
Abstract
Background
Physical activity (PA) interventions have an encouraging role in gestational diabetes mellitus (GDM) management. Digital technologies can potentially be used at scale to support PA. The aim of this study was to assess the feasibility and acceptability of + Stay-Active: a complex intervention which combines motivational interviewing with a smartphone application to promote PA levels in women with GDM.
Methods
This non-randomised feasibility study used a mixed methods approach. Participants were recruited from the GDM antenatal clinic at Oxford University Hospitals. Following baseline assessments (visit 1) including self-reported and device determined PA measurements (wrist worn accelerometer), women participated in an online motivational interview, and then downloaded (visit 2) and used the Stay-Active app (Android or iOS). Women had access to Stay-Active until 36 weeks’ gestation, when acceptability and PA levels were reassessed (visit 3). The primary outcome measures were recruitment and retention rates, participant engagement, and acceptability and fidelity of the intervention. Secondary outcome measures included PA levels, app usage, blood glucose and perinatal outcomes. Descriptive statistics were performed for assessments at study visits. Statistics software package Stata 14 and R were used.
Results
Over the recruitment period (46 weeks), 114 of 285 women met inclusion criteria and 67 (58%) enrolled in the study. Mean recruitment rate of 1.5 participants/clinic with 2.5 women/clinic meeting inclusion criteria. Fifty-six (83%) received the intervention at visit 2 and 53 (79%) completed the study. Compliance to accelerometer measurement protocols were sufficient in 78% of participants (52/67); wearing the device for more than 10 h on 5 or more days at baseline and 61% (41/67) at 36 weeks. There was high engagement with Stay-Active; 82% (55/67) of participants set goals on Stay-Active. Sustained engagement was evident, participants regularly accessed and logged multiples activities on Stay-Active. The intervention was deemed acceptable; 85% of women rated their care was satisfactory or above, supported by written feedback.
Conclusions
This combined intervention was feasible and accepted. Recruitment rates were lower than expected. However, retention rates remained satisfactory and participant compliance with PA measurements and engagement was a high. Future work will explore the intervention’s efficacy to increase PA and impact on clinical outcomes.
Trial registration
The study has received a favourable opinion from South Central—Hampshire B Research Ethics Committee; REC reference: 20/SC/0342. ISRCTN11366562.
Similar content being viewed by others


Introduction
Gestational diabetes mellitus (GDM) is defined as any degree of glucose intolerance first detected during pregnancy [1]. There are serious associated complications for both mother and baby [2,3,4]. Glycaemic control is fundamental to GDM management [5]. Increasing blood glucose concentrations have been suggested as one of the main mechanisms for the increased risk of adverse maternal and infant outcomes [6]. Management interventions include blood glucose monitoring, lifestyle intervention and pharmacological therapy. Of those lifestyle interventions, only dietary modifications and physical activity (PA) have demonstrated possible health benefits for maternal and fetal outcomes [7].
Evidence supporting the benefits of PA amongst women with GDM is growing. Improvements in glycaemic control and reduced insulin requirements has been shown in meta-analyses of PA interventions amongst women with GDM [8, 9]. The National Institute for Health and Care Excellence (NICE), recommends women with GDM to exercise regularly, for example, walking for 30 min after a meal [10]. Women have highlighted their request for clear, simple and specific PA messages with accommodating options [11].
Behaviour Change Techniques (BCTs) are felt to be fundamental to successful PA interventions. A BCT is defined as the smallest “active ingredient” of an intervention. There are 93 internationally agreed and validated BCTs [12]. Techniques such as goal setting and action planning, shaping knowledge and comparison of outcomes have been effective in attenuating the observed decline of PA during pregnancy [13].
Our previous work has shown promise that motivational interviewing (using several BCTs) can help to increase PA in women with GDM [14]. Motivational interviewing was embedded into the routine clinical care for 64 women with GDM. Women were invited to a 20-min individual motivational interview focusing on increasing or maintaining PA during their pregnancy. A specific motivational interviewing framework was used. This included essential micro-skills such as individual goal setting, activity planning and specific information about the benefits and types of recommended PA. A significant increase in self-reported PA levels after two weeks was found [14]. Whilst motivational interviewing provides an initial catalyst for behaviour change, supporting these lifestyle changes remains challenging.
In the UK, many hospital trusts are using digital technologies to support remote monitoring and glycaemic control management [15]. Remote digital devices provide an enlightening prospect to support PA remotely. A smartphone application ‘Stay-Active’, (referred to as the ‘app’) was designed to enhance and support women following the existing motivational interviewing intervention. A systematic approach using the Behaviour Change Wheel (BCW) [16] underpinned the design of this multi-component application. Current evidence, focus groups and input from key stakeholders all informed the development process [17]. Stay-Active delivers ten BCTs through a bespoke educational resource centre, using goal setting and action planning features and tailored performance feedback with individualised messages. A distinctive feature is the clinicians’ ability to interact with the user. Recorded PA can be reviewed by clinicians remotely and specific tailored messages can be sent to users to support their PA levels. This study aimed to determine the feasibility and acceptability of the complex intervention + Stay-Active in women with GDM. + Stay Active combines an initial motivational interview with the smartphone application ‘Stay-Active’ to empower and support women; utilising PA in the management of GDM. This information will determine if a randomised control trial (RCT) to evaluate this intervention is feasible.
Methods
The purpose of the study is to evaluate how women with GDM interact, engage with, and respond to a complex intervention, known as + Stay-Active. The study protocol has been previously published and contains a detailed description of the methods used, study outcomes and progression criteria [18].
Study design
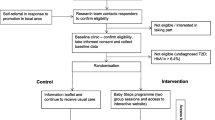
This feasibility study was a non-randomised single arm trial, with all participants receiving the + Stay-Active intervention. A mixed methods approach was used. Figure 1 illustrates a flow chart of the study design, visits, and assessments.

A flow chart of the study design
Setting & study participants
All participants were recruited from National Health Service (NHS) maternity clinics at the Women’s Centre, Oxford University Hospitals NHS Foundation Trust. Pregnant women at least 20 weeks gestation with a confirmed diagnosed of GDM (defined by the testing method used in this NHS hospital at the time of recruitment) were eligible to take part. During recruitment, the diagnosis of GDM was as per the NICE Diabetes in Pregnancy 2015 guideline [19]. From April 2020, the unit adopted the Royal College of Obstetricians & Gynaecologists (UK) guidance [20] during the COVID-19 pandemic. From January 2022 the unit changed to use the NICE thresholds for the 75 g OGTT diagnosis [21]. Recruitment ran from April 2021 to April 2022.
Visit 1: Recruitment and baseline assessments
Women attending the GDM clinic who met the inclusion criteria (see Table 1) were identified by the clinical team at their appointment. Following their clinic appointment, women were invited to enrol on the study. Participants were then asked to complete a baseline assessment of PA using an online version of Pregnancy Physical Activity Questionnaire (PPAQ) [22] and the exercise vital sign assessment (EVS) [23]. Participants wore a tri-axial accelerometer (GENEActiv, Active Insights Ltd, Kimbolton, UK) on their non-dominant wrist for at least seven consecutive days (day and night). This duration of measurement has been shown to provide robust and reliable estimates of moderate to vigorous physical activity (MVPA) during pregnancy [24]. The GENEActiv accelerometer objectively measures and stores movement acceleration in g (the standard SI unit of acceleration) at a high frequency (100 Hz or 100 times per second) for offline analysis, thereby allowing a range of data processing techniques to be applied post data-collection to derive estimates of PA. Participants were provided with an instruction sheet which includes general care instructions.
Intervention
Visit 2: Motivational interview & smartphone app download
At visit 2, within 7 days of enrolment, participants received the + Stay-Active intervention. This involved attending a study visit conducted online (via the secure NHS online platform ‘Attend Anywhere’) or by telephone, depending on participant’s preference. During this visit, participants received a 20-min motivational interview with a trained research midwife and agreed on a set of weekly PA goals. Participants were also encouraged to download the ‘Stay-Active’ smartphone app and were shown the main features which include: recording their activities, reviewing their PA goals, and exploring the resource centre. Following the interview, participants completed the validated modified Oxford Maternity Diabetes Treatment Satisfaction Questionnaire (OMDTSQ) [26] (Supplement material 1) and were also asked to wear the accelerometer for a further week (total of 2 weeks) before returning it to the research team in the post.
All motivational interviews were audio recorded using a dictaphone (where participants consented to this). No patient identifiable data was recorded, the audio-file was labelled with a unique study specific number and transcriptions were de-identified. A randomly selected ten percent of motivational interview recordings were coded using the Motivational Interviewing Treatment Integrity Code (MITI 4.2.1) [27] by an experienced coder to assess the fidelity of the interview. MITI has two components: global summary scores (relational and technical dimensions) and behaviour counts. Global scores capture the coder’s overall impression of how well, or poorly, the interviewer performs in relation to the dimension being measured. Global scores are assigned to a five-point Likert scale with “1” being poor practice, “3” mixed practice, and “5” best practice. Behaviour counts are running tallies of the number of times a particular interview behaviour occurred and these are combined to give a further summary score. % Complex Reflection (%CR) is the percentage of total reflections which are judged complex (> 40% considered fair practice). A further summary of score for behaviour counts is the ratio of Reflections to Questions (R:Q): a 1:1 ratio is considered fair practice and 2:1 good practice.
Participants received a weekly telephone call from a member of the research team to review and adjust their activity goals. Participants were provided with individual motivational feedback messages from the research team at least weekly by text message via the Stay-Active app.
Follow-up assessment & completion of intervention
All participants were asked to attend a follow-up appointment at approximately 36 weeks’ gestation; during follow-up participants completed an online version of PPAQ [22], EVS [23] and OMDTSQ, and were provided with an accelerometer which they were asked to wear for 1 week before returning it to the research team by post. Participants were prompted to complete a feedback form on the intervention via the notifications on Stay-Active. The feedback form compromised of a 5- star rating system and free-text comment box to assess participants rating of goal setting, goal tracking, automated motivational messages and personalised messages about PA. A thematic analysis of the comments, and how these related back to behaviour change techniques and behaviour sources, was performed. Access to the Stay-Active app was terminated 1 week after the routine 36 weeks gestation follow-up appointment. Access was terminated as all data had been collected and support was no longer offered. The planned sample size was 60.
Study outcomes
Primary outcomes
The primary outcomes were the feasibility and acceptability of the intervention to inform a decision on whether a subsequent randomised controlled trial is warranted. They were assessed against a set of predefined criteria (outlined in Fig. 2) related to (i) recruitment and (ii) retention rates, (iii) participant engagement with the intervention, (iv) acceptability and (iv) fidelity of the intervention. A traffic light system was used to determine the progression to a definitive trial. This system has been suggested to be preferable to the stop/go pass/fail approach [28]. The primary objectives with outcome measures, indications of success and timepoints are shown in Table 2 and Fig. 2.

Primary outcome criteria
Secondary outcomes
Secondary outcomes include assessment of PA, usage, and participant attitudes to + Stay- Active; assessment of blood glucose measurements and control, description of maternal and neonatal outcomes, a description of additional health costs and any refinements required of the intervention (Table 2). Further details regarding the secondary outcome can be found in this study’s protocol publication [18].
Statistics & analysis
The results consisted of descriptive statistics from assessments points. The statistics software packages Stata 14 (StataCorp, Texas, USA) and R (R Statistical Software (v4.1.2; R Core Team 2021) were used. Summary statistics were calculated for all measures. Continuous variables were reported as means, medians, standard deviations, percentiles (when appropriate), maximum and minimum values. Binary variables were reported as counts and percentages. The number of missing values were reported.
Results
Participants demographics
Sixty seven women enrolled in the study, with baseline demographics summarised in Table 3. The mean age of participants was 34 years and 52% were primiparous. Mean booking BMI was 30 kg/m2 and 65% of women classed themselves as of white ethnicity. Mean gestational age at recruitment was 27.5 weeks. Only one participant was taking pharmacological medication for GDM at recruitment.
Primary outcomes
Recruitment and retention rate
Over the 46-week recruitment period, 114 of 295 women met the inclusion criteria and 67 (58%) were enrolled in the study. Mean recruitment rate of 1.5 participants per clinic with 2.5 women per clinic meeting inclusion criteria (mean of 5.8 participant per month). Fifty-six (83%) received the intervention and 53 (79%) completed the study. Fourteen women (21%) who were enrolled in intervention did not complete the study. The majority of withdrawals (11 women) occurred prior to visit 2 with non-attendance to the online motivational interview being cited as the main reason. The three withdraws after visit 2 were related to health reasons (Fig. 3).

Flow chart of participants during the study
The results of the primary outcomes against the purposed traffic light system criteria are shown in Table 4. Recruitment rate only achieved a ‘red criteria’. Within the retention criteria, PPAQ completion and accelerometer wear achieved red and amber respectively. Once women had received the motivational interview; retention rate and engagement levels were high with 94% (53/56) completing the study and 98% (55/56) of participants set goals on Stay-Active In categories for participant engagement and fidelity of the intervention green criteria were achieved in all aspects and described in more detail below.
Participant engagement with the intervention
Accelerometer data was available for analysis of accelerometer wear-time and PA levels for 59 participants invited to wear an accelerometer at baseline. Of these, 50 provided accelerometer data at 36 weeks, although 5 accelerometer files were not included in analyses of wear-time or physical activity levels. Two files could not be processed (likely device failure as data was not recorded). Three others were excluded: one was not worn at all during the measurement period, one returned implausibly high values for movement acceleration consistent with device malfunction, and one participant wore the device while an inpatient in hospital and thus it was considered that their data would not represent free-living compliance with measurement protocols or typical physical activity. Compliance to accelerometer measurement protocols was good with 78% of participants (52/67) wearing the device for more than 10 h on 5 or more days at baseline and 61% (41/67) at 36 weeks. Including only files available for analysis and adjusting for participants who had withdrawn, at 36 weeks, this rose to 91% (41/45). On average participants provided 6.1 (SD 2.0) valid days of accelerometer wear (> 10 h of wear) out of a possible 7 requested at baseline, and 6.0 (SD 2.1) at 36 weeks. Average daily accelerometer wear was 18.5 h per day (SD 7.4) at baseline and 17.2 h per day (SD 6.1) at 36 weeks (Tables 5 & 6).
There was high engagement with the intervention with 82% of participants (55/67) who engaged in the motivational interview (visit 2), setting goals on the Stay-Active app, and 98% (54/55) submitting at least one PA. Sustained engagement was evident with participants regularly accessing Stay-Active over multiple weeks (Table 7) and over 50% of participants continuing to access the app on a weekly basis until week 10. Completion rates of self-reported PA questionnaires were high; 97% of participants completed the PPAQ (65/67) and 95% the EVS (64/67) at visit 1. This was reduced at visit 3; with PPAQ rates at 58% (39/67) and EVS rates at 40/67 (59%), (Table 5). Accounting for withdrawn participants, this rose to 73% (39/53) and 75% (40/53) respectively.
Acceptability
The responses to the OMDTSQ indicated that women were strongly satisfied with their care throughout the study. Thirty-nine participants completed the questionnaire at visit 2 and 37 at visit 3. Supplement material 2 shows the satisfaction scores for each question demonstrating improvement in most domains particularly in PA specific questions at visit 3. Most participants favoured weekly feedback.
Fidelity of the motivational interviewing intervention
Fifty-six participants (83%) enrolled in the study received a motivational interview. All interviews were recorded. MITI 4.2 coding was performed for six motivational interviews chosen at random. Mean for relational global summary score was 3.25 (SD 0.27), technical global 3.17 (0.26), %CR 18% (14%), R:Q 0.66 (0.38). No interviews met any ‘good’ thresholds. ‘Fair’ thresholds were met in all six interviews for technical global summary score, three interviews for relational global summary score, and one interview for %CRand R:Q.
Secondary outcomes
Physical activity assessment
Accelerometer defined PA levels across the study sample were very variable, and there was a trend for small reductions in activity between baseline and 36 weeks. On average total daily physical activity time (including light moderate and vigorous activity) reduced slightly between baseline (218.4 min per day [70.1]) and 36 weeks (195.8 min per day [64.2]). Daily moderate to vigorous activity also reduced between baseline (50.3 min per day [23.6])) and 36 weeks (43.9 min per day [22.1]) (Tables 5 & 6).
At baseline (visit 1); women reported a mean 78.09 ± 96.1 MET-hr/week moderate PA and vigorous PA of 0.87 ± 3.32 MET-hr/week (0.575 ± 2.49 MET-hr/week). For EVS; visit 1; the mean reported MVPA was 126 min per week (SD 98.2). At visit 3; PA levels were reduced mean 46.2 ± 49.7 MET-hr/week) and vigorous activity 0.1675 ± 0.837 MET-hr/week. However, EVS was higher than the mean reported MVPA at 131 (86.4) minutes per week.
Usage of stay-active
Fifty-five participants (82%) downloaded Stay-Active; it was used most frequently in the first six weeks of the intervention. For analysis, sessions with duration of less than two seconds were removed to reduce bias from accidental / compulsive opening of the app. In week 1; participants opened the application on average 9.0 times each, with a median duration per session of 23 (minimum 2, maximum 487) seconds. This was reduced by week 8, with 3.8 sessions per participant, and median duration of 14 (2, 172) seconds per session (Table 7). Participants logged a total of 699 physical activities (median 5 (1, 115) submissions per participant). In week 1, participants accessed the ‘record my physical activity’ section of the app on average 4.2 times each (median duration 18 (2, 433) seconds per session), this reduced to 1.5 times in week 8 (median duration 12 (2, 140) seconds). Thirty participants accessed the resource centre at least once spending an average time of 21.5 s per session.
Forty-three participants completed feedback on +Stay-Active. On a five-star rating scale (0 worst, 5 best), the percentage of participants rating the motivational interview as four or five stars was 95.3%, goal setting 97.7%, goal tracking 88.4%, automated motivational messages 76.7% and personalised messages about physical activity 93%.
The most common feedback from the free-text comments was that the app was easy to use. Suggestions on how to improve the functionality of the app were also frequent and centred around being able to record physical activity in more detail and review previous activity. Free-text comments (Table 8) demonstrated the effect of the app on a variety of behaviour change techniques and behaviour sources including psychological capability, reflective and automatic motivation [16].
Assessment of blood glucose control
Over the period of enrolment, mean blood glucose fell. In the first week after recruitment (at a mean gestation of 28 weeks) the mean blood glucose was 6.3 mmol/l which reduced to 6.1 mmol/l for the week after the Motivational interview intervention (at a mean gestation of 29 weeks) and reduced further to 5.8 mmol/l at a mean gestation of 36 weeks. This represents a change between these time points of: -0.16 (mean gestational week 28 and 29), -0.54 (mean gestational week 28 and 36) and -0.30 (mean gestational week 29 and 36). This was accounted for by a fall in both the fasting and postprandial blood glucose values (Supplement material 3).
Description of maternal and neonatal outcomes
Outcome data on 59 mother-baby pairs was available. Mean gestational age at birth was 39.2 weeks. 14% of women had a planned caesarean section (CS), 39% of women had an unassisted vaginal birth, 32% had an emergency CS and 15% of women had an assisted vaginal birth. Thirty nine percent of women had post-partum bleeding of more than 500mls, one woman had major perineal trauma, nine women had a hypertensive disorder of pregnancy, and no women required admission to the intensive care unit. There was a mean on 0.82 kg maternal weight gain between recruitment and last recorded weight before birth representing a mean of 0.06 kg weight gain per week.
The mean birth weight was 3401 g, with eight babies having a birth weight above 90th centile. 58% were female. No shoulder dystocia or neonatal hypoglycaemia requiring treatment was reported. Three babies had hyperbilirubinaemia and one had birth trauma. Four babies required admission to the neonatal intensive care for a mean duration of 1.6 days. These adverse outcomes were assessed and found to be not related to the intervention (Supplement material 4).
Assessment of participants contacts
A total of 367 follow-up phone calls were made to participants during the study. Seventy percentage (259) were answered by participants. A total of 959 motivational SMS messages were sent from Stay-Active. An additional 75 messages were sent for the initial setup credentials and forgot password requests.
Discussion
This study is the first to explore the feasibility and acceptability of this combined intervention aimed at maintaining PA levels in women with GDM. All indicators of success were achieved within the categories for participant engagement and fidelity of the intervention, nevertheless not all were fulfilled within recruitment and retention rates. The recruitment rate was lower than expected and the mean number of participants meeting the eligibility criteria was only 2.5 participants/week; the most likely explanation is the reduction in face-to-face consultations during the COVID pandemic. An assessment of future clinical activity and the proportion of women meeting the eligibility criteria would be prudent. Once participants received the motivational interview; they appeared to remain actively engaged in the study but future considerations will be given to maximising participants attendance at this visit.
This study adds to the literature regarding the development of a complex PA intervention to aid the wider management of GDM. Management involves counselling, dietary modification, PA, glucose monitoring, and supplemental pharmacological therapies. The implementation of individual management elements vary. GDM specific smartphone apps can provide an opportunity to improve management. A systematic review of the effectiveness of mobile health applications for GDM included five RCTs and found improved trends in glycemic control, pregnancy and birth related outcomes [29]. The Apps support women with automatic transfer of blood glucose values from a glucometer to their smartphone and onwards to the supporting healthcare team, and some provided varying tailored lifestyle information on diet, PA, breastfeeding and GDM [30, 31]. Similar to + Stay-Active feedback, studies have described that these smartphone apps are appealing to women with overwhelmingly positive feedback [32]. Whilst positive results have been reported in improved compliance of blood glucose monitoring [33, 34], significantly lower blood glucose measurement and lower rate of insulin needed [34]; smartphone-based apps alone have not been clearly shown to improve pregnancy outcomes [35]. Immanuel and Simmons highlight that many studies [15, 31, 34] have been underpowered to detect improvement in pregnancy outcomes [35]. Furthermore, the specific content, measurement or analysis of any PA interventions were limited or not reported [15, 30, 31]. Our work provides a step forward in delivering, measuring, and analysing a specific PA intervention for this population.
Adherence to accelerometer measurement protocols were excellent, with moderate levels of completion rates of self-reported PA assessments and satisfaction questionnaires. This may reflect burden of the high number of questionnaires participants were expected to complete. This could be refined and re-enforces the capability to capture this data in our population.
The evidence supporting the benefits of PA among women with GDM is mounting. A further metanalysis published in 2022; concluded exercise intervention can improve the blood glucose parameters and can also reduce adverse pregnancy outcomes, such as premature birth and macrosomia [36]. This supports separate analyses that found requirements of insulin therapy, dosage and latency to administration were improved in the exercise intervention groups [8, 37]. However, most exercise interventions are supervised and well resourced; potentially being difficult to translate into the healthcare setting. Integration of health coaching and evidence based behavioural strategies (goal setting, monitor and feedback) may provide the most appropriate tools for translation of this evidence into clinical practice [38]. Multicomponent PA interventions appear to be more effective than standalone interventions [39, 40]. In our study, Women responded positively to the combination of motivational interviewing and support through Stay-Active. Re-enforcing this, is promising results from a randomised trial, that used a similar approach to + Stay-Active, found the combination of a mobile phone app and brief counselling increased objectively measured PA over 3 months in physically inactive non-pregnant women [41]. This combined approach has successfully been used to enhance the daily level of PA among older adults [42]. Within pregnant women,,motivational interviewing was found to improve adherence to healthy eating in addition to routine care in women with type 2 diabetes [43] and in a recent prospective RCT involving online health-coaching led to women increasing or at least maintaining their level of PA during the course of their pregnancy [44]. Furthermore, Smartphone apps have been found to be effective for increasing objectively measured PA in pregnant women [45].
The timing of our intervention was essential, building on a potential ‘teachable moment’ [46] following a diagnosis of GDM where there is opportunity for women to re-focus on PA with the health of the baby and glycaemic control being strong motivators. Potentially, optimising the effect of motivational interview.
Sustained engagement was evident with participants regularly accessing the Stay-Active app and logging activity for multiple weeks. The gradual reduction in the number of sessions and time spent on the app may represent increased familiarity of participants with the app and the effect of behaviour change, or disengagement. Evidence of sustained engagement is important, and not always evident. For example, in a large RCTs (n = 170 in each arm) to evaluate the effects of a smartphone app–based lifestyle coaching program ((Habit-GDM) a program comprised 12 interactive lessons); only 49.4% of the intervention women accessed the educational lessons [30]. In another multicentre nested randomised trial involved 162 pregnant; whereby 77 women (77/162) in addition to lifestyle advice were provided with access to a smartphone application designed to encourage women to set dietary and PA goals and monitor their progress only 24 women (31.2%) reported using the smartphone application [47]. Motivational interviewing together with regular follow up and individualised reminder messages, helped maintain engagement over the study period. We feel there is the unique opportunity for clinicians to play a key role by interacting and supporting the service user via Stay-Active.
With the increasing number of women with GDM and greater pressures on health care providers to streamline services; digital technologies are expected to provide remote support at scale. Nevertheless, during our study support was considerable with motivational inteviews, regular telephone follow ups and over 900 text messages sent; the effectiveness on clinical outcomes will need to be balanced with intervention and implementation costs. More robust resource utilization and cost-effective analysis within GDM App studies is required [32] and needs to be consider in future work.
The study demonstrated moderate acceptability for the fidelity of motivational interviewing. with the complex reflections and ratio of reflection to questions were generally below ‘fair’ proficiency. This highlights motivational interviewing is a challenging skill. Multifaceted training, practice and mentoring would be required to meet the accepted proficiency thresholds in the future.
The participant characteristics were typical of this single centre and with only one participant on pharmacological medication for GDM at recruitment. Glycaemia control improved over the study period as one would expect as all women received active clinical management of their GDM. It is encouraging to see this improvement and we can conclude that the addition potential burden of this intervention did not adversely affect glycaemic control. Maternal and neonatal outcomes were also broadly as expected. Weekly weight gain was only 0.06 kg during the study period, 48% of women were on pharmacological treatment at birth which compares with historical cohorts in the same centre and suggests the intervention was not associated with a reduction in the need for pharmacological medication.
Both the PPAQ and objective accelerometer demonstrated a reduction of MVPA by visit 3; however, this is expected with activity levels typically declining during pregnancy [48]. Due to the lack of a control group, drawing conclusions regarding the impact of this intervention on the rate of decline in PA level is not possible. Additionally, there is no normative data for PPAQ within UK populations, and due to variations in methodology and study population, it is difficult to compare activity levels as measured by PPAQ between studies [49]. Within the PPAQ data set in particular, there were a small minority of outlying values with very high PA levels reported. Despite their practicality, it is an established limitation of PA self-reported data that they are subject to significant error and bias. Recalling and reporting PA is challenging, often leading to participants over or under-reporting PA. The resultant misclassification can impact the ability to detect associations or intervention-related behaviour change. With the higher levels of adherence to accelerometer measurement protocols and lower completion rates of the self-reported questionnaires; our further work would focus on using this objective measure of PA.
We believe that a larger multi-centre randomised controlled trial to investigate the effectiveness of this intervention is now warranted. Prior to this, further training is required to ensure motivation interviewing meets the accepted proficiency thresholds. Inclusion criteria should be reviewed to optimise participant recruitment and clinic activity assessed. This study demonstrated this combined behavioural change driven approach maintained high levels of engagement. There is already a commercially available CE-marked smartphone glucose management application GDm-Health [15] embedded within the clinical pathway for women with GDM at the study site, which has previously shown high levels of patient engagement, compliance and usage [26]. Given that + Stay-Active was found to be feasible and acceptable, an additional functionality to apps such as GDm-Health could be considered, improving usability and accessibility allowing users to observe the direct impact of PA of their blood glucose control.
Further work to assess whether this intervention model could be transferred to other populations of pregnant women or non-pregnant patients with comorbidities to evaulated PA and clinical outcomes, is required.
Strengths and limitations of this study
This study used several outcomes to provide evidence on the feasibility and acceptability of this complex intervention. However, the study design and size was not powered to determine intervention efficacy or clinical effectiveness. It was within a single centre, non-randomised and lacked a control group. The study partially recruited during the COVID-19 pandemic, meaning that interviews were remote and opportunities for exercise outside the home may have been limited for some women. Therefore, conclusions cannot be drawn regarding effectiveness of the intervention. Participation was not mandatory, which may have resulted in a selection bias towards those who have a tendency/preference to undertake higher levels of PA.
Conclusions
The delivery of this combined intervention designed to support PA in pregnant women was feasible and well accepted. Recruitment rate was lower than expected and affected by the COVID pandemic. Retention rates were satisfactory and there was a high level of participant compliance with PA measurements and engagement throughout the study. A future RCT to explore the efficacy of this intervention to increase PA and evaluate the effect on clinical outcomes would be feasible.
Availability of data and materials
The datasets generated and analysed during the current study are not publicly available due arrangements specified in ethics approval, but anonymised data is available from the corresponding author on reasonable request.
Abbreviations
- App:
-
Application
- BCTs:
-
Behaviour Change Techniques
- BCW:
-
Behaviour Change Wheel
- EVS:
-
Exercise vital sign assessment
- GDM:
-
Gestational diabetes mellitus
- MVPA:
-
Moderate to vigorous physical activity
- NICE:
-
National Institute for Health and Care Excellence
- OMDTSQ:
-
Oxford Maternity Diabetes Treatment Satisfaction Questionnaire
- %CR:
-
Percentage Complex Reflections
- PA:
-
Physical activity
- PPAQ:
-
Pregnancy Physical Activity Questionnaire
- RCT:
-
Randomised control trial
- R:Q:
-
Reflection to Question ratio
- SD:
-
Standard deviation
References
Basri NI, Mahdy ZA, Ahmad S, Abdul Karim AK, Shan LP, Abdul Manaf MR, Ismail NAM. The World Health Organization (WHO) versus The International Association of Diabetes and Pregnancy Study Group (IADPSG) diagnostic criteria of gestational diabetes mellitus (GDM) and their associated maternal and neonatal outcomes. Horm Mol Biol Clin Investig. 2018;34(1). https://doi.org/10.1515/hmbci-2017-0077.
Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358(19):1991–2002.
Schneider S, Hoeft B, Freerksen N, Fischer B, Roehrig S, Yamamoto S, et al. Neonatal complications and risk factors among women with gestational diabetes mellitus. Acta Obstet Gynecol Scand. 2011;90(3):231–7.
Kim C, Newton KM, Knopp RH. Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care. 2002;25(10):1862–8.
Kim C. Gestational diabetes: risks, management, and treatment options. Int J Womens Health. 2010;2:339–51.
Lowe LP, Metzger BE, Dyer AR, Lowe J, McCance DR, Lappin TR, et al. Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study: associations of maternal A1C and glucose with pregnancy outcomes. Diabetes Care. 2012;35(3):574–80.
Martis R, Crowther CA, Shepherd E, Alsweiler J, Downie MR, Brown J. Treatments for women with gestational diabetes mellitus: an overview of Cochrane systematic reviews. Cochrane Database Syst Rev. 2018;8:CD012327.
Cremona A, O’Gorman C, Cotter A, Saunders J, Donnelly A. Effect of exercise modality on markers of insulin sensitivity and blood glucose control in pregnancies complicated with gestational diabetes mellitus: a systematic review. Obes Sci Pract. 2018;4(5):455–67.
Harrison AL, Shields N, Taylor NF, Frawley HC. Exercise improves glycaemic control in women diagnosed with gestational diabetes mellitus: a systematic review. J Physiother. 2016;62(4):188–96.
National Institute for Health and Care Excellence (NICE). Gestational diabetes: risk assessment, testing,diagnosis and management. Update Dec 2020.
Harrison AL, Taylor NF, Frawley HC, Shields N. Women with gestational diabetes mellitus want clear and practical messages from credible sources about physical activity during pregnancy: a qualitative study. J Physiother. 2019;65(1):37–42.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95.
Currie S, Sinclair M, Murphy MH, Madden E, Dunwoody L, Liddle D. Reducing the decline in physical activity during pregnancy: a systematic review of behaviour change interventions. PLoS One. 2013;8(6):e66385.
Smith R, Ridout A, Livingstone A, Wango N, Kenworthy Y, Barlett K, et al. Motivational interviewing to increase physical activity in women with gestational diabetes. Br J Midwifery. 2021;29(10):550–6.
Mackillop L, Hirst JE, Bartlett KJ, Birks JS, Clifton L, Farmer AJ, et al. Comparing the efficacy of a mobile phone-based blood glucose management system with standard clinic care in women with gestational diabetes: randomized controlled trial. JMIR Mhealth Uhealth. 2018;6(3):e71.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Smith R, Michalopoulou M, Reid H, Payne Riches S, Nicola. W, Kenworthy Y, et al. Applying the behaviour change wheel to develop a smartphone application ‘Stay-Active’ to increase physical activity in women with gestational diabetes. Submitted to BMC Childbirth and Pregnancy. 2021. Under review.
Smith R, Kenworthy Y, Astbury NM, Birks J, Bateman P, Dyson P, et al. Study protocol: use of a smartphone application to support the implementation of a complex physical activity intervention (+). BMJ Open. 2022;12(9):e062525.
(UK) NCCfWsaCsH. Diabetes in pregnancy: management of diabetes and its complications from preconception to the postnatal period. 2015.
Relph S, Thangaratinam S. Maternal medicine in the COVID era. Best Pract Res Clin Obstet Gynaecol. 2021;73:113–24.
National Institute for Health and Care Excellence (NICE). 2018 surveillance of diabetes in pregnancy: management from preconception to the postnatal period (NICE guideline NG3). 2018.
Chasan-Taber L, Schmidt MD, Roberts DE, Hosmer D, Markenson G, Freedson PS. Development and validation of a pregnancy physical activity questionnaire. Med Sci Sports Exerc. 2004;36(10):1750–60.
Coleman KJ, Ngor E, Reynolds K, Quinn VP, Koebnick C, Young DR, et al. Initial validation of an exercise “vital sign” in electronic medical records. Med Sci Sports Exerc. 2012;44(11):2071–6.
da Silva SG, Evenson KR, Ekelund U, da Silva ICM, Domingues MR, da Silva BGC, et al. How many days are needed to estimate wrist-worn accelerometry-assessed physical activity during the second trimester in pregnancy? PLoS One. 2019;14(6):e0211442.
Mottola MF, Davenport MH, Ruchat SM, Davies GA, Poitras VJ, Gray CE, et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br J Sports Med. 2018;52(21):1339–46.
Hirst JE, Mackillop L, Loerup L, Kevat DA, Bartlett K, Gibson O, et al. Acceptability and user satisfaction of a smartphone-based, interactive blood glucose management system in women with gestational diabetes mellitus. J Diabetes Sci Technol. 2015;9(1):111–5.
Moyers TB, Rowell LN, Manuel JK, Ernst D, Houck JM. The Motivational Interviewing Treatment Integrity Code (MITI 4): rationale, preliminary reliability and validity. J Subst Abuse Treat. 2016;65:36–42.
Avery KN, Williamson PR, Gamble C, O’Connell Francischetto E, Metcalfe C, Davidson P, et al. Informing efficient randomised controlled trials: exploration of challenges in developing progression criteria for internal pilot studies. BMJ Open. 2017;7(2):e013537.
Eberle C, Loehnert M, Stichling S. Effectivness of specific mobile health applications (mHealth-apps) in gestational diabtetes mellitus: a systematic review. BMC Pregnancy Childbirth. 2021;21(1):808.
Yew TW, Chi C, Chan SY, van Dam RM, Whitton C, Lim CS, et al. A randomized controlled trial to evaluate the effects of a smartphone application-based lifestyle coaching program on gestational weight gain, glycemic control, and maternal and neonatal outcomes in women with gestational diabetes mellitus: the SMART-GDM study. Diabetes Care. 2021;44(2):456–63.
Borgen I, Småstuen MC, Jacobsen AF, Garnweidner-Holme LM, Fayyad S, Noll J, et al. Effect of the Pregnant+ smartphone application in women with gestational diabetes mellitus: a randomised controlled trial in Norway. BMJ Open. 2019;9(11):e030884.
Smyth S, Curtin E, Tully E, Molphy Z, Breathnach F. Smartphone Apps for surveillance of gestational diabetes: scoping review. JMIR Diabetes. 2022;7(4):e38910.
Guo H, Zhang Y, Li P, Zhou P, Chen LM, Li SY. Evaluating the effects of mobile health intervention on weight management, glycemic control and pregnancy outcomes in patients with gestational diabetes mellitus. J Endocrinol Invest. 2019;42(6):709–14.
Miremberg H, Ben-Ari T, Betzer T, Raphaeli H, Gasnier R, Barda G, et al. The impact of a daily smartphone-based feedback system among women with gestational diabetes on compliance, glycemic control, satisfaction, and pregnancy outcome: a randomized controlled trial. Am J Obstet Gynecol. 2018;218(4):453.e1-.e7.
Immanuel J, Simmons D. Apps and the woman with gestational diabetes mellitus. Diabetes Care. 2021;44(2):313–5.
Li X, Luo R, Qiao B, Ou H. Exercise intervention improves blood glucose levels and adverse pregnancy outcomes in GDM patients: a meta-analysis. Comput Math Methods Med. 2022;2022:9287737.
Medbh H, K. C, Marlene S, H MM. Can physical activity and dietary interventions improve maternal and fetal outcomes in women with gestational diabetes mellitus? A systematic review and meta-analysis. Evid Based Midwif. 2018;16(3):76–83.
Onaade O, Maples JM, Rand B, Fortner KB, Zite NB, Ehrlich SF. Physical activity for blood glucose control in gestational diabetes mellitus: rationale and recommendations for translational behavioral interventions. Clin Diabetes Endocrinol. 2021;7(1):7.
Schoeppe S, Alley S, Van Lippevelde W, Bray NA, Williams SL, Duncan MJ, et al. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: a systematic review. Int J Behav Nutr Phys Act. 2016;13(1):127.
Vetrovsky T, Borowiec A, Juřík R, Wahlich C, Śmigielski W, Steffl M, et al. Do physical activity interventions combining self-monitoring with other components provide an additional benefit compared with self-monitoring alone? A systematic review and meta-analysis. Br J Sports Med. 2022;56(23):1366–74.
Fukuoka Y, Haskell W, Lin F, Vittinghoff E. Short- and long-term effects of a mobile phone app in conjunction with brief in-person counseling on physical activity among physically inactive women: the mPED randomized clinical trial. JAMA Netw Open. 2019;2(5):e194281.
Larsen RT, Korfitsen CB, Keller C, Christensen J, Andersen HB, Juhl C, et al. The MIPAM trial - motivational interviewing and physical activity monitoring to enhance the daily level of physical activity among older adults - a randomized controlled trial. Eur Rev Aging Phys Act. 2021;18(1):12.
Ásbjörnsdóttir B, Vestgaard M, Ringholm L, Andersen LLT, Jensen DM, Damm P, et al. Effect of motivational interviewing on gestational weight gain and fetal growth in pregnant women with type 2 diabetes. BMJ Open Diabetes Res Care. 2019;7(1):e000733.
Téoule J, Woll C, Ray J, Sütterlin M, Filsinger B. The effectiveness of integrated online health-coaching on physical activity and excessive gestational weight gain: a prospective randomized-controlled trial. Arch Gynecol Obstet. 2024. https://doi.org/10.1007/s00404-023-07296-y. Epub ahead of print. PMID: 38217763.
Sharp KJ, Sherar LB, Kettle VE, Sanders JP, Daley AJ. Effectiveness of interventions to increase device-measured physical activity in pregnant women: systematic review and meta-analysis of randomised controlled trials. Int J Behav Nutr Phys Act. 2022;19(1):142.
Lawson PJ, Flocke SA. Teachable moments for health behavior change: a concept analysis. Patient Educ Couns. 2009;76(1):25–30.
Dodd JM, Louise J, Cramp C, Grivell RM, Moran LJ, Deussen AR. Evaluation of a smartphone nutrition and physical activity application to provide lifestyle advice to pregnant women: the SNAPP randomised trial. Matern Child Nutr. 2018;14(1):e12502.
Mitro SD, Peddada S, Gleason JL, He D, Whitcomb B, Russo L, et al. Longitudinal changes in physical activity during pregnancy: national institute of child health and human development fetal growth studies. Med Sci Sports Exerc. 2022;54(9):1466–75.
Silva-Jose C, Sánchez-Polán M, Barakat R, Gil-Ares J, Refoyo I. Level of physical activity in pregnant populations from different geographic regions: a systematic review. J Clin Med. 2022;11(15):4638.
Acknowledgements
This research was supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Funding
This research was supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC). Grant number: N/A.
Author information
Authors and Affiliations
Contributions
RS, LM, CR, MS contributed and helped with design of Stay-Active. RS, IS, RG, JH, MM, NA, JB, PB, SJ, RP, CR, MS, NW, AW and YK assisted with data analysis, drafted and wrote the manuscript. All authors revised the content of the article, and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures will be followed are in accordance with the Declaration of Helsinki.
This study has received a favourable opinion from South Central—Hampshire B Research Ethics Committee; REC reference: 20/SC/0342. Written informed consent was obtained from all participants. To facilitate the extra study visits, travel expenses were paid on presentation of a receipt. This study is registered https://www.isrctn.com/ISRCTN11366562. The study protocol registered with ISRCTN 39136.
Consent for publication
Not applicable.
Competing interests
LM, JH, MM, YK, RS, NW, JB are supported by the NIHR Oxford Biomedical Research Centre. JH is funded by a UKRI Future Leaders fellowship. The remaining authors (RG, NA, IS, PB, SB, RP, CR, MS, AW) have no disclosures of interest and there are no other conflicts to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Smith, R., Gould, R., Kenworthy, Y. et al. A feasibility study using motivational interviewing and a smartphone application to promote physical activity (+Stay-Active) for women with gestational diabetes. BMC Pregnancy Childbirth 24, 360 (2024). https://doi.org/10.1186/s12884-024-06508-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12884-024-06508-w