
Abstract
Background
Self-regulation (SR), or the capacity to control one’s thoughts, emotions, and behaviors in order to achieve a desired goal, shapes health outcomes through many pathways, including supporting adherence to medical treatment regimens. Type 1 Diabetes (T1D) is one specific condition that requires SR to ensure adherence to daily treatment regimens that can be arduous and effortful (e.g., monitoring blood glucose). Adolescents, in particular, have poor adherence to T1D treatment regimens, yet it is essential that they assume increased responsibility for managing their T1D as they approach young adulthood. Adolescence is also a time of rapid changes in SR capacity and thus a compelling period for intervention. Promoting SR among adolescents with T1D may thus be a novel method to improve treatment regimen adherence. The current study tests a behavioral intervention to enhance SR among adolescents with T1D. SR and T1D medical regimen adherence will be examined as primary and secondary outcomes, respectively.
Methods
We will use a randomized control trial design to test the impact of a behavioral intervention on three SR targets: Executive Functioning (EF), Emotion Regulation (ER), and Future Orientation (FO); and T1D medical regimen adherence. Adolescents with T1D (n = 94) will be recruited from pediatric endocrinology clinics and randomly assigned to treatment or control group. The behavioral intervention consists of working memory training (to enhance EF), biofeedback and relaxation training (to enhance ER), and episodic future thinking training (to enhance FO) across an 8-week period. SR and treatment regimen adherence will be assessed at pre- and post-test using multiple methods (behavioral tasks, diabetes device downloads, self- and parent-report). We will use an intent-to-treat framework using generalized linear mixed models to test our hypotheses that: 1) the treatment group will demonstrate greater improvements in SR than the control group, and 2) the treatment group will demonstrate better treatment regimen adherence outcomes than the control group.
Discussion
If successful, SR-focused behavioral interventions could improve health outcomes among adolescents with T1D and have transdiagnostic implications across multiple chronic conditions requiring treatment regimen adherence.
Trial registration
ClinicalTrials.gov: NCT03688919; registered September 28, 2018.
Similar content being viewed by others

Background
Decades of research have demonstrated the importance of self-regulation (SR), or the capacity to control one’s thoughts, emotions, and behaviors in order to achieve a desired goal, in shaping individuals’ health outcomes [1, 2]. SR capacity has been conceptualized as including three component processes: executive functioning skills; emotion regulation strategies; and ability to delay gratification in service of achieving future goals [3, 4]. Low SR capacity has been shown to interfere with individuals’ engagement in a variety of health maintenance behaviors including engaging in regular physical activity [5], consuming a healthy diet [6,7,8], and adhering to medical treatment regimens [9,10,11].
Type 1 Diabetes (T1D) is a condition affecting millions worldwide. For example, in the U.S. about 17,900 children and adolescents younger than age 20 were newly diagnosed with type 1 diabetes during 2011–2012 [12]. Adhering to a recommended treatment regimen is critical in managing glycemic control and establishing long-term health among pediatric T1D patients [13,14,15]. Yet, poor treatment regimen adherence is common among adolescents [16,17,18]. Only 21% of adolescents meet the American Diabetes Association guidelines for Hemoglobin A1c (HbA1c) target level of 7.5% [14, 19], and treatment adherence and glycemic control decline across this developmental period [20]. Poor glycemic control places youth with T1D at substantially increased risk of acute health events including hyper and hypoglycemia and diabetic ketoacidosis, as well as serious, long-term comorbidities such as retinopathy, neuropathy, kidney disease, and cardiovascular disease [21].
To achieve and maintain optimal glycemic control, adolescents must adhere to a complex self-care regimen that includes monitoring blood glucose, administering insulin via daily injections or a pump, regulating carbohydrate intake, engaging in regular physical activity, and minimizing both hyper- and hypoglycemia [22, 23]. Each of these are daily tasks that require SR. For example, executive function (EF) skills such as working memory and planning are needed to recall and ensure adherence to dietary and exercise plans [24,25,26]. Emotion regulation (ER) skills are important for coping with diabetes-related distress, combating depression, and managing feelings of anxiety that interfere with monitoring blood sugar levels [27,28,29]. Future orientation (FO), or the ability to delay gratification and focus on future goals, may be particularly important for adolescents with T1D in order to adhere to their treatment regimen in the face of competing demands.
Positive associations between SR capacity and treatment adherence are consistently reported in prior work among youth with T1D [3, 30, 31] and poor SR has been suggested as a central mechanism contributing to nonadherence [23,24,25,26, 32]. For example, in 13–17 year-olds with T1D, parent-rated EF deficits in working memory and attention were associated with poorer treatment adherence [33], with further research identifying that associations between EF and glycemic control were mediated through treatment adherence [26]. With regard to ER, findings suggest that adolescents with poorer ER skills have higher HbA1c levels, suggestive of poorer glycemic control [34, 35]. Finally, no studies have specifically examined associations between FO and treatment adherence in adolescents with T1D. However, in adults with T1D, results suggest FO skills are positively associated with treatment adherence [36, 37]. Moreover, FO is associated with engagement in several other health behaviors that promote long-term goals [38, 39], including in adolescents [40]. Given this body of research, the pervasiveness of poor treatment adherence among adolescents with T1D, and the fact that the fact that treatment regimens shift from parent-managed to adolescent managed across this period [16, 41,42,43], improving adolescents’ SR capacity may be an important strategy for helping them better manage treatment adherence tasks [3, 44].
Promoting SR may increase adolescents’ ability to engage in diabetes-specific adherence behaviors and thereby improve T1D outcomes [23, 44,45,46]. Specifically, improving EF skills could aid adolescents’ remembering regimen details and timing [33], enhancing ER capacity could improve metabolic control by promoting better regulation of stress hormones, reducing diabetes-related distress, and increasing capacity to focus on regimen adherence [11, 47]; and improving FO capacity may increase adherence by engaging adolescents to invest energy in behaviors that lead to long-term health [48, 49]. Yet, improving SR has not been tested as a mechanism of behavior change in this population.
Study aims and hypotheses
The primary aim of the Adolescent Interventions to Manage Self-Regulation in Type 1 Diabetes (AIMS-T1D) study is to determine whether a behavioral intervention improves SR targets (EF, ER, FO) among adolescents (ages 13–17) with T1D. The secondary aim to determine whether the behavioral intervention improves T1D treatment regimen adherence among participating adolescents. We hypothesize that adolescents randomized to the treatment group will demonstrate significant improvements in EF, ER, and FO compared to adolescents randomized to the control group after 8 weeks of intervention. We hypothesize that adolescents randomized to the treatment group will demonstrate significant improvements in treatment regimen adherence including improved blood glucose monitoring and insulin administration adherence, as well as self-reported treatment regimen adherence).
Methods/design
Approval and trial registration
The AIMS-T1D study is a 24-month randomized controlled trial taking place in Ann Arbor, Michigan. At the time of submission of this manuscript, participants were being enrolled into the trial. The trial has been approved by the University of Michigan Institutional Review Board (HUM00148853) and is registered with ClinicalTrials.gov, ID NCT03688919. An internal Data Safety Monitoring Board consisting of pediatric psychologists, pediatric endocrinologists, and adolescent medicine specialists in T1D was formed to monitor the study (e.g., determine stopping rules, review any adverse events).
A total sample of 94 participants aged 13–17 years with T1D will be recruited from a pediatrics diabetes clinic research registry of patients receiving diabetes care at the University of Michigan.
Inclusion and exclusion criteria
Adolescents must meet the following criteria to participate: 1) been diagnosed with T1D for at least 6 months; 2) aged between 13 and 17 years; 3) reside with a parent/legal guardian who is the primary caregiver; 4) have HbA1c ≥ 7.0; 5) have regular access to Wi-Fi; 6) feel comfortable speaking English enough to complete study activities; and 7) receive diabetes care from providers within Pediatric Endocrinology at Michigan Medicine. All diabetes treatment regimens are included in the study (e.g., multiple dose injection, blood glucose monitoring [BGM], continuous glucose monitoring [CGM], or a combination). Exclusion criteria are: 1) non-fluency in English in parent or child; or 2) psychiatric or cognitive conditions, such as clinically significant depression assessed via phone screen at intake that would impede ability to participate.
Participant recruitment
Participants will be recruited via email, phone, and text message sent to themselves or their parent(s) using contact information obtained by the Pediatrics Endocrinology clinic. The study will also be advertised in newsletters sent by the clinic and via flyers available in clinic. Eligible participants may also be recruited face-to-face during clinic visits. Participants who communicate interest in study participation will complete a phone screening and eligible participants will have their baseline study visit scheduled. Adolescents will be randomized to intervention group when scheduled. A research assistant will obtain informed consent from parents for their own and their child’s participation in the study; adolescents also provide assent for their participation in the study.
Randomization strategy and blinding
Participants will be randomized to receive the AIMS-T1D intervention or the control activities (see below) using an Excel-based randomization tool (2 conditions: treatment and control) and a random number generator. To blind evaluation study team members to participants’ condition assignment, the intervention team will be exclusively responsible for creating and implementing the randomization assignments as well as participant case management during the 8-week intervention period.
Intervention conditions
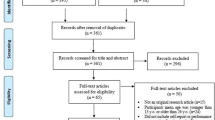
As recommended by the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) Guidelines [50], study procedure details are outlined in Fig. 1 (see Additional file 1 for SPIRIT Checklist). Treatment and control group activities are described below.

Study procedure details
Treatment group activities
The AIMS-T1D intervention is based on prior work that used a multiphase optimization strategy design [51] framework to test different intervention strategies on SR targets among youth, specifically EF, ER, and FO [4]. Intervention activities, which are manualized, will be introduced to participants in person after randomization by trained interventionists. Sessions will be coded for fidelity from video. Participants assigned to the treatment condition will participate in 8-weeks of home practice; participants will have regular contact with interventionists via text-based reminders to help ensure adherence and practice records will be used to assess intervention dose. A detailed description of activities is below and shown in Fig. 2. Note, as the intervention will be conducted in the order described below, we present intervention activities and measures first for FO, then ER, and then EF.

Self-regulation targets and intervention activities
Future orientation
Episodic future thinking (EFT), or projecting to “make the future become the present” can promote FO [38, 39]. We will employ EFT techniques that have been previously used with adolescents [52]. The goal of these activities is to enhance the participants’ ability to “pre-experience” the future in an active, vivid, and concrete manner. A positive personal goal or event is selected, and the feelings and experience of achieving the goal or the event are verbalized and practiced [53]. The interventionist will coach the participant to describe an upcoming, positive event at least 2 months away (i.e., the duration of the study), using present tense and concrete details (e.g., who will be there, where event will take place, visual/sensory information) in order to make the experience as vivid as possible. The participant will generate three such future events, also known as cues. The participant will then be asked to link each cue to their T1D treatment regimen (i.e., “because I checked my blood glucose level on my way to my friend’s house and was able to give insulin to bring my blood glucose in range, I felt more confident spending the evening there”). For home practice, text messages with these cues will be sent at 3 preferred times of day; participants will review the cue and answer on a scale of 1–5 how vividly they are able to bring it to mind.
Emotion regulation
Evidence-based biofeedback and guided relaxation techniques will be used to promote ER [54, 55]. The interventionist will use a computer-based program, HeartMath® to show the participant how to use diaphragmatic breathing to improve heart rate variability coherence [56]. The interventionist will guide the participant to match the pace of their breath to a graphic of a Mandala expanding and contracting (5 min) and how to use diaphragmatic breathing to change a picture of a garden from black-and-white to multi-colored (greater coherence, more of the garden becomes colored). The final activity is a progressive muscle relaxation exercise. ER home practice consists of 5 guided meditations that incorporate diaphragmatic breathing (using Insight Timer, a free meditation app downloaded on the participant’s phone), to be practiced once a day for 5 min.
Executive function
A tablet-based working memory game based on the n-back task will be used to improve EF [57, 58]. This task has shown to improve working memory and also to facilitate transfer effects to other aspects of EF, including inhibitory control [59]. This object-based variant of the n-back displays sequential images (e.g. fruit, animals) and prompts the participant to tap the screen when an image matches a previous. The game becomes more challenging as the participant completes items accurately, requiring matches of two, three, four, etc. images “back”. The game will be introduced by the interventionist and the participant instructed to practice daily on the tablet (10 rounds of the game, approximately 15 min in total per session), sending screenshots to the interventionist in order to earn incentives (below).
Incentives
Participants will be incentivized to complete home practice activities with the opportunity to earn $10 a week for reviewing and completing the one-item cue question described above for at least 12 of the 21 cues they received via text message, and texting four screenshots of meditation practice and four screenshots of the n-back game to the interventionist. Additionally, each screenshot translates to 1 raffle ticket for an Amazon gift card, with an opportunity to earn 2 bonus raffle tickets if every home practice task is completed.
Control group activities
Control group activities consist of enhanced usual care. After randomization, participants assigned to the control condition will meet with an interventionist to receive an interactive PowerPoint presentation reviewing resources from the University of Michigan Pediatric Diabetes clinic website (www.umpedsdiabetes.com), to which all clinic families have access. For the 8-week study period, in lieu of AIMS-T1D intervention activities, participants will receive 1 text message per week with a link to the clinic website and be asked to explore the pages of interest to them. The text messages will be sent at the same time and day each week, selected by the participant.
Study measures and assessment timeline
Measures of all primary and secondary outcomes will be conducted at baseline and again 8 weeks later in order to evaluate change in each outcome among participants in the intervention versus control groups (see Table 1 for list of measures and assessment method). Staff are extensively trained in both questionnaire and behavioral task administration using manuals developed in prior work that used similar assessment strategies [4].
Primary outcome measures (SR)
Primary study outcomes include FO, ER, and EF as indicators of SR. Where appropriate, SR is assessed using a combination of direct assessment (behavioral tasks completed by the participant) plus adolescent self-report and parent-report on standard questionnaires that have been found to be reliable in prior work [4]. Task and questionnaire-based assessments will be analyzed separately as such measurement approaches may represent different aspects of SR. [60]
Future Orientation (FO)
The degree to which one discounts the future is an aspect of FO that will be measured using the 5-trial Delay Discounting Task [61]. Each trial uses one monetary amount (e.g., $1000 to $1000,000). Each participant is asked on the first trial whether they would prefer to receive that amount in 3 weeks or half that amount now. On the next trial the question is repeated but with a different time delay according to the participant’s response on the previous trial. That is, a greater delay is presented on the next trial if the participant chose “now” on the previous trial, whereas a lesser delay is presented if the participant chose the later time on the previous trial. The dependent measure is the steepness of the delay discounting curve; steeper curves indicate that an individual is less future-oriented (i.e. more impulsive).
Considering the future and how one’s actions can affect future consequences is an aspect of FO that will be measured by youth self-report using the Consideration of Future Consequences Scale [62]. Adolescents will answer 14 questions (e.g., “I think about how things would be in days to come, and try to influence those things in my daily behavior”) on a 7-point scale (1 = Not at all like me to 7 = Very much like me). Higher scores indicate a greater consideration of future consequences or future-oriented behavior. Self-efficacy is hypothesized to promote future-oriented thinking, and is thus an aspect of FO that will be measured using a composite of the National Institutes of Health (NIH) Toolbox Self-Efficacy parent report and the self-report form (10 items each) [63]. Participants respond to questions about their child’s or their own (in the case of the child) self-efficacy. Mean scores are generated; higher scores are indicative of greater perceived self-efficacy.
Emotion Regulation (ER)
The adolescent’s ER will be measured using self-reports of dysregulated affect using a 6-item scale based on the Structured Interview for Disorders of Extreme Stress [64] (items are averaged to indicate greater affect dysregulation, range: 1–6); and self-reports of emotion experiences on the 20-item Positive and Negative Affect Schedule [65] (items are summed to indicate more negative [10 items] and fewer positive experiences [10 items]; range: 10–50). A composite measure of parent- and self-reports on the Perceived Stress Survey [63], a 10-item measure of stress in children and youth (items are summed to indicate greater perceived stress; range: 0–40) will also be used. A composite measure will be created by standardizing and averaging affect dysregulation, emotion experience, and perceived stress scores. It will be scored such that higher values indicate poorer ER.
Executive Function (EF)
EF will be measured using standard tasks (Forward/Backward Digit Span, Go-No/Go). Digit span assesses working memory, a key component of EF. In Digit Span [66], participants repeat numbers that the examiner reads aloud in order or reverse order (8 questions, 2 trials each; correct response is 1 point; incorrect or no response is 0 points). Scores are summed for each trial; maximum total raw score is 16 points. The Go-No/Go task [67] is presented on a laptop and assesses inhibitory control, another key component of EF. Participants hit a key to respond when they see the ‘go’ stimulus (presented for 300 ms) but not when they see the no-go stimulus. Go-No/Go responses are scored based on reaction time (seconds) and accuracy (0–100%). A composite variable indexing better behavioral EF based on Digit Span and Go-No/Go tasks will be created by generating standardized z-scores for each task variable and calculating a mean score.
EF will also be assessed using the parent- and self-report versions of the Behavior Rating Inventory of Executive Functioning, 2nd Edition, a standardized EF measure [68]. Subscales assess ability to control impulses, flexibly change direction, pay attention, modulate responses, and anticipate events. Items are combined to form a Global Executive Composite score, which is a standardized score representing overall EF difficulties (range 0–100). Self- and parent reports will be used to measure overall Global Executive Functioning, scored such that higher scores indicate greater difficulties in EF functioning.
Secondary outcome measures (treatment regimen adherence)
Secondary outcomes assess adherence to the participant’s T1D regimen, specifically blood glucose monitoring (BGM), insulin administration, and scores on the Self-Care Inventory Revised (SCI-R) [69]. The continuum of adolescents’ adherence will be examined, as well as changes in the proportion of adolescents “adherent” vs. “nonadherent” based on clinical criteria [70].
BGM frequency will be assessed by downloading data from the prior 2 weeks from the adolescent’s glucometer or relevant blood glucose monitoring device (e.g., CGM). Adherence to BGM is defined as an average of 4 blood glucose measurements/day and/or wearing a CGM pump 6 out of 7 days. Insulin administration adherence is defined as at least 3 short acting insulin boluses/day. Insulin administration frequency for participants an insulin pump can be measured using data from software downloads (e.g., Glooko/diasend, Tidepool). For participants on injections, the number of short-acting insulin boluses will be measured by self-report.
Finally, the SCI-R [69] is a 14-item self- and parent-report measure of multiple T1D self-care adherence behaviors. Items reflect main aspects of the T1D regimen, including: monitoring and recording glucose, administering and adjusting insulin, regulating meals and exercise, and keeping appointments. Respondents report on adherence behaviors on a 5-point scale (1=“never do it”; 5=“always do this as recommended without fail”; or N/A). Adolescent and parent responses will be summed and analyzed separately.
Data analysis
After secure data entry, coding, cleaning, and creating and checking the psychometric properties of any composite variables, we will conduct our study analyses. We will use an intent-to-treat analytic framework to test whether the AIMS-T1D intervention was effective in changing SR targets (primary outcome) and treatment regimen adherence (secondary outcome) variables. We will compare change in the group assigned to treatment compared to the group assigned to the control condition from pre- to post-test across the 8-week intervention period. All analyses will use an alpha value of p < .05 and will be conducted in SAS. Baseline comparability of the groups will first be assessed using bivariate analyses (t-tests, X2) as appropriate.
We will conduct our primary and secondary outcome analyses using linear mixed effects models (for continuous outcomes) and generalized linear mixed models (for dichotomous outcomes) to compare changes in SR and adherence across the two groups (treatment vs. control). The mixed effects models will account for the within-subject correlations due to having repeating measurements in individual subjects over time. Both unadjusted and adjusted analyses will be performed, with adjustment for important baseline covariates that relate to the outcome, including participant age and sex.
We anticipate that some participants will have only partial adherence to the AIMS-T1D intervention (i.e. complete only some home practice sessions), thus we will also conduct a dose-response analysis where dose corresponds to number of sessions, controlling for covariates that relate to dosage and outcome of interest.
Power
We based our power analysis on prior work detecting change in SR targets [4] and T1D medication adherence literature [10, 11]. We anticipate medium effect sizes of 0.6 with the bundled interventions, so our proposed sample size of 94 (47 per group) should result in sufficient statistical Power of 82% to detect such effects using a two-sided Type I error alpha of 0.05. In addition, controlling for baseline variables that relate to outcome will reduce the residual variance and further increase statistical Power.
Discussion
Given that only about a fifth of adolescents with T1D meet recommended T1D treatment targets, there remains an urgent need to identify effective strategies to improve treatment regimen adherence among this population. As responsibility for diabetes management shifts from parent to child across the adolescent period, identifying interventions that are engaging and effective for this developmental stage is essential. Difficulties with SR may underlie poor T1D treatment regimen adherence during adolescence, a time characterized by continued SR maturation and daily challenges to SR due to typically developing demands (e.g., social, academic, emotional). Indeed, developmental neuroscience suggests adolescence is a time of uneven growth in SR skills such as EF, but is also characterized by increasing ability to take broader perspectives and envision the future, including health behaviors; thus, adolescence is a unique and compelling period for intervention [71]. Every day, adolescents with T1D must engage in tasks that require a high degree of SR, including monitoring blood sugar and carbohydrate intake, maintaining a schedule for eating as well as physical exercise, and ensuring adequate access to T1D supplies and resources in the event that blood sugars are too high or too low. Further, as psychological adjustment to and coping with T1D can also interfere with treatment adherence [27], ER strategies may play a critical role in promoting adherence. Finally, adhering to T1D regimens requires FO, which allows adolescents to understand and appreciate how achieving current adherence goals, which may be difficult, can help maintain optimal HbA1c levels in order to avoid long-term complications.
The current randomized control trial proposes to test whether the AIMS-T1D behavioral intervention can improve adolescents’ SR and treatment regimen adherence. The study takes an experimental medicine approach to behavior change by testing the impact of an intervention targeting SR as a primary outcome [72]. As prior work using similar interventions suggests that these aspects of SR are malleable [52, 54, 59], the next step in a systematic experimental medicine approach to building and testing better interventions is to test whether these early findings can generalize to a new population, specifically adolescents with T1D. A benefit of this approach is that by identifying whether the interventions designed to change SR actually do so, we will gain critical information about the utility of such interventions for future research in new populations. To our knowledge, this is one of the first studies to test a SR-focused intervention in youth in relation to a health-relevant outcome. From a prevention perspective, it is more cost-effective to prevent negative health outcomes associated with poor treatment regimen adherence than to treat the long-term sequelae of poor adherence. Further, by improving SR during adolescence, we may achieve not only better T1D treatment regimen adherence in the short term, but impact lasting improvements both in SR and the health trajectory of those with T1D. From a trans-diagnostic perspective, if this trial demonstrates meaningful improvements in adolescents’ SR, the intervention may be a novel approach to health behavior change among other populations of adolescents with medical needs that require strict adherence to treatment regimens. Therefore, findings from the AIMS-T1D study not only have the possibility of informing our understanding of SR as a mechanism of behavior change among adolescents with T1D, but also have implications, and thus the potential, for broad impact.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AIMS-T1D:
-
Adolescent Interventions to Manage Self-Regulation in Type 1 Diabetes
- BGM:
-
Blood Glucose Monitoring
- CGM:
-
Continuous Glucose Monitoring
- EF:
-
Executive Function
- EFT:
-
Episodic Future Thinking
- ER:
-
Emotion Regulation
- FO:
-
Future Orientation/Motivation
- HbA1c:
-
Hemoglobin A1c
- NIH:
-
National Institutes of Health
- SCI-R:
-
Self-Care Inventory Revised
- SR:
-
Self-regulation
- T1D:
-
Type 1 Diabetes
References
Mann T, De Ridder D, Fujita K. Self-regulation of health behavior: social psychological approaches to goal setting and goal striving. Health Psychol. 2013;32(5):487.
Hagger MS. Self-regulation: an important construct in health psychology research and practice. Health Psychol Rev. 2010;4(2):57–65. https://doi.org/10.1080/17437199.2010.503594.
Lansing AH, Berg CA. Topical review: adolescent self-regulation as a Foundation for Chronic Illness Self-Management. J Pediatr Psychol. 2014;39(10):1091–6.
Miller AL, Gearhardt AN, Fredericks EM, Katz B, Shapiro LF, Holden K, et al. Targeting self-regulation to promote health behaviors in children. Behav Res Ther. 2018;101:71–81.
Pfeffer I, Strobach T. Executive functions, trait self-control, and the intention-behavior gap in physical activity behavior. J Sport Exerc Psychol. 2017;39(4):277–92.
Martin AA, Davidson TL, McCrory MA. Deficits in episodic memory are related to uncontrolled eating in a sample of healthy adults. Appetite. 2018;124:33–42.
Wyckoff EP, Evans BC, Manasse SM, Butryn ML, Forman EM. Executive functioning and dietary intake: neurocognitive correlates of fruit, vegetable, and saturated fat intake in adults with obesity. Appetite. 2017;111:79–85.
Limbers CA, Young D. Executive functions and consumption of fruits/ vegetables and high saturated fat foods in young adults. J Health Psychol. 2015;20(5):602–11.
Lebeau G, Consoli SM, Le Bouc R, Sola-Gazagnes A, Hartemann A, Simon D, et al. Delay discounting of gains and losses, glycemic control and therapeutic adherence in type 2 diabetes. Behav Process. 2016;132:42–8.
Berg CA, Wiebe DJ, Suchy Y, Turner SL, Butner J, Munion A, et al. Executive function predicting longitudinal change in type 1 diabetes management during the transition to emerging adulthood. Diabetes Care. 2018;41(11):2281–8.
Berg CA, Wiebe DJ, Suchy Y, Hughes AE, Anderson JH, Godbey EI, et al. Individual differences and day-to-day fluctuations in perceived self-regulation associated with daily adherence in late adolescents with type 1 diabetes. J Pediatr Psychol. 2014;39(9):1038–48.
Mayer-Davis EJ, Lawrence JM, Dabelea D, Divers J, Isom S, Dolan L, et al. Incidence trends of type 1 and type 2 diabetes among youths, 2002–2012. N Engl J Med. 2017;376(15):1419–29.
Hood KK, Peterson CM, Rohan JM, Drotar D. Association between adherence and glycemic control in pediatric type 1 diabetes: a meta-analysis. Pediatrics. 2009;124(6):e1171–e9.
Chiang JL, Kirkman MS, Laffel LM, Peters AL. Type 1 diabetes through the life span: a position statement of the American Diabetes Association. Diabetes Care. 2014;37(7):2034–54.
Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353(25):2643–53.
Rausch JR, Hood KK, Delamater A, Shroff Pendley J, Rohan JM, Reeves G, et al. Changes in treatment adherence and glycemic control during the transition to adolescence in type 1 diabetes. Diabetes Care. 2012;35(6):1219–24.
Wang JT, Wiebe DJ, White PC. Developmental trajectories of metabolic control among White, black, and Hispanic youth with type 1 diabetes. J Pediatr. 2011;159(4):571–6.
Helgeson VS, Snyder PR, Seltman H, Escobar O, Becker D, Siminerio L. Brief report: trajectories of glycemic control over early to middle adolescence. J Pediatr Psychol. 2010;35(10):1161–7.
Wood JR, Miller KM, Maahs DM, Beck RW, DiMeglio LA, Libman IM, et al. Most youth with type 1 diabetes in the T1D exchange clinic registry do not meet American Diabetes Association or international society for pediatric and adolescent diabetes clinical guidelines. Diabetes Care. 2013;36(7):2035–7.
Gandhi K, Vu B-MK, Eshtehardi SS, Wasserman RM, Hilliard ME. Adherence in adolescents with Type 1 diabetes: strategies and considerations for assessment in research and practice. Diab Manage (London, England). 2015;5(6):485.
Nathan DM. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: overview. Diabetes Care. 2014;37(1):9–16.
American Diabetes Association. Introduction: Standards of Medical Care in Diabetes—2018. Diab Care. 2018;41(Suppl 1):S1–S2. https://doi.org/10.2337/dc18-Sint01.
Gonzalez JS, Tanenbaum ML, Commissariat PV. Psychosocial factors in medication adherence and diabetes self-management: implications for research and practice. Am Psychol. 2016;71(7):539.
Duke DC, Harris MA. Executive function, adherence, and glycemic control in adolescents with type 1 diabetes: a literature review. Curr Diab Rep. 2014;14(10):532.
Smith LB, Kugler BB, Lewin AB, Duke DC, Storch EA, Geffken GR. Executive functioning, parenting stress, and family factors as predictors of diabetes Management in Pediatric Patients with type 1 diabetes using intensive regimens. Childrens Health Care. 2014;43(3):234–52.
McNally K, Rohan J, Pendley JS, Delamater A, Drotar D. Executive functioning, treatment adherence, and glycemic control in children with type 1 diabetes. Diabetes Care. 2010;33(6):1159–62.
Hagger V, Hendrieckx C, Sturt J, Skinner TC, Speight J. Diabetes distress among adolescents with type 1 diabetes: a systematic review. Curr Diab Rep. 2016;16(1):9.
Hood KK, Iturralde E, Rausch J, Weissberg-Benchell J. Preventing diabetes distress in adolescents with type 1 diabetes: results 1 year after participation in the STePS program. Diabetes Care. 2018;41(8):1623.
Lašaitė L, Dobrovolskienė R, Danytė E, Stankutė I, Ražanskaitė-Virbickienė D, Schwitzgebel V, et al. Diabetes distress in males and females with type 1 diabetes in adolescence and emerging adulthood. J Diabetes Complicat. 2016;30(8):1500–5.
Miller MM, Rohan JM, Delamater A, Shroff-Pendley J, Dolan LM, Reeves G, et al. Changes in executive functioning and self-Management in Adolescents with Type 1 diabetes: a growth curve analysis. J Pediatr Psychol. 2013;38(1):18–29.
Stupiansky NW, Hanna KM, Slaven JE, Weaver MT, Fortenberry JD. Impulse control, diabetes-specific self-efficacy, and diabetes management among emerging adults with type 1 diabetes. J Pediatr Psychol. 2013;38(3):247–54.
Bagner DM, Williams LB, Geffken GR, Silverstein JH, Storch EA. Type 1 diabetes in youth: the relationship between adherence and executive functioning. Childrens Health Care. 2007;36(2):169–79.
Perez KM, Patel NJ, Lord JH, Savin KL, Monzon AD, Whittemore R, et al. Executive function in adolescents with type 1 diabetes: relationship to adherence, glycemic control, and psychosocial outcomes. J Pediatr Psychol. 2017;42(6):636–46.
Hughes AE, Berg CA, Wiebe DJ. Emotional processing and self-control in adolescents with type 1 diabetes. J Pediatr Psychol. 2012;37(8):925–34.
Graziano PA, Geffken GR, Williams LB, Lewin AB, Duke DC, Storch EA, et al. Gender differences in the relationship between parental report of self-regulation skills and adolescents' management of type 1 diabetes. Pediatr Diabetes. 2011;12(4 Pt 2):410–8.
Hall PA, Fong GT, Cheng AY. Time perspective and weight management behaviors in newly diagnosed type 2 diabetes: a mediational analysis. J Behav Med. 2012;35(6):569–80.
Sansbury B, Dasgupta A, Guthrie L, Ward M. Time perspective and medication adherence among individuals with hypertension or diabetes mellitus. Patient Educ Couns. 2014;95(1):104–10.
Schacter DL, Benoit RG, Szpunar KK. Episodic future thinking: mechanisms and functions. Curr Opin Behav Sci. 2017;17:41–50.
Andre L, van Vianen AE, Peetsma TT, Oort FJ. Motivational power of future time perspective: meta-analyses in education, work, and health. PLoS One. 2018;13(1):e0190492.
Johnson SR, Blum RW, Cheng TL. Future orientation: a construct with implications for adolescent health and wellbeing. Int J Adolesc Med Health. 2014;26(4):459–68.
Kieckhefer GM, Trahms CM. Supporting development of children with chronic conditions: from compliance toward shared management. Pediatr Nurs. 2000;26(4):354–63.
Young MT, Lord JH, Patel NJ, Gruhn MA, Jaser SS. Good cop, bad cop: quality of parental involvement in type 1 diabetes management in youth. Curr Diab Rep. 2014;14(11):546.
Berg CA, Butner J, Wiebe DJ, Lansing AH, Osborn P, King PS, et al. Developmental model of parent-child coordination for self-regulation across childhood and into emerging adulthood: type 1 diabetes management as an example. Dev Rev. 2017;46:1–26.
Powell PW, Hilliard ME, Anderson BJ. Motivational interviewing to promote adherence behaviors in pediatric type 1 diabetes. Curr Diab Rep. 2014;14(10):531.
Jaser SS, Patel N, Linsky R, Whittemore R. Development of a positive psychology intervention to improve adherence in adolescents with type 1 diabetes. J Pediatr Health Care. 2014;28(6):478–85.
Jaser SS, Patel N, Rothman RL, Choi L, Whittemore R. Check it! A randomized pilot of a positive psychology intervention to improve adherence in adolescents with type 1 diabetes. Diab Educ. 2014;40(5):659–67.
Fortenberry KT, Butler JM, Butner J, Berg CA, Upchurch R, Wiebe DJ. Perceived diabetes task competence mediates the relationship of both negative and positive affect with blood glucose in adolescents with type 1 diabetes. Ann Behav Med. 2009;37(1):1–9.
Strait GG, McQuillin S, Smith B, Englund JA. Using motivational interviewing with children and adolescents: a cognitive and neurodevelopmental perspective. Adv School Ment Health Promot. 2012;5(4):290–304.
Steiger RM, Stoddard SA, Pierce J. Adolescents' future orientation and nonmedical use of prescription drugs. Addict Behav. 2017;65:269–74.
Chan A-W, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin JA, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586.
Collins LM, Murphy SA, Strecher V. The multiphase optimization strategy (MOST) and the sequential multiple assignment randomized trial (SMART): new methods for more potent eHealth interventions. Am J Prev Med. 2007;32(5 Suppl):S112–S8.
Daniel TO, Said M, Stanton CM, Epstein LH. Episodic future thinking reduces delay discounting and energy intake in children. Eat Behav. 2015;18:20–4.
Rung JM, Madden GJ. Demand characteristics in episodic future thinking II: the role of cues and cue content in changing delay discounting. Exp Clin Psychopharmacol. 2019;27(5):482.
Prinsloo GE, Rauch HG, Karpul D, Derman WE. The effect of a single session of short duration heart rate variability biofeedback on EEG: a pilot study. Appl Psychophysiol Biofeedback. 2013;38(1):45–56.
Pawlow LA, Jones GE. The impact of abbreviated progressive muscle relaxation on salivary cortisol. Biol Psychol. 2002;60(1):1–16.
Lloyd A, Brett D, Wesnes K. Coherence training in children with attention-deficit hyperactivity disorder: cognitive functions and behavioral changes. Altern Ther Health Med. 2010;16(4):34–42.
Jaeggi SM, Buschkuehl M, Jonides J, Shah P. Short- and long-term benefits of cognitive training. Proc Natl Acad Sci U S A. 2011;108(25):10081–6.
Katz B, Jaeggi S, Buschkuehl M, Stegman A, Shah P. Differential effect of motivational features on training improvements in school-based cognitive training. Front Hum Neurosci. 2014;8:242.
Jones MR, Katz B, Buschkuehl M, Jaeggi SM, Shah P. Exploring N-Back cognitive training for children with ADHD. J Atten Disord. 2018. https://doi.org/10.1177/1087054718779230.
Eisenberg IW, Bissett PG, Zeynep Enkavi A, Li J, MacKinnon DP, Marsch LA, et al. Uncovering the structure of self-regulation through data-driven ontology discovery. Nat Commun. 2019;10(1):2319.
Koffarnus MN, Bickel WK. A 5-trial adjusting delay discounting task: accurate discount rates in less than one minute. Exp Clin Psychopharmacol. 2014;22(3):222–8.
Joireman J, Shaffer MJ, Balliet D, Strathman A. Promotion orientation explains why future-oriented people exercise and eat healthy:evidence from the two-factor consideration of future Consequences-14 scale. Personal Soc Psychol Bull. 2012;38(10):1272–87.
Salsman JM, Butt Z, Pilkonis PA, Cyranowski JM, Zill N, Hendrie HC, et al. Emotion assessment using the NIH toolbox. Neurology. 2013;80(11 Suppl 3):S76–86.
Brown LK, Houck C, Lescano C, Donenberg G, Tolou-Shams M, Mello J. Affect regulation and HIV risk among youth in therapeutic schools. AIDS Behav. 2012;16(8):2272–8.
Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54(6):1063–70.
D. W. Wechsler Intelligence Scale for Children - WISC-IV: Psychological Corporation; 2003.
Wessel JR. Prepotent motor activity and inhibitory control demands in different variants of the go/no-go paradigm. Psychophysiology. 2018;55(3). https://doi.org/10.1111/psyp.12871.
Gioia GA, Isquith PK, Retzlaff PD, Espy KA. Confirmatory factor analysis of the behavior rating inventory of executive function (BRIEF) in a clinical sample. Child Neuropsychol. 2002;8(4):249–57.
Lewin AB, LaGreca AM, Geffken GR, Williams LB, Duke DC, Storch EA, et al. Validity and reliability of an adolescent and parent rating scale of type 1 diabetes adherence behaviors: the self-care inventory (SCI). J Pediatr Psychol. 2009;34(9):999–1007.
Campbell MS, Schatz DA, Chen V, Wong JC, Steck A, Tamborlane WV, et al. A contrast between children and adolescents with excellent and poor control: the T1D exchange clinic registry experience. Pediatr Diabetes. 2014;15(2):110–7.
Dahl RE, Vanderschuren LJMJ. The feeling of motivation in the developing brain. Dev Cogn Neurosci. 2011;1(4):361–3.
Nielsen L, Riddle M, King JW, Aklin WM, Chen W, Clark D, et al. The NIH science of behavior change program: transforming the science through a focus on mechanisms of change. Behav Res Ther. 2018;101:3–11.
Acknowledgements
We would like to acknowledge Leonard H. Epstein, PhD and his lab at the University at Buffalo Department of Pediatrics, Jacobs School of Medicine and Biomedical Sciences, who helped train our team in their Episodic Future Thinking intervention techniques, and other fellow SOBC Network scientists for assistance with measurement and scientific discussions.
Funding
This protocol was peer-reviewed as part of the grant award process. This research was supported by the National Institutes of Health (NIH) Science of Behavior Change (SOBC) Common Fund Program through awards administered by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD UH2HD087979 and UH3HD087979), and NICHD T32HD079350 and F32HD100025. The opinions expressed herein and the interpretation and reporting of these data are the responsibility of the authors and in no way should be seen as an official recommendation, interpretation, or policy of the National Institutes of Health or the US government.
Author information
Authors and Affiliations
Contributions
ALM designed the study, directed the planned data acquisition, and wrote the first draft of the manuscript; SLL conducted intervention activities and gave substantive feedback on the manuscript; DA pediatric endocrinology recruitment strategies, assisted with intervention development, and gave substantive feedback on the manuscript; JL oversaw pediatric endocrinology recruitment strategies and gave substantive feedback on the manuscript; CH gave substantive feedback on the manuscript; KWB assisted with data acquisition plans and gave substantive feedback on the manuscript; RK gave substantive feedback on the manuscript; KMC assisted with project management and gave substantive feedback on the manuscript; KC conducted intervention activities and gave substantive feedback on the manuscript; NK developed data analysis plans and gave substantive feedback on the manuscript; BK provided input on the EF intervention and gave substantive feedback on the manuscript; EMF helped to design the study, direct the planned data acquisition, and gave substantive feedback on the manuscript. All authors read and approved the final manuscript and agree to be accountable for their contributions.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this study was provided by the Institutional Review Board of the University of Michigan (HUM00148853). A parent/primary caregiver for each child provided written informed consent for their child and themselves to participate in the study. Youth provided written assent for themselves.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
SPIRIT Checklist: Recommended items to address in a clinical trial protocol and related documents.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Miller, A.L., Lo, S.L., Albright, D. et al. Adolescent Interventions to Manage Self-Regulation in Type 1 Diabetes (AIMS-T1D): randomized control trial study protocol. BMC Pediatr 20, 112 (2020). https://doi.org/10.1186/s12887-020-2012-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-020-2012-7