
Abstract
Background
Remimazolam tosilate (RT) is a novel short-acting GABA (A) receptor agonist that has a rapid recovery from procedural sedation and can be fully reversed by flumazenil. To date, there have been relatively few articles comparing RT and propofol for general anesthesia. This study aimed to assess the efficacy and safety of RT with or without flumazenil compared with propofol in general anesthesia for day surgery.
Methods
115 patients scheduled for day surgery were randomized into three groups: RT (n = 39), RT + flumazenil (n = 38) and propofol (n = 38). The primary endpoints were anesthesia induction time and time until fully alert. Anesthesia success rate, bispectral index (BIS) values, injection pain, opioid and vasopressor dosages, postoperative recovery profiles and perioperative inflammatory and cognitive changes were assessed. Any adverse events were recorded.
Results
Induction times were similar among the three groups (P = 0.437), but the median time until fully alert in patients treated with RT was longer than that of the propofol or RT + flumazenil groups (17.6 min vs. 12.3 min vs. 12.3 min, P < 0.001). The three groups had comparable postoperative recovery quality and inflammatory and cognitive state changes (P > 0.05). Smaller percentages of patients who received RT (26.3%) and RT + flumazenil (31.6%) developed hypotension during anesthesia maintenance compared with propofol (68.4%), and consequently less ephedrine (P < 0.001) and phenylephrine (P = 0.015) were needed in the RT group. Furthermore, serum triglyceride levels were lower (P < 0.001) and injection pain was much less frequent in the RT with or without flumazenil groups compared with the propofol group (5.3% vs. 0% vs. 18.4%).
Conclusion
RT permits rapid induction and comparable recovery profile compared with propofol in general anesthesia for day surgery, but has a prolonged recovery time without flumazenil. The safety profile of RT was superior to propofol in terms of hypotension and injection pain.
Trial registration
The study was registered at Chinese Clinical Trial Registry http://www.chictr.org.cn/ (Registration date: 19/7/2021; Trial ID: ChiCTR2100048904).
Similar content being viewed by others

Background
Day surgery under general anesthesia has been associated with a shortened hospital stay and earlier mobilization [1]. All commonly-used intravenous (IV) anesthetics currently, including propofol and midazolam, have their respective advantages and disadvantages. Propofol is the most frequently used IV anesthetic for day surgery because of its excellent sedative properties and short terminal half-life. It also reduces the generation of pro-inflammatory cytokines and has been shown to exert a neuroprotective effect by maintaining Th17/Treg cell balance [2]. Despite being widely used, propofol has several disadvantages, including injection pain, cardiorespiratory depression, metabolic acidosis and hyperlipidemia [3]. Midazolam, the most commonly used benzodiazepine, causes less circulatory depression than propofol but has a comparatively longer induction and recovery time due to its longer half-life and active metabolite [4, 5]. Remimazolam besylate, an ultra-short-acting benzodiazepine agonist with propofol’s fast on- and offset characteristics [4], has been shown to be safe and effective in the induction and maintenance of general anesthesia [6, 7]. However, a previous study reported that remimazolam besylate for general anesthesia had prolonged mean time from the end of study drug to eye opening compared with propofol (14.9 ± 11.1 min vs. 10.3 ± 5.1 min) [7]. A temporary reduction in recovery quality compared with propofol was also reported in patients who underwent urologic surgery using remimazolam besylate [8].
Similar to remimazolam besylate in structure and pharmacological properties [9, 10], remimazolam tosilate (RT) is a new short-acting GABA (A) receptor agonist with a tosilate counterion. Like remimazolam besylate, RT has a short half-life which results in the quick acting onset and recovery than currently available short-acting sedatives [9]. In addition, compared with the same dose level of remimazolam besylate, a slightly different recovery time was observed in the dose range of 0.1–0.35 mg/kg of RT, which was equivalent to remimazolam besylate of 0.075-0.3 mg/kg after labeling dose conversion, with a median time to fully alert ranging from 0 to 21.5 min for RT in comparison with 5.5–31.5 min for remimazolam besylate [9]. Recent study established a non-inferior sedation success rate with RT compared with propofol for upper gastrointestinal endoscopy [11] and colonoscopy [12]. RT permits rapid recovery from procedural sedation [12] and is less likely to cause cardiovascular and respiratory depression than propofol [11, 12]. However, little is known about the utility of RT in general anesthesia. Based on the prolonged recovery from general anesthesia of remimazolam besylate and given the complete antagonistic action of flumazenil, a benzodiazepine receptor antagonist, the efficacy and safety of RT in conjunction with flumazenil was taken into account.
We designed this study to assess the efficacy and safety of RT with or without flumazenil compared with propofol in general anesthesia for day surgery with particular interest in postoperative recovery quality and inflammatory and cognitive changes.
Methods
Ethical approval
This study was a single-center randomized, single-blinded, positive-controlled, parallel trial performed in Zhongshan Hospital Fudan University in Shanghai. It was approved by the Ethics Committee of Zhongshan Hospital (Number B2021–360) and was registered with the Chinese Clinical Trial Registry prior to patient enrollment (ChiCTR2100048904; Principal investigator: CM; Date of registration: July 19, 2021). The trial was modified on September 23, 2021 to add an additional arm to test RT + flumazenil. Patients were recruited from October 2021 to December 2021. Written informed consent was obtained from all participants included in the study. This manuscript adheres to the applicable Consolidated Standards of Reporting Trials guidelines.
Participants
This trial included male and female patients aged 18 to 75 years old who had an American Society of Anesthesiologists physical status (ASA) of I or II, a body mass index of 18 to < 30 kg/m2 and underwent day surgery utilizing general anesthesia with a laryngeal mask airway (LMA). Participants were excluded if they had a history of a benzodiazepine allergy, a history of benzodiazepine or opioid use within 1 month of surgery, a history of alcohol abuse, clinically significant renal or hepatic dysfunction, significant cardiorespiratory instability (heart failure, acute lung injury, hypovolemia or sepsis), participated in different drug trials within 3 months of enrollment or were pregnant or breast-feeding.
Randomization and blinding
Participants were divided into three groups in a 1:1:1 ratio via block randomization: RT, RT + flumazenil and propofol. The randomization chart was generated using a web-based randomization system (http://www.randomization.com, USA) that employed a Wichmann and Hill number generator as modified by McLeod. Sealed and numbered envelopes were handed to an anesthesiologist who was involved in drug administration. Intraoperative data was recorded by an anesthesiology assistant. A blinded investigator who was not directly involved in intraoperative anesthesia collected all postoperative data. Both patients and surgeons were blinded to group allocation. Because propofol and RT had different colors and infusion methods, the anesthesiologists and anesthesiology assistants were unblinded to group allocation.
Interventions
General anesthesia was induced with RT (0.3 mg/kg, iv) (Jiangsu Hengrui Medicine Co, Ltd, Jiangsu, China) or propofol (2.0–2.5 mg/kg, iv) (AstraZeneca, United Kingdom) in combination with sufentanil (0.2–0.4 µg/kg, iv). If loss of consciousness (LoC) did not occur within 3 min, an IV dose of RT (0.1 mg/kg) or propofol (1.0 mg/kg) was administered. After LoC was confirmed, muscular paralysis was achieved using rocuronium (0.2–0.4 mg/kg, iv) and an LMA was inserted.
RT was maintained at 1–3 mg/kg/h and propofol was maintained within a range of 6–12 mg/kg/h. Remifentanil was administered at an infusion rate of 0.05–0.15 µg/kg/min. Bispectral index (BIS) was used to evaluate anesthesia depth. IV anesthetic infusion was discontinued when the final surgical dressing was applied. The participant who developed hypotension, defined as systolic blood pressure (SBP) < 80% of baseline, was administered a bolus dose of 6 mg ephedrine or 0.1 mg phenylephrine that was repeated as necessary. Sinus bradycardia, defined as a heart rate (HR) below 40 beats/min, was treated with 0.5 mg of atropine.
Towards the end of the surgery, nalmefene (20 µg, iv), neostigmine (0.04 mg/kg, iv) and atropine (0.02 mg/kg, iv) were allowed to be administered as necessary. In the RT + flumazenil group, 0.2 mg flumazenil (Zhejiang Aotuokang Medicine Co, Ltd, Zhejiang, China) was administered 10 min after the discontinuation of RT. If necessary, a repeated dose of 0.1 mg flumazenil was permitted every minute until the total dose reached 1 mg. Blood pressure, HR, blood oxygen saturation (SpO2) and the BIS were monitored and recorded throughout the course of anesthesia.
Outcome variables
The primary outcomes were anesthesia induction time and time until the patient was fully alert post-operatively. Induction time was defined as the time from when the participant became unresponsive to painful stimulation (namely the squeezing of his/her trapezius) after the start of anesthesia administration. Time to fully alert was defined as the time from the stopping of anesthetic dosing to the patient accurately stating his/her date of birth [13].
Key secondary endpoints included: anesthesia success rate, defined as the absence of (1) intraoperative awakening or recall, (2) the need for rescue sedative medication and (3) body movement; LMA insertion time; the BIS values; the number of patients with BIS values > 60 or < 40 during anesthesia maintenance; % time BIS > 60 during anesthesia maintenance, defined as the percentage of time with BIS values > 60 in the whole anesthesia maintenance period; the recovery time including the time to eye opening, time to LMA extraction and time to the third consecutive Aldrete score ≥ 9 in the post-anesthesia care unit (PACU); postoperative delirium. Time to the third consecutive Aldrete score ≥ 9 was defined as the period from LMA extraction to the measurement of the third consecutive Aldrete score ≥ 9. Postoperative delirium was assessed prior to PACU discharge using the Diagnostic and Statistical Manual of Mental Disorders. After stopping the anesthetic, the dosages of opioids and vasoactive drugs were also recorded. Patients were under monitoring in PACU 60 min after flumazenil administration or 60 min after entering PACU to assess the recovery profiles, especially the sedation status after flumazenil administration. Recovery profiles were assessed based on the scores of the following assessments: modified observer’s alertness/sedation scale (MOAA/S) before the surgery and 60 min after flumazenil administration or 60 min after entering PACU; Aldrete score 60 min after entering PACU; mini-mental state examination (MMSE) before the surgery, in PACU and on 1 day after surgery (POD1); visual analogue scale (VAS) before the surgery, in PACU and on POD1; the post-operative quality of recovery scale (PostopQRS) before the surgery, on POD1 and 14 days after surgery (POD14); a telephone interview to evaluate cognitive status on POD14. Residual cognitive effects (more than 7 days) following ambulatory anesthesia in middle-aged patients have been previously reported [14]. The postoperative follow-up time point was therefore extended to POD14 to permit a comprehensive evaluation of cognitive recovery and complications [15, 16]. Vital signs including SpO2, HR, SBP and diastolic blood pressure (DBP) were recorded at twelve time points: before induction (T1), after induction (T2), after LMA insertion (T3), 5 min after the beginning of surgery (T4), 10 min after the beginning of surgery (T5), 10 min before stopping the study drug (T6), 5 min before stopping the study drug (T7), immediately after stopping the study drug (T8), 10 min after stopping the study drug (T9), 15 min after stopping the study drug (T10), LMA extraction (T11) and before leaving the operating room (T12).
Blood samples were drawn before anesthesia induction and at PACU discharge to measure inflammatory factors and biomarkers relevant to cognitive and lipid profiles, such as neuropeptide Y (NPY), interleukin (IL)-8, IL-1β, IL-10, triglyceride (TG) and very low density lipoprotein (VLDL) levels. The above factors were measured using enzyme-linked immunosorbent assay kits obtained from XLPCC (Shanghai, China) according to the manufacturer’s instructions. In order to explore whether RT had the similar effect to propofol in terms of inflammatory factors activation and Th17/Treg cell balance [2], neutrophil (CD11b/CD18) and Treg cell (CD39/CD73) surface markers were also measured in peripheral blood samples according to the manufacturer’s instructions (BD, San Diego, CA, USA) and then detected using flow cytometry.
Drug-related adverse events (AEs) including hypotension, sinus bradycardia and hypoxia (defined as SpO2 < 90%) were monitored throughout this study. Any AEs related to flumazenil were also recorded. In addition, the incidence of injection pain, intraoperative awareness, body movement, airway intervention after LMA extraction, postoperative nausea and vomiting and complications up to POD14 were calculated.
Statistical analysis
The sample size required for this study was based on pre-trial estimates of induction time and the time until fully alert. The mean induction times of the RT, RT + flumazenil and propofol groups were 55s, 58s and 51s, respectively, and the standard deviations (SD) for each group were 5s, 3s and 2s, respectively. Assuming an α = 0.05 and a power of 80% (two-sided tests), we calculated that a sample of 33 participants for each arm were required using the PASS 15 software (NCSS Corp., USA). The same method was used to estimate that at least 15 participants per arm were required to evaluate time until fully alert. Allowing for dropouts and non-evaluable data, a minimum of 38 participants were recruited for each group.
Analysis was performed according to the modified intention-to-treat principle. Data were presented using mean ± SD or median (25th, 75th percentiles) for continuous variables, and frequency counts and percentages for nominal variables. The Shapiro–Wilk test was used to determine whether continuous outcomes were normally distributed. Normally distributed data were tested using a one-way analysis of variance (ANOVA), with pairwise comparisons made with the least square mean values t test. Nonparametric data were tested with the Kruskal–Wallis test, with pairwise comparisons made with the Wilcoxon-rank sum test. Categorical outcomes were compared with the χ2 analysis or Fisher’s exact test in the setting of low expected cell counts. Endpoints assessed at different times were analyzed using the mixed-model repeated measures analysis. All outcomes were considered exploratory in nature and thus no correction for multiple comparisons was made. All statistical tests were two-tailed, and significance was defined using a P value < 0.05. All statistical analyses were performed using SPSS19.0 software (IBM, Armonk, NY, USA) and R software version 4.1.0 (The R Foundation, Vienna, Austria).
Results
Patient demographic and clinical characteristics
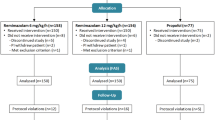
A total of 130 participants were screened for eligibility. Fifteen were excluded, leaving 115 patients to be randomized into three groups: 39 to the RT group, 38 to the RT + flumazenil group and 38 to the propofol group (Fig. 1). One patient in the RT group did not receive the intervention or follow-up due to failed LMA insertion. Patient and surgery characteristics are shown in Table 1. There were no relevant imbalances between the groups at baseline including surgery type and preoperative laboratory tests such as inflammatory biomarkers neutrophil/lymphocyte ratio and platelet/lymphocyte ratio (P > 0.05; Table 1).

Participant flow of the study. LMA, laryngeal mask airway
Primary outcomes
There was no significant difference in anesthesia induction time among the three groups (P = 0.437; Table 2). However, a significant increase in the time to fully alert was detected in the RT group compared with the propofol (P < 0.001) and RT + flumazenil groups (P < 0.001; Table 2). Time to fully alert was comparable between the propofol and RT + flumazenil groups (P = 0.949; Table 2).
Secondary outcomes
Sedation success rates were equivalent among the three groups, with 97.4% each (P = 1.000; Table 2). Time for LMA insertion was also similar among the three groups (P > 0.05 for all comparisons; Table 2). During induction, patients who received RT with or without flumazenil reached LoC with BIS values higher than propofol (RT vs. propofol, P = 0.002; RT + flumazenil vs. propofol, P = 0.002; Table 2; Fig. 2A). The same trend existed at T3-T8 time points (P < 0.001; Fig. 2A). However, BIS values were lower in the RT group compared to the propofol group at T11-T12 time points (P = 0.002, 0.005 respectively; Table 2; Fig. 2A). The number of patients with BIS values > 60 during anesthesia maintenance and % time BIS > 60 during anesthesia maintenance were significantly increased in the RT and RT + flumazenil groups compared with propofol group (P < 0.001 for all comparisons; Table 2). Conversely, fewer patients in the RT (P = 0.018) and RT + flumazenil groups (P = 0.006) had BIS values < 40 compared with the propofol group, indicating deeper sedation with propofol (Table 2). However, no patients in this study reported intraoperative awareness.

Vital signs and bispectral index during the entire procedure. Evaluation of the levels of (A) bispectral index, (B) SBP, (C) DBP, (D) HR and (E) SpO2 before induction (T1), after induction (T2), after laryngeal mask airway insertion (T3), 5 min after the beginning of surgery (T4), 10 min after the beginning of surgery (T5), 10 min before stopping the study drug (T6), 5 min before stopping the study drug (T7), immediately after stopping the study drug (T8), 10 min after stopping the study drug (T9), 15 min after stopping the study drug (T10), after laryngeal mask airway extraction (T11) and before leaving the operating room (T12). Data are shown as mean ± SE or median. SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; SpO2, blood oxygen saturation; RT, remimazolam tosilate; LoC, loss of consciousness. *P < 0.05, **P < 0.01, ***P < 0.001, RT + flumazenil versus propofol group; #P < 0.05, ##P < 0.01, ###P < 0.001, RT versus propofol group
During the recovery phase, all of the patients in the RT + flumazenil group received flumazenil. The average dose of flumazenil was 0.27 mg and the maximum dose was 0.70 mg. No re-sedation occurred 60 min after flumazenil administration according to the MOAA/S scores (5.00 ± 0.00 for all three groups) and Aldrete scores (10.00 ± 0.00 for all three groups) in PACU. Time to eye opening, LMA extraction and the third consecutive Aldrete score ≥ 9 were statistically shorter in the propofol group and RT + flumazenil group compared with the RT group (P ≤ 0.001 for all comparisons; Table 2).
SpO2, HR, SBP and DBP were shown in Fig. 2. There were no significant differences in SpO2 among the three groups at T1–T12 (P > 0.05; Fig. 2E); further, baseline SBP, DBP and HR data were also comparable (P > 0.05; Fig. 2B-D). However, SBP was significantly higher at T3, T6-T8 and T12 (P < 0.05; Fig. 2B), DBP was significantly higher at T2, T3, T6, T8, T11 and T12 (P < 0.05; Fig. 2C), and HR was significantly higher at T3, T4, T7, T11 and T12 (P < 0.05; Fig. 2D) in the RT + flumazenil group compared with the propofol group. SBP, DBP and HR were all significantly higher in the RT group than those in the propofol group at T3 (P < 0.05; Fig. 2B-D). Fewer patients who received RT with or without flumazenil (31.6% and 31.6%) required vasopressors compared with propofol (71.1%, P < 0.001). Ephedrine (P < 0.001) dosage was significantly decreased in both RT groups compared with the propofol group, and phenylephrine (P = 0.015) dosage was significantly lower in the RT group than that in the propofol group (Table 2).
There was no postoperative delirium in any of the three groups prior to PACU discharge and on POD 1 and 14. There were no significant between-group differences in MMSE (PACU, P = 0.724; POD1, P = 0.117) or in PostopQRS scores (POD1, P = 0.072; POD14, P = 0.264) compared with baseline measurements (Table 3). Similarly, no differences were observed among the three groups in the telephone interview for cognitive status on POD14 (P = 0.500; Table 3). The VAS scores were comparable among the three groups with similar dosages of sufentanil (P > 0.05 for all comparisons; Table 2) both in PACU and on POD1 (PACU, P = 0.853; POD1, P = 0.356; Table 3). The serum levels of IL-8, IL-1β and IL-10 were similar before and after anesthesia among the three groups (P > 0.05 for all comparisons; Supplementary Fig. 1A–C). There were no significant differences in the expression of CD39(+), CD73(+), CD39(+)CD73(+), CD11b(+), CD18(+) and CD11b(+)CD18(+) among the three groups before and after anesthesia (P > 0.05 for all comparisons; Supplementary Table 1).
With respect to lipid metabolism, extensive changes in TG were observed in the propofol group in the PACU. The strongest increase of TG after anesthesia was observed in the propofol group compared with the RT with or without flumazenil groups (1.88 ± 1.28 mmol/L, 1.33 ± 0.70 mmol/L, 1.43 ± 0.75 mmol/L, respectively; P < 0.001; Supplementary Fig. 1E). The baseline VLDL measurement in propofol group was significantly lower than that of both RT groups (P < 0.001; Supplementary Fig. 1F). However, following covariance analysis PACU VLDL levels were comparable among the three groups (P = 0.728; Supplementary Fig. 1F). Changes in NPY, which was found to have hypnotic properties and be increased during the sleep inhibition phase [17], were not significant among the three groups (P > 0.05 for all comparisons; Supplementary Fig. 1D).
Adverse events
No patients had a serious AE. The distributions of AEs pertaining to hemodynamics and other complications are shown in Table 4. One patient (2.6%) in the propofol group developed hypoxemia and required an airway intervention in the recovery phase. Postoperative nausea and vomiting occurred in two patients (5.3%) treated with propofol. Smaller percentages of patients who received RT (26.3%) and RT + flumazenil (31.6%) became hypotensive during anesthesia maintenance compared with those who received propofol (68.4%). The incidence of injection pain was 18.4% in the propofol group, 0% in RT group and 5.3% in RT + flumazenil group. No AEs related to flumazenil were observed. No intraoperative arousal or recall was reported in any group. No complications were reported during the POD14 telephone interview in any group.
Discussion
The present study was the first to evaluate RT in general anesthesia for day surgery. RT induction was as rapid as propofol’s. A fast and complete recovery from general anesthesia could be achieved with the use of flumazenil. Although higher BIS values were observed in patients treated with RT, no intraoperative awareness was reported. Vasopressor dosage, injection pain and serum TG levels were decreased in patients who received RT with or without flumazenil compared with propofol.
Because minimally invasive surgery is now well established, more procedures can be performed as day surgeries [1]. Advantages of IV anesthesia with a LMA, which is commonly used for the induction and maintenance of general anesthesia during day surgery, include steady induction, fast recovery and relatively simple administration [18]. To achieve enhanced recovery after a day surgery, short-acting anesthetics are required. RT has been approved for clinical use in China by the National Medical Products Administration as a novel ultrashort-acting benzodiazepine for general anesthesia and sedation since 2021. In this study, RT (0.3 mg/kg, iv) led to rapid LoC during induction in a similar manner to propofol. However, a prior work reported increased induction times with RT compared with propofol when administered as a constant infusion for procedural sedation during intestinal endoscopy [11, 12]. Similar findings were reported when remimazolam besylate was used [7], suggesting that a single IV dose of remimazolam besylate or RT permits faster anesthesia induction than a constant infusion.
The dosing we chose for RT in this study was based on the results of Phase II and III clinical trials of RT [11] and the report on remimazolam besylate for general anesthesia [7]. BIS was used in this study to monitor anesthesia depth. We found that patients who received RT had higher BIS values than those receiving propofol from the time point of reaching LoC to the discontinuation of the study drug, and more patients treated with RT had BIS values > 60 during maintenance compared with propofol, while fewer had BIS values < 40, which is consistent with the findings of previous studies [7, 19] that evaluated remimazolam besylate. However, after LMA extraction and operating room discharge, BIS values were found to be lower only in the RT group but not the RT + flumazenil group compared with the propofol group in this study, indicating that RT achieved a similar recovery from sedation as propofol only when patients were treated with flumazenil. One previous study showed that BIS values during anesthesia with remimazolam were significantly higher than those with propofol despite comparable anesthetic effects [7]. The higher BIS value is partly due to an increment of β waves during administration of benzodiazepine [20]. The validity of the BIS value in anesthesia with benzodiazepine has been controversial [21, 22]. As a result, BIS might not properly reflect the depth of anesthesia with RT compared with propofol. Other efforts have been made in monitoring the depth of remimazolam anesthesia, like Sedline [23], however, it is still not ideal and further studies are needed.
RT was found to achieve a similar recovery time from general anesthesia compared with propofol only when patients were treated with flumazenil 10 min after RT discontinuation in this study. It’s worth noting that BIS values were different between the RT combined with flumazenil group and propofol group, which may affect the result of recovery time. However, RT was reported to have a faster recovery from procedural sedation after upper gastrointestinal endoscopy compared with propofol when administered via intermittent IV injection [11]. The use of RT through continuous infusion in this study may account for the prolonged recovery time. A prior study suggested that when using a controlled infusion of remimazolam or propofol to maintain general anesthesia, the context-sensitive half-time (CSHT) of remimazolam had little relationship with the infusion time, while the CSHT of propofol increased with a prolonged infusion time [24]. Therefore, for patients undergoing day surgeries, which generally have shorter procedural times, propofol may allow for a faster recovery from general anesthesia compared with RT. In the present study, SBP, DBP and HR were higher in the RT or RT + flumazenil group compared to the propofol group at several time points from induction to operating room discharge, while lower dosing of vasopressors and fewer cases of treatment-related hypotension were observed in the patients treated with RT. This may be partly attributed to a lower rate of cardiovascular depression of RT compared with propofol, which are also consistent with previous reports [11, 12]. More patients in the propofol group were under deep anesthesia with BIS values < 40 which also needs to be taken into consideration [25]. Lighter anesthesia may be induced by RT.
A recent study reported lower physical comfort and emotional state recovery quality among patients who received remimazolam besylate keeping BIS ranges between 40 and 60 compared with propofol for urologic surgery on POD1 [8]. The cognitive evaluation performed in this study showed that RT and propofol had similar cognitive recovery during early recovery period, as shown by the MMSE score and telephone interview. Similar results of short-term recovery quality were also observed using PostopQRS in the present work. It suggested that RT and propofol may permit similar recovery quality. However, considering the higher BIS values in the patients receiving RT in our study, remimazolam besylate may have a similar recovery profile to RT under the same depth of anesthesia, which needs further study. It’s also worth pointing out that this real world study included patients aged 18–75 years old and the number of patients aged > 65 years old in each group was balanced. Similar inclusion criteria have been adopted by other studies [26, 27]. Adults aged > 65 years old are the fastest growing segment of the population around the world [28]. As the population ages, the demand for surgery is projected to increase by 18% [29]. Given the improving health status and functional independence in older individuals, it has been considered to change cut-off age from 65 to 75 years old to define “elderly” [30]. Of course, the use of RT in older patients needs further study.
Adverse events linked to flumazenil include pain on injection, agitation and tremors, flushing, dizziness, sweating or shivering, headache, blurred vision and ringing in the ears [31]. The safety of the use of flumazenil was also considered in this study. No AEs related to flumazenil were observed in patients treated with RT in conjunction with flumazenil prior to PACU discharge. Two patients in the RT + flumazenil group experienced injection pain during anesthesia induction, not anesthesia recovery. The injection pain therefore did not occur because of the flumazenil. A prior study suggested that 1.0 to 10.0 mg of flumazenil can increase the risk of AEs in patients who visited the emergency department with impaired consciousness due to benzodiazepine overdose [32]. However, the average dose of flumazenil used in this study was 0.27 mg and the maximum dose was 0.70 mg. The use of flumazenil to reverse benzodiazepine sedation was also found to be safe when used after endoscopy [33] or pediatric anesthesia [34]. Therefore, small doses of flumazenil can be used to reverse the sedative and hypnotic effects of RT and enhance recovery from anesthesia. However, the routine use of flumazenil after RT requires further study.
Prior reports suggested that propofol reduces the generation of pro-inflammatory cytokines and exerts a neuroprotective effect by maintaining Th17/Treg cell balance [2]. Upregulation of CD11 and CD18 on the surface of neutrophils is an important marker of the inflammatory response [35]. Hence, inflammatory factors and the expression of CD11b/CD18 for neutrophils and CD39/CD73 for Tregs [36] were measured in this study. No significant differences were detected in either set of surface markers between the three groups, suggesting that RT may have a similar effect on the patient’s inflammatory profile compared with propofol. A prior work suggested that propofol induces marked changes in lipid profile and a modest increase in total TG [37]. In the present study, increased TG expression after anesthesia was observed in the propofol group but not the RT groups.
This study has several limitations. First, because the present study is limited to patients who underwent day surgery with an LMA, the efficacy and safety of RT during procedures that require intubation may be different. Second, NPY was detected before PACU discharge in this study when patients might fully recover from sleep inhibition. Changes in NPY are suggested to be detected before, during and after the procedures in the future study. Third, propofol and RT may reach different levels of anesthesia depth according to the BIS values. The depth of anesthesia may affect the hemodynamic stability and the recovery time. However, BIS monitoring may not properly reflect the depth of anesthesia with remimazolam. Appropriate ranges of BIS and alternative methods to monitor the depth of RT anesthesia need more researches. Fourth, due to limited experience with the drug, the optimal induction dose and the recovery profile of RT still need to be explored. Anesthesiologists need more experience with RT to its full advantage and initiate tapering off early enough to allow for the fastest recovery. Lastly, patients over 75 years old and above ASA II were not included in this study. Hence, the efficacy and safety of RT and flumazenil in older patients and those with comorbidities requires further study. Larger trials with a more vulnerable patient population are needed before RT can be recommended for general use.
Conclusions
This study demonstrated that RT permits rapid induction and equivalent postoperative recovery quality compared with propofol in general anesthesia for day surgery. However, there was a prolonged recovery time of RT, but not RT in conjunction with flumazenil compared with propofol. RT had a superior safety profile to propofol in terms of hypotension and injection pain. Less changes in lipid metabolism were also observed in the patients receiving RT.
Data availability
Individual participant data that underlies the results of this article can be accessed with approval from the corresponding author on reasonable request. The study protocol and statistical analysis plan is also available.
Abbreviations
- IV:
-
intravenous
- RT:
-
remimazolam tosilate
- ASA:
-
anesthesiologists physical status
- LMA:
-
laryngeal mask airway
- LoC:
-
loss of consciousness
- BIS:
-
bispectral index
- SBP:
-
systolic blood pressure
- HR:
-
heart rate
- SpO2:
-
blood oxygen saturation
- PACU:
-
post-anesthesia care unit
- MOAA/S:
-
modified observer’s alertness/sedation scale
- MMSE:
-
mini-mental state examination
- PostopQRS:
-
post-operative quality of recovery scale
- VAS:
-
visual analogue scale
- POD1 and POD14:
-
1 and 14 days after surgery
- DBP:
-
diastolic blood pressure
- NPY:
-
neuropeptide Y
- IL:
-
interleukin
- TG:
-
triglyceride
- VLDL:
-
very low density lipoprotein
- AEs:
-
adverse events
- SD:
-
standard deviation
- CSHT:
-
context-sensitive half-time
References
Bailey CR, Ahuja M, Bartholomew K, Bew S, Forbes L, Lipp A, et al. Guidelines for day-case surgery 2019: guidelines from the Association of Anaesthetists and the British Association of Day surgery. Anaesthesia. 2019;74(6):778–92.
Cui C, Zhang D, Sun K, Li H, Xu L, Lin G, et al. Propofol maintains Th17/Treg cell balance and reduces inflammation in rats with traumatic brain injury via the miR-145-3p/NFATc2/NFκB axis. Int J Mol Med. 2021;48(1):135.
Lundström S, Twycross R, Mihalyo M, Wilcock A, Propofol. J Pain Symptom Manage. 2010;40(3):466–70.
Borkett KM, Riff DS, Schwartz HI, Winkle PJ, Pambianco DJ, Lees JP, et al. A phase IIa, randomized, double-blind study of remimazolam (CNS 7056) versus midazolam for sedation in upper gastrointestinal endoscopy. Anesth Analg. 2015;120(4):771–80.
Nordt SP, Clark RF. Midazolam: a review of therapeutic uses and toxicity. J Emerg Med. 1997;15(3):357–65.
Doi M, Hirata N, Suzuki T, Morisaki H, Morimatsu H, Sakamoto A. Safety and efficacy of remimazolam in induction and maintenance of general anesthesia in high-risk surgical patients (ASA Class III): results of a multicenter, randomized, double-blind, parallel-group comparative trial. J Anesth. 2020;34(4):491–501.
Doi M, Morita K, Takeda J, Sakamoto A, Yamakage M, Suzuki T. Efficacy and safety of remimazolam versus propofol for general anesthesia: a multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J Anesth. 2020;34(4):543–53.
Mao Y, Guo J, Yuan J, Zhao E, Yang J. Quality of Recovery after General Anesthesia with Remimazolam in patients’ undergoing urologic surgery: a randomized controlled trial comparing remimazolam with Propofol. Drug Des Devel Ther. 2022;16:1199–209. Published 2022 Apr 27.
Zhou Y, Hu P, Huang Y, Nuoer S, Song K, Wang H et al. “Population Pharmacokinetic/Pharmacodynamic Model-Guided Dosing Optimization of a Novel Sedative HR7056 in Chinese Healthy Subjects.” Frontiers in pharmacology vol. 9 1316. 19 Nov. 2018.
Wiltshire HR, Kilpatrick GJ, Tilbrook GS, Borkett KM. A placebo- and midazolam-controlled phase I single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): part II. Population pharmacokinetic and pharmacodynamic modeling and simulation. Anesth Analg. 2012;115:284–96.
Chen SH, Yuan TM, Zhang J, Bai H, Tian M, Pan CX, et al. Remimazolam tosilate in upper gastrointestinal endoscopy: a multicenter, randomized, non-inferiority, phase III trial. J Gastroenterol Hepatol. 2021;36(2):474–81.
Chen S, Wang J, Xu X, Huang Y, Xue S, Wu A, et al. The efficacy and safety of remimazolam tosylate versus propofol in patients undergoing colonoscopy: a multicentered, randomized, positive-controlled, phase III clinical trial. Am J Transl Res. 2020;12(8):4594–603. Published 2020 Aug 15.
Bahar M, Dundee JW, O’Neill MP, Briggs LP, Moore J, Merrett JD. Recovery from intravenous anaesthesia. Comparison of disoprofol with thiopentone and methohexitone. Anaesthesia. 1982;37(12):1171–5.
Lindqvist M, Schening A, Granstrom A, Bjorne H, Jakobsson JG. Cognitive recovery after ambulatory anaesthesia based on desflurane or propofol: a prospective randomised study. Acta Anaesthesiol Scand. 2014;58(9):1111–20.
Kontos AP, Covassin T, Elbin RJ, Parker T. Depression and neurocognitive performance after concussion among male and female high school and collegiate athletes. Arch Phys Med Rehabil. 2012;93(10):1751–6.
Dahlberg K, Jaensson M, Nilsson U. Let the patient decide” - person-centered postoperative follow-up contacts, initiated via a phone app after day surgery: secondary analysis of a randomized controlled trial. Int J Surg. 2019;61:33–7.
Dyzma M, Boudjeltia KZ, Faraut B, Kerkhofs M. Neuropeptide Y and sleep. Sleep Med Rev. 2010;14(3):161–5.
Reves JG, Glass P, lubarsky D, Matthe WD, Evoy MC, Martinez R, et al. Intravenous anesthetics. In: Miller RD, editor. Miller’s anesthesia. 7th ed. San Francisco: Elsevier; 2010. pp. 719–68.
Shi F, Chen Y, Li H, Zhang Y, Zhao T. Efficacy and safety of Remimazolam Tosilate versus Propofol for General Anesthesia in Cirrhotic Patients undergoing endoscopic Variceal Ligation. Int J Gen Med. 2022;15:583–91. Published 2022 Jan 13.
Upton RN, Martinez AM, Grant C. Comparison of the sedative properties of CNS 7056, midazolam, and propofol in sheep. Br J Anaesth. 2009;103(6):848–57.
Miyake W, Oda Y, Ikeda Y, Hagihira S, Iwaki H, Asada A. Electroencephalographic response following midazolam-induced general anesthesia: relationship to plasma and effect-site midazolam concentrations. J Anesth. 2010;24(3):386–93.
Glass PS, Bloom M, Kearse L, Rosow C, Sebel P, Manberg P. Bispectral analysis measures sedation and memory effects of propofol, midazolam, isoflurane, and alfentanil in healthy volunteers. Anesthesiology. 1997;86(4):836–47.
Shirozu K, Nobukuni K, Tsumura S, Imura K, Nakashima K, Takamori S, et al. Neurological sedative indicators during general anesthesia with remimazolam. J Anesth. 2022;36(2):194–200.
Guan Ren D, Xiwei M, Ning Z. Pharmacologic overview of the innovative soft drug remimazolam based on computer simulation. Int J Anesth Resus. 2020;41(10):946–54.
Short TG, Campbell D, Frampton C, et al. Anaesthetic depth and complications after major surgery: an international, randomised controlled trial. Lancet. 2019;394(10212):1907–14.
Pastis NJ, Yarmus LB, Schippers F, Ostroff R, Chen A, Akulian J, et al. Safety and Efficacy of Remimazolam compared with placebo and midazolam for moderate Sedation during Bronchoscopy. Chest. 2019;155(1):137–46.
Tang Y, Yang X, Yu Y, Shu H, Yuan Y, Liu H, et al. Remimazolam besylate versus propofol for long-term sedation during invasive mechanical ventilation: a pilot study. Crit Care. 2022;26(1):279. Published 2022 Sep 16.
Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 2020;139:6–11.
Dall TM, Gallo PD, Chakrabarti R, West T, Semilla AP, Storm MV. An aging population and growing disease burden will require a large and specialized health care workforce by 2025. Health Aff (Millwood). 2013;32(11):2013–20.
Orimo H, Ito H, Suzuki T, Araki A, Hosoi T, Sawabe M. Reviewing the definition of “elderly. Geriatr Gerontol Int. 2006;6(3):149–58.
Ngo AS, Anthony CR, Samuel M, Wong E, Ponampalam R. Should a benzodiazepine antagonist be used in unconscious patients presenting to the emergency department? Resuscitation. 2007;74(1):27–37.
Penninga EI, Graudal N, Ladekarl MB, Jürgens G. Adverse events Associated with Flumazenil Treatment for the management of suspected Benzodiazepine Intoxication–A systematic review with Meta-analyses of Randomised trials. Basic Clin Pharmacol Toxicol. 2016;118(1):37–44.
Lee SP, Sung IK, Kim JH, Lee SY, Park HS, Shim CS. Efficacy and safety of flumazenil injection for the reversal of midazolam sedation after elective outpatient endoscopy. J Dig Dis. 2018;19(2):93–101.
Jones RD, Lawson AD, Andrew LJ, Gunawardene WM, Bacon-Shone J. Antagonism of the hypnotic effect of midazolam in children: a randomized, double-blind study of placebo and flumazenil administered after midazolam-induced anaesthesia. Br J Anaesth. 1991;66(6):660–6.
Rosetti F, Mayadas TN. The many faces of Mac-1 in autoimmune disease. Immunol Rev. 2016;269(1):175–93.
Schuler PJ, Harasymczuk M, Schilling B, Lang S, Whiteside TL. Separation of human CD4 + CD39 + T cells by magnetic beads reveals two phenotypically and functionally different subsets. J Immunol Methods. 2011;369(1–2):59–68.
Nummela AJ, Laaksonen LT, Laitio TT, Kallionpää RE, Långsjö JW, Scheinin JM, et al. Effects of dexmedetomidine, propofol, sevoflurane and S-ketamine on the human metabolome: a randomised trial using nuclear magnetic resonance spectroscopy. Eur J Anaesthesiol. 2022 Jun;1:39:521–32.
Acknowledgements
We gratefully acknowledge Fei Liang (Department of biostatistics, Zhongshan Hospital Fudan University, Shanghai, China) for helping us with the statistics for this study.
Funding
This work was sponsored by the National Natural Science Foundation of China (Numbers 81971868 and 82172187 to J Zhong, 82072213 and 81873948 to CH Miao, Shanghai, China), Program of Shanghai Academic/Technology Research Leader (20XD1423000 to J Zhong, Shanghai, China), Clinical Research Project of Zhongshan Hospital (Number 2020ZSLC41 to J Zhong, Shanghai, China), Excellent Backbone Plan Of Zhongshan Hospital (Number 2021ZSGG16 to J Zhong, Shanghai, China), Smart Health-care Project of Zhongshan Hospital (Number 2020ZHZS25 to CH Miao, Shanghai, China), the Youth Fund of Zhongshan Hospital (Number 2021-011 to MY Liu, Shanghai, China), Fujian National Science Foundation (Number 2022J05331 to Wanxia Xiong, Fujian, China) and Post-graduate Medical Education Project of Shanghai Medical College Fudan University (Number FDYXYBJ-20221003 to CH Miao, Shanghai, China).
Author information
Authors and Affiliations
Contributions
Jing Zhong, Changhong Miao, Mingyue Liu and Wenchen Luo supervised the study and revised the manuscript. Jing Zhong, Mingyue Liu and Minli Sun conceived and designed the study. Jing Zhong, Wenchen Luo and Mingyue Liu interpreted the data. Wenchen Luo and Mingyue Liu drafted the manuscript. Minli Sun, Mingyue Liu, Jie Wan recruited patients and performed the study. Jie Wan, Zhenyu Zhang, Jian Huang, Jinlin Zhang, Wanxia Xiong, Lirong Xia and Peiyao Xu acquired the data. Xuesong Zhang revised the manuscript, checked the data and reanalyzed part of the outcomes. All authors made substantial contributions to study conception and design, data acquisition, data analysis and interpretation and drafting, revising or critically reviewing the article.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Zhongshan Hospital (Number B2021–360) and was registered with the Chinese Clinical Trial Registry prior to patient enrollment (ChiCTR2100048904; Principal investigator: CM; Date of registration: July 19, 2021). The trial was modified on September 23, 2021 to add an additional arm to test RT + flumazenil. Patients were recruited from October 2021 to December 2021 at Zhongshan Hospital Fudan University, Shanghai, China. Written informed consent was obtained from all participants included in the study. This manuscript adheres to the applicable Consolidated Standards of Reporting Trials guidelines. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of interest related to this work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Luo, W., Sun, M., Wan, J. et al. Efficacy and safety of remimazolam tosilate versus propofol in patients undergoing day surgery: a prospective randomized controlled trial. BMC Anesthesiol 23, 182 (2023). https://doi.org/10.1186/s12871-023-02092-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-023-02092-2