
Abstract
Cohort effect refers to the social phenomenon that a certain event manifests differently depending on a group that is born in the same year or a similar time period. It is important to understand adolescents’ depressive symptoms vary from generation to generation. We studied the changes of the depressive symptoms during the eighth to tenth grade and examined the difference between the 1997-birth cohort and 2000-birth cohort. The study included 2,070 students (2014–2016 of 2000-birth-cohort data, from 8th to 10th grade, mean age = 12.95–14.95 years) and 2,278 students (2011–2013 of 1997-birth-cohort data, from 8th to 10th grade, mean age = 12.90–14.90 years) who participated in the Korean Children and Youth Panel Survey. Latent growth curve modeling and multi-group analysis were used to compare depressive symptom trajectories between cohorts. The result of comparing the depression levels of the cohorts showed the initial values and change rates verifying the presence of a significant cohort effect—the depression level of the 2000-birth-cohort (initial value = 17.75) was significantly lower than the depression level of the 1997-birth-cohort (initial value = 19.49). This study has significance in that adolescents’ depression has both age and cohort effects. It is speculated that the cohort effect may have been impacted by two major events: The Children Problem-Behavior Screening Questionare Test (mental health screening test), implemented nationwide in 2012, and the Sewol Ferry Disaster, which occurred in 2014. Based on the results, suggestions for future research were discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Depression is a psychological and emotional struggle most commonly experienced during adolescence. According to a survey by Statistics Korea (2018) among adolescents, 30.3% girls and 20.3% boys were found to suffer from depression. The severity of this illness can have a negative impact on adolescents’ psychological and social development—a severe case of it is known to damage psychological and social function (Bandura, 1997), and increase the risk of suicide contemplation by 7.8 times (Kim, 2008a, b). Therefore, it is crucial to provide intervention to adolescents suffering from depression. In this light, many studies have been conducted on this topic—these employed a cross-sectional or longitudinal analysis to verify the vulnerable mental health status of Korean adolescents, and identify the risk factors and protective factors for preventing and reducing cases of depression (Lee & Hoe, 2015; Shine, 2018; Sung 2016). Some of the studies are significant in that they have verified the “age effect” concerning the depression (i.e., changes in this level as Korean adolescents become older) (Kim, 2010; Lim & Choi, 2016). Such a discovery has a high significance because it cannot be verified in a cross-sectional analysis.
However, age effect is not the only factor behind changes in adolescents’ level of depression over time. Considering that humans’ lifecycle goes from birth to early childhood, childhood, and then adolescence to adulthood and, finally, death, it is necessary to verify not only the age effect but also the cohort effect to account for the influential relationship between various events that occur during one’s lifetime. By definition, age effect refers to the outcome or influence one experiences dependent on one’s age—for instance, physical weakness from aging. Cohort effect, on the other hand, refers to the social phenomenon that a certain event manifests differently depending on a group of people born in the same year or roughly in a similar period—for instance, the social environment that baby boomers experienced was different from that of other generations, which affected their level of psychological and social development. As such, both effects can be blended. In particular, a cohort with a unique life experience in its generation may encounter a situation in history and become exposed to a different development process, which may exert an effect distinct from that of simply getting older. In other words, age effect should be differentiated from the cohort effect. However, previous studies have yet to verify the cohort effect separately.
Nonetheless, various studies have provided evidence to show that each cohort experiences different social and environmental elements, and that can lead to discrepancies in psychological and social development (Keyes et al., 2014; Mo et al., 2019; Sohn 2014; Yoo, 2020; Yoo & Chung, 2020). From 2012 onward, South Korea began to carry out the Students’ Children Problem-Behavior Screening Questionare Test (hereafter “the CPSQ Test”) throughout the country to screen and prevent problems in students’ mental health. It can be speculated that there is a discrepancy between the cohort that received such active intervention for mental health and the cohort that did not. The previous studies, social events, and institutions all suggest the level of Korean childrens’ depression may differ depending on the cohort. Therefore, it is necessary to perform an analysis comparing cohorts to determine whether the age effect or cohort effect is at play when conducting a longitudinal study on the level of adolescents’ depression.
1.1 Adolescence and Depression
Adolescence is the period between childhood and adulthood. Depending on the legal standard and scholarly definition, the age range may vary slightly, but it is generally subdivided into three categories: early adolescence (12 to 14 years), middle adolescence (15 to 18 years), and late adolescence (18 to 20 years) in South Korea (Chung, 2004). From the point of lifecycle and age range, adolescence is a time of transitioning from childhood—needing parental care—to young adulthood—leading an independent life. To become adults, adolescents face various physical, psychological, social, and mental developmental tasks not encountered during childhood. In addition, adolescence is also a period during which their self-identity expands (Erikson, 1980). It thus has two possibilities: adolescents can have either a healthy growth by handling the various developmental tasks successfully or an unhealthy growth by experiencing difficulties and failures. Most of all, the health condition during this period has been found to exert a continuous influence on the health in adulthood. Therefore, it is crucial to investigate how adolescents’ health develops and what factors affect it.
Depression originates from the Greek word “melancholia,” which is made up by “melan” (black) and “chole” (bile) (Tellenbach, 1980). Black bile was believed to cause lethargy, drowsiness, worry, and anxiety. Later, the word “depression” came to mean a sad, hopeless state, accompanying symptoms such as a sleep disorder, and increased or decreased weight and appetite (American Psychiatric Association, 2000). Sadness is an emotion that anyone can experience at any point in life. However, a prolonged and severe depression can have a number of negative ramifications—a severe case of depression damages psychological and social function (Bandura, 1997), and raises the risk of suicide contemplation by 7.8 times than in the case of the non-depressed (Kim, 2008a, b). In particular, depression during adolescence has been found to increase the probability of suffering from recurrent depression in adulthood by two to four times (Bhatia & Bhatia, 2007).
1.2 Factors that Influence Depression During Childhood and Adolescence
Factors behind depression during childhood and adolescence can be divided into personal, family, and school study. Personal factors include gender (Akhtar, 2014), exercise time (Kim & Kang, 2017), and sleep time (Shin, 2018). With regard to gender, many precedent studies on depression have verified that compared to male students, the female students suffer more severe depression (Akhtar, 2014; Park et al., 2015). With regard to exercise time, Kim and Kang (2017) verified that adolescents who spent more time exercising were found to have a lower level of depression. In addition, Shin (2018) found that the risk of suffering from depression and contemplating suicide increases among both middle and high school students when their sleep time is less than adequate.
Family factors include family structure (Siddiqui & Sulrana, 2011), household income (Duncan & Brooks-Gunn, 1997), and history of abuse or neglect (Sung, 2016). With regard to family structure, adolescents living with grandparents as guardians have shown a higher level of depression than their counterpart while those living with both parents have shown a lower level of depression than those who do not (Jeon et al., 2012; Siddiqui & Sulrana, 2011). With regard to household income, underprivileged adolescents have a hard time procuring various resources for handling their developmental tasks successfully. This leads to a sense of deprivation and, eventually, causes psychological problems such as depression (Duncan & Brooks-Gunn, 1997; Lim & Choi, 2016). With regard to abuse or neglect, Sung (2016) conducted a study on the effect of parenting attitude on adolescents’ depression, and found that abusive and neglectful behaviors have a serious impact on it.
School study factors include time spent studying (Yoo et al., 2014), relationship with classmates, and relationship with teachers (Cho, 2009; Kim, 2002). With regard to time spent studying, depression is closely related to sleep time and stress (Yoo et al., 2014). In addition, many studies have shown that adolescents who have a deeper connection with their peers and trust them, and those who have a better relationship with teachers have lower levels of anxiety and depression (Cho, 2009; Kim, 2002).
1.3 Necessity for Cohort Study on Adolescents’ Depression Level
Several studies have been carried out to analyze adolescents’ depression. To name a few, Shin (2018) verified the correlation between adolescents’ sleep time and depression. Kim (2010), Lim and Choi (2016) identified risk factors and protective factors for preventing and reducing adolescents’ depression by showing the depression trajectories in a longitudinal study, which has its significance. These study findings support the age effect—that adolescents’ depression level changes as they get older. However, changes in this level do not always depend on this effect. As mentioned earlier, precedent studies have not verified the cohort effect, and it is possible that the influential relationship between various life events in one’s lifetime blend in and manifest both effects. A cohort is a group of people born at a particular time or during a certain period that share the attributes of a specific topic. For a cohort survey, a group of people who have the same life experience is formed. An individual cohort with a unique life experience in its generation can encounter a historic event and become exposed to a development process in a different manner. Thus, they may manifest a different effect unlike the age effect from the simple process of aging.
As a matter of fact, different pieces of evidence have been found to show that a discrepancy can occur between cohorts. In South Korea, Sohn (2014) conducted a study on indirect trauma in two generations: a generation that experienced the 2014 Sewol Ferry Disaster (hereafter “the Disaster”) and a generation that did not. The results showed that the former suffered from a significant level of trauma. Mo et al. (2019) compared cohorts in terms of Korean adolescents’ use of media, and showed that the use of electronic media increased with every generation. Such a cohort effect was also found in other countries. Keyes et al. (2014) took an interest in the fact that therapeutic approaches to depression and anxiety differ from generation to generation, and investigated the cohort effect. Their study found that the level of psychological stress differs depending on cohorts. In South Korea, the CPSQ Test, which was first conducted in 2012 to screen and prevent problems in students’ mental health, may have caused a discrepancy between the cohort that received such active intervention for mental health and the cohort that did not. Yoo (2020) verified that Korean adolescents manifested different levels of life satisfaction and sleep time depending on cohorts. In this light, it is essential to conduct research that verify whether the level of adolescents’ depression varies by cohort or by age when conducting a longitudinal study on depression, which is a grave concern when it comes to adolescents’ mental health.
1.4 Current Study
This study aims to identify the changes of the depressive symptoms during the eighth to tenth grade and examine the difference between the 1997-birth cohort and 2000-birth cohort. The research questions are as follows: (1) Do the trajectories of depression vary depending on cohorts? (2) Does the predictor for the trajectories of depression vary depending on cohorts? (3) Does the size of the predictor for the trajectories of depression vary depending on cohorts?
2 Methods
2.1 Sample
We conducted a comparative analysis on cohorts in terms of the changes in the level of depression among Korean adolescents. For this, we used the following data from the Korean Children and Youth Panel Survey (hereafter “KCYPS”) collected by the National Youth Policy Institute (NYPI): 4th grader cohort (2000-birth-cohort) data from the surveys in 2014, 2015, and 2016, and 7th grader cohort (1997-birth-cohort) data from the surveys in 2011, 2012, and 2013. The Panel Survey, introduced in 2010, is a longitudinal panel survey conducted nationwide. Through multi-stage stratified cluster sampling, the data are organized to represent the country’s population. In particular, KCYPS has compiled data that can be used for comparative cohort analysis because the surveys on 2000-birth-cohort and 1997-birth-cohort were conducted together.
For a longitudinal analysis covering three years, we conducted a comparative analysis on two cohorts (2000-birth-cohort panel in the fifth year of the survey vs. 1997-birth-cohort panel in the second year of the survey), using 8th grade as the base period. To compare cohorts, surveys should be repeated for the same time period. However, a compilation of comparable data at the time of survey was limited, and the data obtained at a certain point in time lacked information on the key variable. Thus, 8th grade was selected as the base period in this study. In other words, from the 2000-birth-cohort panel survey, the fifth-year data indicate 8th grader data, sixth-year data indicate 9th grader data, and seventh-year data indicate 10th grader data. As for the 1997-birth-cohort panel survey, the second-year data indicate 8th grader data, third-year data indicate 9th grader data, and fourth-year data indicate 10th grader data. The total number of study subjects is 2,070 in the 2000-birth-cohort panel and 2,278 in the 1997-birth-cohort panel.
2.2 Measures
2.2.1 Dependent Variable: Depression
To assess the level of depression, we used a revised questionnaire from the symptom check list (SCL-90-R) (Derogatis, 1992) by excluding three of the 13 items measuring depression. The following measuring items were used: “I don’t have much energy,” “I feel unhappy, sad, and depressed,” “I worry a lot,” “I feel like committing suicide,” “I cry often,” “I often think it is my fault when something goes wrong,” “I feel lonely,” “I am not interested in anything,” “My future is not very hopeful,” and “Everything is hard.” Each item was measured on a 4-point Likert scale—In this study, the range from 10 to 40 was indicated, and the depression increases as the score increases. The reliability of the SCL-90-R was 0.76 (Kim & Kim, 1984). The reliability of the tool in this study was as follows: 0.892–0.905 for the 2000-birth-cohort and 0.888–0.906 for the 1997-birth-cohort.
2.2.2 Individual Factors: Gender, Exercise Time, Sleep Time
With regard to gender, one of the personal factors speculated to affect adolescents’ depression, male was coded as “0” and female as “1.” With regard to exercise time, this study used only one question on exercise time during school class. A five-point Likert scale was used (1 = none, 2 = 1 h, 3 = 2 h, 4 = 3 h, 5 = 4 h or more). In other words, a higher score indicates a longer exercise time. With regard to sleep time, we calculated the difference between the hour of going to bed and the hour of waking up, and used the sum of sleep time on school days and non-school days. To avoid over-representation of non-school days, we applied differentiated ratios (school days = 5/7; non-school days = 2/7) before calculating the sum. The unit of sleep time was changed to hours from minutes (e.g., six hours and 30 min ◊ 6.5 h).
2.2.3 Family Factors: Family Structure, Household Income, History of Abuse, History of Neglect
With regard to family structure, the subjects were divided into two groups: “two-parent family” and “single or no-parent family.” The former was coded as “0” and the latter as “1.” With regard to household income, we used annual household income for examining descriptive statistics. For analyzing it as a predictor, a logarithm was used to avoid bias. With regard to abuse and neglect, we used NYPI’s questionnaire by referring to some of the survey questions concerning child abuse in studies done by Huh (2000) and Kim (2003). The level of abuse and neglect were assessed using the following four items, each scored as the mean of four items rated on a four-point Likert scale (1 = never true to 4 = always true). “My parents punish me too harshly when [I] do something wrong,” “My parents always beat me when I do something wrong,” “My parents often punish me harshly to the point [that] I get bruises and scars,” and “My parents say harsh words or insults.” The reliability of the abuse tool in this study was as follows: 0.841 for the 2000-birth-cohort and 0.847 for the 1997-birth-cohort. With regard to neglect, we used the type of treatment that a subject received from his or her parents. The level of neglect was assessed using the following statements: “My parents value other things (their work or external affairs) over me”; “My parents take [an] interest in me and ask me how I am doing in school,” “My parents always make sure that my body, clothes, and beddings are clean,” and “When I get sick, my parents make sure I get proper medical treatment.” The reliability of the neglect tool was as follows: 0.734 for the 2000-birth-cohort and 0.771 for the 1997-birth-cohort.
2.2.4 School Study Factors: Time Spent in Private Learning, Doing School Assignments, Doing Assignments for Private Learning, Doing Extracurricular Activities, and Relationship With Classmates, Relationship with Teachers
With regard to study time, including time spent in private learning, doing school assignments, doing assignments for private learning, and doing extracurricular activities, we measured the amount of time per day and converted the unit of minutes into that of hour for each sub-category. With regard to relationship with classmates and teachers, we used five items from Students’ Life Satisfaction Scale designed by Min (1991). The items concerning relationship with classmates were: “I get along with my classmates,” “When I argue with a friend, I apologize first,” “When a classmate does not have a textbook or materials for class activities, I share with him or her,” “I get disturbed by [my] classmates,” and “During a game or a group activity, my classmates listen to me.” The items concerning relationship with teachers were: “When I see my school teachers, I greet them cheerfully,” “I feel comfortable talking to my teacher(s),” “I am pleased to see my school teacher(s) outside the school premises,” “My teacher is kind to me,” and “I hope my current teacher will be my homeroom teacher next year.” Each statement was measured on a four-point scale from (1) Strongly agree to (4) Strongly disagree. For convenience in interpreting the score, reverse-coding was used—higher scores indicate closer relationship with classmates and teachers. The reliability of the assessment tool for the 2000-birth-cohort was 0.642 for the items concerning relationship with teachers and 0.844 for those concerning relationship with classmates, and for the 1997-birth-cohort was 0.537 and 0.835, respectively.
2.3 Procedures
To address the main research questions of this study, we conducted latent growth modeling (LGM) analysis and multi-group analysis. Specifically, we conducted a conditional model analysis by applying the factor that is speculated to affect Korean adolescents’ depression based on precedent studies. As for the intercept, the factor loading of the initial value was fixed to 1.
Next, we tried to verify the discrepancy in the severity of Korean adolescents’ depression depending on cohorts. For this, we conducted multi-group analysis between the 2000-birth-cohort and 1997-birth-cohort. Multi-group analysis verifies whether the parameters change depending on a group. Because it can verify the cohort effect, conducting this analysis after verifying the age effect on each cohort through LGCM covers both effects at the same time.
As a method of estimation, we used Full Information Maximum Likelihood by taking the bias stemming from mismeasurement into consideration. To determine the fitness of the model, we used the chi-square value, which is an absolute fit index. Considering that this value is sensitive to the number of cases, we used complementary fit indices such as Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), and Incremental Fit Index (IFI). Generally, the model is good when the chi-square value is not significant. Considering the sensitivity to the model complexity and number of subjects to be analyzed, a model with RMSEA under 0.08 and with Incremental Fit Indices (TLI, CFI, IFI) above 0.9 is considered to have a good fitness (Hair et al., 2009). For descriptive statistics analysis, SPSS 27.0 was used, and for analyzing LGM using the structural equation model, AMOS 27.0 was used.
3 Results
3.1 General Attributes of Study Subjects
Table 1 shows the result of analyzing whether demographic attributes of the study subjects differ by cohort. First, we compared the severity of depression between two cohorts: the 2000-birth-cohort (who are 8th graders in 2014, 9th graders in 2015, and 10th graders in 2016) and 1997-birth-cohort (who are 8th graders in 2011, 9th graders in 2012, and 10th graders in 2013). The result showed that the level of depression in the 2000-birth-cohort was lower than the 1997-birth-cohort.
Next, among the personal factors, with respect to exercise time, the 2000-birth-cohort (mean = 3.27) had significantly more of it than the 1997-birth-cohort (mean = 3.03), (t = 6.02, p < 0.001), and with respect to sleep time, the 2000-birth-cohort (mean = 7.97) had significantly less of it than the 1997-birth-cohort (mean = 8.17), (t = − 6.85, p < 0.001).
Among the family factors, the 2000-birth-cohort had experienced a significantly lower level of abuse (mean = 6.55) and neglect (mean = 7.13) than the 1997-birth-cohort —abuse (mean = 7.37) and neglect (mean = 7.48); (t = − 10.08, p < 0.001; t = − 5.04, p < 0.001).
Among the school study factors, the 2000-birth-cohort had spent significantly less time doing school assignments (mean = 0.48), assignments for private learning (mean = 0.56), and extracurricular activities (mean = 0.72) than the 1997-birth-cohort —doing school assignments (mean = 0.68), assignments for private learning (mean = 0.63), and extracurricular activities (mean = 0.96); (t = − 12.19, p < 0.001; t = − 3.46, p < 0.01; t = − 8.49, p < 0.001). Furthermore, the 2000-birth-cohort showed a significantly closer relationship with classmates (mean = 15.68) and teachers (mean = 14.66) than the 1997-birth-cohort —relationship with classmates (mean = 15.09) and relationship with teachers (mean = 14.02); (t = 9.38, p < 0.001; t = 6.63, p < 0.001).
3.2 Difference in the Trajectories of Depression by Cohorts
3.2.1 Multi-Group Analysis on Unconditional Model: Difference Based on Cohort
Table 2 shows the result of conducting multi-group analysis on the unconditional model to verify whether the trajectories of depression differ between the two cohorts. This analysis requires the comparison between equivalence constraint model (each group is postulated to have same parameters) and non-constraint model (each group is postulated to have different parameters without any constraints). In the unconditional model analysis, we compared the non–constraint model with equivalence constraint model in terms of the structural mean of each group. The result showed a meaningful difference in the trajectories of depression in the two cohorts.
Table 3 shows the estimated parameters of the unconditional model. For the 2000-birth-cohort, the mean of the initial values was 17.750 (p < 0.001) and that of the change rates 0.068 (p > 0.05). By the time they were 8th graders, their depression level was 17.750 on average. It rose by 0.068 times every year, but the increase was not significant. For the 1997-birth-cohort, the mean of the initial values was 19.487 (p < 0.001) and that of the change rates − 0.253 (p < 0.001). Their average level of depression in 8th grade was 19.487. Over time, it decreased by 0.253 times.
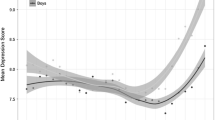
The depression trajectories differed significantly not only between the two cohorts but also among the subjects in each. First, with regard to the difference among the subjects within each cohort, the 2000-birth-cohort’s initial value variate was 20.043 (p < 0.001) and change rate variate was 2.061 (p < 0.001), while the same for 1997-birth-cohort was 23.482 (p < 0.001) and 3.816 (p < 0.001), respectively, which confirmed individual differences on the trajectories of depression for both cohorts. With regard to the difference between the two, they showed a significant difference in terms of the intercept of depression (initial value of depression2000 − birth−cohort = 17.750, initial value of depression1997 − birth−cohort = 19.487; critical ratio for difference = 9.888) and the slope (depression change rate2000 − birth−cohort = 0.068, depression change rate1997 − birth−cohort = –0.253; critical ratio for difference = − 3.383). To be specific, when those in the 2000-birth-cohort became 8th graders, they initially experienced a lower level of depression than the 1997-birth-cohort. However, over time, the 1997-birth-cohort’s depression level decreased at a faster rate than that of the 2000-birth-cohort. Subsequently, the gap in the depression levels between the two decreased (See Fig. 1).

Depressive symptom trajectories according to birth cohorts
3.2.2 Multi-Group Analysis on Conditional Model: Difference Based on Cohort
Table 4 shows the result of conducting multi-group analysis on the conditional model to verify the relations between the trajectories of depression and predictor, and to verify whether such a correlation is observed in the difference between the two cohorts. In this analysis, we first put the constraint of structural weight on each group, and compared the constraint model with the non-constraint model. The result indicate a significant difference in the conditional model between the two cohorts.
Table 5 shows the estimated parameters of the conditional model. The key findings can be summarized as follows: (1) With regard to gender, female subjects had a higher initial value of depression than male subjects in both cohorts (\({\upbeta }\)2000−birth−cohort = 0.189, p < 0.001;\({\upbeta }\)1997−birth−cohort = 0.268, p < 0.001). Thus, gender was found to create the gap in the initial values of depression between the two. In addition, this gap was maintained on the slopes in both cohorts even over time. What is notable is that the effect of gender on the initial value of depression differed between the cohorts (C.R.D. = 2.875), which verified that the initial value of depression differed by gender between the two. (Compared with the past generations, the gender-based gap in the initial value of depression has decreased recently). (2) The exercise time during school class was found to have no correlation with the depression levels of both cohorts. (3) The 2000-birth-cohort subjects who slept more had a lower initial value of depression than those who slept less (\({\upbeta }\) = − 0.085, p < 0.001). However, those who slept more had a faster rate of increase in depression level than those who slept less (\({\upbeta }\) = 0.229, p < 0.05). Thus, the gap in the initial values based on sleep time differed within the cohort and decreased over time. In contrast, sleep time was found to have no correlation with the depression level in the 1997-birth-cohort.
With regard to the family factors, the following observations were made: (1) Family structure was found to have no correlation with depression in either cohort. (2) The depression level in the 2000-birth-cohort was not related to household income, while in the 1997-birth-cohort, the initial value of depression of those with a bigger household income was lower than that of those with a smaller household income (\({\upbeta }\) = − 0.066, p < 0.05)—however, household income did not affect the change rate (\({\upbeta }\) = − 0.004, p = 0.942); it thus generated the gap in the initial values of depression within the group while maintaining the initial value over time. (3) Those who experienced abuse had a high initial value of depression in both cohorts (\({\upbeta }\)2000−birth−cohort = 0.279, p < 0.001; \({\upbeta }\)1997−birth−cohort = 0.324, p < 0.001)—those experiencing more severe abuse showed a slower increase rate in depression in the 2000-birth-cohort (\({\upbeta }\) = − 0.644, p < 0.001) and a faster decrease rate in depression in the 1997-birth-cohort (\({\upbeta }\) = − 0.350, p < 0.001); therefore, the gap in the initial values of depression based on abuse decreased in both cohorts over time. (4) Those in the 2000-birth-cohort experiencing neglect more frequently had a higher initial value of depression than those experiencing it less frequently (\({\upbeta }\) = 0.117, p < 0.001), while neglect was not related to the change rate (\({\upbeta }\) = − 0.087, p = 0.465); thus, the gap in the initial values based on neglect was maintained at the same level over time. In the 1997-birth-cohort, on the other hand, those experiencing neglect more frequently had a higher initial value of depression than those experiencing it less frequently (\({\upbeta }\) = 0.153, p < 0.001); those with a more frequent exposure to neglect had a faster decrease rate (\({\upbeta }\) = − 0.115, p < 0.05), and thus, the gap in the initial values based on neglect decreased over time.
With respect to the school study factors, the results were as follows: (1) The time spent in private learning had no significant relationship with depression in either cohort. What is notable here is that the size of the effect that private learning time exerted on the initial value of depression differed significantly between the cohorts (C.R.D. = 2.002). This verified the difference in the initial values of depression based on time spent in private learning between the two. (Among the past generations, those who spent more time in private learning had the tendency to suffer from more severe depression; among the newer generations, however, those who spend more time in private learning tend to suffer from less severe depression.) (2) The time spent doing school assignments and assignments for private learning showed no correlation with depression in either cohort. (3) Those in the 2000-birth-cohort who spent more time doing extracurricular activities had a lower initial value of depression than those who spent less time (\({\upbeta }\) = − 0.055, p < 0.05), but the time spent doing extracurricular activities was not related to the change rate (\({\upbeta }\) = 0.144, p = 0.208). Thus, the gap in the initial values based on this time was maintained over time. On the other hand, the time spent doing extracurricular activities showed no correlation with depression in the 1997-birth-cohort. (4) In both cohorts, those who had a closer relationship with classmates had a low initial value of depression (\({\upbeta }\)2000−birth−cohort = − 0.374, p < 0.001; \({\upbeta }\)1997−birth−cohort = − 0.261, p < 0.001). Furthermore, 2000-birth-cohort subjects with a better relationship with classmates showed a faster increase rate in depression (\({\upbeta }\) = 0.506, p < 0.001), while 1997-birth-cohort subjects with a better relationship with classmates showed a slower decrease rate in depression (\({\upbeta }\) = 0.219, p < 0.001). Thus, the gap in initial values of depression based on relationship with classmates decreased over time in both cohorts. (5) The 2000-birth-cohort subjects who had a better relationship with teachers had a low initial value of depression (\({\upbeta }\) = − 0.083, p < 0.01), and relationship with teachers was not related to the change rate (\({\upbeta }\) = − 0.084, p = 0.495); thus, the gap in the initial values based on relationship with teachers was maintained over time. In the 1997-birth-cohort, on the other hand, relationship with teachers had no correlation with depression.
4 Discussion
For a longitudinal study covering three years, we carried out a comparative analysis on the level of depression among the 2000-birth-cohort and 1997-birth-cohort using 8th as the base grade. For this, we used the data on the two cohorts from the KCYPS collected by the NYPI—the 2000-birth-cohort data were taken from the fifth survey (2014), sixth survey (2015), and seventh survey (2016); the 2000-birth-cohort data were taken from the second survey (2011), third survey (2012), and fourth survey (2013). Using this data, we conducted LGCM analysis and multi-group analysis. The key findings and their implications are as follows.
First, we examined the trajectories of depression in the two cohorts—in the 2000-birth-cohort, it was maintained without any significant change, while in the 1997-birth-cohort, it showed a decline.
Second, the result of comparing the depression levels of the cohorts showed the initial values and change rates verifying the presence of a significant cohort effect in both—the depression level of the 2000-birth-cohort in the year its subjects became 8th graders were significantly lower than the depression level of the 2000-birth-cohort in the year its subjects were 8th graders. In addition, the change rate of the 2000-birth-cohort was not significant, whereas that of the 1997-birth-cohort decreased significantly. Despite the difference in change rate, the cohort effect was verified.
This result indicates a significant difference in the trajectories of depression depending on cohorts. This is a new finding, which could not be verified in precedent studies on adolescent depression, and it implies that the depression level had a cohort effect when age was controlled. Increased consideration should be given to the phenomenon of the depression level of a newer generation (2000-birth-cohort) decreasing compared with that of an older generation (1997-birth-cohort), thus decreasing the gap in the depression levels between the cohorts. This implies that the newer generation’s mental health has improved compared with the older generation’s, and that the positive effect eventually diminishes over time. With respect to the cohort effect of both in terms of the initial value and change rate, the following explanations can be given. First, with regard to the decreased level of depression in the newer generation of 8th graders compared with the older generation, it is speculated to be the effect of preventative mental health programs for Korean adolescents—tests were conducted among children and adolescents to examine their mental health. The CPSQ measures problem behavior types: internalization (anxiety, depression, stress, friendship), externalization (ADHD, defiant behavior disorder, conduct disorder), cognition (learning), misuse (drugs, Internet), psychosomaticization (convulsions, tics, eating disorders) were made into five sub-domains; responses were made on a 4-point scale (Ministry of Education, 2018). Students selected by the CPSQ are classified into ‘normal’ and ‘interested’. Specifically, students who need a second screening test because their total score on emotional and behavioral problems is higher than the standard score is selected as an ‘interested group.’ This ‘interest group’ is again managed by dividing it into ‘general management group’ and ‘priority management group’ with high problem severity, and is guided to receive diagnosis and treatment at local mental health promotion centers and specialized hospitals (Ministry of Education, 2018). The Ministry of Education applied CPSQ for elementary school students and AMPQ (Adolescent Mental-health Problem-behavior Questionnaire) for middle school students to test students’ mental health problems in 96 schools nationwide, and named it ‘Student Emotion and Behavior Screening Test.’ After a pilot, the CPSQ Test was implemented throughout the country from 2012 onward. In other words, some cohorts received active intervention for mental health such as CPSQ, while others did not. The status of such intervention can create a noticeable discrepancy. What is interesting is that the 2000-birth-cohort subjects represent the condition of adolescents from 2014 to 2016, which is after the implementation of the CPSQ Test. The 1997-birth-cohort, on the other hand, represents the condition of adolescents from 2011 to 2013 before the implementation of the CPSQ Test. In other words, it can be said that the 2000-birth-cohort must have received active intervention since 2012, whereas the 1997-birth-cohort is less likely to have. Such difference may have lowered the depression level significantly among the newer generation of 8th graders (the 2000-birth-cohort) compared with the older generation (the 1997-birth-cohort). This cohort effect has manifested similarly in the life satisfaction of adolescents. Yoo (2020) conducted a comparative cohort analysis on Korean adolescents’ life satisfaction, and verified the cohort effect between the cohorts before and after conducting the CPSQ Test.
Along with this, the phenomenon of the gap in the depression levels based on the cohorts of 8th graders diminishing over time (note: the depression level of the newer generation increased insignificantly from 8th grade) may be associated with the Disaster. Sohn (2014) conducted a study on indirect trauma in the generation that experienced the Disaster and the generation that did not—the result showed that 57.5% of the cohort of the Disaster suffered from a significant level of an indirect post-traumatic stress disorder even though they did not experience the tragedy directly. In the present study, the 2000-birth-cohort (2014–2016) had already experienced the Disaster as 8th graders, while the 1997-birth-cohort (2011–2013) had not. In other words, the newer generation (the 2000-birth-cohort) initially manifested a lower level of depression as 8th graders, with this level increasing insignificantly over time unlike other generations’; this phenomenon can be seen as a cohort effect between the generation that experienced the Disaster and the generation that did not.
Third, we conducted conditional model analysis and multi-group analysis to examine the effect of predictor on the trajectories of depression and to verify the difference in cohorts in terms of the relationship between the predictor and trajectories of depression. The result showed that depending on the predictor of the depression trajectory, there was a discrepancy within each cohort as well as between the two cohorts.
First, findings related to the personal factors were: (1) Gender was found to cause a discrepancy in the initial value of depression within both groups, as female 8th graders had higher initial values of depression than their male counterparts. In addition, such gender-based discrepancy in the initial value of depression was maintained in both cohorts over time. This is in line with the previous study finding that the depression of female students is greater than male students (Akhtar, 2014; Park et al., 2015). Therefore, when conducting interventions against negative psychological emotions, it is necessary to put more focus on female students. What is notable here is that the effect size of gender on the initial value of depression is considerably greater in the 1997-birth-cohort than in the 2000-birth-cohort. In other words, the gender-based discrepancy in depression level is less noticeable in the newer generation than in the older one. This implies that gender-focused intervention has been effective to an extent. Nevertheless, interventions focusing on female students should be continued because gender-based discrepancy in depression level still exist within each group. (2) Exercise time was not significantly related to depression in either cohort. (3) Sleep time exerted a meaningful effect on the depression level in the 2000-birth-cohort but not in the 1997-birth-cohort —those in the former who slept more showed a significantly lower level of depression in the 8th grade. This result supports the previous finding in Shin (2018)’s study that sleeping for less than the ideal amount of time can increase the depression level. In the meantime, it is necessary to conduct further research on the phenomenon of sleep time not showing any significant correlation with depression in the older generation (the 1997-birth-cohort) while exerting an essential effect on the depression level in the newer generation (the 2000-birth-cohort). In other words, investigation should be carried out to verify whether there is a difference in sleep time depending on cohorts of Korean adolescents, and to identify the factor that creates such a discrepancy.
Next, findings related to the family factors were: (1) Family structure was found to have no correlation with depression in either cohort. (2) Household income showed a significant correlation with depression in the 1997-birth-cohort but did not exert any significant effect on it in the 2000-birth-cohort — 1997-birth-cohort subjects with a bigger household income showed a lower level of depression than those with a smaller household income. The discrepancy was maintained over time. This result matches the previous study finding that smaller household income makes it difficult for adolescents to acquire resources for completing their developmental tasks successfully, thus causing a sense of deprivation, which eventually leads to psychological problems such as depression (Duncan & Brooks-Gunn, 1997; Lim & Choi, 2016). In the meantime, the level of depress+ion caused by physical deprivation was not significant in the newer generation compared with the older one. (3) Both abuse and neglect were found to be factors exerting a negative influence on adolescents’ depression in the two cohorts—subjects experiencing abuse and neglect more frequently showed a higher level of depression in 8th grade; in the 2000-birth-cohort, the discrepancy in the depression level based on abuse gradually decreased over time, while that based on neglect was maintained over time. In the 1997-birth-cohort, the discrepancy in the depression level based on abuse and neglect decreased over time. This result is in line with the finding from Sung (2016)’s study that parents’ abusive and neglectful behaviors have a great impact on their children’s depression. Therefore, it is important to provide parenting education to would-be parents and carefully check in with families whether their children are exposed to abuse or neglect.
Last, findings related to the school study factors were: (1) Time spent in private learning, doing school assignments, and doing assignments for private learning did not have a significant correlation with depression in either cohort. However, the effect of time spent in private learning on the initial value of adolescents’ depression was considerably different between the cohorts in terms of direction—newer generation subjects who spent more time in private learning showed a lower level of depression, while older generation subjects who did the same showed a higher level of depression. This result can be interpreted as follows. In the past, time spent in private learning acted as a stressor and increased the level of depression; in recent years, students can reduce their stress related to school study by improving their grades through private learning. This is speculated to lower the level of depression. (2) The time spent doing extracurricular activities was significantly related to the depression in the 2000-birth-cohort, whereas it had no essential correlation with depression in the 1997-birth-cohort —those in the former who spent more time doing extracurricular activities had a lower level of depression in 8th grade than those who spent less time. The discrepancy was maintained over time. This result is similar to the aforementioned finding about the newer generation that contradicts the finding about the older generation regarding the effect of time spent in private learning on depression. In the newer generation, time spent studying can be seen as a factor that reduces anxiety about academic performance, as well as depression level. On the other hand, extracurricular activities were found to be inversely correlated to levels of depression and anxiety in the newer generation. Meaning, an increase in time spent on extracurricular activities showed decreased levels in depression, while other school study factors were not; with regard to the phenomenon, it can be speculated that “school-record-based student selection” played a part. This selection is a newly implemented system to reflect grades and extracurricular activities in the screening of college applicants. Thus, “time spent in learning other things” can apply. In other words, for the newer generation, engaging in extracurricular activities is advantageous in scoring high in the college application screening because as time spent in extracurricular activities increases, the levels of anxiety and depression decrease.
This result can be interpreted as follows. In the older generation, stress level rose as study time increased. However, the newer generation, which feels greater stress over academic performance than the physical stress related to study time, is more motivated to reduce the stress related to grades than the physical stress. In fact, according to the study by Song et al. (2014), there was a significant difference in the levels of stress and depression among elementary and middle school students depending on the level of academic performance. It should, however, be noted that time spent in private learning could cause other types of stress (competition, sleep deprivation), while it can also be a choice for lowering the stress related to school studies. With regard to the phenomenon of depression decreasing with increase in study time, it can be speculated that Korean children and adolescents have no choice but to tolerate other types of stress to reduce the more serious one. Therefore, it is necessary to carefully investigate the interplay of adolescents’ depression with time spent in private learning, academic performance, and stress related to school studies. (3) Relationship with classmates and teachers was found to exert a positive and important influence on adolescents’ depression in both cohorts—those who had a better relationship with classmates and teachers had a lower level of depression in 8th grade. This result is similar to the finding of previous studies that adolescents who have a deeper connection with peers and trust them, and those who have a better relationship with teachers have lower levels of anxiety and depression (Cho, 2009; Kim, 2002). In other words, it is crucial for adolescents to have a good relationship with their peers and teachers at school. Therefore, it is essential to check if adolescents are bullied or alienated in school and provide guidance, while creating a good study environment and school atmosphere as a foundation for positive relationships.
5 Conclusion
This study analysed how Korean adolescents’ depression level changes over time and whether such change is manifested among cohorts. The result led to a new discovery that adolescents’ depression has both age and cohort effects. It is speculated that the cohort effect may have been impacted by two major events: the CPSQ Test, implemented nationwide in 2012, and the Disaster, which occurred in 2014. In addition, this effect was found in the relationships between gender and depression and study time and depression. Such findings imply that intervention programs for the mental health of children and adolescents need to consider the social environment and systems (e.g., mental health screening and national disasters) that can change from generation to generation. The findings also imply that the generation experiencing the COVID-19 pandemic this year is likely to manifest a cohort effect in various areas distinct from past generations. Therefore, such a cohort effect should be further investigated and analyzed from multiple perspectives. Our findings are expected to provide helpful insights to consider the cohort effect ensuing from various social events, policies, and systems when establishing the basis for developing an intervention for adolescents’ psychological, physical, social, and mental health.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
References
Akhtar, A. (2014). A comparative study of depression among adolescents in relation to gender, domicile and family type: with special reference to Kashmir. Indian Journal of Health and Wellbeing, 5(3), 395–397.
American Psychiatric Association. (2000). DSM-IV-TR: Diagnostic and statistical manual of mental disorders, text revision. American Psychiatric Association.
Bandura, A. (1997). Self-efficacy. The exercise of control. W.H. Freeman and Co.
Bhatia, S. K., & Bhatia, S. C. (2007). Childhood and adolescent depression. American Family Physician, 75, 73–80.
Cho, J. A. (2009). The effects of parents, peers and teachers upon changes in mental health on the part of adolescents: a focused on depression and anxiety. Studies on Korean Youth, 20(3), 167–192.
Chung, O. (2004). Understanding youth development. Hagjisa.
Derogatis, L. R. (1992). SCL-90-R. Administration, scoring and procedures manual - II for the revised version (Vol. Second). Clinical Psychometric Research, Inc.
Duncan, G., & Brooks-Gunn, J. (1997). Consequences of growing up poor. Russell Sage Foundation.
Erikson, E. H. (1980). Identity and the life cycle (Vol. 1). WW Norton & Company.
Hair, J. F., Anderson, R. E., Tatham, R. L., & Black, W. C. (2009). Multivariate data analysis. Prentice Hall.
Huh, M. Y. (2000). The study for the development and validation of ‘parenting behavior inventory’ perceived by adolescent. Unpublished doctoral dissertation, Ewha Womans University, Seoul, Korea. Retrieved from http://www.riss.kr/link?id=T10397901. Accessed 18 Apr 2022
Jeon, G. S., Park, S. Y., & Cho, S. (2012). Gender differences in correlates of depression and suicidal ideation among Korean adolescents. The Korean Journal of Health Service Management, 6(4), 295–308.
Keyes, K. M., Nicholson, R., Kinley, J., Raposo, S., Stein, M. B., Goldner, E. M., & Sareen, J. (2014). Age, period, and cohort effects in psychological distress in the United States and Canada. American Journal of Epidemiology, 179(10), 1216–1227.
Kim, A. G. (2002). The relationships among perceived parenting attitudes, social supports, and depression and externalizing problems of early adolescents. The Korean Journal of Educational Psychology, 16(3), 31–50.
Kim, H. (2008a). The structural relationships of stress, hopelessness, and depression to suicidal ideation in the elderly and the adolescents. Unpublished doctoral Dissertation, Dankook University, Seoul, Korea.
Kim, Y. B. (2008b). Correlates of depressive symptoms and suicidal ideation among Korean adults. Unpublished doctoral Dissertation, Cheju National University, Korea.
Kim, J. H., & Kim, K. (1984). The standardization study of symptom Checklist-90-revision in Korea. Mental Health Research, 2, 278–311.
Kim, M., & Kang, S. (2017). Mediation effect of ego-resilience in the impact of exercise hours during physical education class on adolescents’ level of depression. The Korean Journal of Physical Education, 56(3), 193–202.
Kim, S. W. (2003). The effect of social support on abused children’s adjustment. Unpublished master’s thesis. Seoul National University, Seoul, Korea. Retrieved from http://www.riss.kr/link?id=T8876131. Accessed 18 Apr 2022
Kim, S. W. (2010). The heterogeneous developmental trajectories of adolescent depression and their predictors focusing on gender differences. Studies on Korean Youth, 21(1), 171–192.
Lee, S., & Hoe, M. (2015). The analysis of longitudinal causal relationship between depression and delinquency in adolescents. Journal of Youth Welfare, 17(2), 241–264.
Lim, H., & Choi, S. (2016). Developmental trajectories and predictors of adolescent depression: a short-term study. The Korean Journal of Psychology: General, 35(3), 455–480.
Min, B. S. (1991). Effect of school adjustment and self-concept on school achievement. Unpublished master’s thesis, Hongik University, Seoul, Korea. Retrieved from http://www.riss.kr/link?id=T2167733. Accessed 18 Apr 2022
Ministry of education (2018). Student emotion and behavior screening test and management manual. http://mom.eduro.go.k. Accessed 18 June 2021
Mo, S. H., Lee, J., & Han, J. H. (2019). Comparison of cohort to youth media usage trend. http://www.nypi.re.kr. Accessed 18 June 2020
Park, S. H., Yang, J. N., & Choi, E. J. (2015). The relationship among stress, depression, and suicidal ideation in adolescents residing in low-income areas -focused on the mediating effect of depression. Korean Journal of Youth Studies, 22(5), 301–323.
Siddiqui, R. Z., & Sultana, S. (2011). Single parenting a risk factor for depression in adolescents. Pakistan Journal of Psychology, 42(1), 87–100.
Shin, E. (2018). Association between self-reported sleep duration and depression or suicidal ideation in Korean adolescents. Anxiety and Mood, 14(1), 21–27.
Sohn, S. H. (2014). Study of indirect trauma and related variables by social traumatic event to the adolescence: Focusing on the Sewol Ferry Disaster. Korean Journal of Youth Studies, 21(10), 269–294.
Song, Y., Lee, S. S., Kim, D. H., Ham, K. A., & Lee, D. H. (2014). The differences of depression, anxiety, and stress according to academic performance and home economic status among elementary and middle school students. The Journal of Educational Research, 12(1), 29–50.
Statistics Korea (2018). 2018 Statistics on the youth. Retrieved from http://kostat.go.kr. Accessed 18 Apr 2022
Sung, J. M. (2016). The longitudinal factors on depression in Korean adolescents. Journal of Youth Welfare, 18(4), 93–111.
Tellenbach, H. (1980). Melancholy: History of the problem, endogeneity, typology, pathogenesis, clinical considerations. Duquesne University Press.
Yoo, C. (2020). Korean adolescents’ life satisfaction cohort differences caused by mental health intervention and social disaster accident. Child Indicators Research, 13(5), 1875–1892.
Yoo, C., & Chung, I. J. (2020). A comparative study of cohorts for children’s body mass index changes. Social Work in Public Health, 35(4), 213–222.
Yoo, C., Kahng, S. K., & Kim, S. Y. (2014). Relationship between academic stresses and internalization, externalization among adolescents: Mediating effects of self-efficacy and gender differences. Korean Journal of Social Welfare Studies, 45(3), 237–262.
Funding
This study was funded by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (2020S1A5A8040660).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board of Hannam University (No: 2020-E-01-02).
Informed Consent
All participants signed anonymous consent to participate in both studies. All authors consent to the publication of this paper.
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yoo, C. The Birth Cohorts Difference in Depression. Child Ind Res 16, 997–1017 (2023). https://doi.org/10.1007/s12187-022-09985-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12187-022-09985-7