
Abstract
Background
Spin represents specific reporting strategies, either intentional or unintentional, to convince the reader that the beneficial effect of the experimental intervention in terms of efficacy and safety is greater than that shown by the results. The objectives of this study were to 1) develop a classification of spin specific to non-randomized studies assessing an intervention and 2) estimate the prevalence of spin in abstracts of reports of such studies.
Methods
In a first step, we developed a specific classification of spin for non-randomized studies by a literature review and pilot study. In a second step, 2 researchers trained in the field of methodology evaluated the prevalence of spin in the abstract of all non-randomized studies assessing an intervention published in the BioMed Central Medical Series journals between January 1, 2011 and December 31, 2013. All disagreements were resolved by consensus. We also determined whether the level of spin in abstract conclusions was high (spin reported without uncertainty or recommendations for further trials), moderate (spin reported with some uncertainty or recommendations for further trials) or low (spin reported with uncertainty and recommendations for further trials).
Results
Among the 128 assessed articles assessed, 107 (84 %) had at least one example of spin in their abstract. The most prevalent strategy of spin was the use of causal language, identified in 68 (53 %) abstracts. Other frequent strategies were linguistic spin, inadequate implications for clinical practice, and lack of focus on harm, identified in 33 (26 %), 25 (20 %), and 34 (27 %) abstracts respectively. Abstract conclusions of 61 (48 %) articles featured a high level of spin.
Conclusion
Abstract of reports of non-randomized studies assessing an intervention frequently includes spin. Efforts to reduce the prevalence of spin in abstract for such studies are needed.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Spin, or distortion of study findings, can be used by authors to enhance their study findings more than the results justify [1, 2]. Recent studies demonstrated a high prevalence of spin in study reports. Spin was found in more than half of the abstract conclusions of randomized controlled trials with statistically non-significant results for the primary outcome [3]; moreover, one third of reports of diagnostic accuracy studies contained a form of over-interpretation [4]. The spin used consisted mainly of a focus on statistically significant results (within-group comparison, secondary outcomes, subgroup analyses, modified population of analyses); or interpreting statistically non significant results for the primary outcomes as showing treatment equivalence or comparable effectiveness. A recent study in the field of cancer found that the prevalence of spin has increased over time [5]. In the same field, a randomized controlled trial demonstrated that spin in abstracts could modify a reader’s interpretation of study results [6].
Non-randomized studies are commonly used in medical research to evaluate interventions. They are particularly useful to draw conclusions about the safety or efficacy of interventions in real-world settings, to assess rare or long-term adverse events or when randomization is not possible (e.g., surgical procedures). However, these designs have important limitations. Non randomized designs are also susceptible to many type of spin which could be same or different from those previously described [7]. Particularly, contrary to randomized clinical trials, they may not allow for establishing causal inferences but rather, only an association [8–10].
Our study aimed to 1) develop a classification of spin for non-randomized studies assessing therapeutic interventions and 2) estimate the prevalence of spin in the abstracts of non-randomized studies evaluating a therapeutic intervention published in BioMed Central Medical Series journals.
Methods
Development of a classification of spin
Spin was defined as the use of specific reporting strategies, either intentional or unintentional, to convince the reader that the beneficial effect of the experimental treatment in terms of efficacy and safety is higher than is actually shown by the data.
To develop the classification of spin, we performed a literature review of studies of spin for other study designs [3–5, 9, 11] as well as studies of distorted presentation and interpretation of findings from non-randomized studies [12–19]. From these data, we developed a preliminary classification, discussed among the authors and tested by two 2 researchers (CL and RH) with a sample of 15 articles. The classification was discussed until consensus was achieved among the authors.
Prevalence of spin in abstracts
We selected a sample of reports of non-randomized studies evaluating an intervention published in 25 journals of the BioMed Central Medical Series that regularly publish clinical studies. We selected these journals because they are open-access and publish reports of non-randomized studies evaluating therapeutic interventions from a large range of medical specialties.
Search strategy
We searched MEDLINE via PubMed (search date January 21, 2014) for all articles published in the 25 BioMed Central Medical Series journals between January 1, 2011 and December 31, 2013. The list of selected journals and complete search strategy are respectively in Additional files 1 and 2.
Study identification
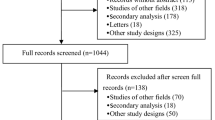
One researcher (CL) screened all titles, abstracts and, if necessary, the full-text articles of the citations retrieved and selected all reports of non-randomized studies assessing a therapeutic intervention defined as a pharmacological or non-pharmacological treatment (e.g., pharmaceutical drugs, surgery, therapeutic education, rehabilitation, paramedical care etc.) proposed to patients to improve their health. We excluded medico-economic assessments of therapeutic interventions and protocols of observational studies (Fig. 1). As a quality control, a second trained researcher (RH) assessed a random selection of 10 % of articles retrieved by the bibliographic search to ensure that some articles were not missed. This second researcher did not retrieve any missed articles in this subset. For every included article, we retrieved the full-text article and the abstract.

Flowchart for the selection and inclusion of articles from the BioMed Central Medical Series Journals assessing therapeutic interventions through non-randomized designs and reasons for exclusion
Data extraction
For each selected article, 2 researchers (CL and RH) trained in the field of methodology independently read the abstract and full-text article and collected data on the general characteristics of the study–study design, sample size, type of therapeutic intervention, comparator, funding sources and whether registration was recorded–using a standardized data-extraction form. They systematically searched for spin in the abstracts using the classification system developed previously.
Level of spin in abstract conclusions
The 2 researchers evaluated the level of spin in the abstract conclusions. A low level of spin was defined as spin reported with uncertainty in the framing and recommendations for further trials, a moderate level as spin reported with some uncertainty in the framing or recommendations for further trials, and a high level as spin reported without any uncertainty or recommendations for further trials.
Any discrepancies were solved by consensus and, if needed, by consultation with a third researcher (IB).
Statistical analysis
Data are reported with median (Q1–Q3) for continuous variables and number (%) for categorical variables. Statistical analyses involved use of R 2.15.0 (http://www.R-project.org, the R Foundation for Statistical Computing, Vienna, Austria) and any appropriate packages.
Results
Selected articles
The search strategies retrieved 1,734 citations; 128 were selected and assessed. The description of included articles is in Table 1. The study designs of the selected articles were prospective cohort studies (n = 42, 33 %), historical cohort studies (n = 39, 30 %) and before–after studies (n = 40, 31 %). The interventions evaluated were drugs (n = 51, 40 %), non-pharmacologic interventions (e.g., surgery, device or equipment, behavioral intervention or participative; n = 48, 38 %), and therapeutic strategy (n = 29, 23 %). The median [Q1–Q3] sample size was 130 [51–458]. The funding source was mainly non-profit (n = 54, 42 %), but for 41 articles (32 %) the funding source was not reported or was unclear.
Classification of spin
The classification of spin we developed was divided into 3 categories: misleading reporting, misleading interpretation and inadequate extrapolation of the results. Each of these categories included several spin strategies, which are detailed below. Table 2 provides a clear definition of each spin category with an example of spin:
-
Misleading reporting of the results was defined as incomplete reporting of the study results that could be misleading for the reader. This type of spin included 1) not reporting adverse events or lack of focus on harms (e.g., no warning on important safety issues), 2) selective reporting of outcomes favoring the beneficial effect of the experimental treatment (e.g., statistically significant results for efficacy outcomes or statistically non-significant results for harm outcomes), 3) misleading reporting of study design, 4) use of linguistic spin or “hype” (i.e., rhetorical manipulations to convince the readers of the beneficial effect of the treatment such as “excellent” results, “encouraging” outcomes, “a trend toward significance”), 5) no consideration of limitations, and 6) selective citation of other studies.
-
Inadequate interpretation of the results was defined as misleading interpretation of the study results overestimating the beneficial effect of the intervention. This type of spin included 1) claiming a beneficial effect of the intervention despite statistically non-significant results, 2) claiming an equivalent effect of the interventions for statistically non-significant results despite wide confidence interval, 3) claiming that the treatment is safe for statistically non-significant safety outcomes despite lack of power, 4) concluding a beneficial effect despite no comparison test performed, 5) interpretation of the results according to statistical significance (p-value) instead of clinical relevance, or 6) claiming a causal effect between the intervention being assessed and the outcome of interest despite a non-randomized design. Use of causal language was defined as any statement addressing the causal relationship of the intervention and outcomes with 1) modal auxiliary verbs, with the intervention as the subject and the outcome as a direct object (e.g., “Surgical experience could shorten the duration of TVT [tension-free vaginal tape] surgery.” [20]); 2) use of terms belonging to the semantic field of causal relationship (e.g., “effective”, “improve”, “enhance”); or 3) use of a tone inferring a strong result (e.g., “The results demonstrate” or “This study shows that”). We did not consider that causal language was used when authors stated only a co-occurrence between the intervention and the outcome (e.g., “subjects with symptomatic bipolar disorders who relapse frequently showed improvements in each of these areas after treatment with RLAI [risperidone long-acting injection]” [21]). We did not consider causal language as spin in studies using a propensity score or instrumental variables [22].
-
Inadequate extrapolation of the results was defined as an inappropriate generalization of the study result by inadequate 1) extrapolation from the population, interventions or outcome actually assessed in the study to a larger population, different interventions or outcomes, or 2) inadequate implications for clinical practice.
Prevalence of spin in abstracts
In total, 107 (84 %) reports had at least one type of spin in their abstracts (Table 3). The median number of type of spin per abstract identified was 2 (Q1–Q3 1–3, range 0–6). The most prevalent spin strategy related to the use of causal language identified in 68 (53 %) abstracts. For example, in a before–after study including 7 patients, the authors stated “Erythropoietin … increases the oxygen partial pressure in the brain tissue … in poor grade SAH [subarachnoid aneurismal hemorrhage] … patients with severe cerebral vasospasm” [23] and in another prospective study including 22 patients, they stated “[Bi-level positive airway pressure-spontaneous/timed] BiPAP S/T with AVAP [average volume assured pressure support] … facilitates rapid recovery of consciousness when compared to traditional BiPAP S/T in patients with chronic obstructive pulmonary disease and hypercapnic encephalopathy” [24].
Other frequent strategies of spin were linguistic spin, inadequate implications for clinical practice and lack of focus on harms, in 33 (26 %), 25 (20 %), and 34 (27 %) abstracts, respectively. For example, we considered linguistic spin frequent when authors indicated that the results were close to significance, despite a p-value > 0.05. For example, in a prospective study including 662 patients, the authors stated “a tendency towards lower all-cause mortality at 3 months with use of Aspirin + dipyramidol” (p = 0.12) [25] and others used superlatives or “hype” to highlight a beneficial effect of the intervention assessed (e.g., “high potential,” “considerably helps,” “excellent results”). Inadequate implications for clinical practice occurred mainly when authors extrapolated some recommendations for clinical practice from their results (e.g., in a retrospective study of 42 patients: “it is a suitable therapeutic option not only for initial drainage but also for salvage therapy” [26]).
We identified selective reporting in more than 12 % of abstracts, (e.g., in a before–after study of 23 patients: “[Internet-based cognitive behavior therapy] ICBT… with therapist support reduces [obsessive-compulsive disorder] OCD symptoms, depressive symptoms and improves general functioning” [27], with no report of the lack of improvement in quality of life found in this study). Also, in 13 % of abstracts, authors concluded on the safety of the intervention solely by a statistically non-significant difference in safety outcome despite lack of power. For example, in a historical cohort of 54 patients, the authors reported “Intravenous sodium valproate is as effective as intravenous phenytoin as the first-line treatment in status epilepticus … with no significant cardiovascular compromise” [28], despite more than twice as many deaths in the intravenous penytoin group (30 % vs 11 %) although not statistically significant.
Level of spin in abstract conclusions
We classified 61 articles (48 %) as containing a high level of spin in abstract conclusions, 24 (19 %) a moderate level of spin and 17 (13 %) a low level of spin. Only 26 articles (20 %) did not have spin in their abstract conclusions.
Discussion
To our knowledge, this is the first study to develop and use a classification of spin for non-randomized studies. Of the 128 reports we evaluated, 84 % of abstracts contained at least one type of spin and 48 % featured a high level of spin. Use of causal language was the most frequent spin strategy. Yet, the use of causal claims is misleading in the interpretation of non-randomized studies because these designs are unable to control for every confounding factor.
Our findings are consistent with results of other studies. Many of the spin strategies we observed are shared with those identified in randomized controlled trials. Spin strategies are varied and frequent and might lead to misleading interpretation of the study results. This situation is problematic because it has been demonstrated [6] that spin in the abstract conclusions of randomized controlled trial reports could bias the interpretation of the results by clinicians [29].
A particular feature of our work was the important prevalence of causal claims in abstracts of non-randomized studies. Causal language is a specific spin strategy for non-randomized studies. Such designs, as opposed to randomized studies, do not allow for concluding a cause-and-effect link between the assessed intervention and the observed outcome but rather, provide information only about association [8, 30, 31]. Some studies have explored the causal language in such designs. Cofield et al. [30] observed a 31 % rate of causal language in a series of 525 peer-reviewed papers on obesity and nutrition. Brown et al. [32] evidenced a 26 % to 50 % rate of studies ascribing greater inferential strength than the study design warranted. Causal claims in epidemiology are a cornerstone of the interpretation of results [33], especially for complex interventions for which randomization is difficult or impossible [11]. In 2012, journal editors of the HEART Group published an editorial review about “the importance of matching language to type of evidence” [34] and concluded with a plea to investigators and editors to “carefully select language used during reporting to match the type of study conducted.” The rating of causal inference by researchers was assessed in a study of 38 randomized clinical trials and 35 non-randomized clinical trials [35]. The results highlighted that authors “might have overstated the strength of causal inference in the abstracts of non-randomized clinical trials, but appeared to report causality appropriately in the main text.”
Our study has several limitations. First, our sample is not representative of all non-randomized studies assessing therapeutic interventions indexed in PubMed. We choose the BioMed Central series of medical journals because it is an open-access and open peer-review collection involving a wide variety of medical specialties, therapeutic interventions and study designs. These journals are also strongly involved in the requirement of reporting guidelines (STROBE, CONSORT) and transparency policies (ICMJE) from authors. Consequently, we cannot extrapolate our results to other journals. Second, the assessment of spin strategies is subjective because the interpretation of the results highly depends on the context. To address this issue, 2 trained researchers independently collected the data using a standardized form, with discrepancies resolved by consensus and the involvement of a third researcher if necessary. Third, our study could not determine whether the spin strategies were conscious attempts to show the treatment as more beneficial than it actually was. We did not assess the impact of spin in abstracts of non-randomized studies on the interpretation of such studies, which can differ depending on the category of spin considered. It is important to recognize that an abstract may contain some spin item but actually be balanced overall. We attempted to take into account this issue and assessed the level of spin in the abstracts conclusions provided some elements about the importance of uncertainty and call for further research for the global tone of a conclusion.
Further studies should be conducted to determine the impact of spin on the readers’ interpretation of the study results. It is possible that the presence of spin item could be counterbalanced by other element in the reporting of abstracts.
Conclusion
We found a high prevalence of spin in abstracts of reports of non-randomized studies. Misleading interpretation of results of such studies could lead to inadequate clinical practices and erroneous beliefs in the effects of therapeutic interventions. The classification we developed should facilitate efforts to reduce the prevalence of spin.
Abbreviations
- (Q1–Q3):
-
Interquartile Range
- A-CPR:
-
Automated CardioPulmonary Resuscitation
- AVAPS:
-
Average Volume Assured Pressure Support
- BiPAP S/T:
-
Bi-level Positive Airway Pressure–Spontaneous / Timed
- CGI-SCH:
-
Clinical Global Impression-Schizophrenia
- CPR:
-
CardioPulmonary Resuscitation
- HR:
-
Hazard Ratio
- ICBT:
-
Internet-based Cognitive Behavior Therapy
- OCD:
-
Obsessive–Compulsive Disorder
- RLAI:
-
Risperidone Long-Acting Injection
- SAH:
-
Sub-Arachnoïdal Hemorrhage
- TVT:
-
Tension-free Vaginal Tape
References
Horton R. The rhetoric of research. BMJ. 1995;310(6985):985–7.
Fletcher RH, Black B. “Spin” in scientific writing: scientific mischief and legal jeopardy. Med Law. 2007;26(3):511–25.
Boutron I, Dutton S, Ravaud P, Altman DG. Reporting and interpretation of randomized controlled trials with statistically nonsignificant results for primary outcomes. JAMA. 2010;303(20):2058–64.
Ochodo EA, De Haan MC, Reitsma JB, Hooft L, Bossuyt PM, Leeflang MM. Overinterpretation and misreporting of diagnostic accuracy studies: evidence of “spin”. Radiology. 2013;267(2):581–8.
Vera-Badillo FE, Shapiro R, Ocana A, Amir E, Tannock IF. Bias in reporting of end points of efficacy and toxicity in randomized, clinical trials for women with breast cancer. Ann Oncol. 2013;24(5):1238–44.
Boutron I, Altman DG, Hopewell S, Vera-Badillo F, Tannock I, Ravaud P: Impact of spin in the abstract of articles reporting results of Randomised Controlled Trials in the field of cancer, the SPIIN Randomised Controlled Trial. Journal of Clinical Oncology 2014 (in press).
Dahabreh IJ, Kent DM. Can the learning health care system be educated with observational data? JAMA. 2014;312(2):129–30.
Parascandola M, Weed DL. Causation in epidemiology. J Epidemiol Community Health. 2001;55(12):905–12.
Vandenbroucke JP. Why do the results of randomised and observational studies differ? BMJ. 2011;343:d7020. doi:10.1136/bmj.d7020.
Vandenbroucke JP. When are observational studies as credible as randomised trials? Lancet. 2004;363(9422):1728–31.
Rickles D. Causality in complex interventions. Med Health Care Philos. 2009;12(1):77–90.
Mathieu S, Boutron I, Moher D, Altman DG, Ravaud P. Comparison of registered and published primary outcomes in randomized controlled trials. JAMA. 2009;302(9):977–84.
Bland JM, Altman DG. Comparisons against baseline within randomised groups are often used and can be highly misleading. Trials. 2011;12(264):1745–6215.
Hernandez AV, Pasupuleti V, Deshpande A, Thota P, Collins JA, Vidal JE. Deficient reporting and interpretation of non-inferiority randomized clinical trials in HIV patients: a systematic review. PLoS One. 2013;8:5.
Al-Marzouki S, Roberts I, Marshall T, Evans S. The effect of scientific misconduct on the results of clinical trials: a Delphi survey. Contemp Clin Trials. 2005;26(3):331–7.
Chan KB, Man-Son-Hing M, Molnar FJ, Laupacis A. How well is the clinical importance of study results reported? An assessment of randomized controlled trials. CMAJ. 2001;165(9):1197–202.
Chan AW, Altman DG. Identifying outcome reporting bias in randomised trials on PubMed: review of publications and survey of authors. BMJ. 2005;330(7494):28.
Hewitt CE, Mitchell N, Torgerson DJ. Listen to the data when results are not significant. BMJ. 2008;336(7634):23–5.
Linden A. Identifying spin in health management evaluations. J Eval Clin Pract. 2011;17(6):1223–30.
Ito H, Yamanaka H, Hagiwara M, Furuuchi T, Matsumoto K, Kanai K, et al. Efficacy of tension-free vaginal tape compared with transobturator tape in the treatment of stress urinary incontinence in women: analysis of learning curve, perioperative changes of voiding function. BMC Urol. 2011;11(13):1471–2490.
Macfadden W, Adler CM, Turkoz I, Haskins JT, Turner N, Alphs L. Adjunctive long-acting risperidone in patients with bipolar disorder who relapse frequently and have active mood symptoms. BMC Psychiatry. 2011;11(171):11–171.
Dekkers OM. On causation in therapeutic research: observational studies, randomised experiments and instrumental variable analysis. Prev Med. 2011;53(4–5):239–41.
Helbok R, Shaker E, Beer R, Chemelli A, Sojer M, Sohm F, et al. High dose erythropoietin increases brain tissue oxygen tension in severe vasospasm after subarachnoid hemorrhage. BMC Neurol. 2012;12(32):1471–2377.
Briones Claudett KH, Briones Claudett M, Chung Sang Wong M, Nuques Martinez A, Soto Espinoza R, Montalvo M, et al. Noninvasive mechanical ventilation with average volume assured pressure support (AVAPS) in patients with chronic obstructive pulmonary disease and hypercapnic encephalopathy. BMC Pulm Med. 2013;13(12):1471–2466.
Arnarsdottir L, Hjalmarsson C, Bokemark L, Andersson B. Comparative evaluation of treatment with low-dose aspirin plus dipyridamole versus aspirin only in patients with acute ischaemic stroke. BMC Neurol. 2012;12(67):1471–2377.
Inatomi O, Bamba S, Shioya M, Mochizuki Y, Ban H, Tsujikawa T, et al. Threaded biliary inside stents are a safe and effective therapeutic option in cases of malignant hilar obstruction. BMC Gastroenterol. 2013;13(31):13–31.
Andersson E, Ljotsson B, Hedman E, Kaldo V, Paxling B, Andersson G, et al. Internet-based cognitive behavior therapy for obsessive compulsive disorder: a pilot study. BMC Psychiatry. 2011;11(125):11–125.
Tiamkao S, Sawanyawisuth K, Chancharoen A. The efficacy of intravenous sodium valproate and phenytoin as the first-line treatment in status epilepticus: a comparison study. BMC Neurol. 2013;13(98):1471–2377.
Kaptchuk TJ. Effect of interpretive bias on research evidence. BMJ. 2003;326(7404):1453–5.
Cofield SS, Corona RV, Allison DB. Use of causal language in observational studies of obesity and nutrition. Obes Facts. 2010;3(6):353–6.
Shahar E, Shahar DJ. On the causal structure of information bias and confounding bias in randomized trials. J Eval Clin Pract. 2009;15(6):1214–6.
Brown AW, Bohan Brown MM, Allison DB. Belief beyond the evidence: using the proposed effect of breakfast on obesity to show 2 practices that distort scientific evidence. Am J Clin Nutr. 2013;98(5):1298–308.
Blettner M, Heuer C, Razum O. Critical reading of epidemiological papers. A guide. Eur J Public Health. 2001;11(1):97–101.
Kohli P, Cannon CP. The importance of matching language to type of evidence: avoiding the pitfalls of reporting outcomes data. Clin Cardiol. 2012;35(12):714–7. doi:10.1002/clc.22066. Epub 2012 Nov 28.
Li LC, Moja L, Romero A, Sayre EC, Grimshaw JM. Nonrandomized quality improvement intervention trials might overstate the strength of causal inference of their findings. J Clin Epidemiol. 2009;62(9):959–66.
Acknowledgment
The authors would like to acknowledge Dr Youri Yordanov (funded by Assistance Publique Hôpitaux de Paris (AP-HP) for his critical revision of the manuscript.
This study received no specific funding.
CL, PR, IB were funded by the University Paris Descartes and the Assistance Publique Hôpitaux de Paris (AP-HP)
RH was funded by the Assistance Publique Hôpitaux de Paris (AP-HP)
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
CL participated in the study concept and design, acquisition of data, analysis and interpretation of the data, and drafting of the manuscript. RH participated in acquisition of data. PR participated in the study concept and design, analysis and interpretation of the data, and the critical revision of the manuscript. IB participated in the study concept and design, acquisition of data, analysis and interpretation of the data, drafting of the manuscript and the critical revision of the manuscript. All authors read and approved the final manuscript.
Additional files
Additional file 1:
Selected journal from the BioMed Central medical journals series. (PDF 7 kb)
Additional file 2:
Complete bibliographic request. (PDF 10 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lazarus, C., Haneef, R., Ravaud, P. et al. Classification and prevalence of spin in abstracts of non-randomized studies evaluating an intervention. BMC Med Res Methodol 15, 85 (2015). https://doi.org/10.1186/s12874-015-0079-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-015-0079-x