
Abstract
Background
Evaluating the effects of cancer diagnosis and treatment on a patient’s overall well-being is crucial and health-related quality of life (HRQoL) is a reliable metric for assessing this impact. Little is known about HRQoL among cancer survivors across various stages and treatments. The study examined individual and clinical factors influencing HRQoL among cancer survivors.
Methods
A cross-sectional study was conducted in two specialised cancer care hospitals in Dhaka, Bangladesh. Cancer-diagnosed adults receiving treatment at selected hospitals from January to May 2022 were enrolled. The 5-level EuroQol-5 Dimensions version (EQ-5D-5L) instrument was used to collect HRQoL data. HRQoL scores were derived using UK value sets. The investigation used a multivariable Tobit regression model to determine the association between independent variables and HRQoL scores.
Results
A total of 607 adult patients were enrolled, with 55% being females and 66% aged 36 to 64 years. Reported health problems in five EQ-5D domains include mobility (11%), self-care (11%), usual daily activities (19%), pain/discomfort (21%), and anxiety/depression (46%). Patients with throat, brain, lung, blood, and liver cancer had lower utility scores. Advanced-stage cancer survivors had lower utility scores (β = -49 units, 95% codfidence interval [CI]: -0.75 to -0.22) compared to early-stage survivors. Physically inactive survivors had lower utility scores by 0.41 units (95% CI: -0.51 to -0.30) compared to their counterparts. Private hospital patients had higher utility scores, whereas patients belonged to poor socioeconomic groups scored worse than wealthier ones.
Conclusions
This study highlights the impact of clinical and individual characteristics on HRQoL among cancer survivors. These findings advocate for an enhanced Bangladeshi cancer patient care model through timely interventions or programs, early detection or diagnosis, tailored treatments, and the promotion of physical activity to bolster HRQoL outcomes.
Similar content being viewed by others


Introduction
Cancer poses a significant challenge worldwide and is a major barrier to increasing life expectancy [1]. According to the 2020 Global Cancer Observatory report, approximately 19.3 million new cases were reported, resulting in around 10 million cancer-related deaths [2]. The increasing burden of cancer incidence and mortality, particularly in low- and middle-income countries (LMICs), highlights the urgency of addressing rising concerns [3]. Like other LMICs, Bangladesh has seen a rise in the number of cancer cases, with 156,775 new cancer cases and 108,990 cancer-related mortality reported in 2020 [4].
High-income countries have seen higher survival rates due to high-quality and cost-effective cancer screening, timely diagnoses, improved therapeutic treatment modalities, and accessible routine follow-up care services [5]. However, many LMICs, including Bangladesh, struggle with lower cancer survival rates due to deficiencies in screening programs and suboptimal cancer management initiatives [6]. Since cancer is a chronic disease that requires persistent treatments, it can adversely impact the quality of life of cancer patients [7, 8]. The treatment phases involve a number of physical and psychosocial challenges for patients, which can affect their quality of life [9,10,11]. Additionally, pre-existing medical conditions/diseases coupled with adverse effects of cancer treatments can severely reduce survivors' functional capacity and overall quality of life [9, 12, 13].
Patient-centric HRQoL has emerged as an important metric and gained recognition as a measurable health outcome in clinical trials and strategies for clinical practice improvement [14,15,16]. Understanding patients’ HRQoL and functional capacity is vital for clinicians because this insight provides prognostic cues and sheds light on patients’ resilience to cancer treatment modalities [14]. Additionally, it helps in identifying specific challenges that might influence treatment decisions, facilitating adapted care for cancer survivors.
The EuroQol-5 dimensions instrument (EQ-5D-5L) has gained popularity as a method to assess HRQoL among cancer survivors in clinical settings [17,18,19,20]. Identifying HRQoL challenges in EQ-5D-5L domains not routinely assessed holds the potential for refining risk mitigation strategies, improving treatment procedures, and increasing survival rates [20, 21]. Therefore, HRQoL insights regarding cancer survivors are essential within clinical practices, offering a better understanding of how HRQoL is shaped by cancer site and stage during treatment. However, the specific relationship between these variables remains largely unexplored in Bangladesh. Therefore, attention to the HRQoL of cancer patients across all stages, focusing not solely on survival but also on systemic treatment-related experiences, is important.
Exploring HRQoL among cancer survivors throughout treatment holds profound implications, aligning with the Sustainable Development Goals (SDGs), particularly target 3.4 aimed at reducing premature death [22]. This exploration informs the development of clinical strategies to alleviate cancer burden, optimise functional capacity, and improve HRQoL. Furthermore, understanding how HRQoL outcomes vary with sociodemographic and clinical factors can offer insights to shape clinical practice, health policy, and appropriate healthcare interventions.
To address these imperatives, this study formulates two specific research questions (RQs):
-
RQ1: What is the distribution of HRQoL among Bangladeshi cancer survivors during systemic and radiotherapy periods, categorised by cancer stages and tumor sites?
-
RQ2: What person and clinical characteristics are associated with increased or decreased HRQoL?
Methods
Study design and settings
A cross-sectional study design was adopted to investigate HRQoL among cancer patients during systemic and radiation therapy. The survey was conducted at the outpatient departments of the two largest cancer management hospitals in Dhaka, Bangladesh. To ensure geographical diversity and maximum coverage of patient treatments within a short study period, we selected the National Institute of Cancer Research & Hospital (NICRH), a government-funded national cancer research and treatment health facility. This 300-bed tertiary care public hospital offers multidisciplinary cancer care. According to hospital records, 83,795 new patients received systemic and radiotherapy treatments from January 2018 to December 2020, coming from eight different administrative divisions in Bangladesh. To capture diverse healthcare settings and multidisciplinary cancer care, we also chose Ahsania Mission Cancer Hospital, a privately funded 50-bed tertiary care hospital that provides advanced cancer care services, and approximately 100 cancer patients visit the hospital's outpatient department each day.
The study hospitals are located in the country’s capital city, where people commonly come for treatment due to availability and potential access to better healthcare facilities for cancer.
Study participants and survey procedures
The study population was cancer patients in Bangladesh with the following inclusion criteria: (i) age at diagnosis equal to or more than 18 years, (ii) receiving treatment, (iii) able to respond to the questions, and (iv) willing to participate in the study. Written consent was taken from each participant prior to the survey. For the illiterate or those with no education, interviewers read the consent document, explained the research details to the participants and approached adult caregivers as witnesses to attest to the prospective subject's apparent understanding and willingness to participate. Then, the subject used a tick mark instead of a signature, and a witness signed the consent form, attesting that the subject agreed to participate.
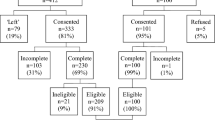
Data were collected through face-to-face interviews by trained interviewers between 1st January and 30th May 2022. A team of two doctors and three medical students conducted the interviews. Before data collection, 3-day training was provided to interviewers about the content of the questionnaire, ethical issues, privacy concerns, and risk management for cancer patients. Following that, the questionnaire was piloted with 24 patients and modified and finalised upon feedback. Eligible patients who were attending the hospital were approached to participate, and daily recruitment was conducted. Upon receiving consent, interviewers confirmed the patients' cancer status by reviewing diagnostic reports (biopsy, CT scan, MRI, X-ray, prescription, etc.). The required minimum sample size was 376 at 90% power, 95% confidence interval [CI] of 0.05 to 1.96, with 53.76% of patients had poor quality of life [23], and the margin of error was 5%. We had an opportunity to collect data from 607 cancer survivors through face-to-face interviews (response rate was 86%). An interview was conducted in a separate place from the patient waiting areas or rooms. Every interview was completed within ~ 10 to15 minutes. Each completed questionnaire was spot-checked by the first author (MS) to assess the accuracy, completeness, and consistency of the data collected. The respondents were not given any financial benefits for participating in the study. Data selection, identification and inclusion flow diagram process are presented in Appendix 1.
Outcome measures
This study examined HRQoL as the primary outcome measure using the EQ-5D-5L in English [24]. The EQ-5D-5L has been a widely used instrument for assessing HRQoL among cancer patients with poor health [20, 25, 26]. The EQ-5D-5L has superior measurement properties compared to EQ-5D-3L [21]. It contains five domains (mobility, self-care, usual activities, pain or discomfort and anxiety or depression), with each having five levels (no problems, some problems, moderate problems, severe problems or extreme problems) [27]. The instrument also rates overall health using EQ-VAS and has been translated into 130 languages [24, 27]. This instrument can be self-administered, and respondents also rate their overall health on the day of the interview on a 0–100 hash-marked, vertical visual analogue scale known as the EuroQol-visual analogue scale (EQ-VAS).
Cancer sites and stages
Various pertinent clinical attributes were taken into account for examination, encompassing the specific site and stage of the diagnosed cancer. Detailed information regarding the diagnosed cancer's typology and its corresponding stage was garnered from the patient's comprehensive pathological diagnostic reports or treatment protocols. Among the spectrum of diagnosed cancers, prevalent categories included oral, breast, blood, pancreatic, liver, lung, brain, throat, and cervical, as well as other diverse tumor sites (such as ocular, cutaneous, osseous, penile, and ovarian malignancies).
Covariates
The analytical explorations encompassed a range of covariates, including individual-level socioeconomic, demographic, lifestyle, and clinical variables. Sociodemographic variables include gender (male vs. female), age categories (18–35, 36–45, 46–64, and > 64 years), body-mass-index [BMI] (underweight: < 18.49 kg/m2, healthy weight: 18.50–24.99 kg/m2, overweight: 25–29.99 kg/m2, and obese: ≥ 30 kg/m2), marital status (single/ never married, married, and widowed or divorced or seperated), education (no education, primary: 1–5 years, secondary: 6–10 years, higher secondary: 10–12 years and tertiary: graduate school & above), residence (urban vs. rural), household size (< 4, 4–5 and ≥ 6 members), occupation (unemployed, employed, business, informal workers, housewife, student and other occupations), and monthly household income distributed from the lowest quintile (20% lowest quintile [Q1: poorest] to 20% highest quintile [Q5: richest]). Lifestyle aspects were accounted for through variables such as smoking status (yes vs. no), use of smokeless tobacco: betel leaf with areca nut, zarda, sadapata, and gul (yes vs. no), and adherence to physical activity recommendations: walk > 150 min per week (yes vs. no). Lastly, clinical attributes involving the cancer site and stage, along with the healthcare facility responsible for ongoing treatment (public facility vs. private facility), were encompassed.
Statistical analysis
Descriptive statistics were presented employing frequency and percentages, or mean and standard deviation, as appropriate. Health utility scores were generated from the UK tariff corresponding to each dimension and level of the EQ-5D-5L tool [28], constituting the primary outcome variable. These mean scores were stratified across patients' distinctive attributes and cancer stages. We applied a single imputation method to replace missing data with a single predicted value for estimating health utilities, such as the mean for a given case [29]. To appraise the bivariate relationship between EQ-5D health states and cancer stage, chi-squared tests were employed, with Fisher's exact chi-squared test applied if feasible.
HRQoL data often have a limited range, constrained between a lower boundary (worst health state) and an upper boundary (best health state). Tobit models can accommodate these boundary restrictions, ensuring that the estimated coefficients and predictions stay within the feasible range of HRQoL scores. Unadjusted and adjusted multivariate tobit regression models were used to find the factors influencing patient health utility scores. In the adjusted model, predictor variables were integrated solely if any label of the predictor demonstrated significance at a risk threshold of ≤ 5% in the unadjusted regression model. This adjustment was undertaken to counteract the influence of other potential factors. The analysis was executed using the STATA-15 statistical software (Stata Corp LP, College Station, TX, USA).
Results
Participant’s sociodemographic characteristics
A total of 607 cancer survivors were enrolled. Among them, 55% were female, 44% aged between 46 and 64 years, 88% resided in rural areas, and 88% receiving care at a public health facility. Nearly half (47%) of cancer survivors reported no formal education and 34% belonged to economically disadvantaged households. Active workforce participation was found to be low, with 23% being unemployed, and 41% identifying as housewives. About 70% of cancer survivors engaged in regular physical activity. Common cancer diagnoses included cervical (20%), breast (18%), oral (11%), and lung (11%) cancers and 42% of patients were diagnosed with stage I (Table 1).
Health state using EQ-5D-5L dimensions by stages of cancer
Table 2 represents the various health states within the EQ-5D-5L domains, considering different cancer stages. Patients' health states deteriorated as cancer progressed, leading to significant differences in HRQoL between those with advanced-stage (stage IV) cancer and those with early-stage (stage I) cancer. For instance, patients with advanced-stage cancer reported more severe or extreme problems in all five dimensions compared to early-stage counterparts (mobility [25.00% vs. 0.00%]; self-care [28.13% vs. 10.00%]; daily activities [34.38% vs. 20.00%], pain or discomfort [34.38% vs. 10.00%], and anxiety/depression [56.26% vs. 25.00%]).
A notable percentage of survivors (45.80%) encountered severe or extreme problems of anxiety/depression. Additionally, approximately 21% reported experiencing severe or extreme pain/discomfort, with 19% facing challenges in their daily activities. Across all EQ-5D-5L dimensions—specifically, mobility, self-care, usual activities, and pain/discomfort—a statistically significant association with cancer stage was established (p < 0.05), highlighting the effects of cancer progression on HRQoL outcomes.
Distribution of HRQoL
Table 3 shows EQ-5D-5L scores, showing that cancer site and stage are associated with HRQoL scores. Notably, HRQoL mean scores were lower among survivors afflicted with throat [mean = 0.46, (SD = 0.33)], brain [0.40, (0.36)], lung [0.46, (0.35)], blood [0.48, (0.32)], and liver cancer [0.48, (0.32)] in contrast to those grappling with breast [0.65, (0.25)], pancreas [0.65, (0.39)], oral [0.61, (0.24)], and cervical cancer [0.59 (0.31)]. HRQoL scores decreased with advanced cancer stages and were significantly lower for certain types of cancer. Private health facility and healthy lifestyle factors were associated with higher HRQoL scores. HRQoL scores tend to increase with higher education levels, affluent income brackets, smaller family sizes, and urban residence.
We found that HRQoL scores decrease with the progression of cancer stages. For instance, survivors confronting throat cancer displayed notably higher HRQoL scores at an early stage compared to an advanced stage (stage 0 = 0.85 vs. stage IV = 0.30). This trend persisted among survivors with brain cancer (stage 0 = 0.84 vs. stage III = 0.35) and breast cancer (stage I = 0.68 vs. stage IV = 0.61). Comparable patterns emerged for pancreatic (stage 0 = 0.86 vs. stage IV = 0.20), oral (stage 0 = 0.68 vs. stage IV = 0.47), and cervical cancer survivors (stage 0 = 0.73 vs. stage IV = 0.63). Important differences surfaced concerning HRQoL scores attributed to treatment facilities, where mean scores were markedly higher among patients treated in a private health facility (0.72 vs. public hospital = 0.55).
Factors influencing health utility scores
The outcomes of the tobit regression model, presented in Table 4, revealed the important predictors influencing health utility scores. We found a statistically significant decrement in HRQoL scores among survivors with advanced-stage cancer (stage IV) (β = -0.49, 95% CI: -0.75 to -0.22) compared to patients with early-stage cancer (stage 0). Additionally, physically inactive cancer survivors had significantly lower utility scores (β = -0.41, 95% CI: -0.51 to -0.30) compared to their physically active counterparts. Furthermore, patients receiving treatment in private healthcare showed significantly higher utility scores (β = 0.35, 95% CI: 0.23 to 0.48) relative to those treated in public hospitals. No significant association was found between HRQoL scores and cancer site, gender, education, marital status, residence, or family composition.
Discussion
The current study examined HRQoL within the cohort of cancer survivors in Bangladesh, offering insights into the dynamic interplay between cancer site, stage, and HRQoL trajectories during systemic and radiation therapy. Findings revealed that HRQoL scores differ for cancer survivors based on cancer sites and stages. For instance, the most diminished scores were consistently identified among patients confronted by advanced-stage (stage IV) cancer. Notably, our analysis further underscores the distinct HRQoL profiles associated with varying cancer sites, with throat, brain, lung, blood, and liver cancer survivors encountering markedly lower HRQoL compared to their counterparts diagnosed with breast, pancreatic, oral, or cervical cancer. By substantiating these associations, our study contributes to a more complete understanding of the intricate relationship between cancer characteristics and patients' quality of life outcomes.
Our study has revealed that cancer survivors with advanced-stage (stage IV) had significantly lower HRQoL scores by 0.49 units compared to those who were early-stage (stage-0) survivors. The findings are consistent with prior studies on the relationship between cancer stage and HRQoL, reporting that advanced-stage cancers significantly correlated with worse HRQoL [30, 31]. They also align with the results of a recent meta-analysis that has revealed that patients with stage IV cancer had a 4.92 times higher chance of developing poor HRQoL than those with others [32]. A recent study, however, found that HRQoL was not associated with cancer stage [33]. There are several possible explanations for our findings of lower HRQoL scores among stage-IV cancer patients compared to those with stage-0 cancer. First, this inconsistency according to stage is probably due to the different clinical characteristics of cancers; specifically, potential adverse side effects of the disease are the main domains of HRQoL in various stages of the disease, from non-invasive cancer to a tendency to develop a more advanced-stage (stage IV) cancer [11]. Further research is needed to understand the disproportionate decrease in HRQoL among cancer survivors. The authors urge more awareness of HRQoL cancer survivors and the need to address poor HRQoL in the clinical settings. Second, it is possible that much of the variation in HRQoL occurs during systemic therapy and radiotherapy. This is because HRQoL often falls during the treatment phase due to more fatigue, nausea and vomiting, loss of appetite, and systemic side effects, whereas advanced-stage patients suffer significant functional limitations related to the condition [9, 33, 34]. In other words, HRQoL for patients with advanced-stage cancer is likely affected by the burden of the disease itself and the treatment regimens applied to the disease [7, 33, 35]. Normally, cancer patients with stage 0-II undergo surgery and some receive additional therapy, but patients with stage III & IV cancer most often receive radiation therapy and/or chemotherapy in addition to surgery. Patients undergoing treatment experience a decline in their perceived HRQoL during treatment. It could also indicate a decrease in HRQoL may reflect changes in treatment patterns for late-stage cancers. Therefore, the authors suggest not only a role for multidisciplinary rehabilitation for patients after treatment but also rehabilitation before treatment. Last, it could be due to the fact that the more advanced stage is used as a proxy marker for a poor outcome since the more advanced stage is related to lower HRQoL [9, 10]. In other words, some functional disorders that occur as a result of particular types of treatment, like chemotherapy and immunotherapy, are more likely to result in worse HRQoL [36]. It is pertinent to mention that we assessed the HRQoL of those undergoing systemic therapy and radiotherapy, so there is a high risk of having adverse effects on HRQoL. This is owing to the fact that if the disease is not appropriately treated and controlled, it will worsen over time [31]. Therefore, it is crucial to diagnose cancer at earlier stages for a better treatment outcome and HRQoL.
Specifically, patients with stage IV cancer more commonly reported severe or extreme problems across all EQ-5D domains compared to the first three stages of cancer. Similar results were found in a recent study conducted in Korea has revealed that most cancer patients had severe difficulties in all EQ-5D dimensions [37]. Further, the most frequently reported dimensional problems among cancer survivors were anxiety/depression and pain/discomfort. Conversely, a previous study reported a highly prevalent dimensional problem among cancer survivors were pain/discomfort and mobility [37]. Gao et al. [25] observed that 54.6% of patients reported pain/discomfort, and 41.2% reported anxiety or depression. Conversely, our findings reported 21% of patients suffered from pain/discomfort and 49.1% had anxiety/depression. A possible explanation could be that advanced-stage cancer patients experience a range of symptoms for which standard medical treatments may not provide sufficient relief rather than that systemic therapy and radiotherapy could be contributing to lower HRQoL. In clinical settings, healthcare providers should endeavor to manage these problems to mitigate patients’ symptoms, pain/discomfort, and anxiety/depression by implementing tailored interventions to meet patients’ needs during treatment and when providing healthcare services such as palliative care, particularly for patients at advanced cancer stages.
We found that the HRQoL of cancer survivors differed depending on the cancer site; for example, patients with throat, brain, lung, blood and liver cancer had a lower HRQoL compared to those with breast, pancreatic, oral, and cervical cancer. In a previous study, a similar trend was observed between cancer sites; for example, breast and genital cancer survivors expressed slightly higher HRQoL mean scores than those with cancer in the digestive system [20]. In addition, our study did not find any statistically significant correlation between cancer sites and HRQoL. Contrary to a recent study in Korea, which has shown a statistically significant association between cancer sites and HRQoL [37]. Even though we did not find any significant association between cancer site and HRQoL, it has clinical importance. Therefore, we suggest conducting further studies to identify factors associated with HRQoL differences between cancer sites.
According to our study data, patients who received treatment in a private hospital were more likely to attain better HRQoL compared to those in a public hospital. The findings are supported by another study that revealed that cancer patients treated in private hospitals had a comparatively better HRQoL due to better facilities, advanced treatment modalities, and technologies [38]. There is a significant difference between the cost of care in government-facilitated centers and private centers, which might affect the quality of care as well as the quality of life. In Bangladesh, the public sector provides not-for-profit services that include preventive, curative, promotional, and rehabilitative services. In contrast, the private sector providers are mostly for-profit curative services that operate in urban areas, mainly in the capital city of Dhaka and other major cities. Due to the high cost of private hospitals, most people can’t afford to go there for treatment [39]. The private sector hospitals give the highest priority to serving their patients and try to employ more providers than the public sector. Alarmingly, many doctors employed in the public sector of Bangladesh are sometimes engaged in the private sector as well, which reduces the service capacity of public hospitals [40]. Therefore, the respective authorities should revisit cancer centers for quality care and increase the capacity to afford more cancer patients in public healthcare facilities. The government can ban joint public/private practices because they interfere with public sector efficiency, as well as increase allowances and incentives for public sector employees to ensure quality care. The authors propose the urgent need to formulate a National Cancer Policy encompassing early detection, affordable care, and comprehensive supportive care through well-defined care pathways at public health facilities.
This study has several important clinical, research and policy implications. The current study highlights the declining HRQoL of cancer patients. With treatment and care now becoming more patient-centered, it has become more pertinent to understand the impact of cancer treatments in the advanced stages on the HRQoL of patients. The effect of treatment for certain cancers may be extreme and may involve a great deal of HRQoL. Therefore, the authors stress the importance of conducting research to observe changes in symptoms and HRQoL among cancer patients at different stages of the disease. To better understand how HRQoL varies among cancer stages, future research could be initiated to examine patient HRQoL before, during, and after treatment.
Strengths and limitations
Our study addresses an unexplored avenue within the field of cancer research in Bangladesh. To our knowledge, no prior investigations have undertaken an inclusive examination of HRQoL encompassing all cancer sites and stages during treatment. The study offers a comprehensive perspective by including patients from diverse geographical regions from the country's most prominent public and private cancer hospitals.
The present study, despite its contributions, has some limitations. Firstly, its cross-sectional design inherently poses the risk of selection bias, underscoring the need for a cautious interpretation of the results. Secondly, while the assessment of HRQoL during treatment provides valuable insights, the comprehensive evaluation could be enriched by encompassing pre-treatment and post-treatment stages within the same cohort. Moreover, the absence of EQ-VAS scores as a measure of HRQoL limits the comprehensive evaluation of this multifaceted construct. Further, reliance on self-reported cancer diagnosis, site, and treatment history may entail potential reporting biases. Lastly, the study's age criterion (18 years and above) excludes the exploration of HRQoL among cancer patients below 18 years old, signifying a scope for further research to encompass this demographic segment.
Conclusion
The findings highlight the significant influence of cancer stage and site on survivors' overall HRQoL, with those with advanced-stage disease reporting lower HRQoL scores compared to early-stage survivors. Specifically, survivors of brain, throat, lung, blood, and liver cancer appear to face greater challenges in maintaining HRQoL. Moreover, findings revealed that physically inactive patients with advanced-stage cancer experienced notably lower HRQoL utility scores. This highlights the potential benefits of incorporating physical activity into cancer care strategies, particularly for those facing advanced disease. Survivors who received treatment in a private hospital reported higher HRQoL utility scores compared to their counterparts treated in a public hospital. This observation raises questions about potential disparities in care quality in health facilities and suggests avenues for targeted improvements.
The study emphasises the importance of routine HRQoL assessments for cancer patients, offering a valuable tool for identifying individuals at risk of poor HRQoL outcomes. This proactive approach enables clinicians to tailor interventions, potentially enhancing patients' overall well-being. To facilitate future research on HRQoL among cancer survivors, more cancer centers and an equal number of data from public and private health facilities must be included for better findings.
Availability of data and materials
The data used and/or analysed during the current study are available upon reasonable request from the corresponding author.
Abbreviations
- HRQoL:
-
Health-related quality of life
- LIMCs:
-
Low- and middle-income countries
- SDG:
-
Sustainable Development Goal
- SD:
-
Standard deviation
- EQ-5D-5L:
-
EuroQol-5D-5L
References
The World Health Organization. Cancer. 2022. https://www.who.int/news-room/fact-sheets/detail/cancer. Accessed 22 Nov 2022.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–49.
Kocarnik JM, Compton K, Dean FE, Fu W, Gaw BL, Harvey JD, et al. Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019 a systematic analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022;8:420–44.
Global Cancer Observatory: Bangladesh Fact Sheet; 2020. https://www.who.int/publications/m/item/cancer-bgd-2020. Accessed 15 Aug 2023.
Allemani C, Weir HK, Carreira H, Harewood R, Spika D, Wang XS, et al. Global surveillance of cancer survival 1995–2009: Analysis of individual data for 25 676 887 patients from 279 population-based registries in 67 countries (CONCORD-2). The Lancet. 2015;385:977–1010.
Cancer on the Global Stage: Incidence and Cancer-Related Mortality in Bangladesh - The ASCO Post. https://ascopost.com/issues/february-25-2017/cancer-on-the-global-stage-incidence-and-cancer-related-mortality-in-bangladesh/. Accessed 15 Aug 2023.
Sibeoni J, Picard C, Orri M, Labey M, Bousquet G, Verneuil L, et al. Patients’ quality of life during active cancer treatment: a qualitative study. BMC Cancer. 2018;18(1):951.
Schulte FSM, Chalifour K, Eaton G, Garland SN. Quality of life among survivors of adolescent and young adult cancer in Canada: a Young Adults With Cancer in Their Prime (YACPRIME) study. Cancer. 2021;127:1325–33.
Blagden SP, Cook AD, Poole C, Howells L, McNeish IA, Dean A, et al. Weekly platinum-based chemotherapy versus 3-weekly platinum-based chemotherapy for newly diagnosed ovarian cancer (ICON8): quality-of-life results of a phase 3, randomised, controlled trial. Lancet Oncol. 2020;21:969–77.
Sureda A, Fumadó L, Ferrer M, Garín O, Bonet X, Castells M, et al. Health-related quality of life in men with prostate cancer undergoing active surveillance versus radical prostatectomy, external-beam radiotherapy, prostate brachytherapy and reference population: a cross-sectional study. Health Qual Life Outcomes. 2019;17(1):11.
Voon PJ, Cella D, Hansen AR. Health-related quality-of-life assessment of patients with solid tumors on immuno-oncology therapies. Cancer. 2021;127:1360–8.
de Boer SM, Powell ME, Mileshkin L, Katsaros D, Bessette P, Haie-Meder C, et al. Toxicity and quality of life after adjuvant chemoradiotherapy versus radiotherapy alone for women with high-risk endometrial cancer (PORTEC-3): an open-label, multicentre, randomised, phase 3 trial. Lancet Oncol. 2016;17:1114–26.
Ganz PA, Hays RD, Spritzer KL, Rogatko A, Ko CY, Colangelo LH, et al. Health-related quality of life outcomes after neoadjuvant chemoradiotherapy for rectal cancer in NRG Oncology/NSABP R-04. Cancer. 2022;128:3233–42.
Buiting HM, Olthuis G. Importance of quality-of-life measurement throughout the disease course. JAMA Netw Open. 2020;3:e200388.
Zheng S, He A, Yu Y, Jiang L, Liang J, Wang P. Research trends and hotspots of health-related quality of life: a bibliometric analysis from 2000 to 2019. Health Qual Life Outcomes. 2021;19:5–8.
Zapatero A, Pijoan XM, Gómez-Caamaño A, Masferrer JP, Hernández VM, Morón AH, et al. Health-related quality of life in men with localized prostate cancer treated with radiotherapy: validation of an abbreviated version of the expanded prostate cancer index composite for clinical practice in Spain. Health Qual Life Outcomes. 2021;19:4–6.
Devlin N, Herdman M, Pavesi M, Phung D, Naidoo S, Beer TM, et al. Health-related quality of life effects of enzalutamide in patients with metastatic castration-resistant prostate cancer: an in-depth post hoc analysis of EQ-5D data from the PREVAIL trial. Health Qual Life Outcomes. 2017;15(1):130.
Verrill M, Wardley AM, Retzler J, Smith AB, Bottomley C, NíDhochartaigh S, et al. Health-related quality of life and work productivity in UK patients with HER2-positive breast cancer: a cross-sectional study evaluating the relationships between disease and treatment stage. Health Qual Life Outcomes. 2020;18(1):353.
Su M, Yao N, Shang M, Shen Y, Qin T, Wang J, et al. Frailty and its association with health-related quality of life among older cancer patients: an evidence-based study from China. Health Qual Life Outcomes. 2022;20(1):124.
Pickard AS, Jiang R, Lin HW, Rosenbloom S, Cella D. Using patient-reported outcomes to compare relative burden of cancer: EQ-5D and functional assessment of cancer therapy-general in eleven types of cancer. Clin Ther. 2016;38:769–77.
Thompson AJ, Turner AJ. A comparison of the EQ-5D-3L and EQ-5D-5L. Pharmacoeconomics. 2020;38:575–91.
Sustainable Development Goal 3: Good Health and Well-being | United Nations in Bangladesh. https://bangladesh.un.org/en/sdgs/3. Accessed 11 Jan 2023.
Alam MM, Rahman T, Afroz Z, Chakraborty PA, Wahab A, Zaman S, et al. Quality of life (QoL) of cancer patients and its association with nutritional and performance status: a pilot study. Heliyon. 2020;6:e05250.
EQ-5D-5L. About. Euroqol.org (EQ-5D-5L). https://euroqol.org/. Accessed 11 Sep 2023.
Gao F, Ng GY, Cheung YB, Thumboo J, Pang G, Koo WH, et al. The Singaporean English and Chinese versions of the EQ-5D achieved measurement equivalence in cancer patients. J Clin Epidemiol. 2009;62:206–13.
Kenzik KM, Martin MY, Fouad MN, Pisu M. Health-related quality of life in lung cancer survivors: latent class and latent transition analysis. Cancer. 2015;121:1520–8.
Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20:1727–36.
Pan T, Mulhern B, Viney R, Norman R, Hanmer J, Devlin N. A comparison of PROPr and EQ-5D-5L value sets. Pharmacoeconomics. 2022;40:297–307.
Gabrio A, Mason AJ, Baio G. Handling missing data in within-trial cost-effectiveness analysis: a review with future recommendations. PharmacoEconomics - Open. 2017;1:79–97.
Ramsey SD, Andersen MR, Etzioni R, Moinpour C, Peacock S, Potosky A, et al. Quality of life in survivors of colorectal carcinoma. Cancer. 2000;88:1294–303.
Liao KC, Chuang HC, Chien CY, Lin YT, Tsai MH, Su YY, et al. Quality of life as a mediator between cancer stage and long-term mortality in nasopharyngeal cancer patients treated with intensity-modulated radiotherapy. Cancers (Basel). 2021;13(20):5063.
Ayalew TL, Wale BG, Haile KE, Zewudie BT, Feleke MG. Health-related quality of life and associated factors among cancer patients in Ethiopia: Systematic review and meta-analysis. PLoS ONE. 2022;17:e0277839.
Ramasubbu SK, Pasricha RK, Nath UK, Rawat VS, Das B. Quality of life and factors affecting it in adult cancer patients undergoing cancer chemotherapy in a tertiary care hospital. Cancer Rep. 2021;4:e1312.
Smyth EN, Shen W, Bowman L, Peterson P, John W, Melemed A, et al. Patient-reported pain and other quality of life domains as prognostic factors for survival in a phase III clinical trial of patients with advanced breast cancer. Health Qual Life Outcomes. 2016;14:1–10.
Fenn KM, Evans SB, McCorkle R, DiGiovanna MP, Pusztai L, Sanft T, et al. Impact of financial burden of cancer on survivors’ quality of life. J Oncol Pract. 2014;10:332–8.
Patel VR, Hussaini SMQ, Blaes AH, Morgans AK, Haynes AB, Adamson AS, et al. Trends in the prevalence of functional limitations among US cancer survivors, 1999–2018. JAMA Oncol. 2023;9(7):1001–3.
Ryu M, Hwang JI. Cancer site differences in the health-related quality of life of Korean cancer survivors: results from a population-based survey. Public Health Nurs. 2019;36:144–54.
Malik M, Rizwan I, Hussain A. Health related quality of life among blood cancer patients in Pakistan: a cross sectional survey. Inquiry. 2021;58:004695802110252.
Rahman T, Gasbarro D, Alam K. Financial risk protection against noncommunicable diseases: trends and patterns in Bangladesh. BMC Public Health. 2022;22(1):1835.
Ansar A, Lewis V, McDonald CF, Liu C, Rahman MA. Factors influencing the timeliness of care for patients with lung cancer in Bangladesh. BMC Health Serv Res. 2023;23(1):261.
Acknowledgements
The authors are grateful to the authorities at the National Institute of Cancer Research & Hospital and Ahsania Mission Cancer and General Hospital, Dhaka, Bangladesh, for allowing them to collect data. Also, the authors want to thank Mohammad Morshad Alam for helping initially. We appreciate the data collection advice provided by Md. Shahnawaz Khan Chandan. We also appreciate the help with data collection from Arifa Sultana, Md. Mahbubul Alam, Md. Mahfuzur Rahman and Md. Sazzadul Mizan Sajal.
Funding
This research did not receive funding from any public, commercial, or not-for-profit agency.
Author information
Authors and Affiliations
Contributions
MS and RAM conceived and designed the experiments. MS and RAM designed the analytical strategy and analysed the data. MS and RAM prepared the draft manuscript. MS, AH, MSu, JG, MEH, SKM, and RAM edited and reviewed the manuscript and contributed to the acquisition, analytical exploration, or interpretation of data for the work. RAM coordinated the whole experiment. MS is responsible for the overall content as guarantor. All authors contributed to the critical revision and approved the submitted version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Written consent was obtained from each study participant before the interview following an explanation of the study's aims and objectives. The informed consent form clearly explained the aims and procedures of the study, the risks and benefits associated with participation, their right to voluntary participation, their right to withdraw from the study, and the anonymity and confidentiality of their data. The ethics committee of North South University, Bangladesh approved the study protocol (Ref-2021/OR-NSU/IRB/0401). For data collection in the hospitals, official permission was obtained from the respective authorities. The study was performed in accordance with the declaration of Helsinki for medical research with human beings.
Consent for publication
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
Cite this article
Shahjalal, M., Sultana, M., Gow, J. et al. Assessing health-related quality of life among cancer survivors during systemic and radiation therapy in Bangladesh: a cancer-specific exploration. BMC Cancer 23, 1208 (2023). https://doi.org/10.1186/s12885-023-11670-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-023-11670-z