
Abstract
The contribution of energised environmental debris to injury patterns of the blast casualty is not known. The extent to which personal protective equipment (PPE) limits the injuries sustained by energised environmental debris following an explosive event is also not known. In this study, a cadaveric model exposed to a gas-gun mediated sand blast was utilised which reproduced soft-tissue injuries representative of those seen clinically following blast. Mean sand velocity across experiments was 506 ± 80 ms−1. Cadaveric samples wearing standard-issue PPE were shown to have a reduced injury severity to sand blast compared to control: a statistically significant reduction was seen in the total surface area (143 mm2 vs. 658 mm2, p = 0.004) and depth of injuries (0 vs. 23 deep injuries, odds ratio = 0.0074, 95% confidence intervals 0.0004–0.1379). This study is the first to recreate wounds from propelled sand in a human cadaveric model. These findings implicate environmental debris, such as sand ejected from a blast event, as a critical mechanism of injury in the blast casualty. Tier 1 pelvic PPE was shown to reduce markedly the severity of injury. This injury mechanism should be a key focus of future research and mitigation strategies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Blast injury was the leading cause of morbidity and mortality from recent conflicts in Iraq and Afghanistan, in which the improvised explosive device (IED) was the weapon of choice [1]. These weapons generally originate from the ground, and are often buried beneath the soil, resulting in extremity wounding, particularly of the lower limbs. The burden of such injuries and subsequent management is substantial [2,3,4].
Following detonation of an anti-personnel IED, the most common mechanism of wounding is penetrating injury from energised fragments propelled by the blast [5, 6]. These energised fragments may be from the explosive device itself, or objects from the surrounding environment. Energised environmental fragments and debris are known to travel at speeds of up to 900 ms−1 following blast, before decelerating to 600 ms−1 or less prior to impacting casualties depending upon their distance from the device [7, 8]. Energised fragments have been identified as a significant contributor to morbidity and mortality; however, the contribution of energised environmental debris, such as soil or sand, to injury is not known [5].
Injuries sustained through explosive mechanisms have extensive contamination that is driven deep between tissue planes; this deep contamination subsequently require extensive debridement. Large, complex wounds as seen in the military blast patient contain numerous pockets into which foreign contaminated material is forced [9]. Contamination with environmental debris is known to increase the risk of bacterial and invasive fungal infections (IFIs), both of which are a cause of morbidity and late mortality [10, 11]. To manage this contamination requires a series of operations to remove the foreign material, which may worsen the level of final amputation [12]. Foreign material found within blast wounds consist of ingrained mud, dirt, and sand as well as less obvious contaminants [9]. Wounds with heavy environmental contamination from mud, dirt, and sand have been associated with soft tissue infection of both environmental bacterial organisms in addition to invasive fungi [13]. The delayed morbidity and mortality of invasive bacterial and fungal infections are significant, and can result in high-level amputation or death [10, 11].
In order to mitigate the increasing rate of soft tissue injury to the pelvis and perineum, pelvic personal protective equipment (PPE) was first fielded for UK service personnel in 2010 [14]. This was provided in three hierarchical tiers, designed to be worn in conjunction with one another in response to the perceived threat. Tier 1 is an under-layer to be worn beneath issue combat trousers, covering from waist to knees. It is constructed from a jersey-type material with two layers of high-performance knitted silk protection stitched to the outside to protect vulnerable areas [14].
Evidence of injury reduction from Tier 1 PPE from fragmentation wounds has been observed clinically as a difference in the pattern of injuries suffered by personnel wearing Tier 1 PPE and those not [15]. These data suggest benefit from the use of Tier 1 PPE; however, no evaluation study to date has confirmed its efficacy in mitigating the injuries sustained by energised sand or soil. Similarly, no laboratory study has previously demonstrated the mechanism of injury of energised sand or soil.
Accordingly, the aims of this study were (1) to replicate impact and injury from propelled sand as occurs following blast in a human cadaveric model, utilising a gas-gun system, and (2) to investigate the effect of Tier 1 pelvic PPE on mitigating the injury patterns observed. Our hypothesis was that sand ejecta would contribute to the soft tissue injury seen in dismounted blast and that Tier 1 pelvic PPE would mitigate the injury patterns observed.
Materials and Methods
The tests performed used a setup for investigating injury from sand, utilising a gas-gun system modified to deliver sandy gravel aggregate at high velocities. The experimental design and procedures were carried out in compliance with the Human Tissue Act 2004. Ethical approval was granted from the local regional ethics committee at the Imperial College Healthcare Tissue Bank (ethical approval number: 17/WA/0161). Experiments were carried out using twelve male human cadaveric thigh samples with no prior relevant injury or pathology (median age 38 years, range 36–51 years). Samples were fresh frozen at − 20 °C and thawed at room temperature (21 ± 2 °C) for 24 h prior to testing.
Sand size and properties were chosen based upon NATO unclassified AEP-55 recommendations for typical sandy gravel soil granulometry [16]. A sandy gravel aggregate size range was subsequently chosen to fall as closely as possible to the median value (2 mm, range 0.09–38 mm) of the ideally distributed particle sizes [16]. This consisted of sandy gravel of which 100% passed a 1–2-mm sieve, with any sand subsequently passing a 1-mm sieve removed (the sand size utilised in experiments therefore ranged from 1 to 2 mm). The sand was housed within a 11-g hollow polycarbonate sabot weighed prior to, and following, loading it with sand.
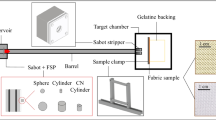
The sabot-sand unit was subsequently loaded into the firing chamber of a double-reservoir gas-gun system. This system utilised a 2-L reservoir charged with air or helium and a Mylar® diaphragm firing mechanism to accelerate the sabot-sand unit down a 3-m-long, 32-mm-bore barrel [17]. To accelerate the sabot-sand unit to the desired velocity, the reservoir section of the gas gun was charged to a predetermined firing pressure prior to release. After release, the sabot-sand unit accelerates down the barrel to exit into the target chamber, where the sabot is separated from the sand by a stainless-steel sabot-stripper. The sabot is halted at this point, whilst the sand continues to travel towards the cadaveric sample at the intended terminal velocity. In order to simulate the distribution and spread of sand ejecta as occurs following blast, two interconnecting fenestrated steel fences, separated by 10 mm and offset to one another by 50% of the diameter of each fenestration, were placed distal to the gas-gun outlet and proximal to the mount (Fig. 1a). Offsetting of the fenestrated steel fences changed the initial stream of sand delivered by the gas gun into multiple streams of differing trajectories which subsequently dispersed into a widely distributed spread of sand (Fig. 1b); this setup achieved blast propagation in three dimensions and acceleration of debris and soil ejecta in all directions, which can be considered a realistic simulation of the event.

a Aerial view of experimental set-up showing cadaveric thigh with standard-issue combat trousers (represented by model) positioned within target chamber (A: proximal thigh, B: medial thigh, C: lateral thigh, D: distal thigh, E: dispersion fence). b Photographs showing the delivery of sand without (top) and with (bottom) the use of fenestrated fences. c Series of high-speed video images illustrating the velocity estimation of the sand cloud based on four unique points of the sand spread (F: front (red), FC: front-centre (blue), C: centre (green), CB: centre-back (yellow))
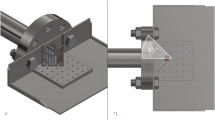
The speed of the sand particles at the point of impact with the sample was estimated using high-speed photography (Phantom VEO710L, AMETEK, USA) at 68,000 fps. An average velocity for the sand cloud as a whole was determined based upon identifying and tracking four unique points spread across the distributed sand. These points varied in velocity and were chosen from the front, front-centre, centre, and centre-back of the peripheries of the sand spread (Fig. 1c). Cadaveric samples were divided into one of two groups: either wearing (1) UK Military Tier 1 pelvic protection [18] (knitted silk of 490 g/m2 areal density) and standard-issue combat trousers or (2) standard-issue combat trousers only (control group). For each individual test, a cadaveric thigh was secured in position within the target chamber. The thigh was placed in a neutral resting position with an abduction angle of 30° from the midline (Fig. 2). The Tier 1 pelvic protection was worn as a whole on the cadaveric thigh, with the sand blast directed to impact with the two layers of high-performance knitted silk protection (Fig. 3).

Experimental setup showing cadaveric thigh with standard-issue combat trousers prior to (top) and during (bottom) impact with sand debris. A: proximal thigh, B: medial thigh, C: lateral thigh, D: distal thigh, E: dispersion fence, F: propelled sand debris at point of impact

Tier 1 pelvic personal protective equipment worn on cadaveric thigh; post-impact delivered to region of two-layer high-performance knitted silk protection
Following impact with the sand, samples were removed from the target chamber and taken for subsequent photography and dissection. A separate photograph was taken of each individual injury, with adjacent ruler, and the film plane of the camera parallel to the injury to avoid parallax errors. Recorded injury patterns included (1) number of injuries sustained, (2) surface area of injuries sustained (surface area per injury and total injured surface area), and (3) maximal anatomical depth of injury sustained (superficial/subcutaneous only, or deep to the subcutaneous tissues/subfascial).
Image Processing and Statistical Analysis
Photographed images were subsequently assessed with image processing software to calculate the surface area of injuries sustained. ImageJ was used for image processing calculations (National Institutes of Health, USA). Image scale was set, followed by tracing the outer edges of the zone of injury for each individual injury sustained to calculate the total surface area.
IBM SPSS was used for statistical analysis (version 26, IBM, USA). The Mann–Whitney test was used to assess significant differences in non-parametric data between groups, including number of injuries sustained and surface area of injuries. Cross-tabulation with Pearson χ2 test was used to assess significant differences in categorical variables between groups, including depth of penetration (subcutaneous only vs. deep (subfascial)).
Results
Impact with sand resulted in soft tissue injuries to all samples. A total of fifty-one experimentally derived injuries were produced from 12 thigh samples. Mean sand mass delivered was 8.9 g ± 0.4 g with a mean velocity of 506 ± 80 ms−1. Tier 1 pelvic PPE markedly reduced the severity of injury seen vs. control: wounds deep to the subcutaneous tissues were eliminated (0 vs. 23, p < 0.001) and a reduction in the total surface area of injuries was seen (median 143 mm2 vs. 658 mm2, p = 0.004). No significant difference was seen between groups in the number of injuries sustained per sample (median 3, range 2–5, vs. median 5, range 3–6, p = 0.051). As detailed in Table 1, a significant reduction was seen in the total surface area of injuries (median 143 mm2, range 115–230 mm2, vs. median 658 mm2, range 529–1319 mm2, p = 0.004) and depth of injuries: all penetrating injuries sustained within the Tier 1 protection group remained superficial whilst the control group sustained the majority (77%) of injuries deep to the underlying fascial layers (0 vs. 23, p < 0.001). Figure 4 displays the damage sustained by standard-issue combat trousers and silk PPE following impact. Figure 5 shows injuries more substantial in volume and depth as sustained in the control group, whilst Fig. 6 demonstrates the substantially reduced injuries seen in the PPE group. No samples within the Tier 1 protection group sustained a penetrating injury from sand ejecta deep to the subcutaneous tissues involving the underlying fascial and muscular layers (odds ratio = 0.0074, 95% confidence intervals 0.0004–0.1379).

Exemplar damage sustained by standard-issue combat trousers (left) and PPE (right) following impact with sand debris

Exemplar wounds sustained by control group following impact with sand debris

Exemplar wounds sustained by PPE group following impact sand debris
Discussion
This study is the first to recreate penetrating injury from propelled sand in a human cadaveric model as a simulacrum for the mineral component of soil ejecta from a blast event. Similarly, this study is the first laboratory study to quantify the severity of penetrating injuries from energised environmental debris in the thigh area and confirm the efficacy of Tier 1 PPE in potentially mitigating these injuries.
Tier 1 pelvic PPE was shown to reduce markedly the severity of injuries in the cadaveric model as quantified by the reducing in total surface area of injuries, and depth of penetration. These findings highlight the importance of Tier 1 PPE use in any environment in which blast injury to the limbs may occur. Our findings are in keeping with clinical literature examining the protective benefits of Tier 1 PPE. Breeze et al. reported that from 174 casualties attending a role 3 hospital in Afghanistan, those wearing Tier 1 pelvic PPE were significantly less likely (odds ratio = 0.1049) to sustain a penetrating wound from a blast event to the pelvis than those unprotected [15]. This is consistent with this laboratory study where no samples within the Tier 1 protection group sustained a penetrating injury from sand ejecta deep to the subcutaneous tissues, involving the underlying fascial and muscular layers (odds ratio = 0.0074, 95% confidence intervals 0.0004–0.1379). In addition, the total injured superficial surface area was 4.6 times smaller (143 mm2 vs. 658 mm2, p = 0.004) in the protection group.
To the best of our knowledge, no previous study has quantified penetrating injury to the thigh from energised environmental debris or assessed the protective benefit provided from Tier 1 PPE. A previous study has examined the mitigation effects of ballistic protective fabric, similar to the properties of Tier 2 PPE, to sand substrate following a controlled explosion [19]. As sand velocity or other injurious variables were not described in this study, there is insufficient information with which to compare our methodologies or findings.
Contamination following blast is extensive, as dirt and other debris are propelled along tissue planes; seeding of environmental debris deep to the subcutaneous tissues results in more extensive contamination than superficial wounds, with infection and delayed amputation frequent [5, 20]. Bacterial and invasive fungal infections following blast can result in delayed amputation or mortality [10, 11]. The findings of the present study show Tier 1 PPE to reduce the severity of injury sustained from impact from environmental debris propelled by blast; this suggests a reduced probability of infection where Tier 1 PPE is worn, through a reduction in wounds deep to the subcutaneous tissues with decreased soft tissue disruption and deep seeding of environmental contaminants.
A limitation of this study is the choice of sand. The sand type and size was based upon recommended values from NATO/PfP AEP-55 for optimal testing conditions of a surrogate TNT mine, buried in water-saturated sandy gravel, for testing blast from anti-vehicle mines [16]. It is not known whether this choice is representative of current threats and our recommendation would be that representative debris is identified before repeating the tests presented here. Furthermore, inherent limitations are associated with a cadaveric study; these include over or underestimating the effect size, and assumptions made with inferring a delayed infection risk. A non-cadaveric controlled clinical study, however, is not ethically feasible. A previous observational study has shown benefit of Tier 1 PPE vs. no protection, whilst the wearing of Tier 1 PPE has been adopted for routine use [14, 15]. Future clinical studies should include comparing current Tier 1 PPE to full under trouser PPE leggings, to assess the rates of wound infection, delayed amputation, and mortality.
This study is the first to recreate penetrating injury from propelled sand in a cadaveric model. It described a mechanism of reproducing sand blast in a laboratory setting utilising a pressurised gas-gun system. Tier 1 silk pelvic protection was shown to reduce markedly two parameters associated with severity of injury: wounds deep to the subcutaneous tissues were eliminated (0 vs. 23, p < 0.001) and a reduction in the total superficial surface area of injuries was seen (143 mm2 vs. 658 mm2, p = 0.004). In turn, this would be expected to reduce the probability of infection, through decreased soft tissue disruption and deep seeding of environmental contaminants. These findings implicate environmental debris such as sand ejected from a blast event to be a critical mechanism of injury in the blast casualty, and this injury mechanism should be a key focus of future research and mitigation strategies.
References
Russell R, Hunt N, Delaney R (2014) The Mortality Peer Review Panel: a report on the deaths on operations of UK Service personnel 2002–2013. J R Army Med Corps 160:150–154
Edwards DS, McMenemy L, Stapley SA, Patel HDL, Clasper JC (2016) 40 years of terrorist bombings—a meta-analysis of the casualty and injury profile. Injury 47:646–652
Owens BD, Kragh JF, Macaitis J, Svoboda SJ, Wenke JC (2007) Characterization of extremity wounds in operation Iraqi freedom and operation enduring freedom. J Orthop Trauma 21:254–257
Griffiths D, Clasper J (2006) (iii) Military limb injuries/ballistic fractures. Curr Orthop 20:346–353
Covey DC, Ficke J (2016) Blast and fragment injuries of the musculoskeletal system. Orthop Disasters Orthop Inj Nat Disasters Mass Casualty Events 269–280. https://doi.org/10.1007/978-3-662-48950-5_25
Edwards DS. Clasper J (2016) Blast injury mechanism. in Blast injury science and engineering 87–104 (Springer International Publishin). https://doi.org/10.1007/978-3-319-21867-0_6
Tremblay J, Bergeron D, Gonzalez R. (1998) KTA1–29: Protection of soft-skinned vehicle occupants from landmine effects. In: Program TTCP, editor. Val-Belair, Canada Def Res Establ Valcartier, Quebec, Canada
Bowyer GW (1996) Management of small fragment wounds: experience from the Afghan border. J Trauma Inj Infect Crit Care 40:170S-172S
Taylor C, Hettiaratchy S, Jeffery SL, Evriviades D, Kay A (2009) Contemporary approaches to definitive extremity reconstruction of military wounds. Artic J R Army Med Corps. https://doi.org/10.1136/jramc-155-04-12
Brown KV, Murray CK, Clasper JC (2010) Infectious complications of combat-related mangled extremity injuries in the British military. J Trauma 69:S109–S115
Rodriguez CJ et al (2014) Risk factors associated with invasive fungal infections in combat trauma. Surg Infect (Larchmt) 15:521–526
Clasper J, Ramasamy A (2013) Traumatic amputations. Br J Pain 7:67–73
Evriviades D et al (2011) Shaping the military wound: issues surrounding the reconstruction of injured servicemen at the Royal Centre for Defence Medicine. Philos Trans R Soc B Biol Sci 366:219–230
Lewis EA, Pigott MA, Randall A, Hepper AE The development and introduction of ballistic protection of the external genitalia and perineum. https://doi.org/10.1136/jramc-2013-000026
Breeze J, Allanson-Bailey LS, Hepper AE, Midwinter MJ (2015) Demonstrating the effectiveness of body armour: a pilot prospective computerised surface wound mapping trial performed at the role 3 hospital in Afghanistan. J R Army Med Corps 161:36–41
NATO/PfP Unclassified (2006) Procedures for evaluating the protection level of logistic and light armoured vehicles volume 2 for mine threat. AEP-55 2, Annex C
Nguyen TTN, Tear GR, Masouros SD, Proud WG (2018) Fragment penetrating injury to long bones. AIP Conf Proc 1979:312–321
Lewis EA, Pigott MA, Randall A, Hepper AE (2013) The development and introduction of ballistic protection of the external genitalia and perineum. J R Army Med Corps 159:i15–i17
Saunders C, Carr D (2018) Towards developing a test method for military pelvic protection. J Text Inst 109:1374–1380
Khatod M et al (2003) Outcomes in open tibia fractures: relationship between delay in treatment and infection. J Trauma 55:949–954
Acknowledgements
This study was conducted in the Royal British Legion Centre for Blast Injury Studies. The authors would like to thank the Royal British Legion for their support. Tissue samples were provided by the Imperial College Healthcare NHS Trust Tissue Bank (ICHTB). Other investigators may have received samples from these same tissues.
Funding
The authors received financial support from the Royal British Legion. The research was supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Imperial College Healthcare NHS Trust and Imperial College London.
All data generated or analysed during this study are included in this published article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rankin, I.A., Nguyen, TT.N., McMenemy, L. et al. Protective Clothing Reduces Lower Limb Injury Severity Against Propelled Sand Debris in a Laboratory Setting. Hum Factors Mech Eng Def Saf 6, 12 (2022). https://doi.org/10.1007/s41314-022-00050-3
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41314-022-00050-3