
Abstract
Background
Diarrhea caused by Salmonella and Shigella species are the leading cause of illness especially in developing countries. These infections are considered as the main public health problems in children, including Ethiopia. This study aimed to assess the prevalence, associated factors, and antimicrobial susceptibility patterns of Salmonella and Shigella species in Sheik Hassan Yabere Referral Hospital Jigjiga, Eastern Ethiopia from August 05 to November 15, 2022.
Method
A cross-sectional study was conducted among 239 under-five children with diarrhea selected through a convenient sampling technique. A structured questionnaire was used to collect associated factors. A stool sample was collected and processed for the identification of Salmonella and Shigella species using MacConkey adar, Xylose Lysine Deoxycholate agar (Oxoid Ltd) and Biochemical tests. The antimicrobial susceptibility pattern of isolates was performed using the Kirby-Bauer disc diffusion technique. The data was entered into Epi-data version 4.6 and exported to the statistical package of social science version 22 for analysis. The association between outcome and independent variables was assessed using bivariate, multivariable, and chi-square and P-value < 0.05 was considered as statistical significance.
Result
Overall prevalence of Salmonella and Shigella species was 6.3% (95% CI, 5.7–6.9%), of which 3.8% (95 CI, 3.2–4.4%) were Salmonella species and 2.5% (95% CI, 1.95-3%) were Shigella species. Unimproved water source (AOR = 5.08, 95% CI = 1.45, 17.25), open field (AOR = 2.3, 95% CI = 1.3, 5.03), rural residence (AOR = 1.8, 95% CI = 1.4, 7.5), Hand-washing practice (p = 0.001), and raw meat consumption (p = 0.002) were associated with occurrence of Salmonella and Shigella species. Salmonella and Shigella isolates were resistant to Ampicilin (100%). However, Salmonella isolates was sensitive to Norfloxacin (100%). About 22.2% and 16.7% of Salmonella and Shigella isolates were multi-drug resistant, respectively.
Conclusion
Prevalence of Salmonella and Shigella species were lower than most studies done in Ethiopia. Hand-washing habit, water source type, Open field waste disposal habit, raw meat consumption and rural residence were associated with Salmonellosis and shigellosis. All isolated Salmonella were sensitive to norfloxacin. The evidence from this study underscores the need for improved water, sanitation and hygiene (WASH) system and the imperative to implement drug susceptibility tests for the treatment of Salmonella and Shigella infection.
Similar content being viewed by others

Introduction
Diarrheal diseases are common public health problems in many parts of the world including Ethiopia. Globally 21% of deaths in children under the age of 5 years results from diarrheal infection mortality, which translates to 2.5 million child deaths. Africa and South Asia are still home to more than 80% of child deaths [1], making diarrhea the second leading cause of death among children under the age of five [2]. Salmonella and Shigella are the major cause of childhood diarrhea associated with a high burden of illness n in the developing world where there is poor sanitation and limited improved health care services [3].
In Ethiopia, Diarrheal diseases are the cornerstone in contribution of child mortality; the total prevalence of diarrhea among under five children was (12%) according to the report of Ethiopian demographic Health survey [4], Particularly by Salmonella and Shigella species, accounting for approximately 8% of all deaths among children under age 5 worldwide [5].
Antibiotic resistance is becoming a significant health problem and leads to a serious threat in public health worldwide. Particularly, Multi-drug resistance pathogen is nowadays increasing which in turn, leads to variety of challenges toward diarrheal disease treatment and control globally [6].
There is no published data on the prevalence, antimicrobial susceptibility and associated factors of Shigella and Salmonella spp among under-five children in the study area. Therefore, the current study was conducted to determine the prevalence, associated factors and antimicrobial susceptibility patterns of Salmonella and Shigella species among diarrheic under-five children in Sultan Sheik Hassan Yabere Referral Hospital, Jigjiga, Eastern Ethiopia.
Materials and methods
Study area and period
The study was conducted in Jigjiga town at Jigjiga University Sultan Sheik Hassan Yabere Referral Hospital from 05 August to 15 November 2022. Jigjiga town is the capital city of the Somali regional state, 630Km away from Addis-Ababa. Based on the 2007 Census conducted by the Central Statistical Agency of Ethiopia, this city has a total population of 277,560, of whom 149,292 are men and 128,268 women [7]. Jigjiga city has three governmental hospitals where two of them are general hospitals and one of them is specialized referral hospital. Jigjiga University Sheik Hassan Yabare referral hospital is comprehensive specialized referral [8].
Study design and population
An institutional based cross-sectional study design was used. All under-five children visited Sheik Hassan Yabere Referral Hospital during the study period were source population. All under-five children with diarrhea disease symptoms attended Sheik Hassan Yabere Referral Hospital during study period were the study population. All under-five children passing loose or watery diarrhea three or more times a day who attend the hospital during the study period were included. Children those who were critically ill and unable to give stool sample and those that were on antibiotic treatment with in the last two weeks were excluded.
Sample size determination and sampling techniques
The sample size was calculated using a single population proportion formula based on the assumption of 5% expected margins of error, considering 95% confidence interval, 10% non-response rate and by taking the prevalence of 17% of Shigella spp from previous study conducted in Arbaminch, southern Ethiopia [9]. The final total study subjects of this study were 239. Eligible study participants (children attending under five outpatients) were enrolled sequentially using convenient sampling technique.
Data and sample collection methods
The data were collected by two professional nurses and two trained medical laboratory professionals. Data on Socio-demographic, socio-economic characteristics, environmental factors and behavioral factors were collected by interview guided pretested structured questionnaire adopted from previous studies [10, 11]. The guardians were instructed to bring a freshly passed diarrhea stool of the study subjects in a sterile stool cup using clean applicator stick and to avoid contamination with urine and other materials. One teaspoonful of diarrhea stool sample was collected using a pre-labeled, clean and sterile screw cup container. The collected diarrhea stool was placed immediately in Cary Blair transport (Oxoid, UK) and transported to Jigjiga University Sultan Sheik Hassan referral hospital microbiology laboratory within 2 h of collection for investigation.
Bacteriological analysis
Prior to subjecting the sample to culture media, physical analysis of the stool sample was performed in order to check whether the sample was diarrheal or not, presence of blood, pus and mucus. Children with diarrhea, blood, mucus were included. Diarrhea stool specimen was inoculated using sterile wire loop on MacConkey Agar (Oxoid, Ltd), and Xylose lysine- Deoxycholate agar (XLD) (Oxoid Ltd). The inoculated plates ware incubated at 37 °C for 24 h (SOPs) [12]. After 24 h incubation, the plates were checked for colony characteristics of Salmonella and Shigella species. Furthermore, colorless to yellow colonies on MacConkey agar and pink to red colonies Xylose Lysine Deoxycholate (XLD) (Oxoid Ltd) [12] agar were typically considered as Non-lactose fomenters. In addition, the colonies considered as non-lactose fomenters were further identified by biochemical tests to confirm the identification to genus level of the pathogens Biochemical tests such as klingler iron agar (KIA), motility indole, lysine medium, simon’s citrate agar, and unease test were used [13].
Antimicrobial susceptibility testing
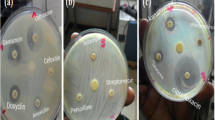
The drug susceptibility test was done by a disk diffusion method by using Muller Hinton Agar (MHA) according the guidelines of the Clinical Laboratory Standard Institute [14]. Colony suspension was made using normal saline (0.85% NaCl) equivalent to 0.5% McFarland standard from grown overnight colonies [15]. A sterile cotton swab was dipped into the suspension in order to remove additional suspensions by gentle rotation of the swab against the surface of the tube and then spread evenly over the Muller Hinton agar (Oxoid, Ltd). The drugs were selected in accordance with the Ethiopian Drug Administration standard treatment guidelines and Control Authority’s and the Clinical Laboratory Standards Institute’s (CLSI). Based on the drugs those professionals use to treat bacteria diarrheal disease, each and every single of the isolates were tested for ampicilin (10 µg), tetracycline (30 µg), chloramphenicol (10 µg), norfloxacin, (5 µg), ciprofloxacin (5 µg), and ceftriaxone (30 µg) on the Muller Hinton agar, the plate were then incubated at 37oC for 18 h and interpreted according Clinical Laboratory Standard Institute [14]. Finally, the diameter of the zone of inhibition was measured and interpreted as sensitive, intermediate, and resistant based on the Clinical and Laboratory Standards Institute [14].
Data quality control
Questionnaires was primarily written in English, translated to Somali and returned back to English to keep uniformity. Manufacturer instructions were followed during culture media preparation and sterilization. Sterility of culture media was checked by incubating 5% of each batch at 37oC overnight and observed for growth. Culture media which show any growth were discarded and replaced by new batch. In addition, Quality control strains of the American Type Culture Collection (ATCC) like Escherichia coli ATCC 25,922, Shigella dysentery ATCC 13,313 and Salmonella typhi ATCC 13,311 [16] were used to check the performance of culture media, biochemical tests and antimicrobial susceptibility testing.
Method of data analysis
The laboratory analysis result was registered on the laboratory data collection pre-coded format sheet. Data were entered to Epi-data version 4.6 and was analyzed using SPSS version 22. Descriptive statistics and frequency table were used to summarize the data. Chi-square, bivariate and multi-variable analysis were used to predict the association between the dependent and independent variables. Variables with p-value ≤ 0.25 on bivariate logistic regression analysis were selected for multi-variable analysis. Adjusted odds ratio (AOR) with 95% confidence interval (CI) was used to measure the strength of the association. A P-value ≤ 0.05 was considered statistical significance.
Operational definitions
Diarrhea
is the passage of three or more loose or liquid stools per day [17].
Multi Drug Resistant (MDR) is a antimicrobial resistance shown by microorganism to at least one antimicrobial drug in three or more antimicrobial categories [18].
Improved drinking water is a source that, by the nature of construction, adequately protects from outside contamination, include piped water into a dwelling, yard of plot, public tap or standpipe, tube-well or borehole, protected spring, protected dug well, and rainwater collection [19].
Unimproved sources of drinking water include unprotected well (dug); unprotected spring, cart with small tank or drum; tanker truck-provided water, surface water [19].
Results
Socio-demographic characteristics, behavioral and environmental characteristics
A total of 239 patients with diarrhea were included in this study, with a response rate of 100%. About half 121/239 (50.6%) of the children were male. The mean age (± SD) of the study participants was 2.1(± 0.8) years with the age of range of 0–5 years. Most (83.7%) of the study participants were from urban area and 72.4% of the parents/guardians were illiterate in educational status (Table 1).
Majority (73.2%) of the study participants wash their hands after toilet usage. About 70.7% of the study participants utilized improved water sources and 71.5% of the parents /care givers used waste bin for waste disposal (Table 2).
Prevalence of Salmonella and Shigella spp
The overall prevalence of isolated Salmonella and Shigella species were 6.3% (15/239) (95% CI; 5.7-6.9%). Among them, more than half of the cases (3.8%, 95%CI; 3.2–4.4%) individuals were Salmonella spp. whereas, the remaining cases (2.5%, 95% CI; 1.95-3%)) patients were Shigella spp. The magnitude of Salmonella and Shigella spp were higher in parents/guardians had no hand washing practice (18.8%) followed by parents with raw meat consumption (14.3%) and used unimproved water sources (14.3%) (Table 3).
Factors associated with Salmonella and Shigella infection
Association between some of the potential factors and prevalence of bacterial diarrhea were assessed using logistic regression analysis. In bivariate logistic regression analysis; sex, residence, water source and waste disposal system were found to be significant (p < 0.25) and were considered as a candidate for multivariable logistic regression analysis. In multivariable, logistic regression analysis, water source, waste disposal system and residence found to be statistically significant with positivity rate of Salmonella and Shigella isolates at p < 0.05.
Water sources type (AOR = 5.08, 95% CI = 1.497–17.251), Open field waste disposal habit (AOR = 2.3, 95% CI = 1.3, 5.03), rural residence (AOR = 1.8, 95% CI = 1.4, 7.5) were associated with Salmonella and Shigella infections (Table 3). Moreover, variables those did not fulfill the assumption of logistic regression analysis were assessed chi-square test such hand-washing habit, raw meat conception and educational status. In chi-square test hand-washing habit and raw meat consumption were found to be statistically significant. Children from parents/guards who had not habit of washing their hands were (p = 0.001) more likely to be infected with Salmonella spp and Shigella spp compared with children from parents/guards who had habit of hand washing. Children who were eating raw meat were (p = 0.002) more likely to be infected with Salmonella spp and Shigella spp compared to these who don’t eat (Table 4).
Antimicrobial susceptibility patterns and multi-drug resistant pattern
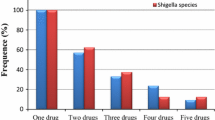
To determine antimicrobial susceptibility patterns of isolates, those 15 bacterial isolates were tested for six different antimicrobial discs. All Salmonella isolates were sensitive to norfloxacin. On the other hand, all Salmonella and Shigella isolates showed (100%) resistance rate to ampicillin. In addition, majority Shigella spp. isolates were resistant to tetracycline (83.3%). Moreover, one-third of Salmonella and Shigella spp. isolates were found to be resistant to ciprofloxacin (Table 5). Furthermore, Two of the nine Salmonella isolates, and one of the six Shigella isolates were multi-drug resistant to ampicillin, tetracycline and Chloramphenicol.
Discussion
Salmonella and Shigella are common diarrheagenic bacterial pathogens in the worldwide. Both are more predominant in under-five children [20]. This study was determining the prevalence and factors associated with Salmonella and Shigella spp in diarrheic under-five children. In this study the prevalence of Salmonella and Shigella spp were (6.3%). And hand-washing habit, raw meat consumption, residence, waste disposal and water source were remained statistically significant at (p < 0.05) with diarrhea caused by Salmonella and Shigella spp.
In this study, the overall prevalence of Salmonella and Shigella spp were 6.3%. It is similar with study done in Jimma, Ethiopia (6.2%) [21], but it is lower than studies done in Arbaminch (17.45%) [9], and Nekemte Referral Hospital Oromia, Ethiopia (9.2%) [10]. However, the prevalence was higher than that reported in Ambo town, Ethiopia (3.86%) [11]. The discrepancy might be due to a difference in the study time and illness due to other enteric pathogens. And Younger age is highly infected with bacterial diarrheal disease [22].
In the current study, the prevalence of Salmonella isolates was 3.8%, which is comparable with studies done in Kenya (3.5%) [23], and Addis Ababa (3.95%), Ethiopia [24]. In contrast our result is higher than the studies conducted in Turkey (1.5%) [25], Nepal (1%) [26], Windhoek, Namibia (2.6%) [27], Hawassa, Southern Ethiopia (2.5%) [28]. However, this finding is lower than studies done in Harar (6.7%) [29], and Dessie (5.2%) Ethiopia [30]. The variation may be due to the difference in the socio-economic status, source of drinking water supply and sanitation. And also, the difference might be due to the divergence of enteric bacterial pathogens since they vary globally from region to region [27].
In the present study, Shigella isolates was 2.5% (95% CI, 1.95-3%). This is agreement with studies done in Kenya (2%) [23], and Jimma, Southern Ethiopia (2.5%) [31]. However, our finding is lower than studies done in Nepal (4.6%) [26], Tehran (7%) [32], studies done in Ethiopia; Mekelle, Ethiopia (6.9%) [33], Nigist Eleni Mohammed (8.3%) [34], Addis Ababa (9.1%) [24], Bahirdar (9.5%) [35], Butajira (4.5%) [36], Robe General Hospital (4.3%) [37], Hawassa town (7%) [28], and Harar (11.5%) [29]. The variation could be due to deference in personal hygiene and environmental sanitation and even between and within countries in an identical geographical region.
Hand-washing practice after toilet by parent/guardians was less likely to be infected with the isolates of Salmonella and Shigella spp. This is in agreement with studies conducted in Igembe district Hospital, Kenya [38], Robe Ethiopia [37], Arbaminch, Ethiopia (2.0, 18.2)] [9]. This could be due to the fact that hand washing is important in reducing occurrence of diarrhea when supported with the availability of water and hand washing facility [39].
In this study, water source was significantly associated with the isolates of Salmonella and Shigella spp with those who used unimproved drinking water had more likely contracting Salmonellosis and Shigellosis than those who used improved water. This is agreement with study conducted in Dessie, Ethiopia [30], Robe, Ethiopia [37]. It was indicated that the consumption of contaminated food and/ or water is responsible for diarrheal diseases caused by Salmonella and Shigella isolates [37].
Waste disposal system was significantly associated with the isolates of Salmonella and Shigella spp with children who live environment with open field disposal system were more likely to be infected by Salmonella spp and Shigella spp than children from waste and disposed environment. This is compared with the study conducted in Arbaminch, southern Ethiopia [9]. Many disease caused by agents responsible in appropriate waste disposal system have been well characterized [40].
In the current study, consumption of raw meat was significantly associated with the isolates of Salmonella and Shigella species with those did not eat are less likely contracting by Salmonellosis and Shigellosis than those ate raw meat this is supported with the study done in Gondar, Ethiopia [41], Addis Ababa, Ethiopia [24]. This is supported that raw meat consumption is predictors of diarrheal diseases [42].
In this study, children who were from rural residents were more likely to be infected Salmonella and Shigella species when compared with those from urban area. This is constant with study done in Harar, Eastern Ethiopia [43]. Because the majority of study participants were being from rural settings, and host fecal flora might be the source of the infection [43].
In this study, Shigella isolates was sensitive to norfloxacin (100%). This finding is concordant with the previous study done in Mohamed Memorial Hospital, South Ethiopia (100%) [34] that showed the susceptibility to norfloxacin (100%). However, in this study Shigella isolates was resistant to ampicillin (100%), and tetracycline (83.3%). This result is in agreement with study done in, Addis Ababa, Ethiopia (95.7%) [24], and Ambo, Ethiopia (83.5%) [11]. However, the finding of this study report revealed that a relatively low rate of ampicillin-resistant Shigella species was isolated compared to the findings reported from Hawassa (63.6%) [28].This difference might be due to miss use of antimicrobial agents without confirmation of etiologic agent.
In this study, Salmonella isolates were sensitive to norfloxacin (100%) and ceftriaxone (77.8%). This result is in line with the studies done in Nigist Eleni Mohamed Memorial Hospital, South Ethiopia indicated sensitivity to norfloxacin (100%) [34] and ceftriaxone (77.9%) in Alamura Health center Southern Ethiopia [44]. But in the current study the bacteria was resistant to ampicillin (100%) that is similar with study conducted in Nigist Eleni Mohamed Memorial Hospital, Ethiopia ampicillin (100%) [34]. However, it is slightly different with the studies performed in Addis Ababa, Ethiopia (80%) [24]. The main reason might be frequent use of these antibiotics, different strains and variation in the number of isolates.
The overall prevalence of multi-drug resistance (MDR) among the isolates was 20% which is comparable with study done in rural Mozambique (23%) [45]. But it is lower than studies done in Butajira (47.1%) [36]. Variation might be different in prescription practice among health care providers and different in usage of drugs by the patients.
Limitations of this study
The current study did not identify bacteria species level due to the lack of anti-sera in the local market. The current study did not identify other cause of diarrhea like virus. In addition, the association between types of diarrhea and educational status of the children with isolated pathogens has not been analyzed.
Conclusion
The prevalence of Salmonella and Shigella spp was lower compared with other studies reported in Ethiopia. Under-five children from parents/guardians with poor habit of hand washing practice after toilet, drink water from unimproved sources, consumption of raw meat, and those did not use waste bin and disposed were more likely to be infected with the isolates of Salmonella and Shigella. All Salmonella and Shigella spp isolates were sensitive to norfloxacin. This study also revealed that ciprofloxacin can be used as the drug of choice against Shigella and Salmonella species. Health care workers and stakeholders should focus on water, sanitation and hygiene and improved environmental sanitation to prevent these diseases in pediatric population.
Data availability
The data sets generated during and/or analyzed during the current study are available from the corresponding authors on reasonable request.
References
WHO. diarrheal. desease 2017 [ https://www.who.int/en/news-room/fact-sheets/detail/diarrhoeal-disease.
Kefyalew S, Kebede G, Keneni A. Prevalence of Shigella related diarrhea in Ambo town and antibiotic susceptibility of the isolated strains. Greener J Epidemiol Public Health. 2015;3(1):001–6.
Kotloff KL, Nataro JP, Blackwelder WC, Nasrin D, Farag TH, Panchalingam S, et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): a prospective, case-control study. Lancet (London England). 2013;382(9888):209–22.
EDHS. Diearheal diseases in children. Maryland, MA, USA: CSA and ICF; 2016.
unicef. under five mortality 2021 [ https://data.unicef.org/topic/child-survival/under-five-mortality/.
Larsson DJ, Flach C-F. Antibiotic resistance in the environment. Nat Rev Microbiol. 2022;20(5):257–69.
Wikipedia. Jijiga (woreda) 2021 [ https://en.wikipedia.org/wiki/Jijiga_(woreda).
jigjiga university. Jigjiga University Sheik Hassen Yabare Referral Hospital 2021 [updated 2022. https://www.google.com/search?q=jigjiga+university+referral+hospital&oq=jig&aqs=chrome.1.69i57j69i59j0i271l3j69i60l3.6170j0j7&sourceid=chrome&ie=UTF-8.
Ameya G, Tsalla T, Getu F, Getu E. Antimicrobial susceptibility pattern, and associated factors of Salmonella and Shigella infections among under five children in Arba Minch, South Ethiopia. Ann Clin Microbiol Antimicrob. 2018;17(1):1–7.
Terfassa A, Jida M. Prevalence and antibiotics susceptibility pattern of Salmonella and Shigella species among diarrheal patients attending Nekemte Referral Hospital, Oromia, Ethiopia. International journal of microbiology. 2018;2018.
Tosisa W, Mihret A, Ararsa A, Eguale T, Abebe T. Prevalence and antimicrobial susceptibility of Salmonella and Shigella species isolated from diarrheic children in Ambo town. BMC Pediatr. 2020;20(1):1–8.
Cheesbrough M. District laboratory practice in tropical countries, part 2. Cambridge University Press; 2005.
Mikoleit M. Biochemical Identification of Salmonella and Shigella Using an Abbreviated Panel of Tests2014.
Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. Clinical and Laboratory Standards Institute Wayne, PA; 2022.
Gebreyohannes G, Moges F, Woldemariam S, Raja N, Reetha D. Isolation and characterization of potential antibiotic producing actinomycetes from water and sediments of Lake Tana, Ethiopia. Asian Pac J Trop Biomed. 2013;3:426–35.
Nunes MR, Magalhães PP, Penna FJ, Nunes JM, Mendes EN. Diarrhea associated with Shigella in children and susceptibility to antimicrobials. Jornal De Pediatria. 2012;88(2):125–8.
WHO. diarheal. disease 2013 [ https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease.
Magiorakos A-P, Srinivasan A, Carey Rt, Carmeli Y, Falagas Mt G, Ct, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–81.
Supply WUJW, Programme SM. Progress on drinking water and sanitation: 2014 update. World Health Organization; 2014.
Shad AA, Shad WA. Shigella sonnei: virulence and antibiotic resistance. Arch Microbiol. 2021;203(1):45–58.
Beyene G, Tasew H. Prevalence of intestinal parasite, Shigella and Salmonella species among diarrheal children in Jimma health center, Jimma Southwest Ethiopia: a cross sectional study. Ann Clin Microbiol Antimicrob. 2014;13(1):1–7.
Mishra R, Sheth M. Burden of Diarrhoeal diseases through Complementary foods: a review. Asian J Dairy Food Res. 2023;42(1):76–82.
Sang WK, Oundo V, Schnabel D. Prevalence and antibiotic resistance of bacterial pathogens isolated from childhood diarrhoea in four provinces of Kenya. J Infect Developing Ctries. 2012;6(07):572–8.
Mamuye Y, Metaferia G, Birhanu A, Desta K, Fantaw S. Isolation and antibiotic susceptibility patterns of Shigella and Salmonella among under 5 children with acute diarrhoea: a cross-sectional study at selected public health facilities in Addis Ababa, Ethiopia. Clinical Microbiology: Open Access; 2015.
Kara TT, Özdemir H, Kurt F, Güriz H, Çiftçi E, Aysev AD, et al. Prevalence of Salmonella and Shigella spp. and Antibiotic Resistance Status in Acute Childhood Gastroenteritis/Akut Çocukluk Çagi Gastroenteritlerindeki Salmonella-Shigella Sikligi ve Antibiyotik Direnç Durumlari. Cocuk Enfeksiyon Dergisi. 2015;9(3):102.
Ansari S, Sherchand J, Parajuli K, Mishra S, Dahal R, Shrestha S et al. Bacterial etiology of acute diarrhea in children under five years of age. J Nepal Health Res Counc. 2012.
Amukoshi M, Maposa I, Moyo SR, Mukesi M. Etiological agents isolated from stool samples of children under the age of five years in Windhoek, Namibia. Edorium J Microbiol. 2017;3:1–9.
Mulatu G, Beyene G, Zeynudin A. Prevalence of Shigella, Salmonella and Cmpylobacter species and their susceptibility patters among under five children with diarrhea in Hawassa town, South Ethiopia. Ethiop J Health Sci. 2014;24(2):101.
Reda AA, Seyoum B, Yimam J, Fiseha S, Jean-Michel V. Antibiotic susceptibility patterns of Salmonella and Shigella isolates in Harar, Eastern Ethiopia. J Infect Dis Immun. 2011;3(8):134–9.
Teferi SC, Prevalence. Antibiotic Susceptibility Profile, and associated risk factors of Salmonella isolate among diarrheal patients visiting Dessie referral hospital, Northeast Ethiopia. International Journal of Microbiology. 2020;2020.
Beyene G, Tasew H. Prevalence of intestinal parasite, Shigella and Salmonella species among diarrheal children in Jimma health center, Jimma Southwest Ethiopia: a cross sectional study. Ann Clin Microbiol Antimicrob. 2014;13(1):10.
Farahani NN, Jazi FM, Nikmanesh B, Asadolahi P, Kalani BS, Amirmozafari N. Prevalence and antibiotic susceptibility patterns of Salmonella and Shigella species isolated from pediatric diarrhea in Tehran. Archives Pediatr Infect Dis. 2018;6(4).
Gebrekidan A, Dejene TA, Kahsay G, Wasihun AG. Prevalence and antimicrobial susceptibility patterns of Shigella among acute diarrheal outpatients in Mekelle hospital, Northern Ethiopia. BMC Res Notes. 2015;8(1):611.
Abebe W, Earsido A, Taye S, Assefa M, Eyasu A, Godebo G. Prevalence and antibiotic susceptibility patterns of Shigella and Salmonella among children aged below five years with diarrhoea attending Nigist Eleni Mohammed memorial hospital, South Ethiopia. BMC Pediatr. 2018;18(1):241.
Admassu M, Yemane G, Kibret M, Abera B, Nibret E, Adal M. Prevalence and antibiogram of Shigella and Salmonella spp. from under five children with acute diarrhea in Bahir Dar Town. Ethiop J Sci Technol. 2015;8(1):27–35.
Mengistu G, Mulugeta G, Lema T, Aseffa A. Prevalence and antimicrobial susceptibility patterns of Salmonella serovars and Shigella species. J Microb Biochem Technol. 2014;6(S2):S2–006.
Assefa A, Girma M. Prevalence and antimicrobial susceptibility patterns of Salmonella and Shigella isolates among children aged below five years with diarrhea attending Robe General Hospital and Goba Referral Hospital, South East Ethiopia. Tropical diseases, travel medicine and vaccines. 2019;5(1):19.
Kiptoo MK, Karambu S, Matiru V, Oundo J. Characterization and factors associated with diarrhoeal diseases caused by enteric bacterial pathogens among children aged five years and below attending Igembe District Hospital, Kenya. 2013.
Adane M, Mengistie B, Mulat W, Medhin G, Kloos H. The Most Important Recommended Times of Hand Washing with soap and water in preventing the occurrence of Acute Diarrhea among Children under five years of age in slums of Addis Ababa, Ethiopia. J Community Health. 2018;43(2):400–5.
Santamaría J, Toranzos GA. Enteric pathogens and soil: a short review. Int Microbiol. 2003;6:5–9.
Alemu A, Geta M, Taye S, Eshetie S, Engda T. Prevalence, associated risk factors and antimicrobial susceptibility patterns of Shigella infections among diarrheic pediatric population attending at Gondar town healthcare institutions, Northwest Ethiopia. Tropical diseases, travel medicine and vaccines. 2019;5(1):7.
Bacterial isolates teshomeb, antimicrobial susceptibility pattern and its associated factors among. patients with diarrhea visiting ADAMA public health facilities, ADAMA, Central Ethiopia. 2017.
Mekonnen S, Prevalence, associated factors and antimicrobial susceptibility pattern of bacterial, urinary tract infections among clinically suspected under five children at hiwot fana specialized university hospital., HARAR, Eastern Ethiopia: Haramaya University; 2021.
Hayamo M, Alemayehu T, Tadesse B, Mitiku E, Bedawi Z. Shigella and Salmonella, antibiotics susceptibility pattern and associated risk factors among diarrheic children in southern Ethiopia: a cross sectional study. 2020.
Mandomando I, Jaintilal D, Pons MJ, Vallès X, Espasa M, Mensa L, et al. Antimicrobial susceptibility and mechanisms of resistance in Shigella and Salmonella isolates from children under five years of age with diarrhea in rural Mozambique. Antimicrob Agents Chemother. 2009;53(6):2450–4.
Acknowledgements
First of all, we would like to acknowledge Haramaya University for funding. Next, we would also like to thank Jigjiga University referral hospital. Appreciation also goes to the participants of the study for their voluntarism of participation to the study.
Funding
This research data collection finance was supported by Haramaya university postgraduate directorate.
Author information
Authors and Affiliations
Contributions
KM contributed in the design of the study, conducted data collection, analyzed the data and drafted the paper. KU, FW, BT and TS participated in the conception and design of the study, analysis and interpretation of the data and revised subsequent drafts of the paper. KU, FW, TS and BT: participated in data collection, conducted data analysis, drafted and finalized the manuscript for publication. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent
The study was conducted out after receiving ethical approval from Haramaya University College of Health Science and Medical Sciences Institutional Health Research Ethics Review Committee (IHRERC 141/2022)). This study was conducted in accordance with the Declaration of Helsinki. Each child’s parent/guardian has been sufficiently informed of the study’s purpose and the importance of their participation by the data collectors and/or the investigator. Permission was gained from Somali Regional Health Bureau, Jigjiga University Sultan Sheik Hassan Yabere Referral Hospital administration. Written, informed, voluntary, and signed consent were taken from all parents/guardians were taken before commencing the study. All parents/guardians were consulted about the benefit of the treatment by a pediatrician who works at Jigjiga University Sultan Shiek Hassen Referral Hospital and the drugs were given free of charge.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Muse, K., Urgessa, K., Shume, T. et al. Prevalence, associated factors and antimicrobial susceptibility patterns of Salmonella and Shigella species among diarrheic under five children in Sultan Sheik Hassan Yabere referral Hospital, Jigjiga, Eastern Ethiopia. BMC Pediatr 24, 311 (2024). https://doi.org/10.1186/s12887-024-04755-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-024-04755-6