
Abstract
This study aimed to assess the role of 18F-fluorodeoxyglucose-positron emission tomography/computed tomography (18FDG-PET/CT) in the differential diagnosis of pericardial disease. The diagnosis is often troublesome because pericardial fluid analysis or biopsy does not always provide answers. 18FDG-PET/CT can visualize both inflammation and malignancy and offers a whole-body assessment. Patients who visited the Pericardial Disease Clinic of Samsung Medical Center with an 18FDG-PET/CT order code were extracted. Exclusion criteria were as follows: (1) the purpose of the differential diagnosis was not pericardial disease; (2) the patient had a known advanced-stage malignancy; (3) the patient already have confirmative diagnosis using a serology, pericardial effusion analysis or biopsy. The analysis included 107 patients. The most common final diagnosis was idiopathic (n = 46, 43.0%), followed by tuberculosis (n = 30, 28.0%) and neoplastic (n = 11, 10.3%). A maximum standardized uptake value (SUVmax) ≥ 5 typically indicates tuberculosis or neoplastic pericarditis except in just one case of autoimmune pericarditis); especially all of the SUVmax scores ≥ 10 had tuberculosis. The diagnostic yield of pericardial biopsy was very low (10.2%). Interestingly, all of the pericardium with an SUVmax < 4.4 had nondiagnostic results. In contrast, targeted biopsies based on 18FDG uptake demonstrated a higher diagnostic yield (38.7%) than pericardium. The sensitivity of 18FDG-PET/CT was 63.6%. The specificity was 71.9%. The positive predictive value was 20.6%. The negative predictive value 94.5%, and the accuracy was 71.0% for excluding malignancy based upon the FDG uptake patterns. It is possible to explore the differential diagnosis in some patients with difficult pericardiocentesis or pericardial biopsy in a noninvasive manner using on the SUVmax or uptake patterns. In addition, the biopsy strategy depending on 18FDG uptake is helpful to achieve biopsy more safely and with a higher yield. 18FDG-PET may enhance the diagnostic efficacy in patients with pericardial disease.
Similar content being viewed by others


Introduction
Pericardial diseases are relatively common in clinical practice and may have varying presentations either as isolated disease or as a manifestation of a systemic disorder1,2,3. The etiology of pericardial disease of various causes is not only limited to disease in the pericardium itself; a systemic approach during the differential diagnosis is therefore frequently required. The amount of pericardial effusion and hemodynamic impact can be easily assessed using echocardiography4; however, limited information exists regarding adjacent organs or the full range of the pericardium itself due to the limited echocardiographic window. It is also difficult to differentiate the properties of effusion by echocardiography alone. Therefore, a multimodal imaging approach has been suggested using computed tomography/magnetic resonance imaging (CT/MRI).
A pericardial fluid analysis is essential to characterize pericardial effusion; however, pericardiocentesis is limited based on its location and the amount of pericardial effusion. Pericardial tissue can be obtained through a surgical approach, but the information is frequently nondiagnostic, and the process itself can be technically challenging due to constriction or adhesions. The presence of an underlying disease that causes pericardial effusion determines the diagnosis and treatment of pericardial disease5. Therefore, noninvasive functional imaging in pericardial disease is helpful to discriminate the presence of inflammation or malignancy not only in the pericardium but also in other organs. As a result, 18F-fluorodeoxyglucose-positron emission tomography/computed tomography (18FDG-PET/CT) is a good candidate to assess pericardial disease, which includes inflammatory or malignant disease, in a single examination6. It has been reported that pericardial SUVmax predict the reversibility of transient constrictive pericarditis7. However, research into the clinical implications of 18FDG-PET/CT in pericardial disease is very limited.
In this study, we investigated the clinical implications of 18FDG-PET/CT in real-world clinics in patients with pericardial disease.
Results
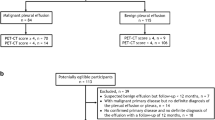
One hundred and nine patients were finally analyzed. The patient selection process is depicted in Fig. 1, including the process for excluding patients. Out of the total 109 patients, 42 (39.2%) had pericardial effusion at their initial presentation and underwent pericardiocentesis or pericardial biopsy before the 18FDG-PET/CT was performed, and the pericardial fluid or tissue analysis was nondiagnostic. Thirty-one patients (29.0%) had no or only minimal pericardial effusion with constrictive physiology or a thickened pericardium. The rest of the patients (n = 34, 31.8%) presented with a small amount of pericardial effusion or inadequate localization for pericardiocentesis.

The study population.
The patients’ general characteristics and past medical history are summarized in Table 1. The median age of the study population was 60.1 ± 15.4 years, and the male sex was dominant. Any underlying disease that could affect the pericardial disease was reviewed. The percentages of patients with a malignancy or tuberculosis were 23.4% and 15.0%, respectively; however, all of them had already been treated, and there was no evidence of a recent recurrence.
After an integrated diagnostic work-up and a follow-up period lasting more than 6 months, the final diagnosis was made by an attending physician (Table 2). Idiopathic pericarditis was the most common finding (43.0%), while tuberculosis accounted for 28.0% of cases, and 10.3% were neoplastic. Details of neoplastic pericarditis is as follows; mesothelioma (n = 3), angiosarcoma (n = 1), hemangioendothelioma (n = 1) and metastatic carcinoma (n = 6, from lung (n = 2), thymus, thyroid, stomach, breast). Less common causes included radiation, post-cardiac injury syndrome, parasitic infection, autoimmune pericarditis, and traumatic hemopericardium.
The pericardial SUVmax was analyzed according to the final diagnosis (Fig. 2). None of the idiopathic pericarditis cases showed a pericardial SUVmax value > 5. Tuberculosis had the highest variation in SUVmax scores. Malignancy had a higher median pericardial SUVmax value than idiopathic pericarditis, but none of the scores were > 10.

A scatter plot of the pericardial SUVmax scores according to the final diagnosis. [Central illustration].
Pericardial biopsy was finally performed in 49 patients, but the diagnostic yield was very low (10.2%) (Fig. 3A left). Pericardial SUVmax in nondiagnostic vs. diagnostic pericardial biopsy is demonstrated in in Fig. 3B. In 31 patients, an additional targeted biopsy based upon the 18FDG-PET/CT findings was performed at 46 biopsy sites other than the pericardium. These sites demonstrated a higher diagnostic yield (38.7%) than the pericardium (Fig. 3A right). The most common targeted biopsy site was a mediastinal mass or a lymph node (39.1%), followed by the supraclavicular lymph nodes and the cervical lymph nodes (Table 3).

(A) A scatter plot of the pericardial SUVmax scores with the diagnostic and nondiagnostic results of the pericardial biopsy. (B) The number of patients who underwent total pericardial biopsy and diagnostic pericardial biopsy/total targeted biopsy (pericardium excluded) and diagnostic targeted biopsy.
Table 4 shows the presumptive diagnosis based upon the 18FDG-PET/CT and the distribution of final diagnoses. Among the cases that suggested malignancy, only 3 of 7 had malignant disease. Four of 73 cases reported as benign were finally diagnosed as malignancies. On the basis of uptake pattern, the negative predictive value of 18FDG-PET/CT to exclude malignancy in pericardial disease was more than 94.5% (69/73).
Difference in the shape and properties of 18FDG accumulation between tuberculous pericarditis and neoplastic disease was also analyzed. Images were categorized as no uptake, focal uptake, diffuse homogeneous uptake, diffuse heterogenous uptake and there was no significant difference between groups (Table 5).
Discussion
The role of 18FDG-PET/CT in pericardial disease is not clearly established, although the 2015 European Society of Cardiology guidelines8 recommend 18FDG-PET/CT in special clinical situations with probable autoimmune disease (large vessel arteritis and sarcoidosis) or neoplasms.
18FDG-PET/CT is indicated to depict the metabolic activity of pericardial disease. In cases with a diagnosed solid cancer or lymphoma, the pericardial uptake of the 18FDG tracer is indicative of malignant pericardial involvement, thus providing essential information on the staging and assessment of the patient’s therapeutic response9. The uptake is usually intense and is often associated with a focal soft tissue mass10. In particular, tuberculous pericarditis was reported to yield higher 18FDG uptakes than idiopathic forms in a small study with only five cases of tuberculosis11. However, the role of 18FDG-PET/CT in the differential diagnosis of cases that initially presented as pericardial disease remains challenging9.
In this study, 18FDG-PET/CT was performed as a second-line diagnostic imaging study for the further evaluation of pericardial disease after pericardial effusion analysis or other imaging study (echocardiography and/or CT). Although the diagnostic yield to differentiate pericardial disease using 18FDG-PET alone was not perfect, it was helpful in clinical practice as follows: First, 18FDG-PET/CT aided in differentiating pericardial tuberculosis. Annual tuberculosis incidence (per 100,000 population) of East Asian Country including China and South Korea are still 25–99 per 100,000 population12, therefore tuberculous pericarditis is still important cause of pericarditis. Furthermore, clinical presentation of tuberculous pericarditis in immunocompetent hosts is various clinical presentation from asymptomatic pericardial effusion to acute pericarditis or constrictive pericarditis, differential diagnosis for tuberculous pericarditis is always critical because of high rate of complication when untreated13.
All cases with a pericardial SUVmax value that was > 9 had tuberculous pericarditis. Furthermore, none of the tuberculous pericarditis cases were interpreted as suggestive of malignancy. Therefore, if the pericardial SUVmax is very high and the 18FDG uptake pattern does not suggest a typical malignancy, the possibility of tuberculous pericarditis will be increased. However, tuberculous pericarditis may also present with a low pericardial SUVmax value, so a low SUVmax does not rule out the diagnosis of tuberculous pericarditis. This trend can be explained by the unique nature of tuberculous pericarditis, which has various clinical presentations in immunocompetent patients13 depending on whether they are in the subacute or chronic inflammatory stage. Second, 18FDG-PET/CT was helpful to determine the best biopsy site for further evaluations. The diagnostic yield of pericardial biopsy is low and frequently non-diagnostic (the most common finding is chronic inflammation) in clinical practice14,15, and our data revealed similar outcomes. Extracardiac tissue biopsy in locations other than the pericardium is often helpful in the diagnosis. However, all surgical procedures carry potential risks, and multiple non-diagnostic findings can be found upon CT imaging without PET images. Extracardiac biopsy targeted by 18FDG-PET/CT findings demonstrated a better diagnostic yield than pericardial biopsy and was critical in deciding the best way to manage the patients’ disease. For example, one patient who presented with a fever and pericarditis with a thickened pericardium had multiple lymph node uptake on 18FDG-PET/CT. A right supraclavicular lymph node biopsy was easily assessible with local anesthesia. The pathology report of that lymph node indicated caseous necrosis, so the patient was treated for tuberculosis, and the pericardial biopsy was canceled (Fig. 4). In addition, pericardial biopsy results in patients with a low pericardial SUVmax < 4 were reported as non-specific inflammatory findings. These results suggest that 18FDG-PET can be helpful to avoid unnecessary pericardial biopsies with a high specificity.

18FDG-PET image of a 21-year-old male patient. Tuberculous pericarditis was diagnosed via biopsy right supraclavicular lymph node with increased FDG uptake (black arrow), instead of initially planned pericardial biopsy.
The limitations of 18FDG-PET/CT have been clearly demonstrated in previous studies9 and were found to be similar in our study. Although Shao et al. reported that the SUVmax could distinguish malignancies from benign tissue16, their study only included patients with tumorous conditions, which makes it a very different study from our data that included patients presenting with pericardial disease of an unknown etiology. In our study, both malignant- and benign-appearing tissues had a large amount of overlap both in the pericardial SUVmax score and the tissue uptake patterns. Various pericardial diseases have a similar area of pericardial SUVmax scores, especially from 1.0–5.0, which is non-specific (Fig. 2). The tissue uptake pattern was also confusing, especially in malignancies, which have no diagnostic value for differentiation. Moreover, 18FDG-PET/CT is expensive and carries a potential amount of radiation exposure when used routinely for pericardial disease. Therefore, our study results should be interpreted with caution and only carefully applied to patients who have trouble with conventional, noninvasive diagnostic methods and who require invasive procedures, such as pericardial or other tissue biopsies.
This study contains the largest dataset of 18FDG-PET used in the differential diagnosis of pericardial disease in real clinical practice to date. Although this was a retrospective observational study, it suggests that the pericardial SUVmax obtained using 18FDG-PET could be helpful to differentiate a high probability of pericardial tuberculosis and also to select a biopsy site that will produce a better yield when compared to conventional approaches, including echocardiography and CT alone. Pericardial disease is commonly comorbid with systemic disease and is not limited to the pericardium. One unique aspect of 18FDG-PET as a functional imaging modality is its use in the localization of multi-organ involvement in systemic disease.
Conclusion
18FDG-PET is a noninvasive imaging tool that can visualize the pericardium and any affected organs during a single examination. In patients who require further evaluations, such as a pericardial biopsy, the 18FDG-PET can be helpful in selecting the biopsy site with the best diagnostic yield. Very high pericardial SUVmax values are helpful when differentiating tuberculous pericarditis from other diseases; however, malignancy cannot be excluded when the pericardial SUVmax is < 9. Therefore, 18FDG-PET can be helpful to diagnose the cause of pericardial disease in selected patients.
Methods
Study population
Patients who visited our pericardial disease clinic from March 2009 to February 2019 were reviewed for inclusion in this study. We retrieved the records of patients who underwent 18FDG-PET/CT from our electrical record system database. The following exclusion criteria were applied for the recruited population; (1) the purpose of 18FDG-PET/CT was to investigate another disease; (2) a definitive diagnosis was confirmed before 18FDG-PET/CT; or (3) the patient already have confirmative diagnosis using a serology, pericardial effusion analysis or biopsy.
All methods were carried out in accordance with relevant guidelines and regulations. The Institutional Review Board of Samsung Medical Center approved the study protocol, and the requirement for written informed consent was waived.
Data collection
Age, sex, height, body weight, body mass index, and past medical history (including hypertension, diabetes, dyslipidemia, chronic kidney disease, cardiocerebrovascular accident, cardiac procedures, open heart surgery, a previous history of malignancy, previous radiation therapy, and a history of tuberculosis) were reviewed using electronic medical records. Chronic kidney disease was defined when a patient was on dialysis or the serum creatinine level remained ≥ 2.0 mg/dl. Cardiocerebrovascular accident was defined as acute coronary syndrome, myocardial infarction, or stroke. Cardiac procedures included percutaneous coronary interventions, radiofrequency catheter ablation, intracardiac device implantation (such as implantable cardioverter-defibrillator, pacemaker, or cardiac resynchronization therapy), and pericardiocentesis.
Imaging acquisition of 18FDG PET/CT
Image acquisition was performed as previously described7. To decrease physiological uptake in the myocardium, preparation of the patients included fasting for at least 12 h before and a low-carbohydrate diet for more than 24 h before the PET/CT examination. Only oral hydration with glucose-free water was allowed during the fasting period. After confirmation of a normal blood glucose level in the peripheral blood (< 150 mg/dl), the patients received an intravenous injection of 18FDG (5 MBq/kg) and then rested for approximately 60 min before undergoing scanning by two dedicated PET/CT scanners (Discovery STe or Discovery LS, GE Healthcare, Milwaukee, WI, USA). Immediately after the non-contrast enhanced CT scan (140 keV, 30–170 mAs with AutomA mode, and section width = 3.75 mm for STe; 140 keV, 40–120 mAs adjusted to body weight and section width = 5 mm for LS), an emission PET scan was obtained from the thigh to the head at baseline or for the thorax after steroid therapy with a 2.5-min acquisition time per frame using the three-dimensional mode for the STe and a 4-min acquisition time per frame in two-dimensional mode for the LS. Attenuation-corrected PET images (voxel size = 4.3 × 4.3 × 3.9 mm for the Discovery LS, 3.9 × 3.9 × 3.3 mm for the STe) were reconstructed using CT data and ordered-subset expectation maximization algorithms (20 subsets and 2 iterations for the STe; 28 subsets and 2 iterations for the LS). The standardized uptake values (SUVs) were derived from the injected dose of 18FDG and the patient’s body weight. Commercial software (Advantage Workstation version 4.4, GE Healthcare) was used to accurately coregister the separate CT and PET scan data and to measure the maximum SUV (SUVmax) value of the pericardium.
Clinical follow-up data analysis
Clinical follow-up data were categorized as follows: (1) final diagnosis six months after the initial presentation; (2) how the result of 18FDG-PET/CT changed the clinical course; (3) The correlation between the 18FDG-PET/CT results and the final diagnosis. In cases that also underwent a pericardial biopsy, the correlation between the pericardial SUVmax value and the diagnostic yield of the pericardial biopsy was also determined. Diagnostic results were defined as when a definite diagnosis was able be made from the biopsy results. For example, granulomatous inflammation with caseous necrosis, positive for AFB stain, culture or TB-PCR for tuberculous pericarditis, and malignant cells confirmed regardless of the origin in neoplastic pericarditis. In addition, we collected information on biopsy sites based on an increased 18FDG uptake in places other than the pericardium and attempted to determine which site was most frequent and what the yield of a targeted biopsy was.
The PET interpretation of the presence of malignant pericardial lesions was carried out according to the following criteria; (1) probably benign: low or no 18FDG uptake in the pericardium without any other organ uptake suspicious for malignancy; (2) equivocal: low or no 18FDG uptake in the pericardium with other organ uptake suspicious for malignancy or a previous cancer history; and (3) probably malignant: a high 18FDG uptake in the pericardium with other organ uptake suspicious for malignancy.
Statistical analysis
Categorical variables are presented as the absolute number and the percentage of relative frequencies. Continuous variables are presented as the average and standard deviation (normal distribution) or the median and interquartile range (non-normal distribution) based on normality testing. The Statistical Package for the Social Sciences (SPSS), version 24 (IBM, Armonk, NY, USA) was used for the statistical analysis.
Abbreviations
- AFB:
-
Acid-fasting bacilli
- BMI:
-
Body mass index
- CMR:
-
Cardiovascular magnetic resonance imaging
- CT:
-
Computed tomography
- 18FDG:
-
[18F]2-deoxy-2-fluoro-d glucose
- PET:
-
Positron emission tomography
- SUV:
-
Standardized uptake value
- SUVmax :
-
Maximum standardized uptake value
- TB-PCR:
-
Mycobacterium tuberculosis-polymerase chain reaction
References
Maisch, B. et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur. Heart J. 25, 587–610. https://doi.org/10.1016/j.ehj.2004.02.002 (2004).
Seferovic, P. M. et al. Pericardial syndromes: An update after the ESC guidelines 2004. Heart Fail. Rev. 18, 255–266. https://doi.org/10.1007/s10741-012-9335-x (2013).
Khandaker, M. H. et al. Pericardial disease: Diagnosis and management. Mayo Clin. Proc. 85, 572–593. https://doi.org/10.4065/mcp.2010.0046 (2010).
Perez-Casares, A., Cesar, S., Brunet-Garcia, L. & Sanchez-de-Toledo, J. Echocardiographic evaluation of pericardial effusion and cardiac tamponade. Front. Pediatr. 5, 79. https://doi.org/10.3389/fped.2017.00079 (2017).
Permanyer-Miralda, G. Acute pericardial disease: Approach to the aetiologic diagnosis. Heart 90, 252–254. https://doi.org/10.1136/hrt.2003.024802 (2004).
Kircher, M. & Lapa, C. Novel noninvasive nuclear medicine imaging techniques for cardiac inflammation. Curr. Cardiovasc. Imaging Rep. 10, 6. https://doi.org/10.1007/s12410-017-9400-x (2017).
Chang, S. A. et al. [(18)F]Fluorodeoxyglucose PET/CT predicts response to steroid therapy in constrictive pericarditis. J. Am. Coll. Cardiol. 69, 750–752. https://doi.org/10.1016/j.jacc.2016.11.059 (2017).
Adler, Y. et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 36, 2921–2964. https://doi.org/10.1093/eurheartj/ehv318 (2015).
Lobert, P. et al. Spectrum of physiological and pathological cardiac and pericardial uptake of FDG in oncology PET-CT. Clin. Radiol. 68, e59-71. https://doi.org/10.1016/j.crad.2012.09.007 (2013).
James, O. G., Christensen, J. D., Wong, T. Z., Borges-Neto, S. & Koweek, L. M. Utility of FDG PET/CT in inflammatory cardiovascular disease. Radiographics 31, 1271–1286. https://doi.org/10.1148/rg.315105222 (2011).
Dong, A. et al. (18)F-FDG PET/CT in differentiating acute tuberculous from idiopathic pericarditis: Preliminary study. Clin. Nucl. Med. 38, e160-165. https://doi.org/10.1097/RLU.0b013e31827a2537 (2013).
MacNeil, A., Glaziou, P., Sismanidis, C., Maloney, S. & Floyd, K. Global epidemiology of tuberculosis and progress toward achieving global targets—2017. MMWR. Morbidity and Mortality Weekly Report 68(11), 263–266. https://www.cdc.gov/mmwr/volumes/68/wr/mm6811a3.htm.
Kim, M. S. et al. The clinical course of tuberculous pericarditis in immunocompetent hosts based on serial echocardiography. Korean Circ. J. 50, 599–609. https://doi.org/10.4070/kcj.2019.0317 (2020).
Fernandes, F., Ianni, B. M., Arteaga, E., Benvenutti, L. & Mady, C. Value of pericardial biopsy in the etiologic diagnosis of pericardial diseases. Arq. Braz. Cardiol. 70, 393–395. https://doi.org/10.1590/s0066-782x1998000600003 (1998).
Maisch, B. et al. Intrapericardial treatment of inflammatory and neoplastic pericarditis guided by pericardioscopy and epicardial biopsy–results from a pilot study. Clin. Cardiol. 22, I17-22. https://doi.org/10.1002/clc.4960221307 (1999).
Shao, D., Wang, S. X., Liang, C. H. & Gao, Q. Differentiation of malignant from benign heart and pericardial lesions using positron emission tomography and computed tomography. J. Nucl. Cardiol. 18, 668–677. https://doi.org/10.1007/s12350-011-9398-4 (2011).
Author information
Authors and Affiliations
Contributions
C.W.H. and S.A.C. wrote the main manuscript. H.K.Y. and J.Y.C. contributed to data analysis and concept of design. S.A.C. and J.Y.C. approved the final manuscript. All authors contributed to data collection and analysis, and reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hyeon, C.W., Yi, H.K., Kim, E.K. et al. The role of 18F-fluorodeoxyglucose-positron emission tomography/computed tomography in the differential diagnosis of pericardial disease. Sci Rep 10, 21524 (2020). https://doi.org/10.1038/s41598-020-78581-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-78581-y
- Springer Nature Limited
This article is cited by
-
Autoimmune Pericarditis: Multimodality Imaging
Current Cardiology Reports (2022)
-
KSNM60 in Cardiology: Regrowth After a Long Pause
Nuclear Medicine and Molecular Imaging (2021)