
Abstract
Background
Abstracts provide readers a concise and readily accessible information of the trials. However, poor reporting quality and spin (misrepresentation of research findings) can lead to an overestimation in trial validity. This methodological study aimed to assess the reporting quality and spin among randomized controlled trial (RCT) abstracts in pediatric dentistry.
Methods
We hand-searched RCTs in five leading pediatric dental journals between 2015 and 2021. Reporting quality in each abstract was assessed using the original 16-item CONSORT for abstracts checklist. Linear regression analyses were performed to identify factors associated with reporting quality. We evaluated the presence and characteristics of spin only in abstracts of parallel-group RCTs with nonsignificant primary outcomes according to pre-determined spin strategies.
Results
One hundred eighty-two abstracts were included in reporting quality evaluation. The mean overall quality score was 4.57 (SD, 0.103; 95% CI, 4.36–4.77; score range, 1–10). Only interventions, objective, and conclusions were adequately reported. Use of flow diagram (P < 0.001) was the only significant factor of higher reporting quality. Of the 51 RCT abstracts included for spin analysis, spin was identified in 40 abstracts (78.4%), among which 23 abstracts (45.1%) had spin in the Results section and 39 in the Conclusions Sect. (76.5%).
Conclusions
The reporting quality of RCT abstracts in pediatric dentistry is suboptimal and the prevalence of spin is high. Joint efforts are needed to improve reporting quality and minimize spin.
Similar content being viewed by others


Background
The research focus in pediatric dentistry has changed from publishing case reports to answering a focused problem [1]. With the introduction of evidence-based dentistry, clinicians are requested to make their clinical decisions through scientific evidence [2]. High-quality randomized controlled trials (RCTs) are considered evidence of the highest grade in the hierarchy of research designs and the gold standard in the evaluation of efficacy and safety of healthcare interventions [3], owing to their robust experimental design and execution. Despite excellent internal validity offered by well-designed RCTs, there are still concerns about the inaccurate reporting of study methods and results in published articles. This can introduce bias into conclusions and interpretations, and potentially mislead healthcare decision-making [4, 5].
Abstracts provide readers with a summary of trial information and are an essential means of disseminating research findings. Given the limited time and access constraints for critical reading, clinicians often rely only on abstracts to extract study information, decide whether to read full texts, or even make their clinical decisions. Therefore, accurate, complete and transparent reporting of abstract is crucial. In recognition of the importance of a well-written abstract, an extension of CONsolidated Standards Of Reporting Trials (CONSORT) statement has been released specifically for reporting of RCT abstracts in journals and conferences in 2008 [6]. However, the reporting quality of RCT abstract still remained inadequate in leading general medical journals and the field of dentistry [3, 7].
Currently, the CONSORT statement has been endorsed by hundreds of journals, requiring adherence to the guideline in their ‘Instructions to Authors’ [8], and a checklist of CONSORT items was provided to ensure reporting the key element. Nevertheless, authors can still intentionally or unintentionally misrepresent or misinterpret their study results, especially in RCTs with nonsignificant primary outcomes. Spin is defined as ‘use of specific reporting strategies, from whatever motive, to highlight that the experimental treatment is beneficial, despite a statistically nonsignificant difference for the primary outcome, or to distract the reader from statistically nonsignificant results’ [5]. Boutron et al. [5] were the first to define spin and developed spin strategies to systematically evaluate spin. Recent studies have indicated that the incidence of spin was common in biomedical research [9] and dentistry [10, 11]. Nevertheless, no guidelines on avoidance of spin have been developed.
As for now, the reporting quality and the incidence of spin among RCT abstracts in the field of pediatric dentistry have not been studied. Therefore, we aimed to (1) assess the reporting quality in recently published RCT abstracts in the field of pediatric dentistry; (2) identify factors associated with reporting quality; and (3) investigate the existence and characteristics of spin in these abstracts.
Methods
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist [12] for research reporting of observational studies was followed in this methodological study with a cross-sectional design (Additional file 1).
Study selection
Since RCTs published in high-impact journals are considered to have high potential impact on dental practice [3] and are more likely to be read. We selected five leading pediatric dental journals to identify potential RCT abstracts according to the 2020 Journal Citation Report [13] as a representative sample in present study. They are European Journal of Paediatric Dentistry (EJPD), International Journal of Paediatric Dentistry (IJPD), Journal of Clinical Pediatric Dentistry (JOCPD), Pediatric Dentistry (PD) and European Archives of Paediatric Dentistry (EAPD). Previous empirical studies have already employed this similar approach for evaluation of reporting quality [14,15,16].
Two authors (W.Y. and D.C.) hand-searched the five journal’s official online archives to identify RCT abstracts published from January 2015 to December 2021, independently and in duplicate. The search duration employed in this study was predetermined. Comparison between studies on the evaluation of reporting quality and spin in RCT abstracts across dental specialties is challenging due to variations in study design (e.g., search duration, inclusion/exclusion criteria) and the inherent subjectivity in assessment [17]. To ensure the comparability of findings, we chose the duration consistent with a previously published article conducted by our team, which aimed to evaluate the existence of spin in orthodontic RCT abstracts [16].
The titles and abstracts of the published articles were screened for relevance, followed by the screening of the full texts. Abstracts that met the eligibility criteria were included. Any discrepancies were resolved through discussion. As decided a prior, we only included abstracts of studies that satisfied the following criteria: human participants, interventions associated with health care, experimental studies, presence of a control group, and random assignment of participants to the study or control group. We excluded abstracts that belonged to non-RCTs, observational studies, in-suit studies, basic studies, quasi-experiment studies or RCTs combined with other study designs. Besides, conference abstracts were not included in this study.
Data extraction
The following information in each included abstract was extracted by two authors (F.G. and W.Y.) independently and in duplicate: title, journal name, publication year, continent (first author), multiple affiliations, number of authors, sample size, abstract word count, treatment arms, multi-center, statistician involvement, reported use of CONSORT statement in the Methods section, use of flow diagram, and reporting of the exact P-value [18], funding status (i.e. funded by industry, funded by others sources, and unfunded or unreported). Any disagreements were resolved via discussion with the other authors.
Assessment of reporting quality
The reporting quality of each included abstract was evaluated by two authors (F.G. and W.Y.) independently and in duplicate, using the original CONSORT for Abstract checklist and associated explanations [6]. Discrepancies were resolved through discussion with two experts (F.H. and H.H.). During quality assessment, 1 item (authors, including contact details for the corresponding author) was excluded as it was particularly related to conference abstracts. Each individual item was recorded as “1” if the item was adequately reported, or “0” if it was reported inadequately or absent. For items containing separate sub-items, only if all corresponding sub-items were adequately reported, the item would be scored a "1". Thereafter, for each abstract, an overall quality score (OQS; score range: 0 to 16) was calculated by adding up the score of each item. Furthermore, the reporting of 11 sub-items of applicable CONSORT quality items was documented to provide supplementary information [6].
Study selection for spin evaluation
Among included RCT abstracts in pediatric dentistry, only abstracts of superiority parallel-grouped RCTs which compared no less than two interventions and had a statistically nonsignificant primary outcome were included in spin evaluation. Although different classifications of spin strategies have evolved for different types of research [5, 19, 20], there has been no commonly accepted standard for classifying spin. The classification of spin strategies we adopted, which concentrated on superiority parallel-grouped RCT design with nonsignificant primary outcomes, was currently the most widely used in research related to spin [5]. Therefore, abstracts were excluded where the corresponding studies were equivalence, non-inferiority, crossover or factorial designs, cost-effectiveness analyses, as well as those that did not perform between-group statistical analyses. Two authors (W.Y. and X.F.) conducted the selection process independently and in duplicate. Any disagreements were resolved through discussion.
Extracted information on the primary outcomes
We identified the primary outcome(s) of each included abstract according to the source order list in previous research. [16, 17]. Primary outcome was the prespecified outcome considered of greatest importance and was the one used in the sample size calculation [6]. It could be explicitly reported as such in the full text. If none were explicitly described in full text, the outcome stated in sample size calculation would be considered. If not applicable, we took the primary outcome reported in corresponding trial registration. If it was not indicated in registration, the main/primary objective would be chosen as primary outcome. Any abstracts or corresponded full texts/registrations that did not contain a clearly identified primary outcome were excluded.
Evaluation of spin
The presence and strategy of spin used in the Results and Conclusions section of each included abstracts were evaluated and recorded (location and spread) respectively by two authors (F.G. and W.Y.) independently and in duplicate based on a pre-determined classification of spin strategies [5, 16, 17]. Any disagreements were resolved through discussion with two experts (F.H. and H.H.).
Spin was considered when:
-
(1)
Focusing on statistically significant results (i.e. focusing on only one statistically significant primary outcome or one significant timepoint of primary outcome irrespective of other nonsignificant primary outcomes, significant within-group comparison for primary outcomes, significant secondary outcomes, or significant subgroup analyses);
-
(2)
Focusing on statistically significant modified population of analyses (e.g., report per-protocol analyses);
-
(3)
Claiming equivalence or non-inferiority for statistically nonsignificant results;
-
(4)
Claiming efficacy with no consideration of the statistically nonsignificant primary outcome;
-
(5)
Acknowledging statistically nonsignificant results for the primary outcome but emphasizing the beneficial effect of treatment; and
-
(6)
Recommendation to use the treatment.
Other spin strategies that were apparent but failed to be classified into the above categories were recorded.
Statistical analyses
SPSS version 26 (IBM Corp, Armonk, NY, USA) was used for statistical analysis. Descriptive statistics were used to summarize characteristics, the overall reporting quality, the adequate reporting proportion of each checklist item/subitem, the presence and strategy of spin. Continuous data were expressed as means ± standard deviations (SDs) and 95% confidence interval (CI), while categorical data were presented as an absolute frequency and percentage.
Additionally, univariate and multivariate linear regression analyses were performed to investigate the association between reporting quality (OQS, dependent variable) and potential predictors: journal, publication year, continent, multiple affiliations, number of authors, sample size, abstract word count, treatment arms, multi-center, statistician involvement, reported use of CONSORT, use of flow diagram and exact P-value, funding status. We carried out univariable analysis first, then entered all variables with p < 0.05 into multivariable modeling. Significant violation of normality was not indicated in assessment of residuals. For the multivariate analysis, multicollinearity was detected using tolerance and variance inflation factor (VIF). Any predictor would be excluded from the final model, if it has a tolerance less than 0.1 and/ or VIF above 10 [21]. Statistical significance was defined as P < 0.05.
Results
Characteristics of include abstracts
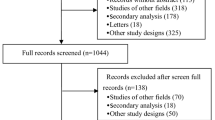
Figure 1 presents the process of abstract selection. A total of 197 abstracts were identified from official archives of five journals. After application of pre-determined eligible criteria, 182 RCT abstracts were included for assessment of reporting quality.

Flow chart of RCT abstract selection
Table 1 summarizes the characteristics of included RCT abstracts in five pediatric dental journals. Among the included abstracts, PD dominated the percentage of published abstracts (n = 50, 27.5%), followed by EAPD (n = 42, 23.1%) and JOCPD (n = 37, 20.3%). Over one-half abstracts were written by first author from Asia (n = 104, 57.1%), have 200–250 words (n = 91, 50.0%), and did not report the exact P-value (n = 108, 59.3%), with the number of authors being 4–7 (n = 117, 64.3%). About three-quarters of relevant RCTs of abstracts were conducted in single center, comparing two arms, and did not report using CONSORT statement. In terms of funding status, only 8 (4.4%) trials were funded by industry, 44 (24.2%) by other sources, and 130 (71.4%) were unfunded or unreported.
Reporting of general items
Table 2 presents the assessment results of reporting each individual item and sub-item. Figure 2 displays the percentage of each item reported in included abstracts in a more intuitive way. Half of abstracts (n = 97, 53.3%) can be identified as randomized through their title, and only 64 abstracts (35.2%) reported their trial design. In addition, a small percentage of abstracts provided details of trial registration (n = 3, 3.8%) and source of funding (n = 4, 2.2%).

The adequate reporting percentage (%) for each CONSORT checklist item in all the included 182 trials. a Outcome reported in Methods section. b Outcome reported in Results section
Reporting of trial methodology
A majority of abstracts adequately reported CONSORT items of interventions (n = 164, 90.1%) and objective (n = 180, 98.9%). In terms of participant, although 151 (83.0%) abstracts described the eligibility criteria for participants, only 11 (6.0%) provided information of settings of data collection. Besides, only 10 abstracts (5.5%) clearly defined the primary outcome of the trial in Methods section. For information regarding randomization, most abstracts (n = 117, 64.3%) reported random assignment, however, sequence generation and allocation concealment were not mentioned in any abstract. Among all included abstracts, 45 (24.7%) provided information on blinding, in which, 17 abstracts (9.3%) clearly specified who were blinded.
Reporting of trial results
Over half of abstracts (n = 93, 51.1%) reported the number of participants randomized to each group, but only a small percentage of abstracts (n = 19, 10.4%) described the number of participants analyzed in each group. The adoption of intention-to-treat analysis or per-protocol analysis was only stated in 2 abstracts (1.1%). In addition, 4 abstracts (2.2%) provided sufficient details of the primary outcome in Results section, including result for each group, the estimated effect size and its precision. Adverse events or side effects were mentioned in 6 abstracts (3.3%). Only one abstract reported the recruitment trial status (e.g., on-going, closed to recruitment and closed to follow-up).
Reporting of trial conclusions
A majority of abstracts (n = 154, 84.6%) reported conclusions that were in agreement with the trial results. Nevertheless, only 11 abstracts (6.0%) balanced the benefits and harms in the Conclusions section.
OQS and associated factors
The mean OQS of the included 182 abstracts was 4.57 (SD, 0.103; 95% CI, 4.36–4.77; score range, 1–10). Table 3 illustrates the results of linear regression analyses. The univariable analyses showed that journal (EAPD, P = 0.010), publication year (P = 0.007), sample size (P = 0.046), use of flow diagram (P < 0.001), and exact P-value (P = 0.016), were five factors significantly associated with OQS. Other factors including continent (P > 0.05), abstract word count (P = 0.523), number of authors (P = 0.942), treatment arms (P > 0.05), multi-center (P = 0.337), multiple affiliations (P = 0.127), statistician involvement (P = 0.356), reported used of CONSORT (P = 0.085) and funding status (P > 0.05) were nonsignificant We entered theses five factors into multivariable models (P < 0.001, R2 = 0.223, adjusted R2 = 0.188). Only use of flow diagram (P < 0.001) remained as a significant factor of higher reporting quality. Journal (P > 0.05), year (P = 0.403), sample size (P = 0.074) and exact P-value (P = 0.086) were nonsignificant factors. Figure 3 displayed the increasing trend of OQS over the years.

Frequency distribution of included RCTs in pediatric dentistry across years and journals and change of mean OQS over years. (N = 182)
Evaluation of spin
Among 182 RCT abstracts, 51 abstracts with statistically nonsignificant primary outcome were further included for spin evaluation. The primary outcome was identified mostly according to the outcome used in sample size calculation (n = 28, 54.9%), followed by full text (n = 18, 35.3%). Of the 51 RCT abstracts, spin was identified in 40 abstracts (78.4%), among which 23 abstracts (45.1%) had spin in the Results section and 39 in the Conclusions Sect. (76.5%). Moreover, 22 abstracts (43.1%) presented spin in both Results and Conclusions sections.
Table 4 demonstrates the frequency distribution of spin strategies in the Results and Conclusions sections, respectively. In the Results section, the most frequent spin strategy was focusing on significant within-group comparison for primary outcomes (n = 11, 21.6%), followed by focusing on only one statistically significant primary outcome or one significant timepoint of primary outcome irrespective of other nonsignificant primary outcomes (n = 10, 19.6%) and focusing on significant secondary outcomes (n = 8, 15.7%). Only one abstract focused on statistically significant subgroup analyses. In addition, one abstract was classified as other spin strategy since the trial interpreted the nonsignificant results as “comparable” between groups.
In the Conclusions section, claiming equivalence or non-inferiority for statistically nonsignificant results was the most common spin strategy (n = 12, 23.5%). Besides, 8 (15.7%) abstracts had spin due to claiming efficacy with no consideration of the statistically nonsignificant primary outcome, and 9 (17.6%) conclusions section of abstracts focused on significant secondary outcomes. Four (7.8%) abstracts concluded focusing on only one statistically significant primary outcome and with-group assessment, respectively. Other spin strategies were listed in Table 4.
Figure 4 displayed the trend of presence of spin over the years. The proportion of spin present in 2015 was the lowest (33.3%) with only 3 abstracts included. The prevalence of spin remained high between 2016 and 2021. However, there was no significance between year and the prevalence of spin (P = 0.376).

Frequency distribution of included RCTs in pediatric dentistry across years and journals and proportion of RCTs with spin. (N = 51)
Discussion
In this study, we evaluated the reporting quality of RCT abstracts published in five leading pediatric dental journals during the last 7 years. Our findings indicated that the reporting quality has much room for improvement, which was consistent with other research in the field of dentistry as a whole [3], endodontics [22], and orthodontics [18]. In addition, some essential aspects regarding methods and results were rarely reported, making it difficult for readers to assess the validity and reliability of RCT abstracts in pediatric dentistry.
The CONSORT statement and its extensions offer a standard way for authors to report their trials. This facilitates complete and transparent reporting while alleviating obstacles arising from inadequate or inaccurate reporting [6, 23, 24]. Earlier, Sarkis-Onofre et al. have concluded that active endorsement of the CONSORT statement by journals can improve the reporting quality of RCTs in dentistry [4]. CONSORT statement has been implemented by many journals [25, 26]. However, there were still discrepancies between specific instructions on how CONSORT should be used by authors in different journals and publishers, for instance, some journals may only require an accompanying completed CONSORT checklist in submission or request the inclusion of a CONSORT flow diagram [8]. In our study, only 22% abstracts mentioned used of CONSORT in Methods section. The effect of journal adherence to CONSORT guidelines has witnessed improvement in reporting quality [27]. Poor reporting quality as a consequence of not following CONSORT statement may prohibit clinicians from critically appraising the methodological quality and the validity of addiction RCT results, thus biasing the treatment effects in subsequent meta-analyses and clinical practice [28].
Among the 16 CONSORT quality items, only three items (interventions, objective, and conclusions) were adequately reported in most abstracts (> 80%), which were in line with the findings of previous studies in periodontology and implantology [29]. One possible explanation might be the structure format of RCT abstract required by journals which included headings of ‘Introduction, Methods, Results, and Conclusion’. Previous research has illustrated that highly structured RCT abstracts were associated with more complete trial reports in leading general medical [30]. Nevertheless, five journals we selected have requested submission of abstracts in structure formats in our study, preventing us from exploring the relationship between structure format and report quality in pediatric dentistry.
Transparent, accurate and complete description in methodology and results of the abstract were crucial for readers to critically appraise the efficacy or safety of intervention in a trial. However, inadequate reporting was common in medical research [22, 27], the same goes for our findings. In this study, a majority of items in the Methods and Results sections (including participant, outcome in the Methods section, blinding, numbers analyzed, recruitment outcome in the Results section, harms) and trial registration and funding were reported adequately only in less than 10% of the abstracts. No abstracts reported randomization. Such serious results should attract attention from publishers, editors, researchers, and readers.
Despite differences in reporting, trial design and execution, inadequate reporting in trial reports often leads to the omission or distortion of important methodology and results details [31]. This can mislead reader’s clinical decision making and result in avoidable research waste. The CONSORT for Abstracts guidelines has placed huge emphasis on the clear and sufficient detailed reporting of essential items in abstracts, such as outcome in the Method and Results section, participant, sequence generation and allocation concealment in randomization. [6] Previous research has pointed out that participant is important to determine the generalizability and applicability of the finding, and the lack of sequence generation and allocation concealment in randomization could generate exaggerated treatment effects and might interfere with clinicians’ assessment [6, 29]. As for the outcome, primary outcome should be clearly stated, which is the prespecified most appropriate outcome variable to address the study objectives, and usually the one used in the sample size calculation [32]. Insufficient reporting of outcome as shown in our study was a common issue in medical research [33, 34]. This indicated that not enough details of primary outcome were provided. The lack of clarity hinders clinicians or statisticians from fully understanding the precise measurements being assessed, thereby compromising the reproducibility of trials. [35].
In our study, after multivariable linear regression analysis, only flow diagram remained as a significant predictor of abstract reporting quality, indicating that RCTs reported use of flow diagram were significantly associated with higher OQS. The finding mirrored the results in previous studies [18, 36] and possible explanations might be that the use of a diagram showing participants flow was recommended by CONSORT guidelines [32]. They demonstrate the knowledge the CONSORT statements and/or trials [3]. The CONSORT has provided the structured flow diagram. Nevertheless, authors often present diagrams with different structures, ignoring some important elements such as the number of participants who actually receive allocated treatment [36]. Therefore, standardization and implementation of CONSORT flow diagram by journals is still needed.
This study was the first to appraise spin in pediatric dentistry, and 51 RCT abstracts which have nonsignificant primary outcomes were included for evaluation. Given the small sample size of included abstracts, we did not conduct regression analysis to explore potential factors associated with the presence of spin. Our study displayed that the occurrence of spin was high among RCT abstracts in pediatric dentistry (78.4%). Publication year was a nonsignificant factor associated with spin. The prevalence of spin has shown a great variation in different research areas and study designs [9]. In the field of dentistry, spin has been explored in dentistry as a whole (61.7%) [37], endodontics (85.0%) [22], orthodontics (62.2%) [16], and periodontology and implantology (69.9%) [17]. The prevalence of spin in academic publications necessitates research to investigate its impact and develop appropriate measurements for addressing this issue.
The frequencies of spin strategies in Results and Conclusions sections mirrored the findings in orthodontics [16]. Since we only included abstracts of superiority RCTs, the primary aim of this trial should concentrate on between-group comparison to show whether the investigated intervention was superior to a commonly accepted treatment or placebo [38]. Accounting for the limitation of word count, the most important result that should be clearly reported was the primary outcome, including results in each group, estimated effect size and its precision [6]. Authors who solely focus on the results of within-group comparisons in a superiority trial, risk misinterpreting it as a before-after study. This can result in inappropriate conclusions, such as claiming treatment equivalence, which distorts readers and impacts clinicians’ assessment about treatment application.
Abstracts with spin can impact clinicians’ interpretation of trial results and the dissemination of content in press releases and news coverage [39, 40]. The presence of spin in academic publications can be attributed to various factors. With the editors’ preference for publishing positive findings, researchers under publication pressure tend to manipulate or selectively report study findings to satisfy their vested interests [41]. This can introduce spin in publications. Besides, the absence of clear guidelines leaves researchers and reviewers with limited standardized guidance on how to accurately and objectively report research findings, increasing the likelihood of spin [37]. As for now, previous studies have identified some related factors associated with spin. Wu et al. [17] found that multi-center RCTs were less likely to have spin in abstracts in periodontology and implantology. In orthodontics, a significantly lower presence of spin was found in studies with international collaboration and trial registration [16]. These relevant factors gave insight into finding ways to address spin for publication.
Suggestions
Our study indicated that the reporting quality has much room for improvement and spin was prevalent among RCT abstracts in pediatric dentistry. Researchers and other stakeholders are recommended to make joint efforts to improve reporting quality and eliminate spin. Researchers in the field of pediatric dentistry should familiarize themselves with the CONSORT for abstract guidelines and adhere strictly to the report. They should also raise awareness of the presence and definition of spin. In this study, we found only a few (12.1%) abstracts mentioned statistician involvement in the full text. Previous research displayed that RCTs with statistician involvement were associated with a lower presence of spin and higher quality of the study [42, 43]. Statisticians' expertise ensures rigorous study design, accurate data interpretation, and reliable statistical analyses, enhancing the overall quality of the research [42]. Collaborating with statisticians can thus prompt the robustness and credibility of RCTs, leading to more reliable and trustworthy findings. Furthermore, we recommended researchers, peer-reviewers and editors receive specific training about recognizing spin, because appending simple instructions about spin to peer reviewers’ comments has shown no significant effect to reduce it [44].
Journal editors should take active endorsement of reporting guidelines, such as inclusion of CONSORT guidelines in instructions to authors and reviewers. The currently available reporting guidelines need to be expanded by adding specific instructions on avoiding spin to improve the presentation and interpretation of trial results and minimize the occurrence of spin. Besides, word count limit has been commonly considered a key constraint for detailed reporting and adherence to reporting guidelines [18]. As the CONSORT for Abstract statements has recommended, 250–300 word count would be enough to adequately report all items in the checklist [7]. Increasing word count and using highly structured format, such as the 12-heading format for RCT abstracts [30], have been proven to promote better reporting [45].
Other relevant stakeholder including readers, clinicians and funders should be capable of identifying spin to reduce avoidable research waste associated with inadequate reporting, and apprise the trial’s reliability and accuracy before applying it into practice.
Limitations
The current study has several limitations. Our study focused on RCT abstracts published in five prominent pediatric dentistry journals. The findings may not be representative of all pediatric RCTs. It is possible that less prestigious pediatric journals may publish studies with more issues. However, RCTs published in high-impact medical journals are considered to have a high potential to influence clinical practice [46]. Selecting abstracts on the basis of impact factor has been used widely in other studies [3, 47, 48]. Our recommendations are applicable to other RCT abstracts in pediatric dentistry as well.
Another limitation is that we only included RCTs that have nonsignificant primary outcomes for spin evaluation in pediatric dentistry, in which the prevalence of spin reported in current study may not be generalized to other study designs or other specialties in dentistry. Standardization of spin classification is needed to promote comparisons between different study designs. Moreover, the small sample size in the spin evaluation hindered statistical analysis to explore associated factors. Additionally, the inclusion of fewer than 15 abstracts per year (especially only 3 in 2011) compromises the reliability of assessing the trend of spin presence over time. On the other side, this observation highlights the inclination of pediatric dentistry journals to publish positive findings rather than negative ones. Finally, our study mirrors several studies focusing mainly on evaluation of reporting quality and spin within abstracts [22]. Further study is needed to identify spin in main text.
Conclusions
In summary, the reporting quality of RCT abstracts in pediatric dentistry is suboptimal. The prevalence of spin among RCT abstracts in pediatric dentistry is high. Joint efforts from researchers and other stakeholders are needed to improve reporting quality and minimize spin presence.
Availability of data and materials
The data underlying this article will be shared on reasonable request to the corresponding author.
Abbreviations
- CONSORT:
-
Consolidated Standards of Reporting Trials
- EAPD:
-
European Archives of Paediatric Dentistry
- EJPD:
-
European Journal of Paediatric Dentistry
- IJPD:
-
International Journal of Paediatric Dentistry
- JOCPD:
-
Journal of Clinical Pediatric Dentistry
- No:
-
Number
- PD:
-
Pediatric Dentistry
- RCT:
-
Randomized controlled trial
- VIF:
-
Variance inflation factor
References
Jayaraman J, Mallineni SK. Editorial: integration of evidence-based research and practice in preventive and pediatric dentistry. Front Oral Health. 2022;3:1017226.
Ismail AI, Bader JD. Evidence-based dentistry in clinical practice. J Am Dent Assoc. 2004;135(1):78–83.
Hua F, Deng L, Kau CH, Jiang H, He H, Walsh T. Reporting quality of randomized controlled trial abstracts: Survey of leading general dental journals. J Am Dent Assoc. 2015;146(9):669-678e661.
Sarkis-Onofre R, Poletto-Neto V, Cenci MS, Moher D, Pereira-Cenci T. CONSORT endorsement improves the quality of reports of randomized clinical trials in dentistry. J Clin Epidemiol. 2020;122:20–6.
Boutron I, Dutton S, Ravaud P, Altman DG. Reporting and interpretation of Randomized controlled trials with statistically nonsignificant results for primary outcomes. JAMA. 2010;303(20):2058–64.
Hopewell S, Clarke M, Moher D, Wager E, Middleton P, Altman DG, Schulz KF, Group C. CONSORT for reporting randomized controlled trials in journal and conference abstracts: explanation and elaboration. PLoS Med. 2008;5(1):e20.
Ghimire S, Kyung E, Kang W, Kim E. Assessment of adherence to the CONSORT statement for quality of reports on randomized controlled trial abstracts from four high-impact general medical journals. Trials. 2012;13(1):77.
Shamseer L, Hopewell S, Altman DG, Moher D, Schulz KF. Update on the endorsement of CONSORT by high impact factor journals: a survey of journal Instructions to Authors in 2014. Trials. 2016;17(1):301.
Chiu K, Grundy Q, Bero L. Spin’ in published biomedical literature: a methodological systematic review. PLoS Biol. 2017;15(9):e2002173.
Fang X, Wu X, Levey C, Chen Z, Hua F, Zhang L. Spin in the abstracts of randomized controlled trials in operative dentistry: a cross-sectional analysis. Oper Dent. 2022;47(3):287–300.
Roszhart JI, Kumar SS, Allareddy V, Childs CA, Elangovan S. Spin in abstracts of randomized controlled trials in dentistry: a cross-sectional analysis. J Am Dent Assoc. 2019;151(1):26–32.
Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, Poole C, Schlesselman JJ, Egger M. Strengthening the reporting of Observational studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4(10):e297.
2020 Journal Citation. Reports® Science Edition. https://jcr.clarivate.com/JCRJournalHomeAction.action.
Al-Namankany AA, Ashley P, Moles DR, Parekh S. Assessment of the quality of reporting of randomized clinical trials in paediatric dentistry journals. Int J Paediatr Dent. 2009;19(5):318–24.
Makou O, Eliades T, Koletsi D. Reporting, interpretation, and extrapolation issues (SPIN) in abstracts of orthodontic meta-analyses published from 2000 to 2020. Eur J Orthod. 2021;43(5):567–75.
Guo F, Fang X, Li C, Qin D, Hua F, He H. The presence and characteristics of ‘spin’ among randomized controlled trial abstracts in orthodontics. Eur J Orthod. 2021;43(5):576–82.
Wu X, Yan Q, Fang X, Hua F, Shi B, Tu Y-K. Spin in the abstracts of randomized controlled trials in periodontology and oral implantology: a cross-sectional analysis. J Clin Periodontol. 2020;47(9):1079–86.
Hua F, Walsh T, Glenny A-M, Worthington H. Reporting quality of randomized controlled trial abstracts presented at European orthodontic society congresses. Eur J Orthod. 2016;38(6):584–92.
Lazarus C, Haneef R, Ravaud P, Boutron I. Classification and prevalence of spin in abstracts of non-randomized studies evaluating an intervention. BMC Med Res Methodol. 2015;15:85.
Yavchitz A, Ravaud P, Altman DG, Moher D, Hrobjartsson A, Lasserson T, Boutron I. A new classification of spin in systematic reviews and meta-analyses was developed and ranked according to the severity. J Clin Epidemiol. 2016;75:56–65.
Norman GR, Streiner DL. Biostatistics: the bare essentials. 3rd ed. Hamilton: PMPH USA (BC Decker); 2008.
Fang X, Hua F, Riley P, Chen F, Zhang L, Walsh T, Chen Z. Abstracts of published randomized controlled trials in endodontics: reporting quality and spin. Int Endod J. 2020;53(8):1050–61.
Begg C, Cho M, Eastwood S, Horton R, Moher D, Olkin I, Pitkin R, Rennie D, Schulz KF, Simel D, et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA. 1996;276(8):637–9.
Moher D, Hopewell S, Schulz KF, Montori V, Gotzsche PC, Devereaux PJ, Elbourne D, Egger M, Altman DG. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c869.
Garrocho-Rangel A, Ruiz-Rodríguez S, Gaitán-Fonseca C, Pozos-Guillén A. Randomized clinical trials in pediatric dentistry: application of evidence-based dentistry through the CONSORT statement. J Clin Pediatr Dent. 2019;43(4):219–30.
Jayaraman J. Guidelines for reporting randomized controlled trials in paediatric dentistry based on the CONSORT statement. Int J Paediatr Dent. 2020;31(Suppl 1):38–55.
Alnamankany A, Ashley P. Assessment of the quality of reporting of randomized clinical trials in paediatric dentistry: a comparative systematic review. J Taibah Univ Med Sci. 2020;15(1):1–7.
Vassar M, Jellison S, Wendelbo H, Wayant C, Gray H, Bibens M. Using the CONSORT statement to evaluate the completeness of reporting of addiction randomised trials: a cross-sectional review. BMJ Open. 2019;9(9):e032024.
Faggion CM Jr, Giannakopoulos NN. Quality of reporting in abstracts of randomized controlled trials published in leading journals of periodontology and implant dentistry: a survey. J Periodontol. 2012;83(10):1251–6.
Hua F, Walsh T, Glenny A-M, Worthington H. Structure formats of randomised controlled trial abstracts: a cross-sectional analysis of their current usage and association with methodology reporting. BMC Med Res Methodol. 2018;18(1):6.
Huwiler-Müntener K, Jüni P, Junker C, Egger M. Quality of reporting of randomized trials as a measure of Methodologic Quality. JAMA. 2002;287(21):2801–4.
Altman DG, Schulz KF, Moher D, Egger M, Davidoff F, Elbourne D, Gøtzsche PC, Lang T. The revised CONSORT statement for reporting randomized trials: explanation and elaboration. Ann Intern Med. 2001;134(8):663–94.
Hua F, Sun Q, Zhao T, Chen X, He H. Reporting quality of randomised controlled trial abstracts presented at the SLEEP Annual meetings: a cross-sectional study. BMJ Open. 2019;9(7):e029270.
Shaqman M, Al-Abedalla K, Wagner J, Swede H, Gunsolley JC, Ioannidou E. Reporting quality and spin in abstracts of randomized clinical trials of periodontal therapy and Cardiovascular Disease outcomes. PLoS One. 2020;15(4):e0230843.
Vetter TR, Mascha EJ. Defining the primary outcomes and justifying secondary outcomes of a study: usually, the fewer, the Better. Anesth Analg. 2017;125(2):678–81.
Egger M, Jüni P, Bartlett C. Value of flow diagrams in reports of randomized controlled trials. JAMA. 2001;285(15):1996–9.
Eleftheriadi I, Ioannou T, Pandis N. Extent and prevalence of spin in randomized controlled trials in dentistry. J Dent. 2020;100:103433.
Christensen E. Methodology of superiority vs. equivalence trials and non-inferiority trials. J Hepatol. 2007;46(5):947–54.
Boutron I, Altman DG, Hopewell S, Vera-Badillo F, Tannock I, Ravaud P. Impact of spin in the abstracts of Articles Reporting results of randomized controlled trials in the field of Cancer: the SPIIN Randomized Controlled Trial. J Clin Oncol. 2014;32(36):4120–6.
Boutron I, Haneef R, Yavchitz A, Baron G, Novack J, Oransky I, Schwitzer G, Ravaud P. Three randomized controlled trials evaluating the impact of spin in health news stories reporting studies of pharmacologic treatments on patients’/caregivers’ interpretation of treatment benefit. BMC Med. 2019;17(1):105.
Emerson GB, Warme WJ, Wolf FM, Heckman JD, Brand RA, Leopold SS. Testing for the Presence of positive-outcome Bias in peer review: a Randomized Controlled Trial. Arch Intern Med. 2010;170(21):1934–9.
Delgado-Rodriguez M, Ruiz-Canela M, De Irala-Estevez J, Llorca J, Martinez-Gonzalez A. Participation of epidemiologists and/or biostatisticians and methodological quality of published controlled clinical trials. J Epidemiol Community Health. 2001;55(8):569–72.
Guo F, Zhao T, Zhai Q, Fang X, Yue H, Hua F, He H. ‘Spin’ among abstracts of randomised controlled trials in sleep medicine: A research-on-research study. Sleep. 2023;2:zsad041.
Ghannad M, Yang B, Leeflang M, Aldcroft A, Bossuyt PM, Schroter S, Boutron I. A randomized trial of an editorial intervention to reduce spin in the abstract’s conclusion of manuscripts showed no significant effect. J Clin Epidemiol. 2021;130:69–77.
Helbach J, Hoffmann F, Pieper D, Allers K. Reporting according to the preferred reporting items for systematic reviews and meta-analyses for abstracts (PRISMA-A) depends on abstract length. J Clin Epidemiol. 2023;154:167–77.
Berwanger O, Ribeiro RA, Finkelsztejn A, Watanabe M, Suzumura EA, Duncan BB, Devereaux PJ, Cook D. The quality of reporting of trial abstracts is suboptimal: survey of major general medical journals. J Clin Epidemiol. 2009;62(4):387–92.
Nascimento DP, Almeida MO, Scola LFC, Vanin AA, Oliveira LA, Costa LCM, Costa LOP. Letter to the editor – not even the top general medical journals are free of spin: a wake-up call based on an overview of reviews. J Clin Epidemiol. 2021;139:232–4.
Pulikkotil SJ, Jayaraman J, Nagendrababu V. Quality of abstract of systematic reviews and meta-analyses in paediatric dentistry journals. Eur Arch Paediatr Dent. 2019;20(5):383–91.
Acknowledgements
None
Funding
This work was supported by the Chinese Stomatological Association COS Basic Research Fund (No. COS-B2021-08), and the Wuhan University School of Medicine Teaching Research Project (No. 2021074).
Author information
Authors and Affiliations
Contributions
Study concepts: F.H. and H.H.;Study design: F.G., W.Y. and F.H.; Manuscript writing: F.G. and W.Y.; Manuscript editing: D.Q., X.F., F.H. and H.H.; Data extraction: W.Y., D.Q. and X.F.; Data elaboration and interpretation: F.G., W.Y., F.H. and H.H.; Statistical analysis: F.G., W.Y.; Manuscript revision and approval of submission in its present form: F.G., W.Y., D.Q., X.F., F.H. and H.H.;All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable. This study does not involve human participants, human data or human tissue.
Consent for publication
Not applicable. This study does not involve individual data.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
STROBE Statement—checklist of items that should be included in reports of observational studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Guo, F., Ye, W., Qin, D. et al. Abstracts of randomized controlled trials in pediatric dentistry: reporting quality and spin. BMC Med Res Methodol 23, 263 (2023). https://doi.org/10.1186/s12874-023-02085-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-023-02085-2