
Abstract
Obesity in adolescents has reached epidemic proportions and is associated with the inflammatory response and viral infections. The aim of this study was to understand the profile of inflammatory cytokines and chemokines associated with the inflammatory response and metabolic syndrome (MetS) in obese adolescents with positive serology for adenovirus 36 (ADV36). Thirty-six overweight, 36 obese, and 25 severe obesity adolescents aged 10 to 16 years were included in the study. The following variables were analyzed: sex, age, body mass index (BMI), blood pressure, total cholesterol and fractions, triglycerides, glucose, serum cytokine concentrations, and ADV36 antibodies. Cytokines and chemokines were quantified by cytometry and ADV36 serology was determined by enzyme-linked immunosorbent assay (ELISA). The results showed higher levels of the cytokines interleukin-1beta (IL-1β), IL-6, IL-10 and of the chemokine interferon-gamma-inducible protein 10 (IP-10) in severe obesity adolescents compared to the obese and overweight groups, as well as in the group with MetS compared to the group without this syndrome. The frequency of ADV36-positive individuals did not differ between groups. The findings revealed differences in BMI between the obese and severe obesity groups versus the overweight group in the presence of positivity for ADV36, suggesting an association with weight gain and possibly MetS installation.
Similar content being viewed by others

Introduction
Obesity in children and adolescents has acquired alarming and epidemic proportions in recent decades on several continents1,2,3 and is considered a serious public and social health problem. Since 2015, obesity has been recognized as a “disease” and no longer as a complicating factor associated with another disease4. This fact has led to an increase in the incidence and prevalence of comorbidities and diseases in children, adolescents, and adults3, 5,6,7.
The high prevalence of obesity in adolescents is associated with an increased risk of bone alterations/wear-and-tear, cancer, type 2 diabetes mellitus, arterial hypertension, heart disease, stroke, increased risk of early mortality, and metabolic syndrome (MetS)7,8,9,10,11,12. Identifying MetS in obese adolescents is important to suggest early interventions in diet, lifestyle and therapy when necessary13, with the prevention of the consequences of excessive weight gain that seems to occur at increasingly earlier ages5. Metabolic syndrome consists of a set of metabolic alterations and is recognized as a risk factor for the development of cardiovascular diseases and type 2 diabetes mellitus14. The determinant factors of this syndrome are obesity, hypertension, dyslipidemia, and hyperglycemia15.
The origin of the complications associated with obesity lies in the systemic and chronic inflammation of adipose tissue16,17,18. The production of inflammatory cytokines is generally associated with a certain subpopulation of macrophages, called classically activated or M1 macrophages, which participate in the pathophysiology of obesity19. Macrophages are the main cells that produce the inflammatory cytokines IL-1β, IL-6, IL-8, IL-10, IL-12, and tumor necrosis factor-alpha (TNF-α), as well as chemokines that also seem to be produced by adipose tissue in obesity20, 21. The chemokines produced by macrophages/monocytes and linked to obesity are IP-10 or chemokine (C-X-C motif) ligand 10 (CXCL10), which is associated with decreased angiogenesis in adipose tissue and inflammation due to the lack of vascularization and is expressed in morbidly obese patients22, and regulated on activation, normal T cell expressed and secreted (RANTES) or chemokine (C–C motif) ligand 5 (CCL5), which contributes to resistance to insulin23, 24. Other chemokines that are being investigated in obese individuals and that have been associated with inflammation in adipose tissue are monocyte chemoattractant protein-1 (MCP-1) or CCL2 and monokine induced by interferon-gamma (MIG) or CXCL920, 25.
It is also believed that obesity has an infectious component, i.e., some viral infections may play a role in weight gain and obesity. Within this context, several studies have linked obesity to infection with adenovirus 36 (ADV36), a virus already described in adults, adolescents, and children26, 27. This adenovirus interferes with insulin resistance and cytokine production in obese individuals. Some studies reported the presence of ADV36 in adipose tissue removed from obese patients, reinforcing the association of this adenovirus infection with obesity28.
Within this context, the aim of the present study was to identify and quantify serum concentrations of inflammatory cytokines and chemokines associated with the inflammatory profile of M1 macrophages, as well as to evaluate associations with the grade of obesity, positive ADV serology, and presence of MetS in adolescents.
Results
Anthropometric data and biochemical assessment for the characterization of MetS
Ninety-seven patients were included. These patients were divided into three groups according to BMI (Table 1). Some data on sexual maturation were not obtained due to the patient’s refusal during the evaluation. All patients were submitted to biochemical assessment for the identification of MetS and characterization of the groups (Table 1).
Inflammatory cytokines IL-1β, IL-6 and IL-10 associated with MetS
Cytokines were measured in all groups. Differences between the overweight, obese and severe obesity groups were observed for IL-1β, IL-6, and IL-10 (Table 2). The levels of these cytokines differed between the groups without and with MetS (Table 3). The areas under the receiver operating characteristics (ROC) curve were also higher for these cytokines, with values ranging from 0.88 to 1.0 (Fig. 1).

ROC curve of cytokines. Analysis of IL-1β, IL-6, IL-8, IL-10, IL-12p40, and TNF-α in serum of adolescents with excess weight. AUC = area under the curve indicating the accuracy of each cytokine as a diagnostic marker of MetS in overweight and obese adolescents.
Chemokine IP-10 associated with MetS
Chemokines were measured in all groups. There were differences in IP-10 levels between the severe obesity groups and the other groups, while the overweight group did not differ from the obese group for any of the chemokines evaluated (Table 4). A difference in IP-10 was observed between the groups without and with MetS (Table 3). The ROC curve for IP-10 showed an accuracy of 0.76, with a cut-off value of 150.36 pg/mL (Fig. 2). There was no significant difference in the other chemokines between groups.

ROC curve of chemokine IP-10. Analysis of IP-10 in serum of adolescents with excess weight. AUC = area under the curve indicating the accuracy of the chemokine as a diagnostic marker of MetS in overweight and obese adolescents. Cut-off = 150.36 pg/mL; specificity = 0.28; sensitivity = 0.70.
Anti-ADV36 antibody in the overweigh, obese and severe obesity groups
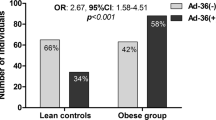
There was no difference in positivity for ADV36 between the degrees of obesity, presence of MetS and association with levels of cytokines IL-1β, IL-6 and IL-10 (Table 5). The evaluation of BMI in the ADV36 positive group separated BMI into only two groups, that is, BMI of obese individuals was equal to BMI of severe obesity individuals and both were higher than the group of overweight adolescents (Table 6). This difference in BMI in two groups did not occur when adolescents who were negative for ADV36 were evaluated; this comparison showed overweight BMI < obese BMI < severe obesity BMI (Table 6).
Discussion
The results revealed differences in inflammatory and anti-inflammatory cytokines between the groups studied, as demonstrated by the difference in the levels of IL-1β, IL-6 and IL-10, cytokines produced by M1 and M2 macrophages. The group of adolescents with excess weight had higher levels than those with lower weight and BMI, suggesting the potential use of these cytokines as diagnostic markers of comorbidities and MetS in obese adolescents. Associations of inflammatory cytokines with obesity and BMI and their participation in the pathophysiology of weight gain are frequently reported. Therefore, obesity is referred to as a state of low-grade chronic metabolic inflammation or meta-inflammation16, 17.
Meta-inflammation involves the participation of immune response cells, especially activated monocytes and macrophages. These cells infiltrate adipose tissue where they are transformed to macrophages or adipose tissue macrophages, inducing the maturation and expansion of adipose tissue and an increase in the size of fat cells. Adipose tissue macrophages can be classified as M1 macrophages, which produce IL-6, TNF-α, MCP-1, CD11c, and inducible nitric oxide synthase (iNOS), and M2 macrophages, which produce IL-10, transforming growth factor beta 1 (TGF-β1) and arginine30.
IL-1β, which is produced and detected in meta-inflammation of obesity, alters the production of inflammatory cytokines and chemokines in pre-adipocytes. Pre-adipocytes incubated with IL-1β release chemokines and inflammatory cytokines within a period of 24 h. An increase could also be detected by quantitative polymerase chain reaction after 4 h of incubation. IL-1β stimulates the secretion of IL-6, IL-8, IL-10, IL-13, MCP-4, TNF-α and IP-10 by monocytes, macrophages, preadipocytes, and adipocytes. These cells seem to be sensitive to the action of and exposure to IL-1β, inducing the secretion of inflammatory cytokines. These facts suggest that elevation of this cytokine may be a trigger for the production of inflammatory cytokines and chemokines associated with vascular and tissue damage in obesity31, 32.
IL-6 is secreted by M1 macrophages, adipocytes, and fibroblasts. This production is associated with exposure to high levels of glucose33. In addition to these effects, IL-6 seems to regulate body weight, lipid metabolism34, 35, insulin resistance36,37,38, and the production of C-reactive protein. Stating that IL-6 is a cause or a consequence of meta-inflammation is still controversial but some studies have demonstrated that adipocytes respond positively to this cytokine or produce it. Obesity upregulates IL-6 expression and IL-6 receptor (IL-6R) in adipose tissue and that this production contributes to the meta-inflammation in obesity37, 39.
Macrophages are sources of IL-10 in overweight inflammation. This cytokine plays a role in the containment of the immune response, modulating and interfering with the innate and adaptive response. The increase in IL-10 is cited as an independent factor of nonalcoholic fatty liver disease (NAFLD) in obese children, suggesting that this cytokine is a protective factor against NAFLD40. A study investigating the participation of IL-10 in an experimental model of steatosis suggested that CCR7+ mononuclear cells in the liver could regulate obesity-induced hepatic steatosis via the induction of IL-10-expressing invariant natural killer T cells41.
Cytokines in general may serve as auxiliary tools in the diagnosis of MetS but should not be employed individually. These mediators of innate immunity can complement clinical and laboratory parameters already documented in obese adolescents. It is important to point out that, although obesity is characterized by a state of inflammation, not all cytokines are detectable in serum. The present study analyzed cytokines produced by M1 macrophages, the target cells in obesity studies. Obese individuals with metabolic problems exhibit an increase in TNF-α, IL-6 and IL-1β accompanied by a decrease in adiponectin42. Several studies have suggested an association with the presence of M1 macrophages and metabolic disorder.
The use of these cytokines as a diagnostic method must be interpreted with caution. In general, the accuracy values obtained in the present study for the cytokines are considered good (0.80 to 0.89) but not excellent (> 0.90)43. However, these cytokines certainly reflect the inflammatory state of the individual with excess weight and can be used to monitor the presence of inflammation which, in turn, causes tissue and vascular damage and induces metabolic changes.
The evaluation of MCP-1 and MIG chemokine levels did not differ in the groups studied, except for IP-10. The levels of IP-10 were higher in the severe obesity group and the accuracy obtained for this chemokine was 0.8. Among obese individuals, elevated serum IP-10 levels have been observed in patients with heart problems compared to those without such problems and have been associated with left ventricular failure and possible unsuccessful cardiac remodeling44, 45. This chemokine is secreted by macrophages and monocytes after stimulation with interferon gamma (IFN-γ) and is chemotactic for monocytes/macrophages, T cells, natural killer cells, and dendritic cells. In addition to these associations, IP-10 induces the proliferation of vascular smooth muscle cells, suggesting its participation in the onset and aggravation of atherosclerosis46.
Obesity is a chronic inflammatory state that is characterized by the presence of inflammatory and anti-inflammatory cytokines and chemokines produced by M1 macrophages. Elucidating their role in the pathophysiology of obesity and its comorbidities may permit to identify intracellular activation pathways and therapeutic targets47. The chemokines MCP-1, IP-10 and IL-8 have been indicated as therapeutic targets for hypertension because of their participation in atherosclerosis, myocardial complications, and renal fibrosis48.
Regarding the presence of ADV36, this evaluation was not significant in the comparison between the groups of obesity and positivity for ADV36, but there was a difference in the evaluation within the severe obesity group, with a higher frequency of severe obesity adolescents positive for ADV36. The presence of infection is related to increased BMI (Table 6).
The association of the presence of ADV36 with obesity has been described since 2000 in adults49 and since 2010 in children50. ADV36 induces differentiation or adipogenesis of somatic cells to adipocytes. This change is mediated by incorporation of the viral gene early gene 4, open reading frame 1 (E4-ORF1) in the cell nucleus, which accelerates adipogenesis and induces the production of inflammatory and anti-inflammatory cytokines and adipokines. The increase in adipocytokines such as MCP-1, TNF-α, IL-1, and IL-6 causes an increase in fat nodules and alters fat metabolism during the inflammatory process. M1 macrophages appear to play a key role in cytokine production and adipose tissue inflammation26, 51,52,53,54.
In a study of 291 children, Berger et al.55 found an increase in TNF-α and IL-6 in ADV36-positive children. The odds ratio for TNF-α and IL-6 was 2.2 and 2.4, respectively, in ADV36-positive children aged 9–13 years. In addition to these data, some experimental studies using mouse macrophages have shown that ADV36 induces the production of MCP-1 in vitro53.
In conclusion, IL-1β, IL6, IL-10, and IP-10 levels are elevated in adolescents with severe obesity and these cytokines can serve as a tool for the diagnosis of MetS. As for the limitations of the study, it was not possible to make a food survey, due to the inability to keep adolescents under surveillance of food eaten for 3 days and associate the type of food with inflammation. Regarding the presence of ADV36 infection, there was an increase in BMI in the obese group, bringing these indices closer to the severe obesity group, suggesting that ADV36 causes aggravation of weight gain. A larger sample is needed to confirm the association of infection with BMI gain. The correlation of infection with sex and MetS did not occur, despite the higher frequency in girls.
Methods
Study design
Cross-sectional study of male and female adolescents aged 10 to 16 complete years, who were seen at the Botucatu Medical School, Unesp, from September 2018 to September 2019, and who did not use medications. Participants were consecutively included and allocated to the groups according to the degree of obesity. The sample consisted of 97 adolescents, including 36 overweight, 36 obese and 25 severe obesity individuals.
Ethics declaration
The Ethics Committee on Research Involving Humans of the Botucatu Medical School, Unesp, São Paulo, Brazil, approved the study on November 9, 2020 (Approval number 4.399.388). All methods were performed in accordance with the relevant guidelines and regulations. All adolescents and legal representatives signed the free informed consent form for inclusion in the study.
Clinical variables
Weight and height were obtained according to the National Health and Nutrition Examination Survey56.
The nutritional status was evaluated using age- and sex-specific BMI [weight (kg)/height2 (m)] curves and the respective cut-off points proposed by Kuczmarski et al.56. Overweight, obesity and severe obesity were defined according to Kuczmarski et al.56 and Freedman et al.57. The following sex- and age-specific definitions were adopted: overweight, 85th ≥ BMI < 95th; obese, 95th ≥ BMI ≤ 99th; severe obesity, BMI > 99th.
Waist circumference was measured as described by Rizzo et al.58 and the values were compared to the values of the 90th percentile for abdominal circumference according to age and sex59.
The SBP and DBP were measured twice and the mean of these measurements was used for analysis60.
Laboratory tests
To evaluate the presence of MetS criteria in the adolescents, the following laboratory parameters were measured in a Vitros 950 dry chemical analyzer (Johnson & Johnson): total cholesterol and fractions [high-density lipoprotein (HDL), low-density lipoprotein (LDL) and very low-density lipoprotein (VLDL)], triglycerides, and fasting glucose. The HOMA-IR [(fasting blood glucose mmol/L) × (fasting insulinemia µU/ml)/22.5]61 and QUICKI [1/log (fasting insulinemia µU/ml) + log (fasting blood glucose mg/dl)]62 values were calculated based on the fasting blood glucose and insulin measurements to identify probable insulin resistance. The measurements were performed in the morning after a 10-h fast.
Definition of MetS in adolescents aged 10 to 16 years
MetS was defined based on the presence of central obesity using the respective waist circumference percentiles (≥ 90th percentile for sex and age), combined with three additional factors (elevated triglycerides, low HDL-cholesterol, arterial hypertension, and hyperglycemia). The following altered values were considered for both sexes: triglycerides ≥ 150 mg/dL, HDL-cholesterol < 40 mg/dL, arterial hypertension with SBP ≥ 130 mmHg or DBP ≥ 85 mmHg, and fasting glucose ≥ 100 mg/dL or a previous diagnosis of type 2 diabetes15, 58.
Exclusion criteria
Adolescents with the presence of metabolic, endocrine or genetic disease verified by the history of the current disease, the general physical examination and laboratory or radiodiagnostic procedures, adolescents with diabetes mellitus, gastrointestinal disease, kidney disease, early or late puberty, current or past pregnancy, who used hormonal contraceptives, in corticosteroid therapy and in chronic use of medications, as well as adolescents who did not attend the commitments to measure clinical variables or laboratory tests were excluded from the study.
Quantification of cytokines and chemokines by cytometry
Cytokines IL-1β, IL-6, IL-8, IL-10, IL-12, TNF-α and chemokines IP-10, MCP-1, MIG were quantified by ELISA using beads coated with monoclonal antibodies against each cytokine analyzed. Phycoerythrin (PE) was used as an antibody detector against each cytokine of interest.
Briefly, beads labeled with different fluorescence intensities were mixed in a tube at a rate of 10 µL/test of each bead coated with the specific anti-cytokine antibody and the procedures recommended by the manufacturer were followed. A volume of 50 µL of the bead mixture was transferred to the test tubes and reserved for later addition of the samples and recombinant standard. After this procedure, the PE-labeled detector antibody was added. Fluorescence of the labeled beads was acquired in a FACSCanto II cytometer (BD Biosciences, USA) and the data were analyzed using the FlowJo software, following the procedures of the manufacturer of the Human Inflammation and Human Chemokine kits (BD Biosciences, USA). A total of 1,800 or 300 events were counted for each bead or cytokine.
Quantification of anti-ADV36 antibody in plasma
The anti-ADV36 antibody was analyzed qualitatively by ELISA using the MMBS 9310682 kit (MyBiosource, San Diego, CA, USA). A cut-off value of 0.194 was defined, i.e., samples with an optical density above the cut-off were defined as positive.
Statistical analysis
The results were first analyzed by the Shapiro–Wilk test to verify the normality of the data. Parametric variables were compared between two groups by the unpaired t test and between three or more groups by one-way analysis of variance (ANOVA) followed by the Tukey test. Nonparametric variables were compared between groups using the Mann–Whitney test or Kruskal–Wallis test followed by Dunn’s test. ROC curves were constructed to evaluate the accuracy of the cytokines and the cut-off value of each cytokine was obtained from the inflection point of the curve. The chi-squared test or Fisher’s exact test was used to compare categorical data/frequencies. Data were analyzed using the SigmaPlot 12.0 for Windows statistical package (Jandel Corporation, CA, USA). Differences were considered significant when p < 0.05.
Data availability
All the data generated or analyzed during this study are included in this published article.
References
Bahia, L. et al. The costs of overweight and obesity-related diseases in the Brazilian public health system: Cross-sectional study. BMC Public Health 12, 440 (2012).
Hales, C. M., Carroll, M. D., Fryar, C. D. & Ogden, C. L. Prevalence of obesity among adults and youth: United States, 2015–2016 key findings data from the national health and nutrition examination survey. NCHS Data Br 288, 1–8 (2017).
Weihrauch-Blüher, S., Schwarz, P. & Klusmann, J. H. Childhood obesity: increased risk for cardiometabolic disease and cancer in adulthood. Metabolism 92, 147–152 (2019).
Ponterio, E. & Gnessi, L. Adenovirus 36 and obesity: An overview. Viruses 7, 3719–3740 (2015).
Goodman, E., Daniels, S. R., Meigs, J. B. & Dolan, L. M. Instability in the diagnosis of metabolic syndrome in adolescents. Circulation 115, 2316–2322 (2007).
Kumar, S. & Kelly, A. S. Review of childhood obesity: From epidemiology, etiology, and comorbidities to clinical assessment and treatment. Mayo Clin. Proc. 92, 251–265 (2017).
Fang, X. et al. Causal association of childhood obesity with cancer risk in adulthood: A Mendelian randomization study. Int. J. Cancer 149, 1421–1425 (2021).
Ma, Y. et al. Determinants of racial/ethnic disparities in incidence of diabetes in postmenopausal women in the U.S.: The women’s health initiative 1993–2009. Diabetes Care 35, 2226–2234 (2012).
Zhang, H. & Rodriguez-Monguio, R. Racial disparities in the risk of developing obesity-related diseases: A cross-sectional study. Ethn. Dis. 22, 308–316 (2012).
Kitahara, C. M. et al. Association between class III obesity (BMI of 40–59 kg/m2) and mortality: A pooled analysis of 20 prospective studies. PLoS Med. 11, e1001673 (2014).
Tanamas, S. K. et al. Quantifying the proportion of deaths due to body mass index- and waist circumference-defined obesity. Obesity 24, 735–742 (2016).
Weihe, P., Spielmann, J., Kielstein, H., Henning-Klusmann, J. & Weihrauch-Blüher, S. Childhood obesity and cancer risk in adulthood. Curr. Obes. Rep. 9, 204–212 (2020).
Cook, S., Weitzman, M., Auinger, P., Nguyen, M. & Dietz, W. H. Prevalence of a metabolic syndrome phenotype in adolescents findings from the third national health and nutrition examination survey, 1988–1994. Arch. Pediatr. Adolesc. Med. 157, 821–827 (2003).
Fahed, G. et al. Metabolic syndrome: Updates on pathophysiology and management in 2021. Int. J. Mol. Sci. 23, 786 (2022).
Zimmet, P. et al. The metabolic syndrome in children and adolescents: An IDF consensus report. Pediatr. Diabetes 8, 299–306 (2007).
Gregor, M. F. & Hotamisligil, G. S. Inflammatory mechanisms in obesity. Annu. Rev. Immunol. 29, 415–445 (2011).
Lumeng, C. N. & Saltiel, A. R. Inflammatory links between obesity and metabolic disease. J. Clin. Invest. 121, 2111–2117 (2011).
Guerreiro, V. A., Carvalho, D. & Freitas, P. Obesity, adipose tissue, and inflammation answered in questions. J. Obes. 2022, 1–11 (2022).
Martinez, F. O. & Gordon, S. The M1 and M2 paradigm of macrophage activation: Time for reassessment. F1000Prime Rep. 6, 13 (2014).
Kim, C. S. et al. Circulating levels of MCP-1 and IL-8 are elevated in human obese subjects and associated with obesity-related parameters. Int. J. Obes. (Lond.) 30, 1347–1355 (2006).
Mikhailova, S. V. & Ivanoshchuk, D. E. Innate-immunity genes in obesity. J. Pers. Med. 11, 1201 (2021).
Hueso, L. et al. Upregulation of angiostatic chemokines IP-10/CXCL10 and I-TAC/CXCL11 in human obesity and their implication for adipose tissue angiogenesis. Int. J. Obes. (Lond.) 42, 1406–1417 (2018).
Chang, C. C. et al. Interferon gamma-induced protein 10 is associated with insulin resistance and incident diabetes in patients with nonalcoholic fatty liver disease. Sci. Rep. 5, 10096 (2015).
Chou, S. Y. et al. CCL5/RANTES contributes to hypothalamic insulin signaling for systemic insulin responsiveness through CCR5. Sci. Rep. 6, 37659 (2016).
Harakeh, S. et al. Chemokines and their association with body mass index among healthy Saudis. Saudi J. Biol. Sci. 27, 6–11 (2020).
Genoni, G. et al. Obesity and infection: Two sides of one coin. Eur. J. Pediatr. 173, 25–32 (2014).
Marjani, A. et al. Adenovirus 36 infection and obesity meta-analysis of community-based studies. Rev. Med. Virol. 32, e2255 (2022).
Esposito, S., Preti, V., Consolo, S., Nazzari, E. & Principi, N. Adenovirus 36 infection and obesity. J. Clin. Virol. 55, 95–100 (2012).
Tanner, J. M. Growth and maturation during adolescence. Nutr. Rev. 39, 43–55 (1981).
Michaud, A., Pelletier, M., Noël, S., Bouchard, C. & Tchernof, A. Array and protein array studies demonstrate that abdominal adipose tissues. Obesity (Silver Spring) 21, 2342–2349 (2013).
Alomar, S. Y. et al. PCR array and protein array studies demonstrate that IL-1 β (interleukin-1 β) stimulates the expression and secretion of multiple cytokines and chemokines in human adipocytes. Arch. Physiol. Biochem. 121, 187–193 (2015).
Alomar, S. Y., Gentili, A., Zaibi, M. S., Kępczyńska, M. A. & Trayhurn, P. IL-1β (interleukin-1β) stimulates the production and release of multiple cytokines and chemokines by human preadipocytes. Arch. Physiol. Biochem. 122, 117–122 (2016).
Sundararaj, K. P. et al. Interleukin-6 released from fibroblasts is essential for up-regulation of matrix metalloproteinase-1 expression by U937 macrophages in coculture: Cross-talking between fibroblasts and U937 macrophages exposed to high glucose. J. Biol. Chem. 284, 13714–13724 (2009).
Mohamed-Ali, V. et al. Subcutaneous adipose tissue releases interleukin-6, but not tumor necrosis factor-α, in vivo. J. Clin. Endocrinol. Metab. 82, 4196–4200 (1997).
Shoelson, S. E., Lee, J. & Goldfine, A. B. Inflammation and insulin resistance. Erratum in: J. Clin. Invest. 116, 1793–1801 (2006).
Senn, J. J., Klover, P. J., Nowak, I. A. & Mooney, R. A. Interleukin-6 induces cellular insulin resistance in hepatocytes. Diabetes 51, 3391–3399 (2002).
Eder, K., Baffy, N., Falus, A. & Fulop, A. K. The major inflammatory mediator interleukin-6 and obesity. Inflamm. Res. 58, 727–736 (2009).
Schultz, O. et al. Effects of inhibition of interleukin-6 signalling on insulin sensitivity and lipoprotein (A) levels in human subjects with rheumatoid diseases. PLoS ONE 5, e14328 (2010).
Sindhu, S. et al. Obesity is a positive modulator of IL-6R and IL-6 expression in the subcutaneous adipose tissue: Significance for metabolic inflammation. PLoS ONE 10, e0133494 (2015).
Shi, J.-Q., Shen, W.-X., Wang, X.-Z., Huang, K. E. & Zou, C.-C. Relationship between immune parameters and non-alcoholic fatty liver disease in obese children. Indian Pediatr. 54, 825–829 (2017).
Kim, H. M. et al. iNKT cells prevent obesity-induced hepatic steatosis in mice in a C-C chemokine receptor 7-dependent manner. Int. J. Obes. (Lond.) 42, 270–279 (2018).
Navarro, E., Funtikova, A. N., Fíto, M. & Schröder, H. Can metabolically healthy obesity be explained by diet, genetics, and inflammation?. Mol. Nutr. Food Res. 59, 75–93 (2015).
Polo, T. C. F. & Miot, H. A. Use of roc curves in clinical and experimental studies. J. Vasc. Bras. 19, e20200186 (2020).
Altara, R. et al. Left ventricular dysfunction and CXCR3 ligands in hypertension: From animal experiments to a population-based pilot study. PLoS ONE 10, e0141394 (2015).
Altara, R. et al. CXCL10 is a circulating inflammatory marker in patients with advanced heart failure: A pilot study. J. Cardiovasc. Transl. Res. 9, 302–314 (2016).
Wang, H. J. et al. IP-10/CXCR3 axis promotes the proliferation of vascular smooth muscle cells through ERK1/2/CREB signaling pathway. Cell Biochem. Biophys. 75, 139–147 (2017).
Martos-Moreno, G. A., Kopchick, J. J. & Argente, J. Adipoquinas en el nin˜o sano y con obesidad. An. Pediatr. (Barc.) 78(189), e1-189.e15 (2013).
Martynowicz, H., Janus, A., Nowacki, D. & Mazur, G. The role of chemokines in hypertension. Adv. Clin. Exp. Med. 23, 319–325 (2014).
Dhurandhar, N. V. et al. Increased adiposity in animals due to a human virus. Int. J. Obes. Relat. Metab. Disord. 24, 989–996 (2000).
Almgren, M. et al. Adenovirus-36 is associated with obesity in children and adults in Sweden as determined by rapid ELISA. PLoS ONE 7, e41652 (2012).
Pasarica, M. et al. Adipogenic human adenovirus Ad-36 induces commitment, differentiation, and lipid accumulation in human adipose-derived stem cells. Stem Cells 26, 969–978 (2008).
Rogers, P. M. et al. Human adenovirus Ad-36 induces adipogenesis via its E4 orf-1 gene. Int. J. Obes. (Lond.) 32, 397–406 (2008).
Na, H. N. & Nam, J. H. Adenovirus 36 as an obesity agent maintains the obesity state by increasing MCP-1 and inducing inflammation. J. Infect. Dis. 205, 914–922 (2012).
Kocazeybek, B. et al. Evaluation of Adenovirus-36 (Ad-36) antibody seropositivity and adipokine levels in obese children. Microb. Pathog. 108, 27–31 (2017).
Berger, P. K. et al. Association of adenovirus 36 infection with adiposity and inflammatory-related markers in children. J. Clin. Endocrinol. Metab. 99, 3240–3246 (2014).
Kuczmarski, R. J. et al. 2000 CDC growth charts for the United States: Methods and development. Vital Health Stat. 246, 1–190 (2002).
Freedman, D. S., Mei, Z., Srinivasan, S. R., Berenson, G. S. & Dietz, W. H. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: The Bogalusa heart study. J. Pediatr. 150, 12-17.e2 (2007).
Rizzo, A. C. et al. Metabolic syndrome risk factors in overweight, obese, and extremely obese Brazilian adolescents. Nutr. J. 12, 19 (2013).
Fernández, J. R., Redden, D. T., Pietrobelli, A. & Allison, D. B. Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J. Pediatr. 145, 439–444 (2004).
Sinaiko, A. R. et al. Influence of insulin resistance and body mass index at age 13 on systolic blood pressure, triglycerides, and high-density lipoprotein cholesterol at age 19. Hypertension 48, 730–736 (2006).
Matthews, D. R. et al. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412–419 (1985).
Katz, A. et al. Quantitative insulin sensitivity check index: A simple, accurate method for assessing insulin sensitivity in humans. J. Clin. Endocrinol. Metab. 85, 2402–2410 (2000).
Acknowledgements
This work was supported by the state funding agency Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP; Grant 14/24345-0), Brazil, and by the Pro-Rectory of Research (PROPe; Public Notice 01/2023), Unesp, Brazil.
Author information
Authors and Affiliations
Contributions
M.D.S, T.B.L.G. and C.S.K. designed the study. M.D.S., A.C.B.R., V.L.S., L.N.M., G.G.R., C.M.G., J.P.A.J., G.R.L. and I.R.B. collected the anthropometric and clinical data. M.D.S., A.C.B.R., V.L.S., L.N.M., G.G.R. and C.M.G. contributed to the cytokine measurements. M.D.S. and C.S.K. analyzed the data and wrote the manuscript. All authors reviewed the results and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sanches, M.D., Goldberg, T.B.L., Rizzo, A.d.B. et al. Inflammatory cytokines and chemokines in obese adolescents with antibody against to adenovirus 36. Sci Rep 13, 9918 (2023). https://doi.org/10.1038/s41598-023-33084-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-33084-4
- Springer Nature Limited
This article is cited by
-
Pro- and anti-inflammatory cytokines are the game-changers in childhood obesity-associated metabolic disorders (diabetes and non-alcoholic fatty liver diseases)
Reviews in Endocrine and Metabolic Disorders (2024)