
Abstract
Background
Lipoprotein(a) [Lp(a)] elevation is an important risk factor for coronary artery disease (CAD). However, the correlation between Lp(a) elevations and the risk of recurrent cardiovascular events in patients with established cardiovascular disease is controversial. Some studies have shown that Low-density lipoprotein cholesterol (LDL-C) levels may influence the association between Lp(a) and cardiovascular risk. Our study aims to explore the correlation between Lp(a) elevations and cardiovascular risk in patients with different LDL-C levels.
Methods
We included 516 patients who received coronary stents due to acute coronary syndrome (ACS) and followed them for three years. They were divided into low-Lp(a) group and high-Lp(a) group according to Lp(a) levels, and the incidence of major adverse cardiovascular events (MACE) and acute coronary events (ACE) was compared between the two groups. Then the patients were divided into three subgroups (S1:LDL-C ≥ 1.8 mmol/L; S2:1.4 ≤ LDL-C < 1.8 mmol/L; S3:LDL-C < 1.4 mmol/L). The correlation between Lp(a) elevations and cardiovascular risk in different subgroups was analysed by Cox proportional hazards models.
Results
The incidence of MACE and ACE in the high-Lp(a) group was significantly higher than those in the low-Lp(a) group (P < 0.05). Lp(a) elevations had independent prognostic value from the statistical point of view (MACE: HR = 1.63, 95%CI = 1.12–2.38, P = 0.012; ACE: HR = 1.70, 95%CI = 1.03–2.81, P = 0.037). Subgroup analysis showed that Lp(a) elevations increased cardiovascular risk when LDL-C ≥ 1.4 mmol/L. However, this correlation no longer existed when LDL-C levels were very low (< 1.4 mmol/L) (MACE: HR = 0.49, 95%CI = 0.17–1.42, P = 0.186; ACE: HR = 0.68, 95%CI = 0.18–2.61, P = 0.570).
Conclusions
Lp(a) elevations are associated with recurrent cardiovascular events when LDL-C levels are high, but this association may change when LDL-C levels are extremely low. CAD patients with combination of LDL-C ≥ 1.4 mmol/L and Lp(a) elevations shall be considered as high-risk groups and require further medication for the reduction of their LDL-C levels.
Similar content being viewed by others

Introduction
CAD has a high mortality and disability rate and is one of the primary diseases threatening human health worldwide. Survivors of ACE are still at an increased risk of recurrence despite receiving standard revascularization and secondary prophylaxis treatment. It is estimated that ischemic events’ recurrence rate within one year has reached up to 9.2% after ACS [1]. Accurately identifying the risk of recurrent cardiovascular events in patients with CAD is of great significance to guide secondary prevention and improve prognosis.
Lp(a) is an isomeric protein composed of apolipoprotein(a), apolipoprotein B-100 and lipids such as cholesterol, phospholipids and triglycerides [2]. Previous studies have demonstrated that Lp(a) can promote atherosclerosis, inflammation and thrombosis, and is an independent risk factor for CAD [3, 4]. The 2019 ESC/EAS guideline for dyslipidemia management recommended that every adult should have at least one Lp(a) level assessment in their lifetime [5]. However, the value of Lp(a) in predicting recurrent cardiovascular events in CAD patients receiving secondary prevention strategies is controversial. Some studies have shown that Lp(a) elevations are associated with an increased risk of cardiovascular events in patients irrespective of LDL-C [6,7,8], but others have demonstrated Lp(a) is associated with plaque volume and MACE when LDL-C levels are high, and this association does not exist when LDL-C levels are low [9,10,11]. This study aims to explore the association between Lp(a) elevations and cardiovascular risk in patients with different LDL-C levels, especially those with very low LDL-C (< 1.4 mmol/L).
Methods
The studied population
In this retrospective study, we reviewed a total of 618 patients with ACS [unstable angina (UA), non-ST-elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI)] who received coronary stent implantation in Hangzhou First People's Hospital Affiliated to Zhejiang University School of Medicine from January 1 to December 31, 2017. All patients received standard medication recommended by national guidelines after stent implantation [12, 13]. Patients received dual antiplatelet therapy (100 mg aspirin and 75 mg clopidogrel/180 mg ticagrelor) for at least 12 months and Single antiplatelet therapy (100 mg aspirin or 75 mg clopidogrel) for lifelong. All patients received 10 mg rosuvastatin or 20 mg atorvastatin for lipid-lowering treatment (LLT), with ezetimibe added directly for baseline LDL-C greater than 3.4 mmol/L. Other drugs were prescribed at the discretion of the patient's treating physician.
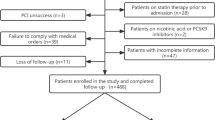
Exclusion criteria: 1. The residual stenosis of target vessel after the operation was more than 20%, TIMI blood flow was less than Grade-III, or serious complications occurred; 2. The patient discontinued or changed the medication without authorization during the follow-up; 3. The LDL-C level fluctuated significantly during the follow-up; 4. Basic information was missing or blood lipids were not monitored as required; 5. the patients had the coronary artery bypass grafting history; 6. The patients had severe hepatic and renal function deficiency; 7. The patients with an estimated survival time of less than 3 years; 8. Loss of follow-up.
Figure 1 shows the flow chart of the study. A total of 516 cases were included in this study. After 3 years of follow-up (average 31.5 months), 114 (22.1%) patients developed MACE and 64 (12.4%) patients developed ACE. It has been demonstrated that the association between Lp(a) and CAD risk is continuous and curvilinear, when Lp(a) exceeds a certain level, CAD risk increases significantly [14]. In China, this critical value is generally considered to be 30 mg/dL [15]. Therefore, we divided patients into low-Lp(a) group (< 30 mg/dL) and high-Lp(a) group (≥ 30 mg/dL) according to the Lp(a) levels at 1 month follow-up. In the subgroup analysis, they were further divided into S1 (LDL-C ≥ 1.8 mmol/L), S2 (1.4 ≤ LDL-C < 1.8 mmol/L), and S3(LDL-C < 1.4 mmol/L) according to LDL-C levels at 1 month follow-up.

Study flow chart
Data collection and follow-up
We recorded demographic data, cardiovascular risk factors, laboratory data and coronary angiography reports of all patients by the electronic medical record system. Cardiovascular risk factors included age, gender, body mass index, smoking status, diabetes, hypertension, and family history. All the patients received fasting blood collection before percutaneous coronary intervention (PCI), and the blood samples were measured and analyzed by the biochemical laboratory of Hangzhou First People's Hospital Affiliated to Zhejiang University School of Medicine. Coronary angiography and PCI are completed by experienced cardiovascular experts.
Patients were followed up through outpatient and inpatient records and telephone contacts for medication use, blood lipids control, and endpoint events at the 36 months after PCI. All patients received outpatient follow-up and repeated measurement of lipids in the first month after discharge. During the follow-up period after discharge, each patient had at least two blood lipids measurements.
Study endpoints
The end points were MACE and ACE. MACE included cardiogenic death, non-fatal myocardial infarction or ischemic stroke, unplanned coronary revascularization, and hospitalization related to UA. Unplanned coronary revascularization referred to ischemia driven revascularization and stenosis driven revascularization. Stenosis driven revascularization was defined as revascularization performed when angiographic review showed significant exacerbation of stenosis without angina symptoms. ACE included STEMI, NSTEMI and UA.
Statistical analysis
The categorical variables were represented as total cases [cases (%)] and analyzed by chi-square test or Fisher's exact test. The continuous variables that met the normal distribution were represented as mean ± SD and analyzed by t-test or variance analysis. Continuous variables with non normal distribution were represented as median (interquartile interval) and analyzed by nonparametric test. Kaplan–Meier curve and the log-rank test were performed to compare the event-free survival among the groups. Cox proportional hazards models were performed to determine the hazard ratio (HR) and 95% confidence interval (CI) for MACE and ACE. All the reported p values in this study are 2-sided and P < 0.05 indicated statistical significance.
Results
Baseline characteristics
The average age of the patients involved in this study was 66.0 ± 9.8 years, including 350 males (67.8%). As shown in Table 1, the levels of total cholesterol (TC), LDL-C and triglyceride were significantly decreased after LLT and lifestyle improvement (P < 0.05). The Lp(a) levels at 1-month follow-up were higher than the baseline (P < 0.05), which related to the use of statins. And there was no notable change in the high-density lipoprotein cholesterol (HDL-C) levels (P > 0.05). Table 2 summarized the baseline characteristics of the patients.
The baseline TC (4.60 ± 1.08 vs. 4.24 ± 1.18, P = 0.001), LDL-C (2.68 ± 0.84 vs. 2.43 ± 0.97, P = 0.001) and HDL-C (1.14 ± 0.29 vs. 1.05 ± 0.27, P = 0.001) in the high-Lp(a) group were higher than those in the low-Lp(a) group. At 1-month follow-up, the TC (3.48 ± 0.65 vs. 3.23 ± 0.71, P < 0.001) and LDL-C (1.75 ± 0.50 vs. 1.60 ± 0.55, P = 0.002) in the high-Lp(a) group were still higher, but there was no statistical difference in HDL-C between the two groups (1.11 ± 0.28 vs. 1.08 ± 1.01, P = 0.606). Higher creatinine (90.77 ± 22.01 vs. 86.99 ± 16.71, P = 0.034), female (39.74% vs. 29.04%, P = 0.018), total coronary occlusion (26.49% vs. 17.26%, P = 0.017) and Triple-vessel lesion (48.34% vs. 38.90%, P = 0.048) were more common to be found in the high-Lp(a) group. There was no statistical significance in other characteristics between the two groups (P > 0.05).
Endpoint events
After 3 years of follow-up (average 31.5 months), 114 MACE and 64 ACE were recorded. As shown in Table 3, The incidence of MACE (P = 0.003) and ACE (P = 0.006) in the High-Lp(a) group was significantly higher than that in the low-Lp(a) group. Further analysis of MACE showed that the rates of hospitalization related to UA (P = 0.026) and unplanned coronary revascularization (P = 0.008) were higher in high-Lp(a) group. The overall incidence of cardiogenic death and nonfatal myocardial infarction or ischemic stroke was low, and there was no statistical difference observed between the two groups (P > 0.05).
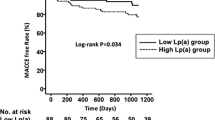
Subsequently, we divided the patients into three subgroups according to LDL-C levels (S1: LDL-C ≥ 1.8 mmol/L; S2: 1.4 ≤ LDL-C < 1.8 mmol/L; S3: LDL-C < 1.4 mmol/L; S0: the entire sample). Kaplan–Meier survival curve was used to compare the correlation between Lp(a) elevations and cardiovascular outcomes in the entire sample and subgroups. As shown in Figs. 2, 3, 4 and 5, Lp(a) elevations were associated with a higher incidence of MACE and ACE in S0 and S1 (P < 0.05). For patients with intermediate levels of LDL-C (S2), Lp(a) elevations were closely related to MACE (P < 0.05). The incidence of ACE in the high-Lp (a) group was also higher than that in the low-Lp (a) group, but the difference was not statistically significant (P > 0.05). Lp(a) elevations in S3 had no correlation with MACE and ACE, even showed an opposite trend.

The Kaplan–Meier survival curves analysis of the entire sample

The Kaplan–Meier survival curves analysis of S1

The Kaplan–Meier survival curves analysis of S2

The Kaplan–Meier survival curves analysis of S3
Cox regression analysis was performed to determine the HR and 95% CI for MACE and ACE. As shown in Table 4, after adjusting for confounding factors such as LDL-C, elevated Lp(a) remained an important risk factor for MACE (HR = 1.63, 95%CI = 1.12–2.38, P = 0.012) and ACE (HR = 1.70, 95%CI = 1.03–2.81, P = 0.037). However, in subgroup analysis, we found that this association was not maintained in patients with LDL-C < 1.4 mmol/L. Patients with LDL-C ≥ 1.8 mmol/L and high-Lp(a) had a 2.33-fold increased risk of recurring ACE than those with low-Lp(a) (HR = 2.33, 95%CI = 1.15–4.72, P = 0.019), and the risk of MACE was also relatively higher (HR = 1.62, 95% CI = 0.95–2.77). In the subgroup of LDL-C between 1.4 and 1.8 mmol/L, patients with Lp(a) elevations had a significantly higher risk of MACE (HR = 2.65, 95%CI = 1.31–5.36, P = 0.007). They were also at higher risk of ACE, but the difference was not statistically significant (HR = 2.01, 95% CI = 0.77–5.23). On the contrary, neither MACE (HR = 0.49, 95% CI = 0.17–1.42, P = 0.186) nor ACE (HR = 0.68, 95% CI = 0.18–2.61, P = 0.570) had any correlation with Lp(a) elevations when LDL-C < 1.4 mmol/L.
Discussion
Our study demonstrated that the correlation between Lp(a) and cardiovascular risk is affected by LDL-C levels. In patients with LDL-C ≥ 1.4 mmol/l, Lp(a) elevations are closely related to MACE and ACE, but there is no correlation in patients with LDL < 1.4 mmol/l. The results emphasize the importance of controlling LDL-C in patients with CAD once again, and provides a new reference for the formulation of lipid-lowering strategies. CAD patients with combination of LDL-C ≥ 1.4 mmol/L and Lp(a) elevations shall be considered as high-risk groups and require further medication for the reduction of their LDL-C levels.
Controlling LDL-C is the cornerstone of the prevention and treatment of atherosclerotic cardiovascular diseases (ASCVD). To further reduce cardiovascular risk, the 2019 ESC/EAS guideline suggested that the LDL-C levels in patients with extremely high risk ASCVD should be controlled below 1.4 mmol/L [5]. According to the guideline, the LDL-C control target of patients with CAD is less than 1.4 mmol/L. However, the current lipids control of CAD patients is not ideal. There are more than 126 million people worldwide suffering from CAD [16], but less than 16% of them achieve the target of LDL-C < 1.4 mmol/L [17]. The risk of recurrent cardiovascular events varies greatly among patients with CAD. Hence, it is of great significance to accurately identify patients at high risk of recurrent cardiovascular events for the guidance of intensive LLT.
Lp(a) is a low-density lipoprotein-like particle that has long been regarded as a risk factor for cardiovascular disease. Prior research has confirmed that Lp(a) elevations are independently associated with the risk of CAD [4, 18]. However, the correlation between Lp(a) elevations and recurrent cardiovascular risk in patients with CAD is controversial. Many studies have demonstrated Lp(a) elevations are not predictive for cardiovascular outcomes in patients medically well controlled [19,20,21]. Considering that LDL-C levels are higher in general population and lower in CAD patients receiving LLT, some scholars attribute the differences in the association between Lp(a) and cardiovascular risk across studies to differences in LDL-C levels. They claim that Lp(a) levels are associated with plaque load and MACE at the high LDL-C levels, and this association has changed when LDL-C levels decreased [9, 22]. On the contrary, some studies have shown that Lp(a) elevations are associated with an increased risk of cardiovascular events in patients with CAD irrespective of LDL-C [6, 7]. A recent study conducted a separate analysis of CAD patients with LDL-C ≤ 1.8 mmol/L and found Lp(a) levels are independently associated with MACE and recurrent MI in patients with well-controlled LDL-C [23].
We carried out this study to better understand the association between Lp(a), LDL-C and recurrent cardiovascular events in patients with CAD. According to the study results, we support the view that the correlation between Lp(a) and the risk of recurrent cardiovascular events was affected by the levels of LDL-C. The mechanism leading to this unique association is not yet clear. It has been reported that The degradation of Lp(a) is partly mediated by the LDL receptors (LDL-R), high-levels of LDL-C may occupy the receptors, competitively inhibit Lp(a) catabolism and enhance the biological effect of Lp(a) [24]. We speculate that patients with very low LDL-C levels tend to have high levels or activity of LDL-R and strong metabolism capacity for Lp(a). Even if Lp(a) levels are high, they can be timely metabolized and the biological effects are weakened. On the contrary, patients with high LDL-C have low levels or activity of LDL-R, Lp(a) can not be metabolized efficiently so that the biological effects are amplified. In order to prove that our results are not caused by accidental factors, we analyzed the patients with LDL-C ≤ 1.8 mmol/L (S2 + S3) and found that there was a positive correlation between Lp(a) elevations and endpoint events, which was consistent with the report of Ren et al. [23]. In addition, when analyzing the entire sample, we found that Lp(a) elevations were independently related to MACE and ACE, which were also consistent with prior reports [6, 7]. Since the proportion of patients with combination of extremely low LDL-C and elevated Lp(a) is very small in clinical practice, we speculate that they play a small role in the statistical analysis of the entire sample and can be easily masked. Therefore, different results were obtained in the holistic analysis and subgroup analysis.
The plasma concentration of Lp(a) tends to remain constant throughout life[25]. But the levels of Lp(a) increased after treatment in our study. It could be attributed to statins. A meta-analysis have shown that statin treatment is associated with an 11% increase in the geometric mean of Lp(a) concentrations compared to placebo[26]. Therefore, monitoring Lp(a) after treatment may be more helpful than baseline Lp(a) in predicting the cardiovascular risk of CAD patients. The recent guidelines and expert consensus emphasize that the cardiovascular risk of CAD patients should be further stratified to identify the most vulnerable patients who need to control LDL-C < 1.4 mmol/L [27,28,29]. Based on our results, we believe the levels of Lp(a) after treatment are helpful to identify the patients at high risk of recurrent cardiovascular events. The patients with combination of LDL-C ≥ 1.4 mmol/L and Lp(a) elevations shall be considered as the vulnerable ones and need to further reduce their LDL-C levels below 1.4 mmol/L.
Limitations
Firstly, this is a single-center study including all ACS patients who underwent PCI in Hangzhou First People's Hospital Affiliated to Zhejiang University School of Medicine within one year. The sample size is relatively small (n = 516). In some results, HR and 95%CI were valuable, but statistically insignificant (P > 0.05). This may be due to the insufficient sample size, so our conclusions need to be further verified by larger clinical studies. Secondly, indicators such as LDL-C differ between the acute and stable phases of CAD. However, most patients measured blood lipids only at admission and during a specific follow-up period. Therefore, there is a lack of data to explain the effect of ACS induced lipids fluctuations on the results.
Conclusions
Lp(a) elevations are associated with recurrent cardiovascular events when LDL-C levels are high, but this association may change when LDL-C levels are extremely low. Patients with combination of LDL-C ≥ 1.4 mmol/L and Lp(a) elevations shall be considered as high-risk groups and require further medication for the reduction of their LDL-C levels. In recent years, some new treatments have been shown to reduce both LDL-C and Lp(a) levels, such as antisense oligonucleotides and PCSK9 inhibitors, which will certainly bring more benefits to the high-risk patients with CAD.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- Lp(a):
-
Lipoprotein(a)
- CAD:
-
Coronary artery disease
- ACS:
-
Acute coronary syndrome
- MACE:
-
Major adverse cardiovascular events
- ACE:
-
Acute coronary events
- UA:
-
Unstable angina
- NSTEMI:
-
Non-ST-elevation myocardial infarction
- STEMI:
-
T-elevation myocardial infarction
- LLT:
-
Lipid-lowering therapy
- TC:
-
Total cholesterol therosclerotic
- LDL-C:
-
Low-density lipoprotein cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- ASCVD:
-
Atherosclerotic cardiovascular disease
- LDL-R:
-
Low-density lipoprotein receptors
References
Hess CN, Clare RM, Neely ML, Tricoci P, Mahaffey KW, James SK, et al. Differential occurrence, profile, and impact of first recurrent cardiovascular events after an acute coronary syndrome. Am Heart J. 2017;187:194–203.
Cegla J, France M, Marcovina SM, Neely R, Dermot G. Lp(a) level: when and how to measure it. Ann Clin Biochem. 2021;58:16–21.
Tada H, Takamura M, Kawashiri M. Lipoprotein(a) as an old and new causal risk factor of atherosclerotic cardiovascular disease. J Atheroscler Thromb. 2019;26:583–91.
Emerging Risk Factors Collaboration, Erqou S, Kaptoge S, Perry PL, Di Angelantonio E, et al. Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009;302(4):412–23.
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41:111–88.
O’Donoghue ML, Fazio S, Giugliano RP, Stroes ESG, Kanevsky E, et al. Lipoprotein(a), PCSK9 Inhibition, and cardiovascular risk. Circulation. 2019;139(12):1483–92.
Hoogeveen RC, Ballantyne CM. Residual cardiovascular risk at low LDL: remnants, Lipoprotein(a), and inflammation. Clin Chem. 2021;67(1):143–53.
Szarek M, Bittner VA, Aylward P, Baccara-Dinet M, Bhatt DL, et al. Lipoprotein(a) lowering by alirocumab reduces the total burden of cardiovascular events independent of low-density lipoprotein cholesterol lowering: ODYSSEY OUTCOMES trial. Eur Heart J. 2020;41(44):4245–55.
Maher VM, Brown BG, Marcovina SM, Hillger LA, Zhao XQ, Albers JJ. Effects of Lowering Elevated LDL Cholesterol on the Cardiovascular Risk of Lipoprotein(A). JAMA. 1995;274:1771–4.
Afshar M, Rong J, Zhan Y, Chen HY, Engert JC, et al. Risks of incident cardiovascular disease associated with concomitant elevations in Lipoprotein(a) and low-density lipoprotein cholesterol-the Framingham Heart Study. J Am Heart Assoc. 2020;9(18):e014711.
O’Donoghue ML, Morrow DA, Tsimikas S, Sloan S, Ren AF, Hoffman EB, et al. Lipoprotein(a) for risk assessment in patients with established coronary artery disease. J Am Coll Cardiol. 2014;63:520–7.
Thiele H, Desch S, Waha S. Acute myocardial infarction in patients with ST-segment elevation myocardial infarction: ESC guidelines 2017. Herz. 2017;42:728–38.
Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2020;41:3495–7.
Nordestgaard BG, Chapman MJ, Ray K, Borén J. Lipoprotein(a) as a cardiovascular risk factor: current status. Eur Heart J. 2010;31(23):2844–53.
Joint committee issued Chinese guideline for the management of dyslipidemia in adults. [2016 Chinese guideline for the management of dyslipidemia in adults]. Zhonghua Xin Xue Guan Bing Za Zhi. 2016; 44(10):833–853.
Dai H, Much AA, Maor E. Global, regional, and national burden of ischemic heart disease and its attributable risk factors, 1990–2017: results from the global Burden of Disease Study 2017. Eur Heart J Qual Care Clin Outcomes. 2020;8:50–60.
Noack F, Schwaab B, Voeller H, Eckrich K, Guha M, et al. The current LDL-C target <1.4mmol/l of the ESC is achieved in less than 16% of patients with Coronary Heart Disease despite effective lipid-lowering therapy: data from the LLT-R registry. Eur Heart J. 2020;41:ehaa946.2998.
Clarke R, Peden JF, Hopewell JC, Kyriakou T, Goel A, et al. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med. 2009;361(26):2518–28. https://doi.org/10.1056/NEJMoa0902604.
Gencer B, Rigamonti F, Nanchen D, Vuilleumier N, Kern I, et al. Prognostic value of elevated lipoprotein(a) in patients with acute coronary syndromes. Eur J Clin Invest. 2019;49(7):e13117.
Forbes CA, Quek RG, Deshpande S, Worthy G, Wolff R, et al. The relationship between Lp(a) and CVD outcomes: a systematic review. Lipids Health Dis. 2016;17(15):95.
Puri R, Ballantyne CM, Hoogeveen RC, Shao M, Barter P, et al. Lipoprotein(a) and coronary atheroma progression rates during long-term high-intensity statin therapy: Insights from SATURN. Atherosclerosis. 2017;263:137–44.
Gencer B, Rigamonti F, Nanchen D, Vuilleumier N, Kern I, Aghlmandi S, et al. Prognostic value of elevated lipoprotein(a) in patients with acute coronary syndromes. Eur J Clin Invest. 2019;49:e13117.
Ren Y, Pan W, Li X, Wang S, Lv H, et al. The predictive value of Lp(a) for adverse cardiovascular event in ACS patients with an achieved LDL-C target at follow up after PCI. J Cardiovasc Transl Res. 2021;15:67–74.
Cai A, Li L, Zhang Y, Mo Y, Li Z, Mai W, et al. Baseline LDL-C level and Lp(a) level elevations portend a high risk of coronary revascularization in patients after stent placement. Dis Markers. 2013;35:857–62.
Sahebkar A, Simental-Mendía LE, Pirro M, Banach M, Watts GF, Sirtori C, et al. Impact of ezetimibe on plasma lipoprotein(a) concentrations as monotherapy or in combination with statins: a systematic review and meta-analysis of randomized controlled trials. Sci Rep. 2018;8:17887.
Tsimikas S, Gordts PLSM, Nora C, Yeang C, Witztum JL. Statin therapy increases lipoprotein(a) levels. Eur Heart J. 2020;41(24):2275–84.
Group of atherosclerosis and coronary heart disease, Chinese society of Cardiology, editorial board of Chinese Journal of Cardiology. Chinese expert consensus on lipid management of very high-risk atherosclerotic cardiovascular disease patients. Chin J Cardiol 2020;48: 280–6.
Robinson JG, Jayanna MB, Brown AS, Aspry K, Orringer C, Gill EA, et al. Enhancing the value of PCSK9 monoclonal antibodies by identifying patients most likely to benefit: a consensus statement from the National Lipid Association. J Clin Lipidol. 2019;13:525–37.
Jellinger PS, Handelsman Y, Rosenblit PD, Bloomgarden ZT, Fonseca VA, Garber AJ, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr Pract. 2017;23:1–87.
Acknowledgements
The authors express their gratitude to cardiac interventional therapy center of Hangzhou First People's Hospital Affiliated to Zhejiang University School of Medicine for their cooperation and assistance.
Funding
None.
Author information
Authors and Affiliations
Contributions
LJZ contributed to the conception and design of the work. JMZ and XBJ contributed to the analysis and interpretation of the study data. BBG and YH contributed to patients follow-up. LZJ drafted the manuscript. JYH and LZ critically revised the manuscript. All authors provided final approval and agree to be accountable for all aspects of work, ensuring integrity and accuracy. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol for the study was approved by the ethics committee of the Hangzhou first people's Hospital Affiliated to Medical College of Zhejiang University. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from each participant at each examination phase.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Univariate COX analysis results.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhu, L., Zheng, J., Gao, B. et al. The correlation between lipoprotein(a) elevations and the risk of recurrent cardiovascular events in CAD patients with different LDL-C levels. BMC Cardiovasc Disord 22, 171 (2022). https://doi.org/10.1186/s12872-022-02618-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02618-5