
Abstract
Background
The negative impact of the COVID-19 pandemic on the mental health is now clearly established. However, information on the levels of mental ill health of people infected with COVID-19 and potential correlates of poor mental health is still limited. Therefore, the current study aimed to study indicative of potential mental health problems in individuals with a history of probable or confirmed SARS CoV-2 infection/infections and address the impacts of post-COVID impairments and fatigue following COVID-19 infection/infections on depression, anxiety, and insomnia.
Methods
A web-survey including demographics, questions related to COVID-19 status and post-COVID impairments, and standardized measures of depression, anxiety, insomnia, and fatigue was completed by 507 individuals with a history of probable or confirmed SARS CoV-2 infection/infections.
Results
We found significant rates of significant depression, anxiety, and insomnia in our sample, with more than 70% experiencing levels above the clinical cut offs for at least one psychological health problems. Higher levels of depression, anxiety, and insomnia were associated with the severity of COVID-19 infection in the acute phase, hospitalization because of COVID-19, and higher levels of post-COVID impairments and fatigue. Reduced motivation emerged as the strongest predictor for mental ill health.
Conclusions
These findings highlight that individuals infected with COVID-19, especially those who still have experienced post-COVID impairments, are more likely to suffer from mental ill-health and may be more vulnerable for poor mental health outcomes. Therefore, more effective actions are needed to take in order to promote and protect mental health of individuals with a history of COVID-19 infection.
Similar content being viewed by others


Background
Since the beginning of the COVID-19 pandemic, the study of mental health has been the focus for many investigations around the world. Early studies focused mainly on the psychosocial response to the COVID-19 pandemic and impacts of pandemic-related strategies, such as quarantine, lockdown, closing schools/universities, movement and travel restrictions, on mental health outcomes in the general population [1,2,3,4,5,6]. Findings from studies in different countries showed that the prevalence of mental health problems increased significantly in the general population during the COVID-19 pandemic [7,8,9,10,11]. In Sweden, studies of mental health in the early phase of the COVID-19 pandemic showed elevated rates of depression, anxiety, and insomnia in the general population compared with before the pandemic, the same as in other counties [12, 13].
With increasing number of COVID-19 cases and hospitalization due to COVID-19 in the different countries, a possible bidirectional association between COVID-19 and mental health problems was attracting the attention of researchers [14,15,16]. On the one hand, pre‐existing mental health problems could increase the risk to get COVID infection, or make the outcomes of the infection worse [17,18,19,20,21]. On the other hand, a significant proportion of patients with and survivors of COVID-19 reported numbers of psychological issues, such as post-traumatic stress disorder (PTSD), depression, anxiety, insomnia, and obsessive–compulsive symptoms [22,23,24,25,26].
Follow-up studies on COVID-19 survivors after discharge from hospital or/and recover from COVID-19 reported an unexpected result called post COVID-19 condition [27,28,29]. This condition affects individuals infected with COVID-19 and is characterized by a wide range of persistent symptoms even after months of the onset of disease or hospitalization [28, 30,31,32,33,34,35]. The post COVID-19 condition has also been widely reported by individuals with the mild-to-moderate symptoms in the acute phase of SARS-CoV-2 disease, mostly recovered without requiring special treatment or/and hospitalization [36]. A recent meta-analysis, including data from fifty studies, shows that the global prevalence of post-COVID condition was 0.43 (95% confidence interval [CI], 0.39–0.46). In other words, nearly half of the people with a history of probable or confirmed SARS CoV-2 infection experienced mid- and long-term symptoms after recovery from COVID-19 [37]. Long‐term impacts of COVID‐19 infection can be multi-systemic problems and disabilities, and fatigue in general was the most commonly reported symptom in previous studies [37,38,39,40,41,42].
A collaborative cross-sectional study in Japan and Sweden examining associations between mental health and post-COVID conditions showed that post-COVID condition includes mental health issues, such as depression and anxiety, were significantly higher in groups with post-COVID conditions, compared to noninfected groups and infected group without post-COVID conditions. In addition, post-COVID conditions was demonstrated to be a risk for developing mental health illness [43]. Another study, conducted in Sweden reexamined the prevalence of depression, anxiety, and insomnia in the general population and the impact of COVID-19-related persistent symptoms on these psychiatric symptoms two years after the first appearance of COVID-19. Findings showed that the level of depression did not change significantly, the level of anxiety decreased, and the level of insomnia had increased compared with the early phase of the pandemic in Sweden. COVID-19-related persistent symptoms were found as an important vulnerability factor for mental ill-health [44]. However, research on the mental health of people infected with COVID-19 is still limited, and it is not clear how post-COVID impairments and fatigue, as the most common persistent symptom, might interrelate with mental health outcomes. The first purpose of the current study was to determine indicative of potential mental health problems in individuals with a history of probable or confirmed SARS CoV-2 infection/infections. To further enhance the knowledge, the second aim of the study was to address the impacts of post-COVID impairments and fatigue on mental health outcomes following COVID-19 infection/infections.
Methods
Participants and setting of the study
A total 507 people was included in the current study. Inclusion criteria were: (i) infected with COVID-19; (ii) age (≥ 18 years); (iii) being a resident of Sweden; (iv) ability to understand Swedish and use the internet in order to complete web-survey. The following exclusion criteria was used; (i) age under 18 years old, (ii) did not complete scales, or (iii) not infected with COVID-19. They were therefore unable to complete COVID-19-related and post-COVID questions. We used convenience sampling to recruit participants in the current study. In that, an announcement including information about the study and a link to a web-survey was posted in COVID-19-related Facebook groups and sites, and the Karolinska institute homepages. In order to recruit potential participants, the study information was administered at four primary care centers treating post-COVID patients in Stockholm, Sweden.. The participants’ age ranged between 19 and 81 years old (M = 47.72, SD = 10.62). Demographic information about the participants is presented in Table 1.
Table 2 presents the descriptive statistics of COVID-19-related variables. The majority of the participants reported they had been infected with COVID-19 for the first time in the first and second wave of COVID-19 in Sweden, spring and autumn 2020 [45].
Measures
Demographic information
Demographic variables were age, gender, education, marital status, work status, and economic status.
COVID-19-related variables
COVID-19-related variables included infected with COVID-19, hospitalization due to COVID-19, been high-risk group for COVID-19, vaccinated against COVID-19, and COVID-19 severity in the acute phase. Infected with COVID-19 was measured by a single item in which respondents stated on a 4-point scale if they have/had a confirmed COVID-19 infection supported by positive tests for COVID-19 virus (PCR) and/or positive rapid antigen test on a 4-point scale (yes, I have had it one time, yes, I have had it two times, yes, I have had it more than two times, yes, I believe I've had it, but have not had it confirmed). Respondent also were asked to state on a binary scale (yes, no) if they have/had been hospitalized because of COVID-19, high-risk group for COVID-19 (including high blood pressure, angina, stroke, heart disease, diabetes, cancer, smoking, respiratory diseases, and impaired immune system), and vaccinated against COVID-19. COVID-19 severity in the acute phase was measured with 15 items, including fever, fatigue, cough, loss of smell/taste, difficulty breathing/shortness of breath, headache/migraine, aches or pain in body, diarrhea, rash on skin, runny or blocked nose, nausea/vomiting, arrhythmia/palpitations, sore throat, cognitive difficulties such as memory and attention difficulties, and mental health issues such as sleep problems, depression and anxiety [46, 47]. Here participants rated symptoms that they had at the beginning of the infection or infections and those the following 4 weeks on a 4-point scale (0 = no, 1 = mild, 2 = moderate, 3 = severe) considering acute COVID-19 usually can last up to 4 weeks from the onset of symptoms [48]. The respondents’ answers to the 15 symptoms of COVID-19 items were summed up to calculate a COVID-19 severity in the acute phase (range 0—45, α = 0.77).
Post-COVID impairments
The post-COVID impairments in the current study were assessed with 54 items used in our previous study [38]. The items were based on previous questionnaires developed to examine long-term impacts of COVID-infection such as the Functional Compass COVID-19 questionnaire and the Long COVID Symptom and Impact Tools [36, 49] and comprehensive literature review of the long-term effects of COVID-19 [32, 33, 48, 50, 51]. Participants rated their impairments due to COVID-19 infection/infections on a 4-point scale (0 = no, 1 = mild, 2 = moderate, 3 = severe). Items were categorized into four sub-categories according to the International Classification of Functioning, Disability and Health [52] as impairments in mental functions including impaired orientation, brain fatigue, lack of appetite, sleep problems, concentration difficulties, attention difficulties, memory problems, impaired organization and planning, impaired mental functions of language, depression, anxiety, stress, obsessions, and compulsions; impairments in sensory functions and pain including poor quality of vision, dry/red/itchy eyes, ringing in ears or tinnitus, dizziness, disturbed balance, loss of taste, loss of smell, feeling of numbness/tingling, generalized pain, pain in head, chest pain, pain in stomach or abdomen, joint pain, and pain in multiple body parts; impairments body system functions including voice problems, impaired heart functions, respiratory distress, cough, tiredness or lack of energy (physical), shortness of breath, sore throat/difficult to swallow, vomiting, impaired nutrient uptake, diarrhea, weight change, nausea, fever/feeling of fever, chills/the feeling of freezing, impaired sexual desire and functions, impaired mobility of movement, decreased muscle power, movement problems, skin changes, rash, and hair loss; and impairments in activities and participation including difficulty taking care of yourself, impaired control of other diseases and drugs, keep special diet, and difficulties in doing housework, impaired work ability/study ability, and difficulty being to leisure activities. The respondents’ answers to each sub-category of post-COVID impairments were summed up and divided the number of items in order to obtain mean for each sub-category as a common way to analysis scores from observational measures in social sciences [53].
Fatigue
The Multidimensional Fatigue Inventory (MFI) is self-report instrument to measure fatigue. The MFI is a 20-item scale and consists of five subscales: general fatigue (GF), physical fatigue (PF), reduced motivation (RM), reduced activity (RA), and mental fatigue (MF). Each scale contains four items. The items are rated on 5-point scale, from 1 (Yes, that is true) to 5 (No, that is not true), scores range from 0 to 20 [54]. This test yields a total score (the sum of all items) and five scale scores calculated as the sum of the items within each subscale. Higher scores indicate higher fatigue levels. The subscale score > 12 was considered clinically significant fatigue [55], and the total score > 60 was considered clinically significant multidimensional fatigue [56]. In this study, we used the Swedish version. Psychometric studies show that the Swedish version of the instrument is reliable and valid [57, 58].
Mental health variables
Mental health variables were considered as outcome variables in the current study and consisted of depression, anxiety, and insomnia. Depression was measured with the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 consists of nine items answered on a four-point scale (0–3), with the total score ranging from 0 to 27 [59, 60]. Anxiety was assessed with the General Anxiety Disorder-7 (GAD-7). The GAD-7 includes seven items answered on a four-point scale (0–3), scores range from 0 to 21 [61,62,63,64]. Insomnia was measured with the Insomnia Severity Index-7 (ISI-7). The ISI-7 consists of seven items to assess the nature, severity, and impact of insomnia answered on a five-point scale (0–4), the total score ranges from 0 to 28 [65, 66]. We used the recommended cutoff scores of ≥ 10 for detecting the clinically significant depression, anxiety, and insomnia in the current study [59, 64, 66].
Procedure
The study was approved by the Swedish national ethical board (dnr 2021–06,617-01) and informed consent was obtained from all participants. Participants answered the survey in the online platform, Research Electronic Data Capture (REDCap), hosted locally at Karolinska institute [67, 68]. Data were collected between the 23th of February and the 5th of April 2022.
Statistical analysis
The data were analyzed using IBM SPSS (IBM, Version 26) [69] and checked for normality, missing values, outliers, or any errors in data. The mean, standard deviation, and numbers or percentage were calculated for each continuous and categorical variable. For purposes of analysis, categorical variables were dichotomized; education (dichotomous: high education, low education), marital status (dichotomous: in relationship, not relationship), work status (dichotomous: not working, working), economic status (dichotomous: above average, average and below average), and infected with COVID-19 (dichotomous: confirmed COVID-19 infection, not confirmed COVID-19 infection). Zero-order correlations (Pearson's r) were calculated to examine the relationship among all measures and to identify primary predictors of the model. To address the second aim, hierarchical linear regression models were applied to explore the contribution of potential predictors on mental health outcomes. Three separate analyses were employed to estimate the predictors’ association with depression, anxiety, and insomnia as dependent variables. For all three regression models, the significant variables were considered as potential predictors. Due to performing multiple tests on a single dataset, alpha-level was adjusted to p ≤ 0.01 in the current study.
Results
Descriptive statistics for mental health, fatigue, and post-COVID impairments variables
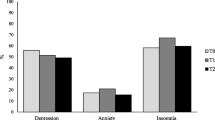
Table 3 presents descriptive statistics for the measures of depression, anxiety, and insomnia. In that, 55%, 20.5%, and 60.9% of the participants reached the cutoff for clinical depression, anxiety, and insomnia, respectively. The majority of the participants reached cutoff for at least one psychological health problems (74.7%). Intercorrelations between these measures were r = 0.71 for depression and anxiety scores, r = 0.58 for depression and insomnia scores, and r = 0.58 for anxiety and insomnia scores.
Table 4 includes summary results from the fatigue scores and prevalence rates per domain. Of all participants, 94.7% (n = 481) reached cutoff for severe fatigue on at least one fatigue dimension, based on cutoff scores > 12. For more details, 89.9% (n = 456), 85.6% (n = 434), 84.8% (n = 430), 51.6% (n = 255), and 73.4% (n = 372) met criteria for likely clinically significant general fatigue, physical fatigue, reduced activity, reduced motivation, and mental fatigue, respectively. Of all participants, 39.3% (n = 194) reached the cutoff for clinically significant multidimensional fatigue. As seen in Table 4, these measures are intercorrelated (see Table 4).
Those surveyed also provided data on post-COVID impairments, each on a scale from 0 to 3, higher scores indicating higher levels of impairments. Table 5 includes summary results from the post-COVID impairments. The highest level of impairment was impairments in activities and participation, followed by impairments in mental functions. As seen in Table 5, these variables are intercorrelated (see Table 5).
Correlational analyses
Table 6 presents correlations between the outcome variables with participant background, COVID-19-related factors, post-COVID impairments, and fatigue dimensions. Notably, the background variables failed to significantly correlate with the mental health outcomes. More serious condition in the acute phase of COVID-19 infection was significantly related with all three outcome variables. Hospitalization because of COVID-19 achieved significant but small correlation with insomnia. Post-COVID impairments and fatigue variables significantly positively correlated with depression, anxiety, and insomnia.
Regression analyses
Table 7 presents the final results of the hierarchical regression models for depression, anxiety, and insomnia. In a three-block model, COVID-19-related factors including severity of COVID-19 infection in the acute phase and hospitalization for COVID-19 were entered into the first block, followed by post-COVID impairments including impairments in mental functions, sensory functions and pain, body system functions, and activities and participation, entered in block 2, and fatigue factors including general fatigue, physical fatigue, reduced activity, reduced motivation, and mental fatigue, entered in block 3. All three blocks reached statistical significance for each of the outcome variables. For depression, fatigue accounted for the largest part of the variance, with \(\Delta\) R2 accounting for 23% of the variance. For anxiety, both fatigue factors and post-COVID impairments accounted similar variance in the equations, with \(\Delta\) R2 accounting for 12% of the variance. For insomnia, COVID-19-related factors accounted for the largest part of the variance. Interestingly, out of all variables, reduced motivation came out as the most important predictor for all three mental health outcomes.
Discussion
The first aim of the current study was to examine levels of mental health problems following COVID-19 infection/infections. The second aim was to study associations between COVID-19-related factors, post-COVID impairments as well as fatigue and mental health problems in individuals with a history of probable or confirmed SARS CoV-2 infection/infections. Results showed significant rates of significant depression (55%), anxiety (20.5%), and insomnia (60.9%) in our sample. The correlational analyses show that severity of COVID-19 infection in the acute phase and hospitalization due to COVID-19 were significantly correlated with mental health outcomes. All post-COVID impairments and fatigue dimensions were significantly associated with depression, anxiety, and insomnia. In multivariate models, generally, severity of COVID-19 infection in the acute phase explained a portion of the variance in depression and insomnia and impairments in mental functions explained variance in depression and anxiety. However, reduced motivation emerged as the most consistent predictor of all three mental health outcomes.
In our study, rates of mental health problems were clearly higher than previous studies using the same measures and cut-off levels, noticeably in depression and insomnia. There are a number of likely explanations. The first possible explanation for these findings lies in our sample and inclusion criteria. In the previous studies, the participants were recruited from social media and age ≥ 18 was a main inclusion criterion [12, 43, 44], whereas we used convenience sampling targeting individuals with a history of probable or confirmed COVID-19 infection. As a result, in studies by Matsumoto et al. [43] and Brocki et al. [44], 13% and 51.2% of the participants reported that they have been infected with the COVID-19, respectively, whereas in our study, 85% of the participants reported confirmed COVID-19 infection/infections supported by positive tests for COVID-19 virus (PCR) and/or positive rapid antigen test, including one time, 61.9%, two times, 20.7%, and more than two times, 2.4%. The second possible explanation of these results is that diagnosis of COVID-19 is likely to be associated with increased rates of mental health problems and subsequent psychiatric diagnoses. In that, psychiatric illness and mental health problems such as depression, anxiety, insomnia, post-traumatic stress disorder, obsessive–compulsive symptoms, and substance use disorders are highly prevalent in patients diagnosed with COVID-19 [16, 21,22,23,24,25,26, 70, 71]. The third possible explanation is that a major proportion of participants in the current study had experienced the post-COVID impairments, such as impairments in mental function, sensory functions and pain, and body system functions. These findings are in line with a previous study that showed that incidence of clinically significant mental health problems was higher in COVID-19-infected participants, and it was more prominent in those with post-COVID conditions [43]. Furthermore, there are a number of previous studies indicating co-occurrence between pain, physical health problems and mental health illness [72,73,74]. The final possible explanation is the timing of data collection. Data for the current study was collected after the peak of the Omicron variant in Sweden, January 2022, which increased COVID-19 cases dramatically and tightened the restrictions. As a result, the rate of reinfection increased. In our sample, 19% (n = 99) of the participants reported that they had been infected for a second time and even a third time in January/February 2022. Considering possible explanations, we can safely say that individuals infected with COVID-19, especially those experiencing post-COVID impairments, are more likely to suffer from mental ill-health and may be more vulnerable for poor mental health outcomes.
Looking at potential predictors, prior severity of COVID-19 infection, post-COVID impairments and fatigue dimensions were associated with poor mental health outcomes and hospitalization because of COVID-19 was positively correlated with insomnia (see Table 6). These results are in line with previous studies showing high levels of mental health problems months after COVID-19 recovery, and a more serious COVID-19 infection in acute phase might be a risk factor for developing mental health illness [75, 76]. In more detail, individuals infected with COVID-19 showed the higher levels of mental health symptoms in the form of depression, generalized anxiety, and post-traumatic stress [43]. In more recent studies, post-COVID condition is clearly linked to mental ill-health [43, 76, 77].
Multivariate analyses were used to estimate the unique variance accounted for in depression, anxiety, and insomnia scores. The block of COVID-19-related variables explained unique variance in depression and insomnia and severity of COVID-19 infection appeared to contribute unique variance in depression and insomnia. The block of post-COVID impairments explained unique variance in depression and anxiety. The results are consistent with previous study reporting higher levels of mental health problems in individuals with post-COVID conditions compared with individuals who had developed COVID-19 without post-COVID conditions [43]. Looking at the importance of the separate variables within the set, impairments in mental functions appeared to contribute unique variance in depression and anxiety even we adjusted this variable to exclude depression, anxiety, stress, or sleep problems. It seems that impairments in mental functions such as impaired orientation, brain fatigue, concentration and attention difficulties, memory problem, and impaired organization and planning might be a risk factor for poor mental health outcomes. The block of fatigue variables, including general fatigue, physical fatigue, reduced activity reduced motivation, and mental fatigue, contributed unique variance in all three mental health outcomes. We further found that reduced motivation was interestingly the strongest predictors of risk for poor outcomes in depression, anxiety and insomnia. In other words, lower levels of motivation were associated with an increased risk of depression, anxiety, and insomnia symptoms. In the current study, motivation was assessed through four questions related to motivation dimension of the MFI-20 including “I feel like doing all sorts of nice things”, “I dread having to do things”, “I have a lot of plans”, and “I don’t feel like doing anything”. One possible explanation relies in that constancy in the face of difficulties as occurred during the COVID-19 pandemic is an important factor for lower wellbeing [78]. Life has been changed during the pandemic and a wide range of difficulties has been constantly experienced by many people such as financial difficulty, loneliness, fear of illness with COVID-19, loss of work, difficulties acquiring medication, difficulties accessing food, threats to personal safety, and difficulties in social functioning [9, 79, 80]. Therefore, reduced motivation could be a result of mental health issues or/and the pandemic period. Another possible explanation is that to stay motivated seems to play a key role for mental health outcomes in individuals infected with COVID-19. It has been nearly two years and a half since the COVID-19 pandemic started. People are tired to cope with pandemic and its consequences and demotivated to struggle with their post-COVID condition and improve their well-being beside the negative impacts on their life.
Conclusion
In conclusion, the current study outlines that individuals with a history of probable or confirmed SARS CoV-2 infection/infections are more likely to suffer from mental health problems. Therefore, policies are needed in order to promote and protect mental health in the individuals infected with COVID-19 especially those who still have experienced post-COVID impairments.
Implication
The identified factors that contribute to the level of mental health problems can be used for screening purposes in order to provide interventions for individuals infected with COVID-19 especially among those who still have experienced post-COVID condition. For example, the finding that reduced motivation was the strongest predictor of poor mental health suggests that staying motivated seems to be a core component in individuals infected with COVID-19 in order to manage their mental health. In the health care systems, the interventions targeting this group could use techniques like motivational interviewing in order to encourage patients to seek help, provide the initial motivation for treatment and increase likelihood of behavior changes [81,82,83,84].
Limitations and future directions
There are several important limitations in the current study. First, using the cross-sectional design in this study did not enable us to interpret the findings as implying causality. Longitudinal studies are needed to identify how mental health outcomes change over time and the causal factors of changes. Second, we conducted this study on a convenience sample, which limits the generalizability of findings. Further studies are warranted to examine the mental health using more representative samples. Third, we gathered self-report data in this study. Self-report biases and poor recall should therefore be considered when interpreting the findings. Fourth, lack of baseline data related to mental health before infection/ infections did not enable us to examine confidently the impacts of post-COVID impairments and fatigue on mental health outcome. Fifth, lack of a control group of non-COVID affected subjects did not enable us to assess the weight of COVID infection versus psychosocial factors of the pandemic on mental health outcomes. Further studies are warranted to study mental ill health by comparing COVID affected and non-COVID affected subjects. Finally, the findings that reduced motivation and impaired mental functions were the strong predictor of poor mental health outcomes in the current study raise the chicken-and-the-egg dilemma. Further studies are vital to address the bidirectional associations between motivation as well as cognitive functions and mental health outcomes in individuals infected with COVID-19 especially those with post-COVID conditions.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Arora T, Grey I, Östlundh L, Lam KB, Omar OM, Arnone D. The prevalence of psychological consequences of COVID-19: a systematic review and meta-analysis of observational studies. J Health Psychol. 2022;27(4):805–24. https://doi.org/10.1177/1359105320966639.
Lee Y, Lui LM, Chen-Li D, Liao Y, Mansur RB, Brietzke E, Rosenblat JD, Ho R, Rodrigues NB, Lipsitz O, Nasri F. Government response moderates the mental health impact of COVID-19: a systematic review and meta-analysis of depression outcomes across countries. J Affect Disord. 2021;290:364–77. https://doi.org/10.1016/j.jad.2021.04.050.
Nochaiwong S, Ruengorn C, Thavorn K, Hutton B, Awiphan R, Phosuya C, Ruanta Y, Wongpakaran N, Wongpakaran T. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: a systematic review and meta-analysis. Sci Rep. 2021;11(1):1–8. https://doi.org/10.1038/s41598-021-89700-8.
Prati G, Mancini AD. The psychological impact of COVID-19 pandemic lockdowns: a review and meta-analysis of longitudinal studies and natural experiments. Psychol Med. 2021;51(2):201–11. https://doi.org/10.1017/S0033291721000015.
Ren X, Huang W, Pan H, Huang T, Wang X, Ma Y. Mental health during the Covid-19 outbreak in China: a meta-analysis. Psychiatr Q. 2020;91(4):1033–45. https://doi.org/10.1007/s11126-020-09796-5.
Robinson E, Sutin AR, Daly M, Jones A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J Affect Disord. 2022;296:567–76. https://doi.org/10.1016/j.jad.2021.09.098.
Ahmed MZ, Ahmed O, Aibao Z, Hanbin S, Siyu L, Ahmad A. Epidemic of COVID-19 in China and associated psychological problems. Asian J Psychiatr. 2020;51:102092. https://doi.org/10.1016/j.ajp.2020.102092.
Mazza C, Ricci E, Biondi S, Colasanti M, Ferracuti S, Napoli C, Roma P. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: immediate psychological responses and associated factors. Int J Environ Res Public Health. 2020;17(9):3165. https://doi.org/10.3390/ijerph17093165.
Tull MT, Edmonds KA, Scamaldo KM, Richmond JR, Rose JP, Gratz KL. Psychological outcomes associated with stay-at-home orders and the perceived impact of COVID-19 on daily life. Psychiatry Res. 2020;289:113098. https://doi.org/10.1016/j.psychres.2020.113098.
Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, Ho RC. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. https://doi.org/10.3390/ijerph17051729.
Wu T, Jia X, Shi H, Niu J, Yin X, Xie J, Wang X. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. 2021;281:91–8. https://doi.org/10.1016/j.jad.2020.11.117.
McCracken LM, Badinlou F, Buhrman M, Brocki KC. Psychological impact of COVID-19 in the Swedish population: Depression, anxiety, and insomnia and their associations to risk and vulnerability factors. Eur Psychiatry. 2020;63(1). https://doi.org/10.1192/j.eurpsy.2020.8
Rondung E, Leiler A, Meurling J, Bjärtå A. Symptoms of depression and anxiety during the early phase of the COVID-19 pandemic in Sweden. Front public health. 2021:690. https://doi.org/10.3389/fpubh.2021.562437.
Senra H. Bidirectional associations and common inflammatory biomarkers in COVID-19 and mental health disorders: A window of opportunity for future research?. BBI - Health. 2021;13. https://doi.org/10.1016/j.bbih.2021.100237.
Taquet M, Harrison PJ. Why is COVID-19 associated with mental illness? Med. 2021;2(8):899–902. https://doi.org/10.1016/j.medj.2021.06.009.
Taquet M, Luciano S, Geddes JR, Harrison PJ. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry. 2021;8(2):130–40. https://doi.org/10.1016/S2215-0366(20)30462-4.
Lee SW, Yang JM, Moon SY, Yoo IK, Ha EK, Kim SY, Park UM, Choi S, Lee SH, Ahn YM, Kim JM. Association between mental illness and COVID-19 susceptibility and clinical outcomes in South Korea: a nationwide cohort study. Lancet Psychiatry. 2020;7(12):1025–31. https://doi.org/10.1016/S2215-0366(20)30421-1.
Maripuu M, Bendix M, Öhlund L, Widerström M, Werneke U. Death associated with coronavirus (COVID-19) infection in individuals with severe mental disorders in Sweden during the early months of the outbreak—an exploratory cross-sectional analysis of a population-based register study. Front Psychiatry. 2021;11:609579. https://doi.org/10.3389/fpsyt.2020.609579.
Nemani K, Li C, Olfson M, Blessing EM, Razavian N, Chen J, Petkova E, Goff DC. Association of psychiatric disorders with mortality among patients with COVID-19. JAMA Psychiat. 2021;78(4):380–6. https://doi.org/10.1001/jamapsychiatry.2020.4442.
Sisó-Almirall A, Kostov B, Mas-Heredia M, Vilanova-Rotllan S, Sequeira-Aymar E, Sans-Corrales M, Sant-Arderiu E, Cayuelas-Redondo L, Martínez-Pérez A, Garcia-Plana N, Anguita-Guimet A. Prognostic factors in Spanish COVID-19 patients: a case series from Barcelona. PLoS ONE. 2020;15(8):e0237960. https://doi.org/10.1371/journal.pone.0237960.
Wang QQ, Kaelber DC, Xu R, Volkow ND. COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol Psychiatry;26(1):30–9. https://doi.org/10.1038/s41380-020-00880-7.
Ma YF, Li W, Deng HB, Wang L, Wang Y, Wang PH, Bo HX, Cao J, Wang Y, Zhu LY, Yang Y. Prevalence of depression and its association with quality of life in clinically stable patients with COVID-19. J Affect Disord. 2020;275:145–8. https://doi.org/10.1016/j.jad.2020.06.033.
Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, Melloni EM, Furlan R, Ciceri F, Rovere-Querini P, Benedetti F. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. BBI - Health. 2020;89:594–600. https://doi.org/10.1016/j.bbi.2020.07.037.
Xie Q, Liu XB, Xu YM, Zhong BL. Understanding the psychiatric symptoms of COVID-19: a meta-analysis of studies assessing psychiatric symptoms in Chinese patients with and survivors of COVID-19 and SARS by using the Symptom Checklist-90-Revised. Transl Psychiatry. 2021;11(1):1. https://doi.org/10.1038/s41398-021-01416-5.
Yuan K, Zheng YB, Wang YJ, Sun YK, Gong YM, Huang YT, Chen X, Liu XX, Zhong Y, Su SZ, Gao N. A systematic review and meta-analysis on prevalence of and risk factors associated with depression, anxiety and insomnia in infectious diseases, including COVID-19: a call to action. Mol Psychiatry. 2022:1–9. https://doi.org/10.1038/s41380-022-01638-z.
Zarghami A, Farjam M, Fakhraei B, Hashemzadeh K, Yazdanpanah MH. A report of the telepsychiatric evaluation of SARS-CoV-2 patients. TELEMED E-HEALTH. 2020;26(12):1461–5. https://doi.org/10.1089/tmj.2020.0125.
Alwan NA, Johnson L. Defining long COVID: Going back to the start. Med. 2021;2(5):501–4. https://doi.org/10.1016/j.medj.2021.03.003.
Fernández-de-Las-Peñas C, Palacios-Ceña D, Gómez-Mayordomo V, Florencio LL, Cuadrado ML, Plaza-Manzano G, Navarro-Santana M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur J Intern Med. 2021;92:55–70. https://doi.org/10.1016/j.ejim.2021.06.009.
Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV, Group WC. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 2021. https://doi.org/10.1016/S1473-3099(21)00703-9
Ceban F, Ling S, Lui LM, Lee Y, Gill H, Teopiz KM, Rodrigues NB, Subramaniapillai M, Di Vincenzo JD, Cao B, Lin K. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: a systematic review and meta-analysis. Brain Behav Immun. 2022;101:93–135. https://doi.org/10.1016/j.bbi.2021.12.020.
Han Q, Zheng B, Daines L, Sheikh A. Long-Term sequelae of COVID-19: A systematic review and meta-analysis of one-year follow-up studies on post-COVID symptoms. Pathogens. 2022;11(2):269. https://doi.org/10.3390/pathogens11020269.
Lopez-Leon S, Wegman-Ostrosky T, Perelman C, Sepulveda R, Rebolledo PA, Cuapio A, Villapol S. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Sci Rep. 2021;11(1):1–2. https://doi.org/10.1038/s41598-021-95565-8.
Michelen M, Manoharan L, Elkheir N, Cheng V, Dagens A, Hastie C, O’Hara M, Suett J, Dahmash D, Bugaeva P, Rigby I. Characterising long COVID: a living systematic review. BMJ Glob Health. 2021;6(9):e005427. https://doi.org/10.1136/bmjgh-2021-005427.
Schou TM, Joca S, Wegener G, Bay-Richter C. Psychiatric and neuropsychiatric sequelae of COVID-19–a systematic review. Brain Behav Immun. 2021;97:328–48. https://doi.org/10.1016/j.bbi.2021.07.018.
Whitaker M, Elliott J, Chadeau-Hyam M, Riley S, Darzi A, Cooke G, Ward H, Elliott P. Persistent symptoms following SARS-CoV-2 infection in a random community sample of 508,707 people. Medrxiv. 2021. https://doi.org/10.1101/2021.06.28.21259452.
Norrefalk JR, Kristian BO, Bileviciute-Ljungar I. Self-scored impairments in functioning and disability in post-COVID syndrome following mild COVID-19 infection. J Rehabil Med. 2021;53(11). https://doi.org/10.2340/jrm.v53.188.
Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, Mukherjee B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J Infect Dis. 2022. https://doi.org/10.1093/infdis/jiac136.
Badinlou F, Forsström D, Jansson-Fröjmark M, Abzhandadze T, Lundgren T. Impairments following COVID-19 infection: Manifestations and investigations of related factors. Manuscript submitted for publication. 2022.
El Sayed S, Shokry D, Gomaa SM. Post-COVID-19 fatigue and anhedonia: a cross-sectional study and their correlation to post-recovery period. Neuropsychopharmacol Rep. 2021;41(1):50–5. https://doi.org/10.1002/npr2.12154.
Logue JK, Franko NM, McCulloch DJ, McDonald D, Magedson A, Wolf CR, Chu HY. Sequelae in adults at 6 months after COVID-19 infection. JAMA Netw Open. 2021;4(2):e210830. https://doi.org/10.1001/jamanetworkopen.2021.0830.
Sudre CH, Murray B, Varsavsky T, Graham MS, Penfold RS, Bowyer RC, Pujol JC, Klaser K, Antonelli M, Canas LS, Molteni E. Attributes and predictors of long COVID. Nat Med. 2021;27(4):626–31. https://doi.org/10.1038/s41591-021-01292-y.
Sykes DL, Holdsworth L, Jawad N, Gunasekera P, Morice AH, Crooks MG. Post-COVID-19 symptom burden: what is long-COVID and how should we manage it? Lung. 2021;199(2):113–9. https://doi.org/10.1007/s00408-021-00423-z.
Matsumoto K, Hamatani S, Shimizu E, Käll A, Andersson G. Impact of post-COVID conditions on mental health: a cross-sectional study in Japan and Sweden. BMC Psychiatry. 2022;22(1):1–3. https://doi.org/10.1186/s12888-022-03874-7.
Brocki KC, Buhrman M, Badinlou F, McCracke LM. The Context of COVID-19 at 18 Months: Depression, Anxiety, Insomnia, and “Long COVID”. Manuscript submitted for publication. 2022.
The Swedish National Board of Health and Welfare (Socialstyrelsen). Statistics on COVID-19. 2022. https://www.socialstyrelsen.se/en/statistics-and-data/statistics/statistics-on-covid-19. Accessed July 2022.
Public Health Agency of Sweden (Folkhälsomyndigheten). COVID-19. Available: https://www.folkhalsomyndigheten.se/the-public-health-agency-of-sweden/communicable-disease-control/covid-19/.2021. Accessed October 2021.
World Health Organization (WHO). Coronavirus disease (COVID-19). https://www.who.int/health-topics/coronavirus#tab=tab_3. 2021. Accessed October 2021.
Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, Cook JR, Nordvig AS, Shalev D, Sehrawat TS, Ahluwalia N. Post-acute COVID-19 syndrome. Nat Med. 2021;27(4):601–15. https://doi.org/10.1038/s41591-021-01283-z.
Tran VT, Riveros C, Clepier B, Desvarieux M, Collet C, Yordanov Y, Ravaud P. Development and validation of the long covid symptom and impact tools, a set of patient-reported instruments constructed from patients’ lived experience. medRxiv. 2021. https://doi.org/10.1101/2021.03.18.21253903.
Alkodaymi MS, Omrani OA, Fawzy NA, Abou Shaar B, Almamlouk R, Riaz M, Obeidat M, Obeidat Y, Gerberi D, Taha RM, Kashour Z. Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: A systematic review and meta-analysis. Clin Microbiol Infect. 2022. https://doi.org/10.1016/j.cmi.2022.01.014.
Maglietta G, Diodati F, Puntoni M, Lazzarelli S, Marcomini B, Patrizi L, Caminiti C. Prognostic factors for post-COVID-19 syndrome: a systematic review and meta-analysis. J Clin Med. 2022;11(6):1541. https://doi.org/10.3390/jcm11061541.
World Health Organization (WHO). The International Classification of Functioning, Disability and Health (ICF). 2001. Available from: https://www.who.int/classifications/international-classification-of-functioningdisability-and-health. Accessed January 2022.
McNeish D, Wolf MG. Thinking twice about sum scores. Behav Res Methods. 2020;52(6):2287–305. https://doi.org/10.3758/s13428-020-01398-0.
Smets EM, Garssen B, Bonke BD, De Haes JC. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. 1995;39(3):315–25. https://doi.org/10.1016/0022-3999(94)00125-O.
Schwarz R, Krauss O, Hinz A. Fatigue in the general population. Oncol Res Treat. 2003;26(2):140–4. https://doi.org/10.1159/000069834.
Tian J, Hong JS. Application of the Chinese version of the MFI-20 in detecting the severe fatigue in cancer patients. Support Care Cancer. 2013;21(8):2217–23. https://doi.org/10.1007/s00520-013-1783-x.
Ericsson A, Mannerkorpi K. Assessment of fatigue in patients with fibromyalgia and chronic widespread pain. Reliability and validity of the Swedish version of the MFI-20. Disabil. 2007;29(22):1665–70. https://doi.org/10.1080/09638280601055782.
Lundh Hagelin C, Wengström Y, Runesdotter S, Johan FC. The psychometric properties of the Swedish Multidimensional Fatigue Inventory MFI-20 in four different populations. Acta Oncol. 2007;46(1):97–104. https://doi.org/10.1080/02841860601009430.
Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. 2002;32(9):509–15. https://doi.org/10.3928/0048-5713-20020901-06.
Titov N, Dear BF, McMillan D, Anderson T, Zou J, Sunderland M. Psychometric comparison of the PHQ-9 and BDI-II for measuring response during treatment of depression. Cogn Behav Therapy. 2011;40(2):126–36. https://doi.org/10.1080/16506073.2010.550059.
Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–7. https://doi.org/10.1001/archinte.166.10.1092.
Rutter, LA, Brown, TA. Psychometric properties of the Generalized Anxiety Disorder Scale-7 (GAD-7) in outpatients with anxiety and mood disorders. J Psychopathol Behav Assess. 2017;39:140–6. https://doi.org/10.1007/s10862-016-9571-9.
Beard, C, Björgvinsson, T. Beyond generalized anxiety disorder: psychometric properties of the GAD-7 in a heterogeneous psychiatric sample. J Anxiety Disord. 2014;28:547–52. https://doi.org/10.1016/j.janxdis.2014.06.002.
Löwe, B, Spitzer, RL, Williams, JB, Mussell, M, Schellberg, D, Kroenke, K. Depression, anxiety and somatization in primary care: syndrome overlap and functional impairment. Gen Hosp Psychiatry. 2008;30:191–9. https://doi.org/10.1016/j.genhosppsych.2008.01.001.
Bastien, CH, Vallieres, A, Morin, CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2:297–307. https://doi.org/10.1016/S1389-9457(00)00065-4.
Morin, CM, Belleville, G, Belanger, L, Ivers, H. The insomnia severity index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34:601–8. https://doi.org/10.1093/sleep/34.5.601.
Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81. https://doi.org/10.1016/j.jbi.2008.08.010.
Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. https://doi.org/10.1016/j.jbi.2019.103208.
IBM. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM; 2019.
Bo HX, Li W, Yang Y, Wang Y, Zhang Q, Cheung T, Wu X, Xiang YT. Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol Med. 2021;51(6):1052–3. https://doi.org/10.1017/S0033291720000999.
Raman B, Cassar MP, Tunnicliffe EM, Filippini N, Griffanti L, Alfaro-Almagro F, Okell T, Sheerin F, Xie C, Mahmod M, Mózes FE. Medium-term effects of SARS-CoV-2 infection on multiple vital organs, exercise capacity, cognition, quality of life and mental health, post-hospital discharge. EClinicalMedicine. 2021;31:100683. https://doi.org/10.1016/j.eclinm.2020.100683.
Daré LO, Bruand PE, Gérard D, Marin B, Lameyre V, Boumédiène F, Preux PM. Co-morbidities of mental disorders and chronic physical diseases in developing and emerging countries: a meta-analysis. BMC Public Health. 2019;19(1):1–2. https://doi.org/10.1186/s12889-019-6623-6.
Doherty AM, Gaughran F. The interface of physical and mental health. Soc Psychiatry Psychiatr Epidemiol. 2014;49(5):673–82. https://doi.org/10.1007/s00127-014-0847-7.
Tang NK, Wright KJ, Salkovskis PM. Prevalence and correlates of clinical insomnia co-occurring with chronic back pain. J Sleep Res. 2007;16(1):85–95. https://doi.org/10.1111/j.1365-2869.2007.00571.x.
Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, Kang L, Guo L, Liu M, Zhou X, Luo J. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220–32. https://doi.org/10.1016/S0140-6736(20)32656-8.
Centers for Disease Control and Prevention (CDC). Long COVID or Post-COVID Conditions. 2022. https:// www. cdc. gov/ coron avirus/ 2019- ncov/ long- term- effec ts/ index.html? CDC_ AA_ refVal= https% 3A% 2F% 2Fwww. cdc. gov% 2Fcor onavi rus%2F2019- ncov% 2Flong- term- effec ts. Html. Accessed July 2022.
Bellan M, Soddu D, Balbo PE, Baricich A, Zeppegno P, Avanzi GC, Baldon G, Bartolomei G, Battaglia M, Battistini S, Binda V. Respiratory and psychophysical sequelae among patients with COVID-19 four months after hospital discharge. JAMA Netw Open. 2021;4(1):e2036142-. https://doi.org/10.1001/jamanetworkopen.2020.36142.
O’Connor RC, Wetherall K, Cleare S, McClelland H, Melson AJ, Niedzwiedz CL, O’Carroll RE, O’Connor DB, Platt S, Scowcroft E, Watson B. Mental health and well-being during the COVID-19 pandemic: longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. BJPsych. 2021;218(6):326–33. https://doi.org/10.1192/bjp.2020.212.
Rogers JP, Chesney E, Oliver D, Pollak TA, McGuire P, Fusar-Poli P, Zandi MS, Lewis G, David AS. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. 2020;7(7):611–27. https://doi.org/10.1016/S2215-0366(20)30203-0.
Wright L, Steptoe A, Fancourt D. Does thinking make it so? Differential associations between adversity worries and experiences and mental health during the COVID-19 pandemic. J Epidemiol Community Health. 2021;75(9):817–23. https://doi.org/10.1136/jech-2020-215598.
Matthews EE, Schmiege SJ, Cook PF, Berger AM, Aloia MS. Adherence to cognitive behavioral therapy for insomnia (CBTI) among women following primary breast cancer treatment: a pilot study. Behav Sleep Med. 2012;10(3):217–29. https://doi.org/10.1080/15402002.2012.666220.
Meyer E, Shavitt RG, Leukefeld C, Heldt E, Souza FP, Knapp P, Cordioli AV. Adding motivational interviewing and thought mapping to cognitive-behavioral group therapy: results from a randomized clinical trial. Braz J Psychiatry. 2010;32:20–9. https://doi.org/10.1590/S1516-44462010000100006.
Rollnick S, Miller WR, Butler CC. Motivational interviewing in health care: helping patients change behavior. New York: Guilford press; 2008.
Westra HA, Arkowitz H, Dozois DJ. Adding a motivational interviewing pretreatment to cognitive behavioral therapy for generalized anxiety disorder: a preliminary randomized controlled trial. J Anxiety Disord. 2009;23(8):1106–17. https://doi.org/10.1016/j.janxdis.2009.07.014.
Acknowledgements
We would like to thank all participants that took part in this study.
Funding
Open access funding provided by Karolinska Institute. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conceptualization, F.B, T.L, and M.J.F.; data curation, F.B.; formal analysis, F.B.; methodology, F.B, T.L, and M.J.F.; investigation, F.B, T.L, and M.J.F.; project administration, F.B.; writing – original draft, F.B.; writing – review & editing, F.B, T.L, and M.J.F. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The study was approved by the Swedish national ethical board (dnr 2021–06617-01) and informed consent was obtained from all participants. All procedures utilized in collecting data for the current paper follow the ethical standards of the Helsinki Declaration of 1964 and subsequent amendments.
Consent for publication
Not applicable.
Competing interests
The authors report no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Badinlou, F., Lundgren, T. & Jansson-Fröjmark, M. Mental health outcomes following COVID-19 infection: impacts of post-COVID impairments and fatigue on depression, anxiety, and insomnia — a web survey in Sweden. BMC Psychiatry 22, 743 (2022). https://doi.org/10.1186/s12888-022-04405-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-022-04405-0