
Abstract
Purpose
The diagnosis of pulmonary hamartoma (PH) based on computed tomography (CT) is a challenge, especially in patients with atypical imaging characteristics. This study was aimed at summarizing the imaging characteristic of 18F-Fluoro-d-glucose positron emission tomography-computed tomography (18F-FDG PET-CT) in PH and exploring the application value of PET-CT in the diagnosis of PH.
Data and methods
Patients diagnosed with PH who had undergone PET-CT from literature pertaining were retrospectively analyzed, which were cases of publications from the Cochrane Library, PubMed, Excerpta Medica Database (EMBASE), China National Knowledge Infrastructure (CNKI) and Wanfang databases, from 2008 to June 2022. The other 20 cases of the collection were patients from our hospital from 2008 to June 2022. Patients’ symptoms, imaging characteristics of chest CT, PET-CT characteristics, the reason for PET-CT and the complications were analyzed.
Results
In this retrospective study, a total of 216 patients were diagnosed with PH and had been examined by PET-CT. 20 of the cases were patients of our hospital from January 2008 to June 2022. The other cases were collected from the literature. The mean diameter of most PH lesions is 1.7 ± 1.0 cm. The mean maximum standardized uptake value (SUVmax) of the PH lesions was 1.2 ± 1.1. Most of their SUVmax were lower than internationally recognized cut-off value (SUVmax = 2.5). PET-CT was superior to CT in the diagnosis of PH but there was a correlation of between CT diagnosis and PET-CT diagnosis for the PH lesions. In order to draw the Receiver operating characteristic (ROC), we selected 29 patients with a clear SUVmax value of their PH lesion, and 29 lung cancer patients with clear SUVmax value in our hospital were collected as a control group. ROC curve analysis showed that the area under curve (AUC) of SUVmax was 0.899, and the optimal diagnostic threshold was SUVmax > 2.65. PET-CT could distinguish PH from malignant lesions with a sensitivity of 89.66% by applying a SUVmax of 2.65 as a cut-off in this study.
Conclusion
PET-CT might be a useful tool to diagnose PH, which shows a better diagnostic sensitivity than CT. But PET-CT can not be used as a single diagnostic approach, which should be combined with other methods and the patients’ history to make the most correct diagnosis.
Similar content being viewed by others


Introduction
Pulmonary hamartoma (PH) is the most common benign lung tumor. When the popcorn calcification is present at the computed tomography (CT) scan, it usually suggests the diagnosis of PH [1]. Most PHs appear as solitary pulmonary nodules (SPN) and don’t need surgical resection. The benign diagnosis by CT helps guide the next step to formulate the time for reexamination and evaluating the lesion regularly. However, the typical findings can be seen in only 20% of all the cases [2], the atypical imaging characteristics make the diagnosis and differential diagnosis problematic. Sometimes it can be even misdiagnosed as lung cancer [3, 4].
Nowadays, the 18F-Fluoro-d-glucose positron emission tomography-computed tomography (18F-FDG PET-CT) plays an important role in the diagnosis, assessment of therapeutic effect and prognosis in SPN [5], inflammatory disorders [6] and rare diseases [7, 8]. It has been reported that PET-CT has a high accuracy for the detection and characterization of SPNs in lung diseases [9], the cut-off maximum standardized uptake values (SUVmax) of 2.5 is currently accepted [10]. When PH is diagnosed as a malignant or suspicious lesion by CT, PET-CT is feasible for further examination. However, PET-CT can only make a preliminary diagnosis, and the diagnostic gold standard still depends on pathology. At the same time, some PH with increased 18F-Fluoro-d-glucose (FDG) uptake could be identified malignant by PET-CT.
Up to now, only a few studies concentrated on the characteristics of PH in PET-CT and the diagnostic value of PET-CT in PH. Most of the literatures consider that the SUVmax of PH is low, manifested as low or no FDG uptake. However, there is no more suitable cut-off value to distinguish PH from pulmonary malignancy. Therefore, the goal of this retrospective study was to further explore the diagnostic value of PET-CT in PH, including the imaging characteristics of PH in PET-CT, the diagnostic sensitivity of PET-CT, and the cut-off value based on our data. In order to provide more basis for early and accurate diagnosis.
Methods and materials
Literature search and data collection
This retrospective study integrated the data of the single center and the patients who met the inclusion criteria in the literature. Publications regarding the use of 18F-FDG PET-CT in patients with PH were retrieved from the Cochrane Library, PubMed, Excerpta Medica Database (EMBASE), China National Knowledge Infrastructure (CNKI) and Wanfang databases, from 2008 to June 2022, using the terms of “pulmonary hamartoma”, “PH”, “positron emission tomography-computed tomography”, “PET-CT” and “PET/CT”. Duplicated references were excluded. Patients’ age, gender, clinical characteristics, chest CT findings, 18F-FDG PET-CT characteristics and the SUVmax of the PH lesions were extracted from each study for retrospective analysis. 20 involved patients were from The First Affiliated Hospital of Soochow University from January 2008 to June 2022. In addition, 29 lung cancer patients with SUVmax value in our hospital were collected to draw the ROC (receiver operating characteristic) curve as a control group. This retrospective single-center study was approved by the Ethics Committee of The First Affiliated Hospital of Soochow University, and the patient information was anonymized and de-identified prior to analysis. All methods were performed in accordance with the relevant guidelines and regulations.
Image analysis
CT images and PET-CT images of 20 patients in our hospital were reviewed by 3 experienced radiologists and nuclear medicine specialists with > 10 years of experience blinded to the pathology. In case of conflict of opinions, 3 physicians will make diagnosis based on comprehensive analysis and complete discussion combined with relevant clinical data.
Statistical analysis
All statistical analyses were performed using the SPSS® statistical software v. 25.0 (IBM Corp., New York, NY). Differences in proportions were assessed by χ2 test. P < 0.05 was considered statistically significant.
Results
Characteristics of the screened studies
A total of 216 patients confirmed to have PH and had undergone PET-CT were included in this study. A total of 10 eligible publications were retrieved [3, 4, 11,12,13,14,15,16,17,18], which involved 196 patients. And the rest 20 cases of the collection were patients from the First Affiliated Hospital of Soochow University. In order to draw the ROC curve, we enrolled 29 patients pathologically confirmed lung cancer from our hospital. Appropriate cases were selected for each analysis based on the differences in clinical data provided.
Mean diameter and mean SUVmax analyzed in literature
A total of 165 eligible cases were included in this analysis, based on data from 4 articles [11,12,13,14]. All these cases were diagnosed PH pathologically. These 165 patients appeared as different whole in the 4 articles, which only provided the mean size and mean SUVmax, while the specific lesion size and SUVmax value of each patient were not provided. According to the table, the mean diameter of most PH lesions is 1.7 ± 1.0 cm. The mean SUVmax of the PH lesion was 1.2 ± 1.1, which means that most of their SUVmax values were lower than internationally recognized cut-off value (SUVmax = 2.5) [10], indicating low uptake or no uptake. It is consistent with the uptake characteristics of benign tumors.
Comparison of diagnostic sensitivity between CT and PET-CT
In order to compare the diagnostic sensitivity between CT and PET-CT, a total of 84 eligible cases were included in this analysis. These 84 cases were provided with concurrent CT and PET-CT diagnosis, based on data of 64 patients from 7 articles [3, 4, 11, 13, 15,16,17] and 20 patients of our hospital, and all these cases had pathologic diagnosis of PH. There were significant differences between the two diagnostic methods (χ2 = 14.235, P < 0.001). The sensitivity of PET-CT was 78.6% (66/84); while CT has a sensitivity of 52.4% (44/84), indicating that PET-CT is superior to CT in the diagnosis of PH (Tables 1, 2).
Correlation between CT diagnosis and PET-CT diagnosis
In order to analyze the connection of diagnostic results between CT and PET-CT, a total of 84 eligible cases with concurrent CT and PET-CT diagnosis were included in this analysis, the inclusion criteria are the same as above. and all these cases had pathologic diagnoses of PH. As shown in Table 3, there was a specific correlation between CT diagnosis and PETCT diagnosis (χ2 = 4.671, P < 0.05). Among the 43 patients diagnosed benign by CT, the diagnostic sensitivity of PET-CT was 86.3% (38/44), but among the 40 patients diagnosed malignant by CT, the diagnostic sensitivity of PET-CT was only 70.0% (28/40). The results showed that there is a correlation of diagnostic sensitivity between CT and PET-CT, PET-CT showed a lower diagnostic sensitivity for PH lesions misdiagnosed as malignant by CT, which showed the limitation of PET-CT.
Major imaging characteristics of CT in patients with PH
In order to analyze the imaging characteristics of CT of PH, we need to collect cases with detailed clinical data. A total of 25 eligible cases with CT characteristics and diagnosis were included in this analysis, based on data of 5 patients from 5 articles [3, 4, 15,16,17] and 20 patients from our hospital. All these cases had pathological confirmation of PH. These 25 patients had complete case data for detailed analysis. Detailed data were shown in Table 4. Except for one large lesion with a diameter of 180 mm, which was a pulmonary mass, other lesions ranged in size from 4 to 30 mm, which belonged to SPN. Five patients (5/25) had hamartoma lesions with calcification, 6 patients (6/25) had hamartoma lesions with fat density, and one patient had both calcification and fat density; none of the patients had typical popcorn calcification on imaging. Among all the cases, 3 patients were diagnosed benign (2 of which considered as hamartoma), 11 patients were diagnosed malignant, and the diagnosis of rest 11 cases was indeterminate. 8 patients underwent enhanced CT examination, and 4 of them showed enhancement in the CT images.
Major imaging characteristics of 18F-FDG PET-CT in patients with PH
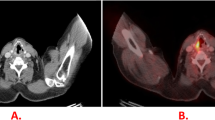
A total of 25 eligible cases with PET-CT characteristics and diagnosis were included in this analysis, same as above. All these cases were diagnosed PH pathologically. Detailed data were shown in Table 5. PET-CT images of one case’s PH are shown in Fig. 1. All patients underwent PET-CT examination because the malignant possibility of the PH lesion could not be excluded. The cases included 2 patients combined with lung cancer, 1 patient combined with cervical cancer, which were confirmed by pathology. The results showed that only 2 patients had higher FDG uptake with a SUVmax of 3.0, which was higher than the recognized cut-off value. There were 5 cases combined with lymph node uptake. Of which 3 demonstrated submaxillary lymph node uptake, one demonstrated left cervical lymph node uptake combined with left upper lung cancer, one demonstrated right hilar lymph node uptake combined with right upper pulmonary mechanized pneumonia. No significant enlargement or increased FDG uptake of the mediastinal lymph nodes and rest hilar lymph nodes were observed.

A kind of round nodular opacity was observed in the dorsal segment of the right lower lung, with a diameter of about 13 mm. No significant abnormal increase in FDG uptake was observed
On the whole, 14 cases were diagnosed as benign while 11 cases were diagnosed as malignant by means of PET-CT. Factors contributing to the diagnosis of malignancy included possible combination of malignant tumor or malignant tumor metastasis (3/11), multiple PH (1/11), giant PH (1/11), and purely misdiagnosis (6/11).
The cut-off value we concluded based on our cases
A total of 29 eligible PH patients were included in this analysis, including 9 patients from literatures [3, 4, 12,13,14,15,16,17,18] and 20 in our hospital. The PH lesion of the 29 patients had clear SUVmax value for us to analysis and draw the ROC curve. In addition, 29 lung cancer patients with clear SUVmax value in our hospital were collected to draw the ROC curve as a control group. The SPN of the 29 patients was pathologically confirmed as early primary lung cancer after surgery, showing as single lesions on CT imaging. ROC curve analysis for discriminating malignant lesions and hamartoma lesions was performed. The ROC curve obtained was shown in Fig. 2. The area under the ROC curve (AUC) of SUVmax was 0.899 for malignant lesions and hamartoma lesions. The cutoff value of SUVmax, which distinguishing malignant lesions from hamartoma lesions was > 2.65 (Sensitivity 89.66%, specificity 86.21%), and the difference was statistically significant (P < 0.001). PET-CT could distinguish PH from malignant lesions with a sensitivity of 89.66% by applying a SUVmax of 2.65 as a cut-off in this study.

The ROC curve for SUVmax threshold to distinguishing malignant lesions from hamartoma lesions
Discussion
PH is usually asymptomatic, presenting as small, single, well-circumscribed round nodules [19]. However, typical findings might not be observed, thus CT findings cannot be diagnostic regarding malignancy [16, 17, 20]. At this point, PET-CT can be used for further evaluation. Like other benign lung lesion, PH usually shows a lower FDG uptake than malignant tumor. The SUVmax together with visual assessment improved the diagnostic accuracy [21].
First, a total of 165 cases were included in this analysis from 4 literatures, and the results are shown in Table 1. The SUVmax value of pulmonary hamartoma is lower than the internationally recognized cut-off value (SUVmax = 2.5) [10], indicating low uptake or no uptake. And the mean size of the PH lesion is 1.7 cm, which were in line with previous experience [22, 23].
We analyzed and compared the diagnostic differences between PET-CT and CT, and the results were shown in Table 2. In our study, the differences between the two diagnosis was statistically significant and the diagnostic sensitivity of PET-CT is superior to CT, which showed that PET-CT could be a valuable tool to evaluate PH with a higher diagnostic accuracy due to less misdiagnosed rate, which was consistent with the previous experience [21].
Based on the CT characteristics of the lesion, PET-CT further evaluate the lesions by combining the FDG uptake of the lesion and the surrounding lymph nodes [24]. In our study, we used PET/CT to evaluate the hilar and mediastinal lymph nodes in PH patients, the results were shown on Table 4. The upper results showing a higher diagnostic accuracy than CT. To explore the association between the two diagnostic modalities, we further analyzed the CT and PET-CT diagnosis of the 84 patients above. In our study, as shown in Table 3, there is a correlation of diagnostic sensitivity between CT and PET-CT, which showed that the diagnostic sensitivity of PET-CT was better than CT, but it still has certain limitations on atypical PH lesions.
Next, we analyzed 25 patients who had received PET-CT examination with detailed clinical data, and the results were shown in Table 4 and 5. PET-CT images of one case’s PH are shown in Fig. 1.
First, we analyzed the CT characteristics of PH lesions. Case 23 was a patient with a giant PH, the diameter of the lesion was up to 18 cm, which was a lung mass. And the other PH lesion of the collection belonged to SPN. Among the 25 patients with PH, most of the patients lacked calcification (23/25), fat density (22/25), and no patients showed popcorn calcification. Atypical CT imaging findings lead to unclear CT diagnosis; Only 2 cases were diagnosed as PH by CT. 9 patients underwent contrast-enhanced CT, and 4 of which showed enhanced images. Christensen et al. showed that PET-CT is preferable to enhanced CT in evaluating indeterminate pulmonary nodules [25].
PET-CT examination was performed in all cases because of the lack of typical PH characteristics and a malignant diagnosis could not be ruled out. According to the results of PET-CT examination, most PH lesions (23/25) and lymph node showed no significant increase in FDG uptake, which was consistent with a benign lesion. In our study, 3 cases were diagnosed as metastatic lung cancer lesion because of the combination of malignant tumor. Because metastatic lung cancer cannot be ruled out, PETCT could make a malignant diagnosis. This result has not been mentioned in previous studies [11,12,13,14, 18].
Based on the above results, we analyzed the factors influencing the diagnostic sensitivity of PET-CT in PH. The factors contributed to diagnosis of PH by means of PET-CT including a single lesion, low SUVmax of lesion (lower than the internationally recognized cut-off value of 2.5) and no other combined malignant tumor. On the contrary, some PH lesions have increased FDG uptake (which may be caused by the large size of the lesions, combined with inflammation, etc.) could cause false negative, which was consistent with the literature [26]. Meantime, according to our results, when patients complicated with other malignant tumors, PH lesions could be misdiagnosed as metastatic malignant nodules. In this situation, the malignant diagnosis of PET-CT is reasonable, but the possibility of combination of benign neoplasms, such as PH, should be considered.
The ability of PET-CT to differentiate benign lesions from malignant is significant for the following clinical decisions. Studies have been performed to examine the accuracy of the cut-off value of 2.5. Aleksandar et al. [27]hold the view that an SUV below 1.25 was always combined with benign lesions. In our study, we obtained one SUVmax cut-off value of 2.65 according to the ROC curve, which was higher than the previous experiences [27,28,29]. Several possible reasons should be taken into consideration. First, the SUV is affected by a large number of technological factors (inter scanner variability, image reconstruction method, etc.) and biological factors (serum glucose level, body weight, etc.) [30]. As PET-CT becomes more widely used in the evaluation of non-malignant tumors and the number of relevant studies has increased, the cut-off value is constantly changing. Second, the cases included to plot the ROC curve were not sufficient enough to be convictive, causing selection bias. Meanwhile, Giant PH [17], multiple PH [16] and PH combined with pneumonia [31] can demonstrated a higher uptake could make the cut-off value increasing. Last, the SUVmax doesn’t take the volume of the tumor into account, this may be a significant limitation because tumor volume could affect the SUVmax, which may affect the results of the study [32]. However, Sim et al. even thought that using threshold SUVmax values to differentiate malignant from benign lesions is unrealistic [24]. Meantime, in our study, other factors should also be considered, including FDG uptake in mediastinal and hilar lymph nodes, the patients’ co-morbidities and nuclear medicine physician experience. In summary, SUVmax cannot be considered as a single diagnostic factor.
There are some limitations to our study. First, our systematic review was based on published studies, potential publication bias may have been present. Second, since there are few literatures on the value of PET-CT in the diagnosis of PH, so most of the literatures we cite are the value of PET-CT in the diagnosis of SPN, which means that our default PH belongs to a kind of SPN. Last, the number of patients is relatively small and these results will need to be verified in a large sample size.
Conclusion
In conclusion, our study showed that PET-CT might be a useful tool in the diagnosis of PH. The diagnostic sensitivity of PET-CT has been improved than CT, but it still has certain limitations on atypical PH lesions. The PET-CT diagnosis and SUVmax value may help patients with indeterminate SPNs with a better selection for surgical resection and radiological follow-up. But PET-CT can not be used as a single diagnostic approach, which should be combined with other methods and the patients’ history to make the most correct diagnosis.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Abbreviations
- PH:
-
Pulmonary hamartoma
- CT:
-
Computed tomography
- 18F-FDG PET-CT:
-
18F-Fluoro-d-glucose positron emission tomography-computed tomography
- SPN:
-
Small pulmonary nodules
- SUVmax:
-
Maximum standardized uptake values
- ROC:
-
Receiver operating characteristic
References
Park CM, Goo JM. Images in clinical medicine. “Popcorn” calcifications in a pulmonary chondroid hamartoma. N Engl J Med. 2009;360(12):e17.
Hochhegger B, Nin CS, Alves GR, Hochhegger DR, de Souza VV, Watte G, et al. Multidetector computed tomography findings in pulmonary hamartomas: a new fat detection threshold. J Thorac Imaging. 2016;31(1):11–4.
Jiang L, Huang Y, Tang Q, Zhao Q, Li Y, Wu X, et al. (18)F-FDG PET/CT characteristics of pulmonary sclerosing hemangioma vs. pulmonary hamartoma. Oncol Lett. 2018;16(1):660–5.
Liu F, Wang S. 18F-FDG PET/CT imaging of pulmonary chondroid hamartoma accompanied with fibrous dysplasia of femur: a misdiagnosed case report. Chin J Nucl Med Mol Imaging. 2017;37(08):492–3.
Tang K, Wang L, Lin J, Zheng X, Wu Y. The value of 18F-FDG PET/CT in the diagnosis of different size of solitary pulmonary nodules. Medicine (Baltimore). 2019;98(11): e14813.
Glaudemans AW, de Vries EF, Galli F, Dierckx RA, Slart RH, Signore A. The use of (18)F-FDG-PET/CT for diagnosis and treatment monitoring of inflammatory and infectious diseases. Clin Dev Immunol. 2013;2013: 623036.
Lei W, Zeng H, Zeng DX, Zhang B, Zhu YH, Jiang JH, et al. (18)F-FDG PET-CT: a powerful tool for the diagnosis and treatment of relapsing polychondritis. Br J Radiol. 2016;89(1057):20150695.
Lei W, Zeng DX, Chen T, Jiang JH, Wang CG, Zhu YH, et al. FDG PET-CT combined with TBNA for the diagnosis of atypical relapsing polychondritis: report of 2 cases and a literature review. J Thorac Dis. 2014;6(9):1285–92.
Divisi D, Barone M, Bertolaccini L, Zaccagna G, Gabriele F, Crisci R. Diagnostic performance of fluorine-18 fluorodeoxyglucose positron emission tomography in the management of solitary pulmonary nodule: a meta-analysis. J Thorac Dis. 2018;10(Suppl 7):S779–89.
Bunyaviroch T, Coleman RE. PET evaluation of lung cancer. J Nucl Med. 2006;47(3):451–69.
De Cicco C, Bellomi M, Bartolomei M, Carbone G, Pelosi G, Veronesi G, et al. Imaging of lung hamartomas by multidetector computed tomography and positron emission tomography. Ann Thorac Surg. 2008;86(6):1769–72.
Tatci E, Ozmen O, Ozturk A, Demirag F. Contribution of (18)F-FDG PET/CT in the differential diagnosis of pulmonary hamartomas and pulmonary carcinoids. Mol Imaging Radionucl Ther. 2021;30(2):101–6.
Liu Y, Wu N, Zhang R, Liang Y, Zhang W, Zhang H, et al. Positron emission tomography CT features of pulmonary hamartomas. Chin J Radiol. 2013;06:513–6.
Zhao J, Wang H. Differential diagnostic value of (18)F-FDG PET/CT in pulmonary carcinoids versus hamartomas. Acad Radiol. 2022;29(Suppl 2):S41–6.
Wang W, Song J, Shi J, Hu H, Wu Y, Yan J, et al. Slight uptake of (18)F-FDG on positron emission tomography in pulmonary hamartoma: a case report. Oncol Lett. 2015;10(1):430–2.
Li L, Jiang C, Tian R. A pulmonary chondromatous hamartoma resembling multiple metastases in the (18)F-FDG PET/CT scan. Hell J Nucl Med. 2016;19(2):176–8.
Lio E, Aisner DL, Askin FB, Kwak JJ. Giant pulmonary chondroid hamartoma: imaging and pathology correlation of a rare tumor demonstrated with bone scintigraphy and 18F-FDG PET/CT. Clin Nucl Med. 2015;40(1):79–81.
Feng Z, De-feng L, Guan-min W, Xue-mei D, Ya-ping X, Tao M. The diagnostic value of 18F-FDG PET/CT dual time point combined with thin-slice CT scan for solitary pulmonary nodules. Labeled Immunoassays and Clin Med. 2019;26(12):2079–83.
Coruh AG, Kul M, Kuru Oz D, Yenigun B, Cansiz Ersoz C, Ozalp Ates F, et al. Is it possible to discriminate pulmonary carcinoids from hamartomas based on CT features? Clin Imaging. 2020;62:49–56.
Liu J, Hong S, Jiang J, Zhou F, He L, Gong H, et al. CT manifestations and misdiagnosis of atypical pulmonary hamartoma. J Pract Radiol. 2019;35(5):730–3.
Fletcher JW, Kymes SM, Gould M, Alazraki N, Coleman RE, Lowe VJ, et al. A comparison of the diagnostic accuracy of 18F-FDG PET and CT in the characterization of solitary pulmonary nodules. J Nucl Med. 2008;49(2):179–85.
Uhlen N, Grundberg O, Jacobsson H, Sundin A, Dobra K, Sanchez-Crespo A, et al. 18F-FDG PET/CT Diagnosis of Bronchopulmonary Carcinoids Versus Pulmonary Hamartomas. Clin Nucl Med. 2016;41(4):263–7.
Liu Y, Wu N, Zhang R, Liang Y, Zhang W, Zhang H, et al. 18F-FDG PET-CT features of benign pulmonary nodules. Oncol Prog. 2013;06:513–6.
Sim YT, Goh YG, Dempsey MF, Han S, Poon FW. PET-CT evaluation of solitary pulmonary nodules: correlation with maximum standardized uptake value and pathology. Lung. 2013;191(6):625–32.
Christensen JA, Nathan MA, Mullan BP, Hartman TE, Swensen SJ, Lowe VJ. Characterization of the solitary pulmonary nodule: 18F-FDG PET versus nodule-enhancement CT. Am J Roentgenol. 2006;187(5):1361–7.
Ergonul AG, Akcam TI, Ozdil A, Turhan K, Cakan A, Cagirici U. Diagnostic value of (18)F-FDG-PET/CT in benign lung diseases. Kardiochir Torakochirurgia Pol. 2018;15(1):1–4.
Grgic A, Yuksel Y, Groschel A, Schafers HJ, Sybrecht GW, Kirsch CM, et al. Risk stratification of solitary pulmonary nodules by means of PET using (18)F-fluorodeoxyglucose and SUV quantification. Eur J Nucl Med Mol Imaging. 2010;37(6):1087–94.
Borghesi A, Tironi A, Benvenuti MR, Bertagna F, De Leonardis MC, Pezzotti S, et al. Pulmonary hamartoma mimicking a mediastinal cyst-like lesion in a heavy smoker. Respir Med Case Rep. 2018;25:133–6.
Hashimoto Y, Tsujikawa T, Kondo C, Maki M, Momose M, Nagai A, et al. Accuracy of PET for diagnosis of solid pulmonary lesions with 18F-FDG uptake below the standardized uptake value of 2.5. J Nucl Med. 2006;47(3):426–31.
Liu Y, Ghesani NV, Zuckier LS. Physiology and pathophysiology of incidental findings detected on FDG-PET scintigraphy. Semin Nucl Med. 2010;40(4):294–315.
Chang JM, Lee HJ, Goo JM, Lee HY, Lee JJ, Chung JK, et al. False positive and false negative FDG-PET scans in various thoracic diseases. Korean J Radiol. 2006;7(1):57–69.
Melloni G, Gajate AM, Sestini S, Gallivanone F, Bandiera A, Landoni C, et al. New positron emission tomography derived parameters as predictive factors for recurrence in resected stage I non-small cell lung cancer. Eur J Surg Oncol. 2013;39(11):1254–61.
Acknowledgements
Not applicable.
Funding
This study was supported by the Gusu youth medical talent (GSWS2020017, WL), The third level “333” high level talent training project of Jiangsu Province (No Grant Numbers, WL). The funding body did not play a role in the study design or data analysis presented in this manuscript.
Author information
Authors and Affiliations
Contributions
CZ and JY contributed to the conception of the study; SY and SM analyzed and interpreted the clinical data and imaging findings, and they were major contributors in writing the manuscript; WL and SB helped perform the analysis with constructive discussions. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This was a retrospective analysis study. The Ethics Committee of The First Affiliated Hospital of Soochow University approved the study. The requirement for informed consent was waived by the Ethics Committee of The First Affiliated Hospital of Soochow University because of the retrospective nature of the study.
Consent for publication
Not applicable.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ye, S., Meng, S., Bian, S. et al. Diagnosis value of 18F-Fluoro-d-glucose positron emission tomography-computed tomography in pulmonary hamartoma: a retrospective study and systematic review. BMC Med Imaging 23, 28 (2023). https://doi.org/10.1186/s12880-023-00981-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-023-00981-z