
Abstract
Multimorbidity (MM) prevalence among older adults is increasing worldwide. Variations regarding the socioeconomic characteristics of the individuals and their context have been described, mostly in high-income settings. However, further research is needed to understand the effect of the coexistence of infectious diseases along with socioeconomic factors regarding MM. This study aims to examine the variation of MM regarding infectious diseases mortality after adjusting for socioeconomic factors. A cross-sectional multilevel study with a nationally representative sample of 17,571 Colombian adults of 60 years of age or older was conducted. Individual socioeconomic, demographic, childhood and health related characteristics, as well as group level variables (multidimensional poverty index and infectious diseases mortality rate) were analyzed. A two-level stepwise structural equation model was used to simultaneously adjust for the individual and contextual effects. Multimorbidity prevalence was 62.3% (95% CI 61.7–62.9). In the multilevel adjusted models, age, female sex, having functional limitations, non-white ethnicity, high body mass index, higher income, physical inactivity and living in urban areas were associated with multimorbidity among the sample for this study. The median odds ratio for multidimensional poverty was 1.18 (1.16–1.19; p = 0.008) and for infectious diseases was 1.25 (1.22–1.28; p = 0.014). This paper demonstrates that MM varies regarding the mortality of infectious diseases and shows a strong association between MM and poverty in a low-middle income country. Differences in the factors involved in the etiology of multimorbidity are expected among wealthy and poor countries regarding availability and prioritization of health services.
Similar content being viewed by others

Introduction
Multimorbidity (MM), considered as the co-existence of two or more chronic conditions1,2 has been estimated to affect approximately 50 million people in Europe3 and one third of adults in Latin American countries4. In Colombia, among the registries of health services provided between 2012 and 2016, almost 6 million correspond to patients living with multimorbidity per year5. This figure is expected to increase since the prevalence of MM pursue advances along with the demographic transition6. Estimates in Europe report figures rising from 11% in adults aged 25–44 years to 65% for those aged 65–84 years, and up to 82% in those 85 years and older7. A similar trend is observed for Colombia with figures ranging from 33.1% in adults to 51.3% in people aged 60 or older5. Moreover, MM has been associated with poor health outcomes including functional decline8,9,10, excess of mortality11,12, decrease in quality of life levels10 and high economic costs of care due to increased hospitalization rates13 and polypharmacy14.
Variations in the prevalence of MM have also been associated with demographic and socioeconomic characteristics, being higher in women, single, widowed or divorced15, persons of lower socioeconomic levels and in those living in disadvantage settings1,10,16. Socioeconomic factors such as low-educational status16,17, childhood adversity18, and reduced lifetime earnings are related to an increased risk of developing MM in late life19. Likewise, previous research have indicated that MM rates are higher among population groups with greater difficulties accessing to drinking-water and energy for lighting sources20, as well as in areas with higher rates of unemployment and household overcrowding21,22. In particular, the prevalence of MM has been reported to be almost twice as high in areas of high socioeconomic deprivation (11.0%, 95% CI 10.9–11.2), compared to more affluent areas (5.9%, 5.8–6.0)21.
As it has been widely recognized, poor populations usually face the simultaneous effects of both chronic and infectious diseases. Similar to the association of chronic conditions with socioeconomic deprivation, those living in poorer communities are also more vulnerable to communicable diseases than the most affluent ones23, and these effects could be more serious in older adults due to the immunosenescence that make this population more susceptible to infections24. As long as the effect of the coexistence of infectious diseases along with socioeconomic factors regarding MM is not recognized, particular measures of prevention or even health needs could be omitted in regions where communicable diseases are endemic. Therefore, in this paper we examined the variation of MM regarding infectious diseases mortality after adjusting for the effects of socioeconomic factors.
Methods
Study design
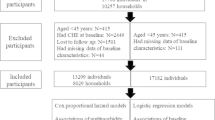
A cross-sectional multilevel study was developed using secondary data from the Colombian population-based survey Health, Wellbeing and Aging (Salud, Bienestar y Envejecimiento—SABE), carried out in 2015. The SABE study included 23,694 individuals aged over 60 years living in urban and rural areas of the 32 Colombian departments (i.e., states). Participants were selected by a probabilistic, multistage and stratified sampling design. Data collection was completed using in-person surveys. For the analyses, a sample of 17,571 participants was used once records with missing information were excluded. Detailed information about the SABE study and the sampling method can be found elsewhere25.
Variables
For the analysis “Multimorbidity” was considered the dependent variable, defined as the coexistence of two or more non-communicable diseases: diabetes, hypertension, cancer, lung disease (chronic obstructive pulmonary disease, asthma, bronchitis or emphysema), heart disease, stroke, joint diseases (arthritis, rheumatism or osteoarthritis), osteoporosis, depressive symptoms and other mental illnesses (mental or psychiatric problem). Except for depression, which was assessed with the Short Form of the Geriatric Depression Scale26, all morbidities were self-reported. A score of 6 or more was used as indicator of depression in the population26,27.
The independent variables of interest were both at individual and at group level. At individual level, the following categorical and continuous sociodemographic characteristics were used: Sex (female/male (reference category)), Age (continuous), Marital status (single, widowed or divorced/married or living with a partner (ref)), Ethnicity (non-white/white (ref)), Income (mean income less than $7.83/day/income of $7.83/day/more than $7.83/day (ref)), Educational level (secondary or lower level/higher level (ref)), Victim of armed displacement, defined as ever been displaced by armed conflict or violence (yes/no (ref)), Area of residence (rural/urban (ref)). Health and lifestyle-related variables included were Functional limitation defined as having a Barthel score of < 10028 (yes/no (ref)), Body Mass Index (BMI) (low (< 22)/overweight/obesity (> 27)/normal weight (22–27) (ref))29, Physical inactivity or a low level score of physical activity in the short-form International Physical Activity Questionnaire—IPAQ-SF30 (yes/no (ref)) and Smoking (current or former smoker/nonsmoker (ref)). Childhood-related factors were also included as Self-perceived childhood economic situation (fair/poor/good (ref)) and Self-perceived childhood health status (poor or fair/good (ref)).
At state-level, we used the prevalence of the multidimensionally poor31 for 201832 and infectious diseases mortality rate for 201633. To evaluate multidimensional poverty (MP), 5 dimensions with 15 indicators are measured, including: education, childhood and youth conditions (school attendance, childcare services), employment (informality, long-term unemployment), health (access, insurance), access to public utilities (water source, sewer system) and housing conditions (floors and walls material, overcrowding)31. Those deprived in 5 or more indicators are considered as multidimensionally poor34.
Statistical analysis
Descriptive analysis of the individual characteristics was based on the absolute and relative frequencies with 95% confidence intervals (95% CI) for categorical variables, and measures of central tendency and dispersion (mean and standard deviation (SD)) for quantitative variables. To identify differences between baseline characteristics, independent X2 test and t-test analyses were developed for categorical and continuous variables respectively. Variables with p-values below 25% were considered for the adjusted models. A first one-level logistic model was used to evaluate the associations between the individual variables with MM, and significant variables (p < 0.05) were included in a multilevel stepwise backward model. To evaluate the variability of MM prevalence across states, the median OR (MOR)35 was calculated. Correlation was evaluated between MM and MP, between MM and infectious diseases mortality, and between infectious diseases mortality and MP, using Pearson correlation coefficients. A two-level structural equation model (SEM) was used to assess the association among individual and contextual variables with MM. The effect of state-level variables that were not measured, due to secondary data availability, was incorporated into the model through a latent variable. MP, BMI, physical activity and functionality were considered correlated in the model36. Sample weights were used in all the analyses.
Ethics declarations
All methods in the present study were carried out in accordance with relevant guidelines and regulations. Ethics approval was granted by the Institutional Committee of Human Ethics of the Fundación Santa Fe de Bogotá Hospital. The approval ID is CCEI-11861-2020. As clinical data was used, participants provided written informed consent before enrolling in the SABE study25.
Results
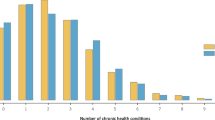
The overall prevalence of MM in the Colombian sample who were 60 years of age or older was 62.3% (95% CI 61.7–62.9%), the average age was 70.8 years (SD = 8.2) and 57.3% (56.7–58.0%) were women. Most frequent diseases in the population were depression, 56.9% (56.2–57.6), hypertension, 53.9% (53.2–54.6), and joint disease, 26.0% (25.3–26.6). Those living with two or more conditions suffered mainly of hypertension and depression (25.5%), hypertension and joint disease (16.3%), and hypertension and diabetes (12.5%) (Table 1).
Crude comparisons at individual-level showed that all variables were significantly associated with MM except for educational status and smoking (Table 2). Once adjusted, the effects that remained significant were age, sex, having functional limitations, body mass index (BMI), income, physical inactivity, non-white ethnicity and living in urban areas (Table 3).
At state-level, the prevalence of MM varied between 42.6% (36.6–48.9) and 74.1% (69.2–78.5), where the ages ranged from 60 to 93 years (mean = 69.0; SD = 7.7) and from 60 to 96 years (mean = 69.3; SD = 7.5), respectively. MP varied from 4.4 to 65.0 (mean = 28.2; SD = 15.1), where ages ranged from 60 to 101 years (mean = 70.8; SD = 8.2) and from 60 to 90 years (mean = 68.7; SD = 6.3), respectively. Infectious diseases mortality rate varied from 12.6/100,000 to 51.0/100,000 (mean = 35.9/100,000; SD = 1.7) (Table 4), and the ages ranged from 60 to 96 years (mean = 69.3; SD = 7.5) and from 60 to 90 years (mean = 68.7; SD = 6.3). Correlation between MM prevalence and MP was of − 0.80 (p < 0.001), between MM and infectious diseases mortality of − 0.40 (p = 0.022), and between infectious diseases mortality and MP of 0.18 (p = 0.320).
Adjusted analyses indicated a significant inter-state variability. The MOR for MP was 1.18 (1.16–1.19; p = 0.008) and for infectious diseases was 1.25 (1.22–1.28; p = 0.014). The association between MP and MM was also mediated by physical inactivity (p = 0.001), BMI (p = 0.002) and functional limitation (p = 0.001). All individual variables were directly associated with MM in the model (Fig. 1).

Final structural equation model (SEM). Odds ratio, median odds ratio and P-values. aMedian odds ratio; *p < 0.001; **p < 0.05; ***p > 0.05.
Discussion
This study found a 63% prevalence of multimorbidity among Colombian older adults when considering a list of ten chronic conditions and a cut-off point of 2 or more concurrent morbidities for its definition, including diabetes, hypertension, cancer, lung disease, heart disease, stroke, joint disease, osteoporosis, depressive symptoms and other mental illnesses. Compared to findings from other authors, this corresponds to earlier studies in developing countries such as Brazil and Argentina, in which the prevalence of MM among older adults has been reported to be of 66.3%37 and 60.6%38, respectively. In this study, around 30% of those living with MM had poor functional status, which reinforces the need for preventive, coordinated and non-fragmented care21.
In this study MM prevalence increases with age, is higher in women and in individuals with high body mass index as reported before6,19. Our results also showed that in the states with higher infectious diseases mortality rate, MM was less likely to be reported. In deprived contexts, where infectious diseases are more prevalent, decision makers are compelled to assign significant portions of resources to the attention and diagnosis of these diseases displacing the care of chronic conditions, in particular MM39.
In contrast to previous studies our results indicate lower levels of MM in people living in middle/high income or less deprived settings. Barnett et al.21 and Salisbury et al.22, in a Scottish and English population, respectively, found that people living in more deprived settings were more likely to be living with MM. These dissimilarities could derive from methodological matters including the use of clinical records and a more specific list of morbidities for the definition of MM in these studies21,22. Also, a better opportunity to be diagnosed or have a medical evaluation in more affluent settings could partly explain them; in fact, in less prosperous contexts, limited availability of resources is associated with a lower rate in diagnosis of non-communicable diseases40,41,42.
Furthermore, the use of self-assessments instead of using medical records, could have led to a difficulty to accurately recall diagnosed chronic diseases. In addition, ongoing treatment might be higher in more affluent populations with better access to medical care which can improve the diagnosis self-reports40.
Living in a rural residence, being non-white ethnicity and low household income, all of which have been related with deprivation, were also associated with lower risk of reporting multiple chronic conditions. Similar findings have been found by previous research40,43, and are also related with the accessibility to public and private services. Therefore, our results might reflect an under-reported prevalence of MM in poor regions and populations due to difficulties in the access to health services and limited resource availability for adequate diagnosis.
Our findings contrast mainly with studies conducted in high-income countries. However, comparisons among national-level figures must consider differences among access to healthcare, services coverages and deprivation level among the poor, which might not be the same between countries. Moreover, an under-diagnosis or the lag in diagnosis also affects prevalence estimations.
Limitations in our study need to be considered. The self-reported measures of conditions (except depressive symptoms) can underestimate the prevalence; also, effects could be underestimated due to differences between analyzed and excluded individuals, who were significantly older, had a higher proportion of women and had less education and income. Likewise, as secondary data were used, care needs or the severity of the diseases could not be included for the analyses. Unequal weights regarding the type and severity of the conditions are warranted to assess the impact of multimorbidity in the population40.
Considering the above, this paper demonstrates that MM varies between areas regarding mortality of infectious diseases and shows a strong association between MM and poverty in a low-middle income setting. This study found lower levels of MM among individuals in states of high infectious disease mortality rate and in less deprived settings. Further research is needed to better understand the role of deprivation due the scarce number of publications coming from the developing world. Considerable differences in the factors involved in the etiology of MM are expected among high-, middle- and low-income countries regarding availability and prioritization of health services.
Data availability
The data that support the findings of this study are available from the Colombian Ministry of Health and Social Protection but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the Ministry of Health and Social Protection. The datasets regarding group level variables generated during and/or analysed during the current study are available in the National Administrative Department of Statistics repository, https://www.dane.gov.co/index.php/estadisticas-por-tema/pobreza-y-condiciones-de-vida/pobreza-y-desigualdad/pobreza-monetaria-y-multidimensional-en-colombia-2018#pobreza-por-departamentos-2018.
References
Xu, X., Mishra, G. D. & Jones, M. Evidence on multimorbidity from definition to intervention: An overview of systematic reviews. Ageing Res. Rev. 37, 53–68. https://doi.org/10.1016/j.arr.2017.05.003 (2017).
World Health Organization. Multimorbidity: Technical Series on Safer Primary Care. https://apps.who.int/iris/bitstream/handle/10665/252275/9789241511650-eng.pdf?sequence=1&isAllowed=y. (Accessed 8 January 2021)
Rijken, M., Struckmann, V., van der Heide, I., et al. European Observatory Policy Briefs. in How to improve care for people with multimorbidity in Europe? (Eds. Richardson, E., Van Ginneken, E.) European Observatory on Health Systems and Policies© NIVEL and TU Berlin (2017).
Macinko, J., Andrade, F. C. D., Nunes, B. P. & Guanais, F. C. Primary care and multimorbidity in six Latin American and Caribbean countries. Rev. Panam. Salud. Publica. 43, e8. https://doi.org/10.26633/rpsp.2019.8 (2019).
Alfonso-Sierra, E., Carabalí, A.A., Torres, J.B., Castro, M.L.L., Ramírez, A.P., Velásquez, L.U. Situación de Multimorbilidad en Colombia 2012–2016 (2016).
Afshar, S., Roderick, P. J., Kowal, P., Dimitrov, B. D. & Hill, A. G. Multimorbidity and the inequalities of global ageing: A cross-sectional study of 28 countries using the World Health Surveys. BMC Public Health 15, 776. https://doi.org/10.1186/s12889-015-2008-7 (2015).
Banerjee, S. Multimorbidity–older adults need health care that can count past one. Lancet 385(9968), 587–589. https://doi.org/10.1016/s0140-6736(14)61596-8 (2015).
Aarts, S. et al. The effect of multimorbidity on health related functioning: Temporary or persistent? Results from a longitudinal cohort study. J. Psychosom. Res. 73(3), 211–217. https://doi.org/10.1016/j.jpsychores.2012.05.014 (2012).
Bao, J., Chua, K. C., Prina, M. & Prince, M. Multimorbidity and care dependence in older adults: A longitudinal analysis of findings from the 10/66 study. BMC Public Health 19(1), 585. https://doi.org/10.1186/s12889-019-6961-4 (2019).
Marengoni, A. et al. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 10(4), 430–439. https://doi.org/10.1016/j.arr.2011.03.003 (2011).
Wolff, J. L., Starfield, B. & Anderson, G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch. Intern. Med. 162(20), 2269–2276 (2002).
Rivera-Almaraz, A. et al. Disability, quality of life and all-cause mortality in older Mexican adults: Association with multimorbidity and frailty. BMC Geriatr. 18(1), 236. https://doi.org/10.1186/s12877-018-0928-7 (2018).
Bahler, C., Huber, C. A., Brungger, B. & Reich, O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: A claims data based observational study. BMC Health Serv. Res. 15, 23. https://doi.org/10.1186/s12913-015-0698-2 (2015).
St John, P. D., Tyas, S. L., Menec, V. & Tate, R. Multimorbidity, disability, and mortality in community-dwelling older adults. Can. Fam. Physician. 60(5), e272–e280 (2014).
Kristensen, K., König, H.-H. & Hajek, A. The association of multimorbidity, loneliness, social exclusion and network size: Findings from the population-based German Ageing Survey. BMC Public Health 19(1), 1383. https://doi.org/10.1186/s12889-019-7741-x (2019).
Pathirana, T. I. & Jackson, C. A. Socioeconomic status and multimorbidity: A systematic review and meta-analysis. Aust. N. Z. J. Public Health. 42(2), 186–194. https://doi.org/10.1111/1753-6405.12762 (2018).
Gontijo Guerra, S., Berbiche, D. & Vasiliadis, H. M. Measuring multimorbidity in older adults: Comparing different data sources. BMC Geriatr. 19(1), 166. https://doi.org/10.1186/s12877-019-1173-4 (2019).
Schiøtz, M. L., Stockmarr, A., Høst, D., Glümer, C. & Frølich, A. Social disparities in the prevalence of multimorbidity—A register-based population study. BMC Public Health 17(1), 422. https://doi.org/10.1186/s12889-017-4314-8 (2017).
Tucker-Seeley, R. D., Li, Y., Sorensen, G. & Subramanian, S. V. Lifecourse socioeconomic circumstances and multimorbidity among older adults. BMC Public Health 11, 313. https://doi.org/10.1186/1471-2458-11-313 (2011).
Ataguba, J. E. Inequalities in multimorbidity in South Africa. Int. J. Equity Health. 12, 64. https://doi.org/10.1186/1475-9276-12-64 (2013).
Barnett, K. et al. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 380(9836), 37–43. https://doi.org/10.1016/s0140-6736(12)60240-2 (2012).
Salisbury, C., Johnson, L., Purdy, S., Valderas, J. M. & Montgomery, A. A. Epidemiology and impact of multimorbidity in primary care: A retrospective cohort study. Br. J. Gen. Pract. 61(582), e12-21. https://doi.org/10.3399/bjgp11X548929 (2011).
European Centre for Disease Prevention and Control. Health Inequalities, The Financial Crisis, and Infectious Disease in Europe (ECDC, 2013).
Pawelec, G. Age and immunity: What is “immunosenescence”?. Exp. Gerontol. 105, 4–9. https://doi.org/10.1016/j.exger.2017.10.024 (2018).
Gomez, F., Corchuelo, J., Curcio, C. L., Calzada, M. T. & Mendez, F. SABE Colombia: Survey on health, well-being, and aging in colombia-study design and protocol. Curr. Gerontol. Geriatr. Res. 2016, 7910205. https://doi.org/10.1155/2016/7910205 (2016).
Sheik, J. & Yesavage, J. Geriatric Depression Scale: Recent Evidence and Development of a Shorter Version. Clinical Gerontology: A Guide to Assessment and Intervention 165–173 (The Hawthorne Press, 1986).
Alexandre Tda, S. et al. Gender differences in incidence and determinants of disability in activities of daily living among elderly individuals: SABE study. Arch. Gerontol. Geriatr. 55(2), 431–437. https://doi.org/10.1016/j.archger.2012.04.001 (2012).
Sainsbury, A., Seebass, G., Bansal, A. & Young, J. B. Reliability of the Barthel Index when used with older people. Age Ageing. 34(3), 228–232. https://doi.org/10.1093/ageing/afi063 (2005).
Lipschitz, D. A. Screening for nutritional status in the elderly. Prim. Care. 21(1), 55–67 (1994).
IPAQ scoring protocol—International Physical Activity Questionnaire (2016)
Angulo R, Díaz Y, Pardo R. Índice de Pobreza Multidimensional para Colombia. 2011. https://EconPapers.repec.org/RePEc:col:000118:009228. (Accessed 1 December 2020)
Departamento Administrativo Nacional de Estadística. Pobreza Monetaria y Multidimensional en Colombia 2018. https://www.dane.gov.co/index.php/estadisticas-por-tema/pobreza-y-condiciones-de-vida/pobreza-y-desigualdad/pobreza-monetaria-y-multidimensional-en-colombia-2018#pobreza-por-departamentos-2018. (Accessed 5 December 2020)
Ministerio de Salud y Protección Social. Análisis de Situación de Salud (ASIS) Colombia, 2017. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/ED/PSP/asis-nacional-2017.pdf. (Accessed 1 December 2020)
Alkire, S. & Santos, M. E. Measuring acute poverty in the developing world: Robustness and scope of the multidimensional poverty index. World Dev. 59, 251–274 (2014).
Merlo, J. et al. A brief conceptual tutorial of multilevel analysis in social epidemiology: Using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J. Epidemiol. Community Health. 60(4), 290–297. https://doi.org/10.1136/jech.2004.029454 (2006).
Pinilla-Roncancio, M. et al. Multidimensional poverty and disability: A case control study in India, Cameroon, and Guatemala. SSM Popul. Health. 11, 100591. https://doi.org/10.1016/j.ssmph.2020.100591 (2020).
Amaral, T. L. M. et al. Multimorbidity, depression and quality of life among elderly people assisted in the Family Health Strategy in Senador Guiomard, Acre, Brazil. Cien. Saude. Colet. 23(9), 3077–3084. https://doi.org/10.1590/1413-81232018239.22532016 (2018) (Multimorbidade, depressão e qualidade de vida em idosos atendidos pela Estratégia de Saúde da Família em Senador Guiomard, Acre, Brasil).
Olivares, D. E. et al. Risk factors for chronic diseases and multimorbidity in a primary care context of Central Argentina: A web-based interactive and cross-sectional study. Int. J. Environ. Res. Public Health. https://doi.org/10.3390/ijerph14030251 (2017).
Kushitor, M. K. & Boatemaa, S. The double burden of disease and the challenge of health access: Evidence from Access, Bottlenecks, Cost and Equity facility survey in Ghana. PLoS ONE 13(3), e0194677. https://doi.org/10.1371/journal.pone.0194677 (2018).
Zhao, Y. et al. Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: An analysis of population-based panel data. Lancet Glob. Health. 8(6), e840–e849. https://doi.org/10.1016/s2214-109x(20)30127-3 (2020).
Cuthbertson, C. C. et al. Socioeconomic status and access to care and the incidence of a heart failure diagnosis in the inpatient and outpatient settings. Ann. Epidemiol. 28(6), 350–355. https://doi.org/10.1016/j.annepidem.2018.04.003 (2018).
Kunna, R., San Sebastian, M. & Stewart Williams, J. Measurement and decomposition of socioeconomic inequality in single and multimorbidity in older adults in China and Ghana: Results from the WHO study on global AGEing and adult health (SAGE). Int. J. Equity Health. 16(1), 79. https://doi.org/10.1186/s12939-017-0578-y (2017).
Foguet-Boreu, Q. et al. Impact of multimorbidity: Acute morbidity, area of residency and use of health services across the life span in a region of south Europe. BMC Fam. Pract. 15, 55. https://doi.org/10.1186/1471-2296-15-55 (2014).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
S.M.B. and J.M.M. conceived the study and analyzed the data. S.M.B. wrote the first and successive drafts of the manuscript, J.M.M. and W.J.A.G. contributed to the writing of the manuscript. All authors critically revised the manuscript for important intellectual content and contributed to the interpretation of results. All authors have given final approval of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ballesteros, S.M., Moreno-Montoya, J., Grooten, W.J.A. et al. Socioeconomic variation of multimorbidity in Colombian older adults. Sci Rep 11, 22738 (2021). https://doi.org/10.1038/s41598-021-02219-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-02219-w
- Springer Nature Limited
This article is cited by
-
Association between polypharmacy and chronic kidney disease among community-dwelling older people: a longitudinal study in southern China
BMC Nephrology (2024)
-
Influence of internal migration on multimorbidity in the Brazilian longitudinal study of adult health (ELSA-Brasil)
Journal of Public Health (2024)