
Abstract
According to current guidelines, targeted therapy with a combination of BRAF plus MEK inhibitors is the preferred first-line treatment for patients with BRAF V600E-mutant metastatic non-small cell lung cancer (NSCLC). In the open-label, single-arm, phase 2 PHAROS trial (NCT03915951), the combination of encorafenib, a potent BRAF inhibitor, and binimetinib, a potent MEK inhibitor, demonstrated durable antitumor activity with a manageable safety profile in this patient population. On the basis of the results of this study, the combination of encorafenib plus binimetinib was approved by the US Food and Drug Administration on October 11, 2023, for patients with BRAF V600E-mutant metastatic NSCLC. In this review, we summarize the efficacy and safety of encorafenib plus binimetinib from the PHAROS study. In addition, we discuss strategies to manage adverse reactions with this combination therapy with the intent of minimizing unnecessary treatment discontinuations in these patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The BRAF plus MEK inhibitor combination of encorafenib plus binimetinib is indicated for the treatment of BRAF V600E-mutant metastatic non-small cell lung cancer. |
Adverse reactions experienced with encorafenib plus binimetinib in clinical trials were well managed with dose modifications. |
There is a need for resources detailing management of adverse reactions with encorafenib plus binimetinib in a clinical setting. |
We describe approaches for managing select adverse reactions as determined by published clinical trial data as well as opinion of an expert panel of oncologists with years of experience treating patients with metastatic non-small cell lung cancer receiving targeted therapy. |
The goal of adverse reaction management is minimizing treatment discontinuations. |
Introduction
Approximately 85% of patients with lung cancer are diagnosed with non-small cell lung cancer (NSCLC), and most NSCLCs have an adenocarcinoma histology [1,2,3]. To date, multiple actionable biomarkers with approved therapies have been identified, including oncogenic alterations in ALK, BRAF V600E, EGFR, HER2, KRAS, MET, NTRK, RET, ROS1, and expression of programmed death ligand 1 [4,5,6,7]. BRAF mutations occur in various solid tumors, including melanoma (≈ 40%), thyroid (≈ 33%), colorectal (CRC; ≈ 9%), and NSCLC (≈ 2–4%) [3, 8]. The BRAF gene encodes a kinase involved in the mitogen-activated protein kinase (MAPK) signaling pathway, which regulates cellular processes, including growth, differentiation, proliferation, and survival [9, 10]. BRAF mutations are grouped into three classes based on dimerization status and kinase activity level [9, 11]. While class I mutations occur exclusively at codon 600, resulting in a constitutively active BRAF monomer, class II and III mutations occur at non-V600 codons, resulting in constitutively active and kinase-dead or kinase-impaired dimers, respectively [11]. Class I mutations account for the majority of BRAF mutations (≈ 77%) in melanoma, whereas NSCLC has a more even distribution, with class I, II, and III mutations accounting for 31–45%, 32–34%, and 23–31% of BRAF-mutant NSCLCs, respectively [8, 12]. The most common BRAF mutation in NSCLC, which accounts for approximately 2% of all NSCLCs, is a class I mutation that replaces the valine at codon 600 with glutamic acid (V600E), resulting in an approximately 500-fold increase in kinase activity [8, 11, 13]. When considering treatment options for NSCLC, identification of oncogenic alterations is critically important since targeted therapy has improved outcomes for many actionable mutations, including BRAF V600E-mutant NSCLC [3, 14,15,16]. Therefore, all patients with advanced or metastatic NSCLC should undergo broad-based molecular testing, as recommended by current guidelines [5, 7].
Available Treatments for BRAF V600E-Mutant Metastatic NSCLC
Clinical investigation of targeted therapy for BRAF V600E-mutant NSCLC began with BRAF inhibitor monotherapy (vemurafenib, dabrafenib) [17, 18]. However, clinical benefit of monotherapy was limited by acquired resistance, which reactivates the MAPK pathway [19]. The addition of a MEK inhibitor (trametinib, binimetinib) to a BRAF inhibitor provided dual inhibition of the MAPK pathway and prolonged antitumor activity with a tolerable safety profile [15, 20, 21]. Dabrafenib plus trametinib was approved as the first BRAF plus MEK inhibitor targeted therapy for patients with BRAF V600E-mutant metastatic NSCLC (mNSCLC) in 2017 [22]. Encorafenib plus binimetinib was approved in October 2023 as the second BRAF and MEK inhibitor combination for this patient population [23]. Currently approved BRAF inhibitors inhibit monomers, and binding to one protomer in a dimer can cause paradoxical activation of the second protomer [9, 24]. Therefore, BRAF monomer inhibitors are not effective for inhibiting class II or III dimers [9, 25]. Novel drugs that inhibit dimers or disrupt dimerization are currently under investigation in preclinical and ongoing clinical trials and have even demonstrated initial efficacy against all three classes of BRAF mutations in preclinical models [25,26,27].
Guidelines for BRAF V600E-mutant NSCLC recommend BRAF and MEK inhibitors as the preferred first-line treatment and immunotherapy, chemotherapy, or a combination as alternative options [5, 7]. Although some clinicians prescribe immunotherapy with or without chemotherapy in the first-line setting, data from studies of immunotherapy or chemotherapy for patients with BRAF V600E-mutant NSCLC are limited with retrospective analyses, small population sizes, and conflicting results [12, 13, 28, 29]. Given the recent approval of encorafenib plus binimetinib for patients with BRAF V600E-mutant mNSCLC [23], we summarize the efficacy and safety profile of this combination therapy and address management of adverse reactions (ARs) in the clinical setting. These management approaches were determined by oncologists on the basis of their experience treating patients with mNSCLC receiving targeted therapy. This article is based on previously conducted studies and does not contain any new studies with human participants.
PHAROS Study: Efficacy and Safety
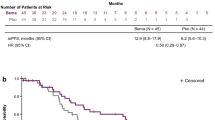
The phase 2 PHAROS (NCT03915951) study enrolled 59 treatment-naïve and 39 previously treated patients with BRAF V600E-mutant mNSCLC [15]. The key inclusion and exclusion criteria for the study are described in Supplementary Materials Table S1 [30]. Patients received orally administered encorafenib 450 mg once daily plus orally administered binimetinib 45 mg twice daily until disease progression, unacceptable toxicity, withdrawal of consent, initiation of subsequent anticancer therapy, or death. Tumor response was determined by independent radiology review (IRR, also called independent review committee) per Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 [15, 31]. For treatment-naïve patients, objective response rate (ORR) by IRR was 75%, median duration of response (DOR) was not estimable (NE), and median time to response was 1.9 months (Table 1) [15]. Median duration of follow-up for progression-free survival (PFS) by IRR was 18.2 months, median PFS was NE, and median overall survival (OS) was NE. For previously treated patients, ORR by IRR was 46%, median DOR was 16.7 months, and median time to response was 1.7 months. Median duration of follow-up for PFS by IRR was 12.8 months, median PFS was 9.3 months, and median OS was NE.
In the published primary analysis of PHAROS, safety data were reported as treatment-related adverse events and resulting dose modifications [15]. However, the US Food and Drug Administration (FDA) labels report all-causality ARs that occurred in ≥ 10% of patients in PHAROS and resulting dose modifications [31, 32]. Safety analysis of the 98 patients revealed that the most common ARs reported in ≥ 25% of patients included fatigue, nausea, diarrhea, musculoskeletal pain, vomiting, abdominal pain, visual impairment, dyspnea, rash, constipation, and cough (Table 2) [31, 32]. Pyrexia was reported in 22% of patients, with no grade 3 or 4 events. Serious ARs occurred in 38% of patients; ARs occurring in ≥ 2% of patients were hemorrhage (6%); diarrhea (4%); anemia, dyspnea, and pneumonia (3% each); and arrhythmia, device-related infection, edema, myocardial infarction, and pleural effusion (2% each). Dose modifications were generally related to gastrointestinal (GI) ARs. For encorafenib, ARs led to dose interruption in 59% of patients with diarrhea (17%) as the most common, dose reduction in 30% of patients with diarrhea and nausea (8% each) as the most common, and permanent discontinuation in 16% of patients with diarrhea and musculoskeletal pain (3% each) as the most common [31]. For binimetinib, ARs led to dose interruption in 62% of patients with diarrhea (17%) as the most common, dose reduction in 33% of patients with diarrhea (8%) as the most common, and permanent discontinuation in 17% of patients with diarrhea (3%) as the most common [32]. Treatment-related ARs led to dose interruption, dose reduction, and permanent discontinuations of both encorafenib plus binimetinib in 44%, 24%, and 15% of patients, respectively [15].
Dabrafenib plus Trametinib for Patients with BRAF V600E-Mutant mNSCLC
In the updated analysis of the phase 2 study of dabrafenib plus trametinib in patients with BRAF V600E-mutant mNSCLC, the ORR and median PFS were 64% and 10.8 months in treatment-naïve patients (n = 36) and 68% and 10.2 months in previously treated patients (n = 57) [14]. According to the US FDA label, the most common ARs in the overall population (n = 93) were pyrexia (55%), fatigue (51%), and nausea (45%) (Supplementary Materials Table S2) [33, 34]. While the incidence of cutaneous squamous cell carcinoma (SCC) was 12% with dabrafenib monotherapy in a previous trial, SCC was reported in 4% of patients receiving dabrafenib plus trametinib [18, 20]. The most common treatment-emergent laboratory abnormalities were hyperglycemia (71%), increased alkaline phosphatase (64%), and increased aspartate aminotransferase (AST; 61%) [33, 34]. For dabrafenib, ARs led to dose interruption in 62% of patients with pyrexia (27%) as the most common, dose reduction in 35% of patients with pyrexia (10%) as the most common, and permanent discontinuation in 18% of patients with pyrexia, decreased ejection fraction, and respiratory distress (2% each) as the most common [33]. For trametinib, ARs led to dose interruption in 57% of patients with pyrexia (16%) as the most common, dose reduction in 30% of patients with pyrexia (5%) as the most common, and permanent discontinuation in 19% of patients with pyrexia, decreased ejection fraction, and respiratory distress (2% each) as the most common [34]. Management strategies for ARs associated with dabrafenib plus trametinib have been summarized in previous publications, and the strategies generally focus on patient education, proactive evaluations, supportive care, and dose modifications [35, 36]. Pyrexia was the leading cause for dose modifications for patients treated with dabrafenib plus trametinib [33, 34]. Therefore, there is an emphasis on managing pyrexia for patients receiving dabrafenib plus trametinib [35, 36].
Encorafenib plus Binimetinib for Patients with Other Solid Tumors
In 2018, encorafenib plus binimetinib was approved by the US FDA for BRAF V600E/K-mutant unresectable or metastatic melanoma [37]. This approval was based on the phase 3 COLUMBUS study, which evaluated encorafenib (n = 194), encorafenib plus binimetinib (n = 192), and vemurafenib (n = 191) [37, 38]. According to the US FDA labels, the most common ARs were fatigue (43%), nausea (41%), and vomiting (30%) (Supplementary Materials Table S3) [31, 32]. The most common laboratory abnormalities were increased creatinine (93%), increased gamma glutamyl transferase (45%), and anemia (36%). For encorafenib, ARs led to dose interruption in 30% of patients with nausea and vomiting (7% each) as the most common, dose reduction in 14% of patients with arthralgia, fatigue, and nausea (2% each) as the most common, and permanent discontinuations in 5% of patients with hemorrhage (2%) as the most common [31]. For binimetinib, ARs led to dose interruption in 33% of patients with left ventricular dysfunction (6%) as the most common, dose reduction in 19% of patients with left ventricular dysfunction and serous retinopathy (3% each) as the most common, and permanent discontinuations in 5% of patients with hemorrhage (2%) as the most common [32].
The PHAROS study demonstrated that the safety profile and pharmacokinetic data (Table 3) for encorafenib plus binimetinib were generally consistent with those reported in previous melanoma studies [15, 39, 40]. Direct comparisons between the clinical trials cannot be made because of differences in trial designs, populations, and analyses; however, dose modification rates vary between melanoma and NSCLC [31, 32]. For patients with BRAF V600E-mutant mNSCLC, GI ARs were the most common reason for both encorafenib and binimetinib dose modifications. For patients with BRAF V600E/K-mutant melanoma, GI ARs, arthralgia, fatigue, and nausea were the most common reasons for encorafenib dose modifications and left ventricular dysfunction, serous retinopathy, and hemorrhage were the most common reasons for binimetinib dose modifications.
Encorafenib, in combination with cetuximab, is approved for patients with previously treated BRAF V600E-mutant metastatic CRC [31]. This approval was based on the phase 3 BEACON study, which compared encorafenib plus cetuximab with or without binimetinib (n = 224 and n = 220, respectively) with investigator’s choice of chemotherapy plus cetuximab (n = 221) in patients with previously treated BRAF V600E-mutant CRC [41, 42]. Management strategies for ARs associated with this treatment combination were previously published [43].
Management of Encorafenib plus Binimetinib–Associated ARs in Clinical Practice Treating Patients with BRAF V600E-Mutant NSCLC
While clinical trials monitor and manage ARs [44], this publication outlines real-world strategies for healthcare providers. Providing healthcare providers with management strategies can potentially improve the patient’s experience on treatment, decrease incidence of permanent discontinuations, increase duration of treatment, and improve treatment outcomes [35, 44, 45]. While the NSCLC indication for encorafenib plus binimetinib was recently approved, this combination has been used to treat patients in standard of care with melanoma since 2018 [23, 37]. Therefore, clinicians have years of experience managing the associated ARs, and AR management strategies for patients with melanoma have been previously published [44, 45]. These AR management strategies for patients with BRAF V600E-mutant mNSCLC were developed on the basis of clinical data from the PHAROS trial and recommendations from oncologists experienced in treating patients for NSCLC with encorafenib plus binimetinib along with prior recommendations for treating patients with melanoma.
Prior to beginning treatment with encorafenib plus binimetinib, patients and caregivers should be educated on the potential ARs and what to do should they occur [44]. Special attention should be given to Gl ARs as these are common reasons for dose interruption and reduction [31, 32]. Patients should keep track of ARs between appointments to discuss with their healthcare providers. Baseline and recurring evaluations should be conducted for liver function, electrolytes, creatinine with creatine phosphokinase (CPK), echocardiogram or multiple gated acquisition (MUGA) scan, and dermatologic examinations [31, 32]. Ophthalmologic evaluations should be done at regular intervals and when assessing new or worsening symptoms. Patients with certain comorbidities (e.g., cardiovascular risks) should be closely monitored.
Some ARs can be managed with lifestyle changes or over-the-counter (OTC) medications (Table 4) [44]. However, dose modifications are typically recommended for higher grade or recurrent ARs, and recommendations for general ARs are summarized in Fig. 1 [31, 32]. Starting doses and dose modifications are similar for patients with NSCLC or melanoma; however, for patients with BRAF V600E/K-mutant melanoma, if there is moderate or severe hepatic impairment, the recommended starting dose for binimetinib is 30 mg instead of 45 mg [31, 32]. For BRAF V600E-mutant metastatic CRC, the recommended starting dose of encorafenib is 300 mg instead of 450 mg and the minimum dose is 150 mg instead of 225 mg [31]. ARs of hepatotoxicity, uveitis, dermatologic conditions, cardiomyopathy, new primary malignancy, corrected QT interval (QTc) prolongation, rhabdomyolysis, serous retinopathy, retinal vein occlusion, venous thromboembolism, and interstitial lung disease have specific dose modification recommendations (Fig. 2). Some ARs are associated with either encorafenib or binimetinib and necessitate dose modification of that agent alone (Fig. 2b, c). If encorafenib is permanently discontinued, binimetinib should be discontinued [32]. If binimetinib is withheld, encorafenib should be reduced to a maximum of 300 mg once daily [31]. The following sections describe ARs observed in PHAROS and corresponding management strategies.


Dose modifications for specific ARs [31, 32]. a ARs that require encorafenib plus binimetinib dose modifications. b ARs that require encorafenib dose modifications. c ARs that require binimetinib dose modifications. ALT alanine aminotransferase, AR adverse reaction. AST aspartate aminotransferase, CPK creatine phosphokinase, DVT deep vein thrombosis, LLN lower limit of normal, LVEF left ventricular ejection fraction, PE pulmonary embolism, QTc corrected QT interval, QTcF Fridericia correction formula
General Disorders
General disorders, comprising systemic instead of localized reactions, were the most common group of ARs, including fatigue (61%), edema (23%), and pyrexia (22%) (Table 2) [31, 32]. For fatigue, management strategies include resting when necessary [44] and exercising when tolerable (Table 4). The appropriate level of physical activity should be determined by several factors, including anemia, comorbidities, and safety (e.g., fall risk) [46]. Additionally, referral for rehabilitation (e.g., physical therapy, occupational therapy, physical medicine) or nutrition consultation should be considered. For edema, compression and elevation may help relieve swelling [45]. For pyrexia, all reported pyrexia events in PHAROS were grade ≤ 2 [31, 32]. For mild to moderate pyrexia (100.4–104.0 °F or 38.0–40.0 °C), management strategies include OTC medications (e.g., acetaminophen, nonsteroidal anti-inflammatory drugs [NSAIDs]) and fluids to maintain hydration [44, 47]. While severe to life-threatening pyrexia (grade ≥ 3 [104.0 °F or 40 °C]) was not reported in PHAROS, it was reported by 4% of patients receiving encorafenib plus binimetinib in previous melanoma trials [31, 32, 47]. Management strategies that can be considered for symptomatic, recurrent, refractory, or grade ≥ 3 pyrexia include treatment interruptions, antibiotics, antipyretics, or low-dose corticosteroids (e.g., prednisone) [44, 48]. Alternative causes for these ARs, such as infection, disease progression, or a hematologic abnormality (e.g., anemia), should also be considered and addressed accordingly. Although most general disorder ARs in PHAROS were grade ≤ 2, dose modifications were required by some patients [31, 32]. Dose modifications are recommended for ARs that are either recurrent grade 2 or any occurrence of grade ≥ 3 (Fig. 1).
Gastrointestinal ARs
GI ARs are class effects associated with BRAF plus MEK inhibitors and are typically mild or moderate [31, 32, 44, 45]. In PHAROS, GI effects included nausea (58%), diarrhea (52%), vomiting (37%), abdominal pain (32%), and constipation (27%) (Table 2) [31, 32]. Most GI ARs can be managed with non-pharmacological or pharmacological strategies on an outpatient basis [44]. Non-pharmacological management strategies include dietary changes, such as eating frequent, small meals and reducing fiber consumption (Table 4) [44]. Encorafenib and binimetinib can be taken with or without food [31, 32]. Eating a small meal with treatment may help with nausea. No data evaluating the impact of fasting on efficacy and tolerability of encorafenib plus binimetinib for patients from PHAROS are available. Hydration is critical given the potential for loss of fluids through vomiting and diarrhea to lead to dehydration, hypotension, or, in severe incidences, kidney failure [45]. Sports drinks are an option for remaining hydrated and replacing electrolytes.
OTC medications, antiemetics (e.g., dexamethasone, lorazepam, metoclopramide, olanzapine, prochlorperazine, 5-hydroxytryptamine-3 [5-HT3] receptor antagonists), and anti-diarrheal medications (e.g., loperamide, diphenoxylate/atropine, octreotide) can be used to relieve GI symptoms [44, 49]. When prescribing drugs for coadministration, healthcare providers should consider all current medications and be cautious of potential drug interactions. Encorafenib is associated with QTc prolongation, so when administered with other drugs that may prolong QT intervals (e.g., olanzapine, metoclopramide, 5-HT3 receptor antagonists), patients should be monitored by electrocardiogram [31, 49]. Dexamethasone is a CYP3A4 inducer and may lower encorafenib plasma concentration and subsequently efficacy [31, 50]. Other causes of GI effects, such as infections (e.g., Clostridium difficile) or progressive disease, should also be considered [45]. Although most GI ARs in PHAROS were grade ≤ 2, they were the most common reasons for dose interruptions, reductions, and permanent discontinuations for both encorafenib and binimetinib [31, 32]. Dose modifications are recommended for GI ARs that are either recurrent grade 2 or any occurrence of grade ≥ 3 (Fig. 1).
Musculoskeletal and Connective Tissue Disorders
Musculoskeletal pain, which included events such as back pain, arthralgia, myalgia, and non-cardiac chest pain, was reported by 48% of patients [31, 32]. Although not reported in PHAROS, arthritis occurred in 1% and 2% of patients receiving encorafenib with and without binimetinib, respectively, in a prior melanoma trial; polyarthritis occurred in 2% of patients receiving encorafenib, including grade 3 in 1% [38]. Medication (e.g., analgesics, NSAIDs, low-dose anti-inflammatory drugs, or steroids) [44], physical therapy, stretching, and hot and cold compresses may relieve pain and swelling of joints. Moderate- to high-dose steroids should be considered for severe ARs, including myositis or vasculitis [44, 45]. A rheumatologist consultation may be recommended for select cases, including if considering intra-articular or high-dose steroids. If a patient is refractory to steroids, leflunomide or methotrexate may be considered after a rheumatologist consultation. Recurring or severe musculoskeletal ARs should be managed with dose modifications (Fig. 1) [31, 32].
In addition to musculoskeletal pain, increased CPK was a laboratory abnormality observed in 41% of patients, including grade ≥ 3 in 3% of patients [31, 32]. Increased CPK may be a potential sign of rhabdomyolysis, which is the rapid breakdown of skeletal muscle and has been associated with encorafenib plus binimetinib treatment in previous trials with melanoma (0.1%) [32, 51]. CPK and creatinine levels should be measured prior to initiating treatment and periodically throughout treatment [32]. If a patient has asymptomatic grade 4 CPK elevation (> 10 × upper limit of normal) or any-grade symptomatic CPK elevation or renal impairment, binimetinib should be withheld ≤ 4 weeks (Fig. 2c) [32, 47]. If CPK levels have improved to grade ≤ 1 (≤ 2.5 × upper limit of normal), binimetinib can be resumed at a reduced dose. However, if there is no improvement, binimetinib should be permanently discontinued and the dose of encorafenib adjusted [31, 32, 47]. In clinical practice, if the patient has low-grade symptomatic CPK but is otherwise doing well, it would be considered reasonable to continue treatment under close observation.
Hepatotoxicity
Hepatotoxicity manifests as increased liver enzymes in laboratory tests, including alanine aminotransferase (ALT) and AST. ALT was increased in 34% of patients, with grade 3 or 4 in 9% [31, 32]. AST was increased in 31% of patients, with grade 3 or 4 in 10%. Patients should be aware of the possible signs of liver dysfunction, such as jaundice, dark or brown urine, nausea, vomiting, loss of appetite, fatigue, bruising, and bleeding [31, 32]. Liver function should be evaluated prior to treatment and monthly throughout treatment [31, 32]. Specific dose modification guidance for ALT and AST elevations is found in Fig. 2a. A differential diagnosis should be conducted, and alternative causes considered, such as liver injury or infection [45].
Ocular Disorders
Ocular disorders are class effects associated with BRAF and MEK inhibitors [35, 44]. Visual impairment was observed in 29% of patients, with grade ≥ 3 events in 2% of patients (Table 2) [31, 32]. Additionally, serous retinopathy without blindness (2%) and uveitis (1%) were reported in PHAROS. In previous clinical trials with encorafenib plus binimetinib for patients with melanoma, serous retinopathy without blindness (20%), uveitis (4%), and retinal vein occlusion (0.1%) were reported. Visual symptoms should be assessed at each visit, and ophthalmologic evaluations should be performed at regular intervals and as directed for new visual disturbances. Safety has not been determined for patients with a history of or risk factors for retinal vein occlusion [32]. In clinical practice, asymptomatic patients might not undergo ophthalmologic evaluations [31, 32]. However, this approach may differ, and it is best to use clinical judgment when determining when ophthalmologic examinations are necessary. Patients should be educated about the possibility of changes to their vision and be advised to inform their healthcare provider. For symptomatic relief, management strategies include topical NSAIDs or carbonic anhydrase inhibitors [44]. For some cases, an ophthalmologist may be consulted. Symptomatic serous retinopathy or retinal pigment epithelial detachments should be managed by withholding binimetinib for up to 10 days (Fig. 2c) [32]. If the condition improves and is asymptomatic, binimetinib should be resumed at a reduced dose. However, if the condition does not improve, binimetinib could be resumed at a reduced dose or discontinued.
Skin and Subcutaneous Tissue Disorders
Dermatologic ARs are considered a class effect of both BRAF and MEK inhibitors (Table 2, Supplementary Materials Table S3) [35, 44]. In PHAROS, dermatological ARs included rash (27%), pruritus (16%), dry skin (13%), and alopecia (12%) [31, 32]. It is important for patients to inform their healthcare provider about any skin changes immediately [31, 32]. Management strategies for mild rashes include creams, emollients, topical corticosteroids (e.g., hydrocortisone) [44], changes in clothing, or lotions. Moderate to severe cases may require additional medications, such as topical steroids (e.g., triamcinolone, clobetasol), prednisone, antihistamines, or referral to a dermatologist [44]. Photosensitivity was reported by 4% of patients in a previous trial of encorafenib plus binimetinib for melanoma [52]. Patients should proactively prevent photosensitive reactions by applying broad-spectrum sunscreen and lip balm, wearing ultraviolet-protective clothing, avoiding sun exposure [44], and avoiding alcohol-based fragrances or lotions. Dose modifications for general dermatologic ARs are summarized in Fig. 2a.
New skin cancers, including cutaneous SCC and basal cell carcinoma, are associated with encorafenib and other BRAF inhibitors [21, 31, 53]. In PHAROS, cutaneous SCC and skin papilloma each occurred in 2% of patients [31]. The incidence of SCC is decreased by the addition of MEK inhibitors [20, 53]. For instance, in previous trials with encorafenib monotherapy and encorafenib plus binimetinib for patients with melanoma, cutaneous SCC occurred in 8% and 3% of patients, respectively [31]. Proactive management is important as the median onset to first occurrence for cutaneous SCC with encorafenib plus binimetinib for patients with melanoma was 5.8 months. Patients should proactively check their skin for any changes (e.g., new wart, a sore that bleeds or does not heal, changes to a mole) and alert their healthcare provider. Healthcare providers should check the patient’s skin before treatment and every 2 months during treatment and up to 6 months after treatment. In clinical practice, ongoing dermatologic evaluations every 3 to 6 months are suggested. Dose modifications are not recommended for new primary cutaneous malignancies, but non-cutaneous malignancies can also occur. Patients should be monitored for symptoms of non-cutaneous malignancies, and encorafenib should be discontinued for RAS-mutant non-cutaneous malignancies (Fig. 2b).
Cardiac Disorders
In PHAROS, cardiomyopathy manifesting as left ventricular dysfunction was reported in 11% of patients, with grade 3 in 1% (Table 2) [31, 32]. In a previous melanoma trial, left ventricular dysfunction occurred in 7% of patients, with grade 3 in 2% and a median time to onset of 3.6 months. Cardiomyopathy resolved in 82% and 87% of patients in NSCLC and melanoma trials, respectively. Ejection fraction should be assessed by echocardiogram or MUGA scan before initiating treatment, 1 month after treatment initiation, and every 2 to 3 months during treatment. Safety of encorafenib plus binimetinib has not been evaluated in patients with baseline ejection fraction that is < 50% or below institutional lower limit of normal. In addition, dose-dependent QTc prolongation has been associated with encorafenib treatment, with an increase in QTcF to > 500 ms in 2.1% of patients in PHAROS [31]. Electrolytes should be evaluated, and abnormalities should be remedied. Close monitoring should be instituted for patients with cardiovascular risks, including current or risk for developing QTc prolongation [31, 32]. Patients who experience a decrease in left ventricular ejection fraction or prolongation in QTc need to be carefully assessed, and treatment should be withheld, dose reduced, or permanently discontinued on the basis of severity and recurrence as outlined in Fig. 2. Consultation with a cardiologist should also be considered [44].
Conclusion
In the PHAROS study, encorafenib plus binimetinib was an effective therapy option for patients with BRAF V600E-mutant mNSCLC and was generally well tolerated, with most ARs being grade ≤ 2 [15, 31, 32]. ARs were generally managed with dose interruptions or dose reductions, with ARs resulting in permanent discontinuation of encorafenib or binimetinib in only 16% and 17% of patients, respectively. The safety profile was generally consistent with that observed in patients with BRAF V600E- or V600K-mutant unresectable or metastatic melanoma. The 5-year updated analysis from that trial demonstrated continued tolerability with no new safety concerns [52]. Management of ARs associated with encorafenib plus binimetinib involves proactive communication, supportive care, and occasional dose modifications. Proactive AR management may prevent unnecessary treatment discontinuations and enable patients to remain on encorafenib and binimetinib while deriving clinical benefit.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Change history
04 June 2024
A Correction to this paper has been published: https://doi.org/10.1007/s12325-024-02907-9
References
American Cancer Society. Key statistics for lung cancer. https://www.cancer.org/cancer/types/lung-cancer/about/key-statistics.html. Accessed 20 Nov 2023.
Ganti AK, Klein AB, Cotarla I, Seal B, Chou E. Update of incidence, prevalence, survival, and initial treatment in patients with non-small cell lung cancer in the US. JAMA Oncol. 2021;7(12):1824–32.
Barlesi F, Mazieres J, Merlio JP, et al. Routine molecular profiling of patients with advanced non-small-cell lung cancer: results of a 1-year nationwide programme of the French Cooperative Thoracic Intergroup (IFCT). Lancet. 2016;387(10026):1415–26.
Baik CS, Myall NJ, Wakelee HA. Targeting BRAF-mutant non-small cell lung cancer: from molecular profiling to rationally designed therapy. Oncologist. 2017;22(7):786–96.
Hendriks LE, Kerr KM, Menis J, et al. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(4):339–57.
Negrao MV, Skoulidis F, Montesion M, et al. Oncogene-specific differences in tumor mutational burden, PD-L1 expression, and outcomes from immunotherapy in non-small cell lung cancer. J Immunother Cancer. 2021;9(8):e002891.
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V.5.2023. © National Comprehensive Cancer Network, Inc. 2023. All rights reserved. Accessed [29 Nov 2023]. To view the most recent complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way. NCCN, National Comprehensive Cancer Network® (NCCN®).
Owsley J, Stein MK, Porter J, et al. Prevalence of class I-III BRAF mutations among 114,662 cancer patients in a large genomic database. Exp Biol Med (Maywood). 2021;246(1):31–9.
Yaeger R, Corcoran RB. Targeting alterations in the RAF-MEK pathway. Cancer Discov. 2019;9(3):329–41.
Ottaviano M, Giunta EF, Tortora M, et al. BRAF gene and melanoma: back to the future. Int J Mol Sci. 2021;22(7):3474.
Śmiech M, Leszczyński P, Kono H, Wardell C, Taniguchi H. Emerging BRAF mutations in cancer progression and their possible effects on transcriptional networks. Genes (Basel). 2020;11(11):1342.
Dagogo-Jack I, Martinez P, Yeap BY, et al. Impact of BRAF mutation class on disease characteristics and clinical outcomes in BRAF-mutant lung cancer. Clin Cancer Res. 2019;25(1):158–65.
Cardarella S, Ogino A, Nishino M, et al. Clinical, pathologic, and biologic features associated with BRAF mutations in non-small cell lung cancer. Clin Cancer Res. 2013;19(16):4532–40.
Planchard D, Besse B, Groen HJM, et al. Phase 2 study of dabrafenib plus trametinib in patients with BRAF V600E-mutant metastatic NSCLC: updated 5-year survival rates and genomic analysis. J Thorac Oncol. 2022;17(1):103–15.
Riely GJ, Smit EF, Ahn MJ, et al. Phase II, open-label study of encorafenib plus binimetinib in patients with BRAFV600-mutant metastatic non-small-cell lung cancer. J Clin Oncol. 2023;41(21):3700–11.
Waterhouse DM, Tseng WY, Espirito JL, Robert NJ. Understanding contemporary molecular biomarker testing rates and trends for metastatic NSCLC among community oncologists. Clin Lung Cancer. 2021;22(6):e901–10.
Hyman DM, Puzanov I, Subbiah V, et al. Vemurafenib in multiple nonmelanoma cancers with BRAF V600 mutations. N Engl J Med. 2015;373(8):726–36.
Planchard D, Kim TM, Mazieres J, et al. Dabrafenib in patients with BRAF(V600E)-positive advanced non-small-cell lung cancer: a single-arm, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016;17(5):642–50.
Subbiah V, Baik C, Kirkwood JM. Clinical development of BRAF plus MEK inhibitor combinations. Trends Cancer. 2020;6(9):797–810.
Planchard D, Besse B, Groen HJM, et al. Dabrafenib plus trametinib in patients with previously treated BRAF(V600E)-mutant metastatic non-small cell lung cancer: an open-label, multicentre phase 2 trial. Lancet Oncol. 2016;17(7):984–93.
Planchard D, Smit EF, Groen HJM, et al. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: an open-label, phase 2 trial. Lancet Oncol. 2017;18(10):1307–16.
US Food and Drug Administration. FDA grants regular approval to dabrafenib and trametinib combination for metastatic NSCLC with BRAF V600E mutation. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-regular-approval-dabrafenib-and-trametinib-combination-metastatic-nsclc-braf-v600e. Accessed 2 Feb 2023.
US Food and Drug Administration. FDA approves encorafenib with binimetinib for metastatic non-small cell lung cancer with a BRAF V600E mutation. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-encorafenib-binimetinib-metastatic-non-small-cell-lung-cancer-braf-v600e-mutation. Accessed 20 Nov 2023.
Poulikakos PI, Zhang C, Bollag G, Shokat KM, Rosen N. RAF inhibitors transactivate RAF dimers and ERK signalling in cells with wild-type BRAF. Nature. 2010;464(7287):427–30.
Franovic A, Miller N, Severson P, et al. The next-generation pan-RAF inhibitor, KIN-2787, is active in class II and class III BRAF mutant models. J Clin Oncol. 2021;39(15_suppl):3116.
Cook FA, Cook SJ. Inhibition of RAF dimers: it takes two to tango. Biochem Soc Trans. 2021;49(1):237–51.
Rasco DW, Medina T, Corrie P, et al. Phase 1 study of the pan-RAF inhibitor tovorafenib in patients with advanced solid tumors followed by dose expansion in patients with metastatic melanoma. Cancer Chemother Pharmacol. 2023;92(1):15–28.
Dudnik E, Peled N, Nechushtan H, et al. BRAF mutant lung cancer: programmed death ligand 1 expression, tumor mutational burden, microsatellite instability status, and response to immune check-point inhibitors. J Thorac Oncol. 2018;13(8):1128–37.
Guisier F, Dubos-Arvis C, Vinas F, et al. Efficacy and safety of anti-PD-1 immunotherapy in patients with advanced NSCLC with BRAF, HER2, or MET mutations or RET translocation: GFPC 01–2018. J Thorac Oncol. 2020;15(4):628–36.
Riely GJ, Ahn MJ, Felip E, et al. Encorafenib plus binimetinib in patients with BRAFV600-mutant non-small cell lung cancer: phase II PHAROS study design. Future Oncol. 2022;18(7):781–91.
Array BioPharma Inc. Braftovi (encorafenib). Package insert. https://www.accessdata.fda.gov/spl/data/c2eedf4c-59b6-43ed-9820-a5621fa3e18f/c2eedf4c-59b6-43ed-9820-a5621fa3e18f.xml. Accessed 20 Nov 2023.
Array BioPharma Inc. Mektovi (binimetinib). Package insert. https://www.accessdata.fda.gov/spl/data/4e0f2551-01a9-46c6-8019-bd5535c09ee6/4e0f2551-01a9-46c6-8019-bd5535c09ee6.xml. Accessed 20 Nov 2023.
Novartis Pharmaceuticals Corporation. Tafinlar (dabrafenib). Package insert. https://www.accessdata.fda.gov/spl/data/23689dc5-f2a5-4475-bbc1-bd73107e51ba/23689dc5-f2a5-4475-bbc1-bd73107e51ba.xml. Accessed 25 Jan 2024.
Novartis Pharmaceuticals Corporation. Mekinist (trametinib). Package insert. https://www.accessdata.fda.gov/spl/data/26a4b56c-c10d-4b34-97d2-e46d150f2043/26a4b56c-c10d-4b34-97d2-e46d150f2043.xml. Accessed 29 Jan 2024.
Chalmers A, Cannon L, Akerley W. Adverse event management in patients with BRAF V600E-mutant non-small cell lung cancer treated with dabrafenib plus trametinib. Oncologist. 2019;24(7):963–72.
Schadendorf D, Robert C, Dummer R, et al. Pyrexia in patients treated with dabrafenib plus trametinib across clinical trials in BRAF-mutant cancers. Eur J Cancer. 2021;153:234–41.
US Food and Drug Administration. FDA approves encorafenib and binimetinib in combination for unresectable or metastatic melanoma with BRAF mutations. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-encorafenib-and-binimetinib-combination-unresectable-or-metastatic-melanoma-braf. Accessed 20 Nov 2023.
Dummer R, Ascierto PA, Gogas HJ, et al. Encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF-mutant melanoma (COLUMBUS): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2018;19(5):603–15.
Sullivan RJ, Weber J, Patel S, et al. A phase Ib/II study of the BRAF inhibitor encorafenib plus the MEK inhibitor binimetinib in patients with BRAF(V600E/K)-mutant solid tumors. Clin Cancer Res. 2020;26(19):5102–12.
Delord JP, Robert C, Nyakas M, et al. Phase I dose-escalation and -expansion study of the BRAF inhibitor encorafenib (LGX818) in metastatic BRAF-mutant melanoma. Clin Cancer Res. 2017;23(18):5339–48.
US Food and Drug Administration. FDA approves encorafenib in combination with cetuximab for metastatic colorectal cancer with a BRAF V600E mutation. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-encorafenib-combination-cetuximab-metastatic-colorectal-cancer-braf-v600e-mutation. Accessed 30 Jan 2024.
Tabernero J, Grothey A, Van Cutsem E, et al. Encorafenib plus cetuximab as a new standard of care for previously treated BRAF V600E-mutant metastatic colorectal cancer: updated survival results and subgroup analyses from the BEACON study. J Clin Oncol. 2021;39(4):273–84.
Tabernero J, Velz L, Trevino TL, et al. Management of adverse events from the treatment of encorafenib plus cetuximab for patients with BRAF V600E-mutant metastatic colorectal cancer: insights from the BEACON CRC study. ESMO Open. 2021;6(6):100328.
Augustyn K, Joseph J, Patel AB, Razmandi A, Ali AN, Tawbi HA. Treatment experience with encorafenib plus binimetinib for BRAF V600-mutant metastatic melanoma: management insights for clinical practice. Melanoma Res. 2023;33(5):406–16.
Heinzerling L, Eigentler TK, Fluck M, et al. Tolerability of BRAF/MEK inhibitor combinations: adverse event evaluation and management. ESMO Open. 2019;4(3):e000491.
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Cancer-Related Fatigue V.2.2024. © National Comprehensive Cancer Network, Inc. 2023. All rights reserved. Accessed [29 Nov 2023]. To view the most recent complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
US Department of Health and Human Services. Common terminology criteria for adverse events (CTCAE). https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf. Accessed 20 Nov 2023.
Welsh SJ, Corrie PG. Management of BRAF and MEK inhibitor toxicities in patients with metastatic melanoma. Ther Adv Med Oncol. 2015;7(2):122–36.
Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Antiemesis V.1.2024. © National Comprehensive Cancer Network, Inc. 2023. All rights reserved. Accessed [4 Mar 2024]. To view the most recent complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
Hikma Pharmaceuticals USA Inc. Dexamethasone package insert. https://www.accessdata.fda.gov/spl/data/d46e603b-62eb-4cf5-8d38-b28fc7eb3f95/d46e603b-62eb-4cf5-8d38-b28fc7eb3f95.xml. Accessed 20 Nov 2023.
Torres PA, Helmstetter JA, Kaye AM, Kaye AD. Rhabdomyolysis: pathogenesis, diagnosis, and treatment. Ochsner J. 2015;15:58–69.
Dummer R, Flaherty KT, Robert C, et al. COLUMBUS 5-year update: a randomized, open-label, phase III trial of encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF V600-mutant melanoma. J Clin Oncol. 2022;40(36):4178–88.
Gogas HJ, Flaherty KT, Dummer R, et al. Adverse events associated with encorafenib plus binimetinib in the COLUMBUS study: incidence, course and management. Eur J Cancer. 2019;119:97–106.
Piscitelli J, Hens B, Tomaszewska I, et al. Effect of food and a proton-pump inhibitor on the absorption of encorafenib: an in vivo-in vitro-in silico approach. Mol Pharm. 2023;20(5):2589–99.
Medical Writing/Editorial Assistance.
Medical writing support was provided by Caitlin Cash, PhD, of Nucleus Global and was funded by Pfizer.
Funding
The PHAROS study was sponsored by Pfizer. The Rapid Service Fee and Open Access Fee for this manuscript were funded by Pfizer.
Author information
Authors and Affiliations
Contributions
Christina Baik, Michael Cheng, Martin Dietrich, Jhanelle Gray, and Nagla Karim contributed to the drafting and revisions of the manuscript, take responsibility for the integrity of the work, and have provided their approval for the final version.
Corresponding author
Ethics declarations
Conflict of Interest
Christina Baik reports grant funding from AstraZeneca, Rain Oncology, Nuvalent, Blueprint, TurningPoint, Bristol Myers Squibb, Lilly, Jansen, Daiichi Sankyo, Spectrum, Pfizer, Loxo, Boehringer Ingelheim, Genentech/Roche, and the National Institutes of Health/National Cancer Institute, as well as consulting fees from Daiichi Sankyo, Boehringer Ingelheim, Novartis, Jansen, Regeneron, Silverback, Pfizer, AstraZeneca, Guardant, TurningPoint, Takeda, and Genentech. Michael Cheng reports honoraria from the Lynx Group, WebMD, and Potomac Center for Medical Education; has had a consulting or advisory role with AstraZeneca, Inivata, Boehringer Ingelheim, Cephied, Mirati, Janssen, Pfizer, and Noetik; research funding from Palleon Pharmaceuticals; and travel, accommodations, and expenses from Daiichi Sankyo, AstraZeneca, and Genzyme. Martin Dietrich reports a speaking or service role with Amgen, AstraZeneca, Bayer, Blueprint Medicines, Bristol Myers Squibb, Caris Life Sciences, Daiichi Sankyo, Eli Lilly & Co, EMD Serono, Epizyme, Foundation Medicine, G1 Therapeutics, Genentech, Gilead Pharmaceuticals, Janssen Pharmaceuticals, Mirati Therapeutics, Myriad, Novartis, Pfizer, Puma, Regeneron, Sanofi Genzyme, Stemline Oncology, and Takeda; and a consulting role with Amgen, AstraZeneca, Bayer, Blueprint Medicines, Bristol Myers Squibb, Caris Life Sciences, Daiichi Sankyo, Eli Lilly & Co, EMD Serono, Epizyme, Foundation Medicine, G1 Therapeutics, Genentech, Gilead Pharmaceuticals, Janssen Pharmaceuticals, Mirati Therapeutics, Myriad, Novartis, Pfizer, Puma, Regeneron, Sanofi Genzyme, Stemline Oncology, and Takeda. Jhanelle Gray reports a consulting role with Amgen, Gilead, and Grid; grants and personal fees from AstraZeneca, Bristol Myers Squibb, Genentech, Merck & Co, Inc, and Novartis; personal fees from AbbVie, Axiom HC Strategies, Blueprint Medicines, Celgene, Daiichi Sankyo, Inc, EMD Serono—Merck KGaA, Inivata, Janssen Scientific, Jazz Pharmaceuticals, Loxo Oncology Inc, OncoCyte Biotechnology, Sanofi Pharmaceuticals, and Takeda Pharmaceuticals; grants from Boehringer Ingelheim, G1 Therapeutics, Ludwig Institute of Cancer Research, and Pfizer; and research funding from Gilead and Pfizer. Nagla Karim reports research funding from Pfizer, Bristol Myers Squibb, Exelixis, and Genentech; speaker’s bureau from Regeneron, AstraZeneca, and Sanofi; and advisory board role with Jazz, Merck, Pfizer, Amgen, and G1 Therapeutics.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Additional information
The original version was revised due to update in Table 1.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Baik, C., Cheng, M.L., Dietrich, M. et al. A Practical Review of Encorafenib and Binimetinib Therapy Management in Patients with BRAF V600E-Mutant Metastatic Non-Small Cell Lung Cancer. Adv Ther 41, 2586–2605 (2024). https://doi.org/10.1007/s12325-024-02839-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-024-02839-4