
Abstract
Background
The COVID-19 pandemic has triggered a global mental health crisis. Yet, we know little about the lasting effects of COVID-19 infection on mental health. This prospective longitudinal study aimed to investigate the trajectories of mental health changes in individuals infected with COVID-19 and to identify potential predictors that may influence these changes.
Methods
A web-survey that targeted individuals that had been infected with COVID-19 was used at three time-points: T0 (baseline), T1 (six months), and T2 (twelve months). The survey included demographics, questions related to COVID-19 status, previous psychiatric diagnosis, post-COVID impairments, fatigue, and standardized measures of depression, anxiety, insomnia. Linear mixed models were used to examine changes in depression, anxiety, and insomnia over time and identify factors that impacted trajectories of mental health outcomes.
Results
A total of 236 individuals completed assessments and was included in the longitudinal sample. The participants’ age ranged between 19 and 81 years old (M = 48.71, SD = 10.74). The results revealed notable changes in mental health outcomes over time. The trajectory of depression showed significant improvement over time while the trends in anxiety and insomnia did not exhibit significant changes over time. Younger participants and individuals who experienced severe COVID-19 infection in the acute phase were identified as high-risk groups with worst mental ill-health. The main predictors of the changes in the mental health outcomes were fatigue and post-COVID impairments.
Conclusions
The findings of our study suggest that mental health outcomes following COVID-19 infection exhibit a dynamic pattern over time. The study provides valuable insights into the mental health trajectory following COVID-19 infection, emphasizing the need for ongoing assessment, support, and interventions tailored to the evolving mental health needs of this population.
Similar content being viewed by others


Background
The SARS-CoV-2 infection (COVID-19) outbreak has led to mental health problems in the general population [1,2,3], most profoundly affected by demographical variables such as age, sex, and education as well as pre-exiting mental health problems [4, 5]. In addition, there have been notable changes in mental health problems since the onset of the pandemic, marked by a spike during the first wave of the COVID-19 pandemic and a subsequent decline from the initial baseline assessment to subsequent follow-ups [6,7,8,9]. However, levels of mental ill-health have been found to be more elevated in individuals infected with COVID-19 compared to the general population [10], suggesting that the mechanisms through which COVID-19 infection impacts mental health may differ from those observed in the general population.
Studies investigating mental ill-health following COVID-19 infection shed light on a bidirectional association between SARS-CoV-2 infection and mental ill-health [11,12,13,14,15]. However, the impact of COVID-19 infection on mental health becomes more intricate in the context of long-term complaints of COVID-19. Follow-up studies on COVID-19 survivors highlighted the associations between mental ill-health and post-COVID complications [10, 16]. Long term impacts after COVID-19-infection include multi-systemic problems, disabilities, and mental health problems, of which fatigue has emerged as the most reported symptom [17,18,19]. As many as almost half of all who have a history of probable or confirmed COVID 19-infection experience symptoms after recovery from infection [18], and about 40% of COVID-19 survivors experience fatigue three months after infection, with anxiety, depression and psychiatric comorbidity generating elevated risk [20]. We have previously shown in a cohort study that individuals with a history of probable or confirmed COVID-19 infection/infections are more likely to suffer from mental health problems, with post-COVID impairments and fatigue appearing as the main predictors of mental ill-health [10].
To summarize, available data highlights that COVID 19-patients are a high-risk group for mental ill-health, and points to an interplay between COVID-19-infection and mental ill-health and a possible bi-directional association. However, more knowledge is needed regarding the specific role of post-COVID impairments, especially fatigue, on mental health following COVID-19 infection. Hence, we aimed to investigate the trajectories of mental health changes over time in individuals infected with COVID-19; and to explore potential predictors that may influence these changes.
Methods
Participants
In this longitudinal study, we used data from a web-based longitudinal project to study the impacts of COVID-19 infection on a sample of Swedish population [10, 17]. To recruit participants, we used convenience sampling by spreading e-posters on platforms of COVID-19-related Facebook groups, Swedish COVID-organization (Svenska Covidföreningen), and the Karolinska Institutet website. Participants could access the web-survey through an online platform, Research Electronic Data Capture (REDCap), hosted locally at Karolinska institutet [21, 22]. Inclusion criteria were: (i) having been infected with COVID-19; (ii) age (≥ 18 years); (iii) ability to understand Swedish, and use the internet in order to complete the web-survey. The main exclusion criteria in the current study was absence of a prior COVID-19 infection, serving as a key parameter for participating.
The web-based survey was conducted at three time points: (i) at baseline or T0 (February/March 2022), (ii) first follow-up or T1 (September/October 2022), and (iii) second follow-up or T2 (February/March 2023). The number of participants in each cross-sectional data collection varied. A total of 501 participants responded at the baseline (T0), while the response rate was 60.1% at T1 and 57.3% at T2. The longitudinal analysis included 236 (47.1%) participants who completed the survey at all time points.
Ethical considerations
The study was approved by the Swedish national ethical board (Dnr 2021–06617-01). Informed consent was obtained from all participants. All procedures utilized in collecting data for the current paper followed the ethical standards of the Helsinki Declaration of 1964 and subsequent amendments [23].
Measures
Time-invariant covariates
Time-invariant covariates in the current study consisted of sociodemographic variables, COVID-19-related variables, and previous psychiatric diagnosis, which were obtained at T0 and assumed to remain unchanged across the study. Sociodemographic variables included age, gender, educational level, work status, and economic status. The ages were grouped by decades.
COVID-19-related variables included time of first infection, hospitalization for COVID-19, being vaccinated against COVID-19, and COVID-19 severity in the acute phase. Time of first infection was measured by a single item in which respondents stated date of first infection (year and month). The variable was dichotomized into during the year 2020 versus during the year 2021 and 2022, in line with our previous study that revealed that individuals who were infected for the first time during the first and second pandemic waves in Sweden (the spring and autumn of 2020) experienced more COVID-19 related problems [17]. Hospitalization for COVID-19 was measured using a single item in which respondents stated on a binary question if they had been hospitalized because of COVID-19 (yes/no). Being vaccinated against COVID-19 was measured with a single item in which respondents indicated if they have received vaccine against COVID-19 on a binary question (yes/no). COVID-19 severity in the acute phase was measured with a 15-item scale describing common symptoms of the COVID-19 infection, namely fever, fatigue, cough, loss of smell and taste, difficulty breathing or shortness of breath, headache/migraine, aches or pain in the body, diarrhoea, skin rash, runny or blocked nose, nausea/vomiting, arrhythmia/palpitations, sore throat, cognitive difficulties such as memory and attention, and mental health problems such as sleep problems, depression, and anxiety [24, 25]. Participants rated symptoms that they have had at the beginning of the infection and those the following 4 weeks on a 4-point scale (0 = no, 1 = mild, 2 = moderate, 3 = severe). The respondents’ answers to 15 symptoms of COVID-19 items were summed up to calculate a COVID-19 severity in the acute phase (range 0—45, α = 0.77).
Previous psychiatric diagnosis was assessed using a single item in which respondents stated on a binary question if they had received a psychiatric diagnosis before COVID-19 infection (yes/no).
Time-varying covariates
Fatigue and post-COVID impairments were treated as time-varying covariates and assumed to be subject to change across the study. Time-varying covariates were assessed at all three time points (T0, T1, and T2).
Fatigue
The Multidimensional Fatigue Inventory (MFI) is a self-report instrument aiming to measure fatigue. The MFI is a 20-item scale and consists of five subscales namely general fatigue, physical fatigue, reduced motivation, reduced activity, and mental fatigue. Each scale contains four items, each rated on 5-point scale, from 1 (Yes, that is true) to 5 (No, that is not true) [26], and total score is calculated by summing all items. Higher scores indicate higher fatigue levels [27], and total score > 60 has been reported as clinically significant fatigue in a previous study [28]. In this study, we used the Swedish version, which has shown adequate psychometric properties [29, 30].
Post-covid impairments
Post-covid impairments were measured using a scale consisting of 54 items rated on a 4-point Likert scale (0 = no, 1 = mild, 2 = moderate, 3 = severe), developed and used in our previous studies [10, 17]. Items were categorized into four sub-categories according to the International Classification of Functioning, Disability and Health [31] as impairments in mental functions, impairments in sensory functions and pain, impairments in body system functions, and impairments in activities and participation. The respondents’ answers to each sub-category of post-COVID impairments were summed up and divided by the number of items to obtain the mean for each sub-category.
Study outcomes
Mental health variables were considered as study outcomes and consisted of depression, anxiety, and insomnia. Depression was measured with the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 consists of nine items answered on a four-point Likert scale (0–3), with the total score ranging from 0 to 27 [32,33,34]. Anxiety was assessed with the General Anxiety Disorder-7 item scale (GAD-7), which contains seven items answered on a four-point Likert scale (0–3) and with a score range from 0 to 21 [35,36,37,38]. Insomnia was measured with the Insomnia Severity Index (ISI), that consists of seven items to assess the nature, severity, and impact of insomnia answered on a five-point Likert scale (0–4), the total score ranges from 0 to 28 [39, 40]. The recommended cutoff score of ≥ 10 on each scale was considered as clinically significant depression, anxiety, and insomnia in the current study [33, 36, 40].
Statistical analysis
Descriptive statistics for sociodemographic variables are provided in terms of percentages, means, and standard deviations for both the baseline and longitudinal samples. Moreover, descriptive statistics for fatigue, post-COVID impairments, and study outcomes are presented in the form of means and standard deviations. Additionally, we computed the intraclass correlation coefficient (ICC) to evaluate variations between the initial baseline and subsequent follow-up assessments for time-varying covariates and study outcomes. An ICC less than 0.4 was categorized as very low, 0.4 to 0.74 as low to acceptable, and 0.75 or higher as excellent [41].
To assess the potential impact of the covariates, we used mixed-effects models, which are well-suited statistical tools for longitudinal data analysis. Participants were included in the model only if data from all three measurements were available for a given mental health outcome. The alpha value of the two-tailed level of significance was set at 0.05.
We ran linear mixed models with random intercepts to examine differences in mental health outcomes (PHQ-9, GAD-7, and ISI scores) over time with adjustment for sociodemographic variables, COVID-19-related variables, and previous psychiatric diagnosis. Furthermore, we ran linear mixed models to identify factors that impacted the trajectories of depression, anxiety, and insomnia by including both time-invariant and time-varying covariates in the model. We considered AIC (Akaike Information Criterion) and BIC (Bayesian Information Criterion) as model fit in the current study. A lower AIC or BIC value indicates a better fit. Statistical analysis was performed using statsmodel library (version 0.13.5) in Python, and IBM Statistical Software Package of Social Science (SPSS; version 26).
Results
Descriptive statistics
Descriptive statistics for sociodemographic variables are presented for the baseline sample and the longitudinal sample (Table 1). We compared whether sociodemographic variables could predict whether participants completed surveys at each time point. The results showed that there were no significant differences between participants who completed the survey at all time points and those who did not complete the survey regarding sex, age, education level, marital status, work status, and economic status.
The majority of the longitudinal sample had been infected with COVID-19 for the first time during the year 2020 (69.5%), had not been hospitalized for COVID-19 (85%), and had been vaccinated against COVID-19 (83.9%). The average severity of COVID-19 in the acute phase was 24.7 (standard deviation = 7.8, ranging from 4 to 44). Furthermore, 27.6% of the respondents reported that they had received a psychiatric diagnosis before COVID-19 infection.
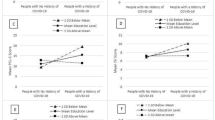
Table 2 presents descriptive statistics for fatigue, post-COVID impairments, and mental health outcomes over time in the longitudinal sample. A decline in mean total fatigue score was observed from T0 to T2. In addition, the prevalence of fatigue (scores > 60 points) decreased constantly from 90.5% to 83.5% from T0 to T2. The mean values of post-COVID impairments decreased slightly from T0 to T2. Figure 1 presents the proportion of clinically significant levels of depression (≥ 10 points on PHQ-9), anxiety (≥ 10 points on GAD-7), and insomnia (≥ 10 points on ISI) over time.

Proportion of people reporting clinically significant levels of depression, anxiety, and insomnia over time
Predictors of the trajectories of depression, anxiety, and insomnia
Adjusted estimates of the changes in depression, anxiety, and insomnia scores over time from the linear mixed models are shown in Table 3. The results demonstrated a significant decline in depression over time, while no significant changes were observed in anxiety and insomnia. We also studied the interaction between time and other variables including sociodemographic variables, COVID-19-related variables, and previous psychiatric diagnosis, but none of the interactions proved significant. The model fit metrics (AIC and BIC) suggested that adding the interactions only diminished the model fit.
Table 4 presents estimates derived from the linear mixed models examining the associations between sociodemographic variables, COVID-19-related variables, previous psychiatric diagnosis and the outcome variables. Separate models were employed for depression, anxiety, and insomnia. The findings indicated that younger adults and individuals experiencing more severe COVID-19 infection in the acute phase exhibited poorer mental health outcomes (Table 4).
The outcome of the linear mixed model, examining the associations between fatigue, post-COVID impairments and the outcome variables (depression, anxiety, and insomnia) are presented in Table 5. We conducted the analysis at the individual level, ensuring implicit adjustment for sociodemographic factors, COVID-related variables, and previous psychiatric diagnosis. The results showed that fatigue appeared to be a significant predictor for all outcomes, and impairments in mental function were an additional significant predictor for depression and anxiety. Both variables had a positive impact on all outcomes, with fatigue being the strongest predictor.
Discussion
We investigated trajectories of mental health outcomes over one year in Swedish adults with COVID-19, using a three-wave survey. Our results demonstrated a significant decline in depression over time, while small, nonsignificant fluctuations were observed in anxiety and insomnia. Furthermore, younger adults and individuals who experienced more severe COVID-19 infections in the acute phase at baseline exhibited poorer mental health outcomes. Fatigue emerged as the most consistent predictor of changes in depression, anxiety, and insomnia. Impairments in mental function due to COVID-19 infection appeared as one of the main predictors of changes in depression and anxiety but not insomnia.
In this study, levels of depression decreased constantly, anxiety exhibited a slight increase, followed by a subsequent decrease, remaining below the baseline level, and insomnia increased slightly and then decreased, consistently remaining above the baseline level. Our findings are in line with previous studies indicating that mental health problems remained more prevalent among individuals who have had COVID-19 infection [42,43,44,45,46,47]. However, symptoms of depression and anxiety decreased over time regardless of the initial severity of the disease [48, 49]. There are several possible explanations for these findings. Firstly, depression and anxiety symptoms have shown a decreasing trend in the general population, including our participants, during the COVID-19 pandemic [50]. During the COVID-19 pandemic in Sweden, individuals were encouraged to work from home when possible. Additionally, gatherings of more than 50 people were prohibited, many businesses and higher education institutions voluntarily transitioned to video conferencing, and non-essential travel was significantly reduced. However, at the onset of the study period in February 2022, Swedish authorities changed their strategies in response to the pandemic similar to other European nations, leading to the lifting of the majority of COVID-19 restrictions [51]. The relaxation or removal of COVID-19-related restrictions, facilitated by the global vaccination campaign, has enabled people to resume their pre-pandemic lifestyles and activities. This transition may have alleviated depression and anxiety symptoms, as individuals restore a sense of normality and participate in activities that provide them with joy and fulfillment. Another potential factor is the enactment of mental health recovery strategies by policymakers in various countries, including Sweden. Strategies include initiatives to monitor, inform, educate, intervene, and research mental health issues in society [52], and efforts target both immediate and long-term mental health outcomes. The third possible explanation for these findings is sustained recovery of COVID-19-related persistent symptoms over time. A substantial proportion of individuals infected with COVID-19 reports experiencing at least one moderate-to-severe impairment due to COVID-19 infection, with fatigue being the most commonly reported symptom [17, 53,54,55,56,57,58,59,60,61]. Furthermore, our previous cross-sectional study revealed that post-COVID impairments and fatigue emerged as significant predictors of mental ill-health in individuals who were infected with COVID-19 infection [10]. However, a progressive improvement has been observed in a wide array of symptoms over time [48, 62, 63]. Our study results indicate that impairments in mental function and fatigue affect depression and anxiety changes over time. These factors shape the dynamics of depression and anxiety and are key for their longitudinal course, thus, managing these complaints may improve mental well-being. In summary, the reduction of symptoms of depression and anxiety observed in this study may be linked to the global recovery from the COVID-19 pandemic and the improvement of post-COVID complaints, especially fatigue.
We found that insomnia, unlike depression and anxiety, increased slightly before decreasing during COVID-19 recovery, but remained above baseline throughout the study period. This indicates a complex interaction of factors affecting sleep quality in this population. These findings are consistent with a previous study which demonstrated a decrease in the symptoms of depression and anxiety whereas increased symptoms of insomnia among COVID-19 patients over time [64]. Additionally, another study indicated that there was no significant change in insomnia over time among COVID-19 patients [65]. Several factors may contribute to this pattern of insomnia exhibiting a different pattern than other symptoms of mental ill-health. First, the rates of insomnia increased significantly during the COVID-19 pandemic like other mental health issues [4] and the prevalence of insomnia was higher in COVID-19 infected patients compared with the general population [10, 64, 66]. The initial increase in insomnia could be attributed to the physiological and psychological effects of the acute phase of COVID-19 infection and the side effects of COVID-19-related medications which disrupted sleep quality and quantity during the early stages of recovery and increased the risk of developing chronic insomnia later after recovery [55, 67,68,69]. Second, sleep-related problems were reported as one of the most common remaining symptoms experienced after recovering from COVID-19 [17, 48]. However, post-COVID impairments did not significantly contribute to changes in insomnia following COVID-19 infection in the current study. Interestingly, it was observed that fatigue emerged as a significant predictor in relation to insomnia. The co-occurrence of fatigue and insomnia has previously been found to be highly prevalent among individuals following recovery from COVID-19 infection [70]. This finding suggests that these two symptoms frequently manifest together in individuals who have experienced the illness. Additionally, several studies have highlighted the presence of fluctuations and relapses in post-COVID-19 fatigue over time [48, 71]. The interplay between fatigue and insomnia can create a vicious cycle, particularly among patients with long-term COVID [72]. Fatigue can contribute to increased sleep difficulties, while insomnia can exacerbate feelings of fatigue and prolong recovery. This bidirectional relationship between fatigue and insomnia may lead to a chronic cycle of symptoms and further impact overall well-being. Lastly, it is essential to consider the bidirectional relationship between mental health and sleep. Insomnia can exacerbate persistent symptoms of depression and anxiety, while these mental health conditions can also contribute to sleep disturbances [73]. To reduce symptoms of depression and anxiety may help to improve insomnia in COVID-19 survivors, and better mental health and coping skills can improve sleep quality. Insomnia needs ongoing assessment and treatment in individuals infected with COVID-19. In addition, addressing fatigue and mood may also reduce insomnia.
Further analysis revealed that younger adults and individuals who experienced more severe COVID-19 infections in the acute phase exhibited poorer mental health outcomes. Previous studies have demonstrated that younger adults have been more profoundly affected by the pandemic and exhibit higher levels of mental health problems [4, 74, 75]. Younger adults, despite primarily experiencing mild COVID-19 infections, faced greater challenges related to the long-term impacts of COVID-19 infection, which significantly disrupted their presentation and performance in their work, education, and daily activities. Hence, it can be concluded that young adults remain within the at-risk group for mental ill-health following COVID-19 infection. Moreover, prior research has consistently demonstrated that the severity of COVID-19 infection in the acute phase is strongly linked to persistent post-infection symptoms [53, 55, 56, 61], emerging as the most robust predictor of post-COVID impairments (Badinlou et al., 2023). Additionally, it has been shown to contribute to higher levels of mental ill-health following COVID-19 infection [10]. Therefore, it is reasonable to conclude that individuals who experienced severe COVID-19 infection in the acute phase continue to be at risk for mental ill-health. These findings highlight the importance of considering sociodemographic and COVID-19-related factors when examining the impact of COVID-19 on mental well-being.
The primary objective of our study was to explore the potential trajectories of mental health changes following COVID-19 infection. To achieve this goal, we focused on minimizing the risk of overlooking real effects (i.e., Type II errors) rather than strictly controlling the risk of falsely identifying effects (i.e., Type I errors). This approach was deemed more appropriate for our exploratory research, since it allowed us to prioritize detecting patterns in the data, even if it meant there was a slightly increased risk of overlooking some effects.
The current study has several practical implications. First, understanding changes in mental health outcomes following COVID-19 infection and identifying risk factors could help healthcare providers to develop targeted interventions to support those who have been infected and may be experiencing psychological problems. Second, the findings provide policymakers with evidence-based insights to implement strategies that can mitigate the long-term mental health impact of the COVID-19 infection, and promote mental well-being in individuals infected with COVID-19, even those who experienced a mild infection. Finally, it contributes to the broader body of research on the mental health consequences of infectious diseases, potentially guiding future pandemic preparedness and response efforts.
Nevertheless, it is important to interpret the results of the study in the context of its limitations and consider potentially confounding factors. First, the current study uses self-reported data for mental health outcomes, which may be biased or inaccurate compared to clinical assessments. Second, it uses a convenience sample, which may limit the generalizability of the findings. Hence, future studies should use more representative samples. Third, it may suffer from non-response bias, as participants who continued or dropped out may differ in important ways. Fourth, we could not establish causality between COVID-19 infection and mental health changes, as there may be other confounding factors. Fifth, it lacks a control group that did not contract COVID-19, which makes it hard to isolate the effects of the infection on mental health. Sixth, majority of participant in the current study was female, introducing the possibility of gender-related biases and potentially limiting the generalizability of the findings to a more balanced demographic.
Conclusions
This study provides a longitudinal perspective on mental health issues following COVID-19 infection, shedding light on the dynamic nature of mental health outcomes over time and underscoring the importance of continued support and interventions tailored to the changing mental health requirements of this affected population. Further research is needed to understand the underlying factors contributing to these changes and to develop targeted interventions for individuals experiencing persistent mental health symptoms.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Leung CM, Ho MK, Bharwani AA, Cogo-Moreira H, Wang Y, Chow MS, Fan X, Galea S, Leung GM, Ni MY. Mental disorders following COVID-19 and other epidemics: a systematic review and meta-analysis. Transl Psychiatry. 2022;12(1):205. https://doi.org/10.1038/s41398-022-01946-6.
Robinson E, Sutin AR, Daly M, Jones A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J Affect Disord. 2022;296:567–76. https://doi.org/10.1016/j.jad.2021.09.098.
Wu T, Jia X, Shi H, Niu J, Yin X, Xie J, Wang X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J Affect Disord. 2021;281:91–8. https://doi.org/10.1016/j.jad.2020.11.117.
McCracken LM, Badinlou F, Buhrman M, Brocki KC. Psychological impact of COVID-19 in the Swedish population: Depression, anxiety, and insomnia and their associations to risk and vulnerability factors. Eur Psychiatry. 2020;63(1): e81. https://doi.org/10.1192/j.eurpsy.2020.81.
Patel K, Robertson E, Kwong AS, Griffith GJ, Willan K, Green MJ, Di Gessa G, Huggins CF, McElroy E, Thompson EJ, Maddock J. Psychological distress before and during the COVID-19 pandemic among adults in the United Kingdom based on coordinated analyses of 11 longitudinal studies. JAMA Netw Open. 2022;5(4):e227629-. https://doi.org/10.1001/jamanetworkopen.2022.7629
Cenat JM, Farahi SM, Dalexis RD, Darius WP, Bekarkhanechi FM, Poisson H, Broussard C, Ukwu G, Auguste E, Nguyen DD, Sehabi G. The global evolution of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis of longitudinal studies. J Affect Disord. 2022;315:70–95. https://doi.org/10.1016/j.jad.2022.07.011.
Hettich N, Entringer TM, Kroeger H, Schmidt P, Tibubos AN, Braehler E, Beutel ME. Impact of the COVID-19 pandemic on depression, anxiety, loneliness, and satisfaction in the German general population: a longitudinal analysis. Soc Psychiatry Psychiatr Epidemiol. 2022;57(12):2481–90. https://doi.org/10.1007/s00127-022-02311-0.
Prati G, Mancini AD. The psychological impact of COVID-19 pandemic lockdowns: a review and meta-analysis of longitudinal studies and natural experiments. Psychol Med. 2021;51(2):201–11. https://doi.org/10.1017/S0033291721000015.
Rehman U, Yıldırım M, Shahnawaz MG. A longitudinal study of depression, anxiety, and stress among Indians during COVID-19 pandemic. Psychol Health Med. 2023;28(1):60–8. https://doi.org/10.1080/13548506.2021.2023751.
Badinlou F, Lundgren T, Jansson-Fröjmark M. Mental health outcomes following COVID-19 infection: Impacts of post-COVID impairments and fatigue on depression, anxiety, and insomnia—A web survey in Sweden. BMC Psychiatry. 2022;22(1):1–1. https://doi.org/10.1186/s12888-022-04405-0.
Ausserhofer D, Mahlknecht A, Engl A, Piccoliori G, Pfitscher G, Silbernagl P, Giacomoni F, Pycha R, Lombardo S, Gärtner T, Mian M. Relationship between depression, anxiety, stress, and SARS-CoV-2 infection: a longitudinal study. Front Psychol. 2023;14:1116566. https://doi.org/10.3389/fpsyg.2023.1116566.
Senra H. Bidirectional associations and common inflammatory biomarkers in COVID-19 and mental health disorders: A window of opportunity for future research?. BBI - Health. 2021;13. https://doi.org/10.1016/j.bbih.2021.100237.
Taquet M, Harrison PJ. Why is COVID-19 associated with mental illness? Med. 2021;2(8):899–902. https://doi.org/10.1016/j.medj.2021.06.009.
Taquet M, Luciano S, Geddes JR, Harrison PJ. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry. 2021;8(2):130–40. https://doi.org/10.1016/S2215-0366(20)30462-4.
Thompson EJ, Stafford J, Moltrecht B, Huggins CF, Kwong AS, Shaw RJ, Zaninotto P, Patel K, Silverwood RJ, McElroy E, Pierce M. Mental health outcomes following COVID-19 infection: Evidence from 11 UK longitudinal population studies. medRxiv. 2022:2022–05. https://doi.org/10.1016/s2215-0366(22)00307-8
Matsumoto K, Hamatani S, Shimizu E, Käll A, Andersson G. Impact of post-COVID conditions on mental health: a cross-sectional study in Japan and Sweden. BMC Psychiatry. 2022;22(1):1–3. https://doi.org/10.1186/s12888-022-03874-7.
Badinlou F, Forsström D, Jansson-Fröjmark M, Abzhandadze T, Lundgren T. Impairments following COVID-19 infection: Manifestations and investigations of related factors. Sci Rep. 2023;13(1):6564. https://doi.org/10.1038/s41598-023-33810-y.
Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J Infect Dis. 2022. https://doi.org/10.1093/infdis/jiac136.
El Sayed S, Shokry D, Gomaa SM. Post-COVID-19 fatigue and anhedonia: a cross-sectional study and their correlation to post-recovery period. Neuropsychopharmacol Rep. 2021;41(1):50–5. https://doi.org/10.1002/npr2.12154.
Poole-Wright K, Guennouni I, Sterry O, Evans RA, Gaughran F, Chalder T. Fatigue outcomes following COVID-19: a systematic review and meta-analysis. BMJ Open. 2023;13(4): e063969. https://doi.org/10.1136/bmjopen-2022-063969.
Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81. https://doi.org/10.1016/j.jbi.2008.08.010.
Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95: 103208. https://doi.org/10.1016/j.jbi.2019.103208.
World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–4. https://doi.org/10.1001/jama.2013.281053.
Public Health Agency of Sweden (Folkhälsomyndigheten). COVID-19. Available: https://www.folkhalsomyndigheten.se/the-public-health-agency-of-sweden/communicable-disease-control/covid-19/.2021. Accessed October 2021.
World Health Organization (WHO). Coronavirus disease (COVID-19). https://www.who.int/health-topics/coronavirus#tab=tab_3. 2021. Accessed October 2021.
Smets EM, Garssen B, Bonke BD, De Haes JC. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. 1995;39(3):315–25. https://doi.org/10.1016/0022-3999(94)00125-O.
Schwarz R, Krauss O, Hinz A. Fatigue in the general population. Oncol Res Treat. 2003;26(2):140–4. https://doi.org/10.1159/000069834.
Tian J, Hong JS. Application of the Chinese version of the MFI-20 in detecting the severe fatigue in cancer patients. Support Care Cancer. 2013;21(8):2217–23. https://doi.org/10.1007/s00520-013-1783-x.
Ericsson A, Mannerkorpi K. Assessment of fatigue in patients with fibromyalgia and chronic widespread pain. Reliability and validity of the Swedish version of the MFI-20. Disabil. 2007;29(22):1665–70. https://doi.org/10.1080/09638280601055782.
Lundh Hagelin C, Wengström Y, Runesdotter S, Johan FC. The psychometric properties of the Swedish Multidimensional Fatigue Inventory MFI-20 in four different populations. Acta Oncol. 2007;46(1):97–104. https://doi.org/10.1080/02841860601009430.
World Health Organization (WHO). The International Classification of Functioning, Disability and Health (ICF). 2001. Available from: https://www.who.int/classifications/international-classification-of-functioningdisability-and-health. Accessed January 2022.
Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. 2002;32(9):509–15. https://doi.org/10.3928/0048-5713-20020901-06.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x.
Titov N, Dear BF, McMillan D, Anderson T, Zou J, Sunderland M. Psychometric comparison of the PHQ-9 and BDI-II for measuring response during treatment of depression. Cogn Behav Therapy. 2011;40(2):126–36. https://doi.org/10.1080/16506073.2010.550059.
Beard C, Björgvinsson T. Beyond generalized anxiety disorder: psychometric properties of the GAD-7 in a heterogeneous psychiatric sample. J Anxiety Disord. 2014;28:547–52. https://doi.org/10.1016/j.janxdis.2014.06.002.
Löwe B, Spitzer RL, Williams JB, Mussell M, Schellberg D, Kroenke K. Depression, anxiety and somatization in primary care: syndrome overlap and functional impairment. Gen Hosp Psychiatry. 2008;30:191–9. https://doi.org/10.1016/j.genhosppsych.2008.01.001.
Rutter LA, Brown TA. Psychometric properties of the Generalized Anxiety Disorder Scale-7 (GAD-7) in outpatients with anxiety and mood disorders. J Psychopathol Behav Assess. 2017;39:140–6. https://doi.org/10.1007/s10862-016-9571-9.
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7. https://doi.org/10.1001/archinte.166.10.1092.
Bastien CH, Vallieres A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2:297–307. https://doi.org/10.1016/S1389-9457(00)00065-4.
Morin CM, Belleville G, Belanger L, Ivers H. The insomnia severity index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34:601–8. https://doi.org/10.1093/sleep/34.5.601.
Fleiss JL. Design and analysis of clinical experiments. John Wiley & Sons; 2011.
Ma YF, Li W, Deng HB, Wang L, Wang Y, Wang PH, Bo HX, Cao J, Wang Y, Zhu LY, Yang Y. Prevalence of depression and its association with quality of life in clinically stable patients with COVID-19. J Affect Disord. 2020;275:145–8. https://doi.org/10.1016/j.jad.2020.06.033.
Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, Melloni EM, Furlan R, Ciceri F, Rovere-Querini P, Benedetti F. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. BBI - Health. 2020;89:594–600. https://doi.org/10.1016/j.bbi.2020.07.037.
Wang QQ, Kaelber DC, Xu R, Volkow ND. COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol Psychiatry;26(1):30–9. https://doi.org/10.1038/s41380-020-00880-7.
Xie Q, Liu XB, Xu YM, Zhong BL. Understanding the psychiatric symptoms of COVID-19: a meta-analysis of studies assessing psychiatric symptoms in Chinese patients with and survivors of COVID-19 and SARS by using the Symptom Checklist-90-Revised. Transl Psychiatry. 2021;11(1):1. https://doi.org/10.1038/s41398-021-01416-5.
Yuan K, Zheng YB, Wang YJ, Sun YK, Gong YM, Huang YT, Chen X, Liu XX, Zhong Y, Su SZ, Gao N. A systematic review and meta-analysis on prevalence of and risk factors associated with depression, anxiety and insomnia in infectious diseases, including COVID-19: a call to action. Mol Psychiatry. 2022:1–9. https://doi.org/10.1038/s41380-022-01638-z.
Zarghami A, Farjam M, Fakhraei B, Hashemzadeh K, Yazdanpanah MH. A report of the telepsychiatric evaluation of SARS-CoV-2 patients. TELEMED E-HEALTH. 2020;26(12):1461–5. https://doi.org/10.1089/tmj.2020.0125.
Huang L, Li X, Gu X, Zhang H, Ren L, Guo L, Liu M, Wang Y, Zhang X. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: a longitudinal cohort study. Ancet Respir Med. 2022;10(9):863–76. https://doi.org/10.1016/s2213-2600(22)00126-6.
Scott ES, Lubetkin EI, Janssen MF, Yfantopolous J, Bonsel GJ, Haagsma JA. Cross-sectional and longitudinal comparison of health-related quality of life and mental well-being between persons with and without post COVID-19 condition. fepid. 2023;3:1144162. https://doi.org/10.3389/fepid.2023.1144162.
Bendau A, Kunas SL, Wyka S, Petzold MB, Plag J, Asselmann E, Ströhle A. Longitudinal changes of anxiety and depressive symptoms during the COVID-19 pandemic in Germany: The role of pre-existing anxiety, depressive, and other mental disorders. J Anxiety Disord. 2021;79: 102377. https://doi.org/10.1016/j.janxdis.2021.102377.
Public Health Agency of Sweden. De flesta åtgärder mot covid-19 upphör den 9 februari. 2022. Available from: https://www.folkhalsomyndigheten.se/nyheter-och-press/nyhetsarkiv/2022/februari/de-flesta-atgarder-mot-covid-19-upphor-den-9-februari/. Accessed December 2023.
Arendt F, Markiewitz A, Mestas M, Scherr S. COVID-19 pandemic, government responses, and public mental health: Investigating consequences through crisis hotline calls in two countries. Soc Sci Med. 2020;265: 113532. https://doi.org/10.1016/j.socscimed.2020.113532.
Boscolo-Rizzo P, Guida F, Polesel J, Marcuzzo AV, Capriotti V, D’Alessandro A, Zanelli E, Marzolino R, Lazzarin C, Antonucci P, Sacchet E. Sequelae in adults at 12 months after mild-to-moderate coronavirus disease 2019 (COVID-19). Int Forum Allergy Rhinol. 2021;11(12):1685–8. https://doi.org/10.1002/alr.22832.
Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, Re'em Y, Redfield S, Austin JP, Akrami A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine. 2021;38. https://doi.org/10.1016/j.eclinm.2021.101019.
Han Q, Zheng B, Daines L, Sheikh A. Long-Term sequelae of COVID-19: A systematic review and meta-analysis of one-year follow-up studies on post-COVID symptoms. Pathogens. 2022;11(2):269. https://doi.org/10.3390/pathogens11020269.
Huang L, Yao Q, Gu X, Wang Q, Ren L, Wang Y, Hu P, Guo L, Liu M, Xu J, Zhang X. 1-year outcomes in hospital survivors with COVID-19: a longitudinal cohort study. The lancet. 2021;398(10302):747–58. https://doi.org/10.1016/S0140-6736(21)01755-4.
Logue JK, Franko NM, McCulloch DJ, McDonald D, Magedson A, Wolf CR, Chu HY. Sequelae in adults at 6 months after COVID-19 infection. JAMA Netw open. 2021;4(2):e210830. https://doi.org/10.1001/jamanetworkopen.2021.0830.
Seeßle J, Waterboer T, Hippchen T, Simon J, Kirchner M, Lim A, Müller B, Merle U. Persistent symptoms in adult patients 1 year after coronavirus disease 2019 (COVID-19): a prospective cohort study. Clin Infect Dis. 2022;74(7):1191–8. https://doi.org/10.1093/cid/ciab611.
Sudre CH, Murray B, Varsavsky T, Graham MS, Penfold RS, Bowyer RC, Pujol JC, Klaser K, Antonelli M, Canas LS, Molteni E. Attributes and predictors of long COVID. Nat Med. 2021;27(4):626–31. https://doi.org/10.1038/s41591-021-01292-y.
Sykes DL, Holdsworth L, Jawad N, Gunasekera P, Morice AH, Crooks MG. Post-COVID-19 symptom burden: what is long-COVID and how should we manage it? Lung. 2021;199(2):113–9. https://doi.org/10.1007/s00408-021-00423-z.
Zhang X, Wang F, Shen Y, Zhang X, Cen Y, Wang B, Zhao S, Zhou Y, Hu B, Wang M, Liu Y. Symptoms and health outcomes among survivors of COVID-19 infection 1 year after discharge from hospitals in Wuhan, China. JAMA Netw open. 2021;4(9):e2127403-. https://doi.org/10.1001/jamanetworkopen.2021.27403.
Hellemons ME, Huijts S, Bek LM, Berentschot JC, Nakshbandi G, Schurink CA, Vlake JH, van Genderen ME, van Bommel J, Gommers D, Odink A. Persistent health problems beyond pulmonary recovery up to 6 months after hospitalization for COVID-19: a longitudinal study of respiratory, physical, and psychological outcomes. Ann Am Thorac Soc. 2022;19(4):551–61. https://doi.org/10.1513/AnnalsATS.202103-340OC.
Tran VT, Riveros C, Clepier B, Desvarieux M, Collet C, Yordanov Y, Ravaud P. Development and validation of the long covid symptom and impact tools, a set of patient-reported instruments constructed from patients’ lived experience. medRxiv. 2021. https://doi.org/10.1101/2021.03.18.21253903.
Liu C, Pan W, Li L, Li B, Ren Y, Ma X. Prevalence of depression, anxiety, and insomnia symptoms among patients with COVID-19: A meta-analysis of quality effects model. J Psychosom Res. 2021;147: 110516. https://doi.org/10.1016/j.jpsychores.2021.110516.
Moseholm E, Midtgaard J, Bollerup S, Apol ÁD, Olesen OB, Jespersen S, Weis N. Psychological distress among hospitalized COVID-19 patients in Denmark during the first 12 months of the pandemic. Int J Environ Res Public Health. 2022;19(16):10097. https://doi.org/10.3390/ijerph191610097.
Jahrami HA, Alhaj OA, Humood AM, Alenezi AF, Fekih-Romdhane F, AlRasheed MM, Saif ZQ, Bragazzi NL, Pandi-Perumal SR, BaHammam AS, Vitiello MV. Sleep disturbances during the COVID-19 pandemic: a systematic review, meta-analysis, and meta-regression. Sleep Med Rev. 2022;62: 101591. https://doi.org/10.1016/j.smrv.2022.101591.
Pudlo R, Jaworska I, Szczegielniak A, Niedziela J, Kułaczkowska Z, Nowowiejska-Wiewióra A, Jaroszewicz J, Gąsior M. Prevalence of insomnia in the early post-COVID-19 recovery period. Int J Environ Res Public Health. 2022;19(21):14224. https://doi.org/10.3390/ijerph192114224.
Shi L, Lu ZA, Que JY, Huang XL, Liu L, Ran MS, Gong YM, Yuan K, Yan W, Sun YK, Shi J. Prevalence of and risk factors associated with mental health symptoms among the general population in China during the coronavirus disease 2019 pandemic. JAMA NETW OPEN. 2020;3(7):e2014053-. https://doi.org/10.1001/jamanetworkopen.2020.14053.
Xu F, Wang X, Yang Y, Zhang K, Shi Y, Xia L, Hu X, Liu H. Depression and insomnia in COVID-19 survivors: a cross-sectional survey from Chinese rehabilitation centers in Anhui province. Sleep Med. 2022;91:161–5. https://doi.org/10.1016/j.sleep.2021.02.002.
Zhao Y, Yang C, An X, Xiong Y, Shang Y, He J, Qiu Y, Zhang N, Huang L, Jia J, Xu Q. Follow-up study on COVID-19 survivors one year after discharge from hospital. nt J Infect Dis. 2021;112:173–82. https://doi.org/10.1016/j.ijid.2021.09.017.
Crook H, Raza S, Nowell J, Young M, Edison P. Long covid—mechanisms, risk factors, and management. bmj. 2021;374. https://doi.org/10.1136/bmj.n1648.
Percze AR, Nagy A, Polivka L, Barczi E, Czaller I, Kovats Z, Varga JT, Ballai JH, Muller V, Horvath G. Fatigue, sleepiness and sleep quality are SARS-CoV-2 variant independent in patients with long COVID symptoms. Inflammopharmacology. 2023:1–7. https://doi.org/10.1007/s10787-023-01190-4.
Meaklim H, Saunders WJ, Byrne ML, Junge MF, Varma P, Finck WA, Jackson ML. Insomnia is a key risk factor for persistent anxiety and depressive symptoms: A 12-month longitudinal cohort study during the COVID-19 pandemic. J Affect Disord. 2023;322:52–62. https://doi.org/10.1016/j.jad.2022.11.021.
Tull MT, Edmonds KA, Scamaldo KM, Richmond JR, Rose JP, Gratz KL. Psychological outcomes associated with stay-at-home orders and the perceived impact of COVID-19 on daily life. Psychiatry Res. 2020;289: 113098. https://doi.org/10.1016/j.psychres.2020.113098.
Maarefvand M, Hosseinzadeh S, Farmani O, Safarabadi Farahani A, Khubchandani J. Coronavirus outbreak and stress in IraniansInt. J Environ Res Public Health. 2020;17(12):4441. https://doi.org/10.3390/ijerph17124441.
Acknowledgements
We would like to thank all athletes that took part in this study.
Funding
Open access funding provided by Karolinska Institute. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
F.B., M.J.F., and T.L. conceptualized the study. F.B. administered the project and collected the data. F.B., and F.R. prepared the data and performed the statistical analyses. F.B., F.R., and M.H–L. wrote the first draft. F.B, F.R., M.H–L., T.L., T.A., and M.J.F. revised the article. F.B, F.R., M.H–L. T.A., and M.J.F. edited the article. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Swedish national ethical board (dnr 2021–06617-01) and informed consent was obtained from all participants. All procedures utilized in collecting data for the current paper follow the ethical standards of the Helsinki Declaration of 1964 and subsequent amendments.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Badinlou, F., Rahimian, F., Hedman-Lagerlöf, M. et al. Trajectories of mental health outcomes following COVID-19 infection: a prospective longitudinal study. BMC Public Health 24, 452 (2024). https://doi.org/10.1186/s12889-024-17997-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-024-17997-x