severe deformity of the proximal femur, or a pre-operative leg length discrepancy of more than 3 cm (Fig. 1). Among the analyzed patients, the patients whose post-operative LLD were equal to or more than 5 mm were grouped as an LLD group [8, 14, 15], while the others were classified as a control group.

Flow-chart of enrolled patients
Operation
All operations were performed by a high- volume hip arthroplasty surgeon (JJY) with more than 20 years of experience using the modified direct lateral approach [16]. One type of cementless THA implant and bearing was used: Bencox Mirabo acetabular cup with Bencox M stem (Corentec, Cheonan, Korea) and alumina-zirconia composite Biolox Delta (CeramTec, Plochingen, Germany) (Fig. 2). The stem is a type I stem that is widely used [17] and features a single wedged, proximally coated, and mid-short length [18].

Bencox Mirabo cup with M femoral stem (Corentec, Cheonan, Korea) and Biolox Delta bearing (Ceramtec, Plochingen, Germany) were used in this study
Preoperative acetate onlay templating was performed in all patients. Templating was used to guide the femoral neck resection level, choice of implant size, and implant position. However, the final decision was based on the intraoperative features of the patients. To make more accurate decisions, intraoperative anteroposterior pelvic radiographs were also routinely taken via cross-table manner right after the insertion of implant trials.
Patients were instructed to walk using crutches with tolerable weight-bearing for post-operative 6 weeks.
Clinical variables
The following data were obtained: age at index surgery, gender, pre-operative diagnosis, BMI, and pre-operative radiological leg length discrepancy.
Radiologic evaluation and analysis
Hip anteroposterior view was taken while standing with 15° internally rotated legs when the beam was incident on the median line 2.5cm above the pubic symphysis [19].
To validate the accuracy of the PACS (INFINITT PACS Viewer, Seoul, South Korea) measuring method, we first draw a circle that perfectly fits the acetabular cup and measured the diameter. Then, the measurements were compared with the actual implant, yielding the ratio between the actual value and the PACS viewer measured value.
Two independent authors (HSK, HJL) who did not participate in the index surgery performed all measurements. The authors repeated the measurement 6 weeks later, and the mean difference was 0.6 ± 0.3 mm with intra-observer reliability of 0.945. Inter-observer reliability using the intra-class correlation coefficient was 0.843. The definition of ICC values was as follows: excellent reliability (> 0.90), good reliability (0.75–0.90), moderate reliability (0.50–0.75), and poor reliability (< 0.50) [20].
Femoral cortical index
On an anteroposterior radiograph of the hip, the femoral cortical index (FCI) was defined as the ratio of cortical width minus canal width to the cortical width at a level of 100 mm below the apex of the lesser trochanter, as described in previous studies [21]. These measurements were repeated 6 weeks later to assess the intra-observer reliability. The mean difference in FCI was 0.04 ± 0.02 and the intra-observer reliability was 0.875. All patients were categorized on the basis of FCI with the cutoff values as follows: >0.6 as Dorr type A, between 0.6 and 0.5 as Dorr type B, and < 0.5 as Dorr type C [9].
Leg length discrepancy
The leg length discrepancy was defined as the perpendicular distance between the lesser trochanters and a horizontal reference line connecting the inferior aspect of the acetabular teardrops on an anteroposterior radiograph of the pelvis at least 6 months after THA [22] (Supplementary Fig. 1). The measurements were repeated 6 weeks later to assess the intra-observer reliability in the corresponding technique. The mean difference in LLD was 0.5 ± 0.4 mm and the intra-observer reliability was 0.902.
Femoral neck resection and cup center level
The femoral neck resection level was measured as the vertical distance from the tip of the lesser trochanter to the bone resection cut on the medial side of the femoral neck. The level of the cup center relative to the greater trochanter was defined as the vertical distance from the tip of the greater trochanter to the cup center.
Statistical analyses
SPSS statistics for Windows (Version 25.0; IBM, Armonk, NY) was used for the statistical analyses. All continuous variables are reported as mean and standard deviation, and categorical variables are reported as numbers and percentages. A Student t-test or Mann-Whitney U test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables were performed. Multiple logistic regression analysis was performed to identify the independent risk factors of post-operative LLD. Significance was defined as a p-value of less than 0.05.
Results
In total, 186 patients were analyzed in this study. Pre-operative and post-operative 6-month radiographs of all patients were examined. An absolute LLD ≥ 5 mm after THA was observed in 45.2% of the patients (84 of 186 hips). The mean post-operative LLD was 5.1 ± 5.2 mm, and the mean FCI was 0.54 ± 0.06. There was no significant difference between the two groups with regard to age, gender, BMI, operated site, and the cause of non-traumatic osteonecrosis of the femoral head (Table 1). A post-hoc analysis was conducted and confirmed that the number of analyzed patients was larger than the minimum sample size with 80% power and an alpha of 0.05.
Minimal LLD before surgery was more likely to be associated with LLD ≥ 5 mm after surgery. The pre-operative LLD of the LLD group was − 3.2 ± 5.1 mm, whereas that of the control group was − 7.9 ± 5.8 mm (p < 0.001) (Fig. 3).

(A) Preoperative hip radiograph with substantial leg length discrepancy (B) Hip radiograph at postoperative 6 weeks with minimal leg length discrepancy (C) Simple hip radiograph with minimal preoperative leg length discrepancy (D) Postoperative 6 weeks radiograph with leg length discrepancy more than 5 mm
The shape of the proximal femur, which was represented by FCI, was not associated with the post-operative LLD (p = 0.292). In terms of implant size choice, no significant difference was found between the two cohorts in acetabular cup size (p = 0.052), femoral stem size (p = 0.087), head size (p = 0.143), and dependent neck length (p = 0.906). In addition, the amount of femoral neck resection and cup center level with respect to the greater trochanter showed little difference between the groups (p = 0.734 and p = 0.164, respectively) (Table 1).
Among eighty-eight patients with minimal LLD (less than 5 mm) preoperatively, the ratio of patients with LLD ≥ 5 mm after surgery was 61.4% (54 of 88). It was higher than that within the patients with preoperative substantial LLD, which was 30.6% (30 of 98) (p < 0.001).
Possible risk factors from the univariate analysis were included in the multiple logistic regression analysis. The analysis showed that pre-operative LLD (p-value < 0.01) was the only independent risk factor associated with post-operative LLD.
The average follow-up period was similar in both groups (2.5 ± 1.9 versus 2.5 ± 1.8 years; p = 0.873).
Discussion
The present findings of this study indicated that the patient with preoperatively balanced leg length showed more imbalance after the surgery and the patient who suffered from substantial difference in limb length resulted in little difference in limb length (Fig. 3). Among other complications, LLD after THA was considered the most troublesome complication, which was directly related to patient satisfaction after surgery and was hard to resolve. Since the successful THA should have complication-free long-term survival and acceptable patient satisfaction, the surgeon should take account of pre-operative LLD.
The presented findings on the association between pre-operative and post-operative LLD have direct clinical applications for THA surgery. Minimal pre-operative LLD led to more post-operative LLD and should be considered as a risk factor for post-operative LLD in cementless type I stems. No significant difference was found between the groups in age, gender, body mass index, femoral cortical index, and implant size. Additional intraoperative procedures such as the usage of high offset stem, additional medullary preparation, or intraoperative radiograph would be needed.
Previously, a broad consensus was accepted that ≤ 10 mm of LLD on radiographs was clinically irrelevant [23, 24]. To date, the definitions of LLD varied based on radiological measurements: 5 mm [8, 14, 15, 25], 6 mm [26], 7 mm [27], 10 mm [28, 29], and 20 mm [30]. Sykes et al. [25] demonstrated that a large number of patients with discrepancies ≥ 5 mm had perceived the difference, and Renkawitz et al. [15] showed that gait kinematics might be induced due to discrepancies ≥ 5 mm. Fujita et al. showed that 7 mm may be a reasonable threshold for reducing residual discomfort [27]. In our study,a cut-off value of 5 mm was used to define LLD after surgery, and the proportion of post-operative LLD was high in patients with minimal pre-operative LLD. To the best of our knowledge, our study is the first to suggest the importance of pre-operative LLD.
Previous studies have suggested possible risk factors for post-operative LLD. In 2019, Mavčič et al. analyzed the effects of gender, age, operated side, surgical approach, body height, and BMI. The authors concluded that patients with smaller body dimensions (i.e. low BMI and small height) will be more likely to report subjective leg length inequality at a given objective LLD, regardless of gender or age [31]. Kishimoto et al. reported that surgeon volume might be an independent risk factor for leg length discrepancy. 79.6% of patients performed by high-volume surgeons had LLD of < 5 mm, while 40.0% of patients performed by low-volume surgeons achieved LLD of < 5 mm (p < 0.001). [11] However, previous studies included various stem designs, several surgeons performing the surgeries, and diverse pre-operative diagnoses. In this study, we designed the study to control these parameters: BMI, height, gender, and age did not influence leg length inequality after surgery. In addition, all index surgeries were performed by high-volume hip surgeons in our study.
Then, intra-operative factors, such as soft tissue laxity or hip flexion contracture, should be investigated. Contracture and adhesion around the hip joint due to the shortened limb could impede appropriate leg lengthening even with extensive soft tissue release. The previous literature has reported that patients with developmental dysplasia of the hip frequently present with moderate flexion contracture of the hip joint, necessitating additional soft tissue release during total hip arthroplasty [32, 33]. In our study, the amount of lengthening in patients with a significant preoperative LLD was shorter than that in the cohort with minimal preoperative LLD. While patients with ONFH tended to exhibit fewer developmental deformities, shortened limb may still lead to soft tissue contracture over time. In contrast, patients with minimal LLD may experience less joint contracture, which prompt surgeons to select larger implants or longer neck components for improved stability. Further studies analyzing the discrepancy between the pre-operative templating and the actual implant used should consider these concerns.
Among other risk factors, the morphology of the proximal femur has been considered important and discussed several times. Brumat et al. [8] concluded that a higher femoral canal flare index increased LLD after surgery when single-wedge femoral stems with cementless metaphyseal fixation were used. With cementless diaphyseal fixation or cemented fixation, however, the canal flare index had no impact on LLD in femoral stems. Lim et al. [9] have also shown that the proximal femoral canal morphology affected LLD. This study utilized more than three different stems, and the index surgeries were performed by three surgeons. In a recent systematic review by Mavčič et al. [34], the authors showed that Dorr type A (FCI > 0.6) increases the risk of leg length inequality after THA, especially when metaphyseal fixation stems were used. In the current study, where the same femoral stem was used and only one surgeon performed the operation, the Dorr type was not associated with post-operative LLD. This is comparable to the recent study of Kishimoto et al. [11] in which the Dorr type showed no association with post-operative LLD. We assumed that the differences in the study methods, surgical approach, and intraoperative medullary preparation might have affected the results.
Subjectively perceived LLD is important but was not analyzed in this study. Some patients would have complained with LLD less than 5 mm, while others would persevere the LLD more than 10 mm without any discomfort. Mavcic et al. [31] previously reported that patients with smaller body dimensions would more likely report subjective leg length inequality even within a given inequality. As so, our definition of LLD (≥ 5 mm) did not always match the patient’s dissatisfaction. However, generally perceived LLD was highly related to and based on objective LLD, which was studied here.
Preoperative templating and intraoperative radiographs would aid in decreasing the leg length discrepancy. We routinely performed preoperative conventional templating with digital PACS. Although the predetermined size of the stem may provide guidance in selecting the actual stem, the decision should be made comprehensively based on the clues in the intraoperative field. In 2018, Strøm and Reikerås reported that templating may be helpful but cannot be regarded as a blueprint for the operative choice [35]. Intraoperative fluoroscopy was also utilized, but care should be taken since the radiograph might be distorted depending on the patient’s posture, leg position, and magnification. Ezzet and McCauley analyzed the use of an intraoperative AP pelvic X-ray after trial component implantation, and found that the operative plan was altered in 50% of the surgeries, with changes being made to either the femoral alignment, leg length, cup medialization, or cup abduction [36]. Even with various perioperative measurements, absolute leg length equality is hard to achieve.
Limitations of this study were present. Firstly, only one disease entity was studied. The results might be different in THA for patients with trauma, infection sequelae, or dysplastic hip. A study with a larger cohort was warranted. Second, the studied stem might not be used in cases where the femoral cortical index is either very high or low. This would lead to selection bias. However, the range of FCI was from 0.35 to 0.67, and a substantial proportion of patients with high and low FCI was included. Lastly, the measurement was performed in plain radiographs. A slight change in patient position or the angle of beam insertion might influence the measured values. CT exam would provide an accurate assessment of limb length, but the cost and radiation hazards were concerns.
Conclusion
This is the first study to show that minimal pre-operative LLD is associated with LLD after THA. The surgeon should implement additional intraoperative procedures such as the usage of a high offset stem, additional medullary preparation, or intraoperative radiograph to avoid post-operative LLD. The Dorr type did not affect post-operative LLD.
Data Availability
The dataset supporting the conclusions of this article is included within the article.
References
Kim SC, Lim YW, Jo WL, Park SB, Kim YS, Kwon SY. Long-term results of total hip arthroplasty in young patients with osteonecrosis after allogeneic bone marrow transplantation for hematological Disease: a Multicenter, Propensity-Matched Cohort Study with a Mean 11-Year Follow-Up. J Arthroplasty. 2021;36(3):1049–54.
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–5.
Roder C, Vogel R, Burri L, Dietrich D, Staub LP. Total hip arthroplasty: leg length inequality impairs functional outcomes and patient satisfaction. BMC Musculoskelet Disord. 2012;13:95.
Wylde V, Whitehouse SL, Taylor AH, Pattison GT, Bannister GC, Blom AW. Prevalence and functional impact of patient-perceived leg length discrepancy after hip replacement. Int Orthop. 2009;33(4):905–9.
Plaass C, Clauss M, Ochsner PE, Ilchmann T. Influence of leg length discrepancy on clinical results after total hip arthroplasty–a prospective clinical trial. Hip Int. 2011;21(4):441–9.
Samuel LT, Sultan AA, Rabin JM, Surace PA, Yao B, Moskal JT, Mont MA. Medical Malpractice Litigation Following Primary Total Joint Arthroplasty: a Comprehensive, Nationwide Analysis of the past Decade. J Arthroplasty. 2019;34(7S):102–S107.
Novi M, Vanni C, Parchi PD, Di Paolo M, Piolanti N, Scaglione M. Claims in total hip arthroplasty: analysis of the instigating factors, costs and possible solution. Musculoskelet Surg. 2020;104(1):43–8.
Brumat P, Pompe B, Antolic V, Mavcic B. The impact of canal flare index on leg length discrepancy after total hip arthroplasty. Arch Orthop Trauma Surg. 2018;138(1):123–9.
Lim YW, Huddleston JI 3rd, Goodman SB, Maloney WJ, Amanatullah DF. Proximal femoral shape changes the risk of a Leg length discrepancy after primary total hip arthroplasty. J Arthroplasty. 2018;33(12):3699–703.
Kennedy JW, Young D, Meek DRM, Patil SR. Obesity is associated with higher complication rates in revision total hip arthroplasty. J Orthop. 2018;15(1):70–2.
Kishimoto Y, Suda H, Kishi T, Takahashi T. A low-volume surgeon is an Independent risk factor for leg length discrepancy after primary total hip arthroplasty: a case-control study. Int Orthop. 2020;44(3):445–51.
Kim HS, Park JW, Lee SJ, Lee YK, Ha YC, Koo KH. High risk of Neck-liner impingement and notching observed with thick femoral Neck implants in ceramic-on-ceramic THA. Clin Orthop Relat Res. 2022;480(4):690–9.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, Initiative S. Strengthening the reporting of Observational studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–8.
Nossa JM, Munoz JM, Riveros EA, Rueda G, Marquez D, Perez J. Leg length discrepancy after total hip arthroplasty: comparison of 3 intraoperative measurement methods. Hip Int. 2018;28(3):254–8.
Renkawitz T, Weber T, Dullien S, Woerner M, Dendorfer S, Grifka J, Weber M. Leg length and offset differences above 5mm after total hip arthroplasty are associated with altered gait kinematics. Gait Posture. 2016;49:196–201.
Mulliken BD, Rorabeck CH, Bourne RB, Nayak N. A modified direct lateral approach in total hip arthroplasty: a comprehensive review. J Arthroplasty. 1998;13(7):737–47.
Katakam A, Hosseinzadeh S, Humphrey TJ, Collins A, Shin D, Melnic CM, Bragdon C, Bedair HS. Different designs of proximal femoral stems for total hip Arthroplasty: Mid-term Clinical and patient-reported functional outcomes. Cureus. 2021;13(11):e19745.
Yang H, Kim K, Kim HS, Yoo JJ. Total hip arthroplasty performed with a Novel Design Type 1 femoral stem: a retrospective minimum 5-Year follow-up study. Clin Orthop Surg. 2022;14(1):28–34.
Lim SJ, Park YS. Plain radiography of the hip: a review of Radiographic techniques and Image features. Hip Pelvis. 2015;27(3):125–34.
Koo TK, Li MY. A Guideline of selecting and reporting Intraclass correlation coefficients for Reliability Research. J Chiropr Med. 2016;15(2):155–63.
Dorr LD, Faugere MC, Mackel AM, Gruen TA, Bognar B, Malluche HH. Structural and cellular assessment of bone quality of proximal femur. Bone. 1993;14(3):231–42.
Ranawat CS, Rao RR, Rodriguez JA, Bhende HS. Correction of limb-length inequality during total hip arthroplasty. J Arthroplasty. 2001;16(6):715–20.
McWilliams AB, Grainger AJ, O’Connor PJ, Redmond AC, Stewart TD, Stone MH. A review of symptomatic leg length inequality following total hip arthroplasty. Hip Int. 2013;23(1):6–14.
Ng VY, Kean JR, Glassman AH. Limb-length discrepancy after hip arthroplasty. J Bone Joint Surg Am. 2013;95(15):1426–36.
Sykes A, Hill J, Orr J, Humphreys P, Rooney A, Morrow E, Beverland D. Patients’ perception of leg length discrepancy post total hip arthroplasty. Hip Int. 2015;25(5):452–6.
Ellapparadja P, Mahajan V, Atiya S, Sankar B, Deep K. Leg length discrepancy in computer navigated total hip arthroplasty - how accurate are we? Hip Int. 2016;26(5):438–43.
Fujita K, Kabata T, Kajino Y, Tsuchiya H. Optimizing leg length correction in total hip arthroplasty. Int Orthop. 2020;44(3):437–43.
Lecoanet P, Vargas M, Pallaro J, Thelen T, Ribes C, Fabre T. Leg length discrepancy after total hip arthroplasty: Can leg length be satisfactorily controlled via anterior approach without a traction table? Evaluation in 56 patients with EOS 3D. Orthopaedics & traumatology, surgery & research: OTSR 2018, 104(8):1143–1148.
Kim CY, Chung YY, Shim SW, Baek SN, Kim CH. Early experience of Direct Anterior Approach Total Hip Arthroplasty: analysis of the First 53 cases. Hip Pelvis. 2020;32(2):78–84.
Zhang Y, He W, Cheng T, Zhang X. Total hip arthroplasty: Leg length discrepancy affects functional outcomes and Patient’s Gait. Cell Biochem Biophys. 2015;72(1):215–9.
Mavcic B, Dolinar D, Pompe B, Antolic V. Patient-dependent risk factors for self-perceived leg length discrepancy after total hip arthroplasty. Eur J Orthop Surg Traumatol. 2019;29(4):793–9.
Yoon PW, Kim JI, Kim DO, Yu CH, Yoo JJ, Kim HJ, Yoon KS. Cementless total hip arthroplasty for patients with Crowe type III or IV developmental dysplasia of the hip: two-stage total hip arthroplasty following skeletal traction after soft tissue release for irreducible hips. Clin Orthop Surg. 2013;5(3):167–73.
Wu X, Li SH, Lou LM, Cai ZD. The techniques of soft tissue release and true socket reconstruction in total hip arthroplasty for patients with severe developmental dysplasia of the hip. Int Orthop. 2012;36(9):1795–801.
Mavcic B, Antolic V. Cementless femoral stem fixation and leg-length discrepancy after total hip arthroplasty in different proximal femoral morphological types. Int Orthop. 2021;45(4):891–6.
Strom NJ, Reikeras O. Templating in uncemented THA. On accuracy and postoperative leg length discrepancy. J Orthop. 2018;15(1):146–50.
Ezzet KA, McCauley JC. Use of intraoperative X-rays to optimize component position and leg length during total hip arthroplasty. J Arthroplasty. 2014;29(3):580–5.
Acknowledgements
None.
Funding
This study is funded by the Seoul National University Hospital Research Fund (Grant no. 06-2003-0630).
Author information
Authors and Affiliations
Contributions
Hong Seok Kim : writing - original draft, data curation, formal analysis, visualizationHan Jin Lee: methodology, investigationJeong Joon Yoo: conceptualization, supervision, writing - review & editing, supervisionAll authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present study was approved from Institutional Review Board of the Seoul National University Hospital (IRB number: H-2104-216-1215). Our study followed the guidelines of the 1975 Declaration of Helsinki, and the informed consent was waived by the Institutional Review Board of Seoul National University Hospital due to its retrospective nature.
Consent for publication
Not applicable.
Conflict of interest
Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kim, H.S., Lee, H.J. & Yoo, J.J. Minimal pre-operative leg length discrepancy as a risk factor of post-operative leg length discrepancy after total hip arthroplasty: a retrospective study of patients with non-traumatic osteonecrosis of the femoral head. BMC Musculoskelet Disord 24, 954 (2023). https://doi.org/10.1186/s12891-023-07086-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-07086-2