
Abstract
Objective
The study analyses the performances of FRAX algorithm and quantitative ultrasound (QUS) tool in relationship to the dual-energy X-ray absorptiometry (DXA) categorization to identify patients at risk of osteoporosis during menopause and to reach new thresholds for recommending the first DXA examination.
Design
Retrospective cohort study.
Patients and measurements
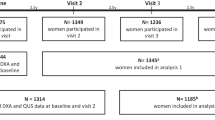
Two hundred eighty-two postmenopausal patients filled out a questionnaire which determined their FRAX index and performed a bone evaluation by QUS of the calcaneus to determine their stiffness index (SI). Thereafter, they underwent assessments by the gold-standard DXA bone examination.
Results
Statistically significant correlations were observed between FRAX (calculated without BMD) and both QUS and DXA diagnosis. FRAX mean indices of risk corresponding to the diagnosis of osteoporosis by QUS and DXA were similar. Receiver operating characteristic (ROC) curve analysis showed that both FRAX and QUS tests were sufficiently accurate in predicting the alteration of bone mineral composition. The ROC curves of QUS allowed us to identify, in our population, SI cutoff for normal patients (SI > 90.5) and for patients having osteoporosis (SI < 78.5). We selected a cutoff screening value from FRAX ROC curve for major clinical fracture (2.94). The following diagnostic algorithm demonstrated that the use of FRAX test alone has a sensitivity of 85.3 % and a specificity of 33.8 % while the use of QUS exam alone showed a sensitivity of 81.3 % and a specificity of 45.1 %. When considering the capacity of QUS exam in combination with FRAX test, the final algorithm showed a sensitivity of 69.4 % and a specificity of 57.7 %.
Conclusions
The use of QUS test with adjusted cutoffs offers a similar performance to the FRAX test alone in terms of sensitivity. The combined use of the tests reduces the sensibility but increases the specificity and adds clinical information related to the bone status of the patient.



Similar content being viewed by others


References
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy (2001) Osteoporosis prevention, diagnosis, and therapy. J Am Med Assoc 285:785–795
Assessment of fracture risk and its application to screening for postmenopausal osteoporosis (1994) Report of a WHO study group. World Health organ tech rep ser 843:1–129 [PMID: 7941614]
Melton LJ 3rd, Chrischilles EA, Cooper C, Lane AW, Riggs BL (1995) How many women have osteoporosis now? J Bone Miner Res 10:175–177
Siris ES, Chen YT, Abbott TA, Brett-Connor E, Miller PD, Wehren LE, Berger ML (2004) Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch Intern Med 164:1108–1112
Kanis JA, Johnell O, De Laet C, Johansson H, Oden A, Delmas P, Eisman J, Fujiwara S, Garnero P, Kroger H, McCloskey EV, Mellstrom D, Melton LJ, Pols H, Reeve J, Silman A, Tenenhouse A (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35:375–382
Johansen A (2012) Q fracture is better than FRAX tool in assessing risk of hip fracture. Br Med J 345:4988
Adami S, Bianchi G, Brandi ML, Di Munno O, Frediani B, Gatti D, Giannini S, Girasole G, Minisola G, Minisola S, Nuti R, Pedrazzoni M, Rossini M, Varenna M (2010) Validation and further development of the WHO 10-year fracture risk assessment tool in Italian postmenopausal women: project rationale and description. Clin Exp Rheumatol 28(4):561–570
Ward KD, Klesges RC (2001) A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcif Tissue Int 68:259–270
Berg KM, Kunins HV, Jackson JL, Nahvi S, Chaudhry A, Harris KA Jr, Malik R, Arnsten JH (2008) Association between alcohol consumption and both osteoporotic fracture and bone density. Am J Med 121:406–418
Piscitelli P, Chitano G, Johannson H, Brandi ML, Kanis JA, Black DM (2013) Updated fracture incidence rates for the Italian version of FRAX®. Osteoporos Int 24(3):859–866
Cortet B, Boutry N, Dubois P, Dubois P, Dubois P, Legroux-Ge´rot I, Cotten A, Marchandise X (2004) Does quantitative ultrasound of bone reflect more bone mineral density than bone microarchitecture? Calci Tissue Int 74:60–67
Sakata S, Barkmann R, Lochmuller E-M, Heller M, Gluer C-C (2004) Assessing bone status beyond BMD: evaluation of bone geometry and porosity by quantitative ultrasound of human finger phalanges. J Bone Miner Res 19:924–930
Njeh CF, Boivin CM, Langton CM (1997) The role of ultrasound in the assessment of osteoporosis: a review. Osteoporos Int 7:7–22
Hosszu E, Meszaros S (2003) Performance Evaluation of the Achilles insight: precision, accuracy, and comparison to central DXA. J Bone Miner Res 18(Supp1):117
Xu Y, Guo B, Gong J, Xu H, Bai Z (2014) The correlation between calcaneus stiffness index calculated by QUS and total body BMD assessed by DXA in Chinese children and adolescents. J Bone Miner Metab 32(2):159–166
Prins SH, Jørgensen HL, Jørgensen LV, Hassager C (1998) The role of quantitative ultrasound in the assessment of bone: a review. Clin Physiol 18(1):3–17
Kanis JA, Oden A, Johansson H, Borgström F, Ström O, McCloskey E (2009) FRAX and its applications to clinical practice. Bone 44(5):734–743
NB Watts, JP Bilezikian, PM Camacho (2010) AACE postmenopausal osteoporosis guidelines. Endocr Pract 16(Suppl 3)
Kanis JA, McCloskey EV, Johansson H (2013) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 24:23–57
Rabar Silvia, Lau Rosa, O’Flynn Norma (2012) Risk assessment of fragility fractures: summary of NICE guidance. BMJ 345:e3698
Glüer CC, Cummings SR, Bauer DC, Stone K, Pressman A, Mathur A, Genant HK (1996) Osteoporosis: association of recent fractures with quantitative US findings. Radiology 199:725–732
Leslie WD, Majumdar SR, Lix LM, Johansson H, Odena A, Mc Closey E, Kanis JA, Manitoba Bone Density Program (2012) High fracture probability with FRAX® usually indicates densitometric osteoporosis: implications for clinical practice. Osteoporos Int 23:391–397
Watts NB, Siris ES, Cummings SR, Bauer DC (2010) Filtering FRAX. Osteoporos Int 21:537–541
Chen XF, Li XL, Zhang H, Liu GJ (2014) Were you identified to be at high fracture risk by FRAX® before your osteoporotic fracture occurred? Clin Rheumatol 33(5):693–698. doi: 10.1007/s10067-014-2533-2 (Epub 2014 Feb 28)
Dawson-Huqhes B, Tosteson AN, Melton LJ 3rd et al (2008) Implications of absolute fracture risk assessment for osteoporosis practice guidelines in the USA. Osteoporos Int 19(4):449–458
Cranney A, Jamal SA, Tsang JF, Josse RG, Leslie WD (2007) Low bone mineral density and fracture burden in postmenopausal women. J Can Med Assoc 177:575–580
Bauer DC, Glüer CC, Cauley JA, Vogt TM, Ensrud KE, Genant HK, Black DM (1997) Broadband ultrasound attenuation predicts fractures strongly and independently of densitometry in older women. Arch Intern Med 157:629–634
Hans D, d’Argent-Molina P, Schott AM (1996) Ultrasonographic heel measurements to predict hip fracture in elderly women. Lancet 348:511–514
Catalano A, Morabito N, Basile G (2013) Fracture risk assessment in postmenopausal women referred to an Italian center for osteoporosis: a single day experience in Messina. Clin Cases Miner Bone Metab 10(3):191–194
Ettinger MP (2003) Aging bone and osteoporosis: strategies for preventing fractures in the elderly. Arch Intern Med 163(18):2237–2246
Glüer CC, Eastell R, Reid DM (2004) Association of five quantitative ultrasound devices and bone densitometry with osteoporotic vertebral fractures in a population-based sample: the OPUS Study. J Bone Miner Res 19(5):782–793
Flöter M, Bittar CK, Zabeu JLA, Carneiro ACR (2011) Review of comparative studies between bone densitometry and quantitative ultrasound of the calcaneus in osteoporosis. Acta Reumatol Port 36:327–335
Trimpou P, Bosaeus I, Bengtsson BA, Landin-Wilhelmsen K (2010) High correlation between quantitative ultrasound and DXA during 7 years of follow-up. Eur J Radiol 73(2):360–364 Epub 2009 Jan 8
Pearson D, Masud T, Sahota O, Earnshaw S, Hosking D (2003) A comparison of calcaneal dual X-ray absorptiometry and calcaneal ultrasound for predicting the diagnosis of osteoporosis from hip and spine bone densitometry. J Clin Densitom 6(4):345–352
Acknowledgments
We are grateful to Elisa Tempestilli for her help and her unrestricted support for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest. This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Ethical approval
All the procedures performed in the study were in accordance with the ethical standards of the institutional research comitee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Villa, P., Lassandro, A.P., Moruzzi, M.C. et al. A non-invasive prevention program model for the assessment of osteoporosis in the early postmenopausal period: a pilot study on FRAX® and QUS tools advantages. J Endocrinol Invest 39, 191–198 (2016). https://doi.org/10.1007/s40618-015-0341-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40618-015-0341-4