
Abstract
Purpose of Review
This article reviews the current imaging role of 18F–fluordeoxyglucose positron emission computed tomography (18F–FDG-PET/CT) combined with cardiac CT angiography (CTA) in infective endocarditis and discusses the strengths and limitations of this technique.
Recent Findings
The diagnosis of infective endocarditis affecting prosthetic valves and intracardiac devices is challenging because echocardiography and, therefore, the modified Duke criteria have well-recognized limitations in this clinical scenario. The high sensitivity of 18F–FDG-PET/CT for the detection of infection associated with the accurate definition of structural damage by gated cardiac CTA in a combined technique (PET/CTA) has provided a significant increase in diagnostic sensitivity for the detection of IE.
Summary
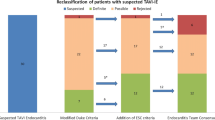
PET/CTA has proven to be a useful diagnostic tool in patients with suspected infective endocarditis. The additional information provided by this technique improves diagnostic performance in prosthetic valve endocarditis when it is used in combination with the Duke criteria. The findings obtained in PET/CTA studies have been included as a major criterion in the recently updated diagnostic algorithm in infective endocarditis guidelines.






Similar content being viewed by others


References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Fernández-Hidalgo N, Tornos Mas P. Epidemiology of infective endocarditis in Spain in the last 20 years. Rev Esp Cardiol. 2013;66:728–33.
Habib G. Management of infective endocarditis. Heart. 2006;92:124–30.
Duval X, Selton-Suty C, Alla F, et al. Endocarditis in patients with a permanent pacemaker: a 1-year epidemiological survey on infective endocarditis due to valvular and/or pacemaker infection. Clin Infect Dis. 2004;39:68–74.
Habib G, Badano L, Tribouilloy C, Vilacosta I, Zamorano JL. Recommendations for the practice of echocardiography in infective endocarditis. Eur Heart J. 2010;11:202–19.
Stumpe KD, Dazzi H, Schaffner A, von Schulthess GK. Infection imaging using whole-body FDG-PET. Eur J Nucl Med. 2000;27:822–32.
Gamelli RL, Liu H, He LK, Hofmann CA. Augmentations of glucose uptake and glucose transporter-1 in macrophages following thermal injury and sepsis in mice. J Leukoc Biol. 1996;59:639–47.
Jamar F, Buscombe J, Chiti A, et al. EANM/SNMMI guideline for 18F-FDG use in inflammation and infection. J Nucl Med. 2013;54:647–58.
•• Saby L, Laas O, Habib G, et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J Am Coll Cardiol. 2013;61:2374–82. The use of 18 F-FDG-PET/CT is helpful for diagnosing prosthetic valve endocarditis. The results of this study supported for the first time addition of abnormal FDG uptake as a novel major criterion for prosthetic valve endocarditis.
Bensimhon L, Lavergne T, Hugonnet F, et al. Whole body [18F]fluorodeoxyglucose positron emission tomography imaging for the diagnosis of pacemaker or implantable cardioverter defibrillator infection: a preliminary prospective study. Clin Microbiol Infect. 2011;17:836–44.
•• Sarrazin JF, Philippon F, Tessier M, et al. Usefulness of fluorine-18 positron emission tomography/computed tomography for identification of cardiovascular implantable electronic device infections. J Am Coll Cardiol. 2012;59:1616–25. 18 F-FDG-PET/CT is useful for differentiating between cardiac device infection and recent post-implant changes. It increases the diagnostic capability and may guide appropriate therapy.
Graziosi M, Nanni C, Lorenzini M, et al. Role of 18F-FDG PET/CT in the diagnosis of infective endocarditis in patients with an implanted cardiac device: a prospective study. Eur J Nucl Med Mol Imaging. 2014;41:1617–23.
Feuchtner GM, Stolzmann P, Dichtl W, et al. Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J Am Coll Cardiol. 2009;53:436–44.
Entrikin DW, Gupta P, Kon ND, Carr JJ. Imaging of infective endocarditis with cardiac CT angiography. J Cardiovasc Comput Tomogr. 2012;6:399–405.
Gahide G, Bommart S, Demaria R, et al. Preoperative evaluation in aortic endocarditis: findings on cardiac CT. AJR Am J Roentgenol. 2010;194:574–8.
•• Pizzi MN, Roque A, Fernández-Hidalgo N, et al. Improving the diagnosis of infective endocarditis in prosthetic valves and intracardiac devices with 18F-FDG-PET/CT-angiography: initial results at an infective endocarditis referral center. Circulation. 2015;132:1113–26. 18 F-FDG-PET/CT improves the diagnostic accuracy of the modified Duke criteria in patients with suspected infective endocarditis and prosthetic valves or cardiac devices, as was seen in previous series. This study found that PET/CTA yields the highest diagnostic performance and provides additional diagnostic benefits. Hence, the use of CTA in combination with PET images should be always encouraged in the evaluation of patients with IE.
Habib G, Lancellotti P, Antunes MJ, et al. ESC guidelines for the management of infective endocarditis. The task force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36:3075–23.
Soussan M, Brillet P-Y, Nunes H, et al. Clinical value of a high-fat and low-carbohydrate diet before FDG-PET/CT for evaluation of patients with suspected cardiac sarcoidosis. J Nucl Cardiol. 2013;20:120–7.
Manabe O, Yoshinaga K, Ohira H, et al. The effects of 18-h fasting with low-carbohydrate diet preparation on suppressed physiological myocardial 18F-fluorodeoxyglucose (FDG) uptake and possible minimal effects of unfractionated heparin use in patients with suspected cardiac involvement sarcoidosis. J Nucl Cardiol. 2016;23:244–52.
Mc Ardle BA, Leung E, Ohira H, et al. The role of F18-fluorodeoxyglucose positron emission tomography in guiding diagnosis and management in patients with known or suspected cardiac sarcoidosis. J Nucl Cardiol. 2013;20:297–306.
Leccisotti L, Perna F, Lago M, et al. Cardiovascular implantable electronic device infection: delayed vs standard FDG PET-CT imaging. J Nucl Cardiol. 2014;21:622–32.
Ellis JH, Cohan RH. Reducing the risk of contrast-induced nephropathy: a perspective on the controversies. AJR Am J Roentgenol. 2009;192:1544–9.
Abbara S, Arbab-Zadeh A, Callister TQ, et al. SCCT guidelines for performance of coronary computed tomographic angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2009;3:190–204.
Ahmed FA, James J, Tout D, Arumugam P, Mamas M, Zaidi AM. Metal artefact reduction algorithms prevent false positive results when assessing patients for cardiac implantable electronic device infection. J Nucl Cardiol. 2015;22:219–20.
Memmott MJ, James J, Armstrong IS, Tout D, Ahmed F. The performance of quantitation methods in the evaluation of cardiac implantable electronic device (CIED) infection: a technical review. J Nucl Cardiol. 2015; doi:10.1007/s12350-015-0293-2.
Bucerius J, Mani V, Moncrieff C, et al. Optimizing 18F-FDG PET/CT imaging of vessel wall inflammation: the impact of 18F-FDG circulation time, injected dose, uptake parameters, and fasting blood glucose levels. Eur J Nucl Med Mol Imaging. 2014;41:369–83.
Rundstrom H, Kennergren C, Andersson R, Alestig K, Hogevik H. Pacemaker endocarditis during 18 years in Goteborg. Scand J Infect Dis. 2004;36:674–9.
Klug D, Lacroix D, Savoye C, et al. Systemic infection related to endocarditis on pacemaker leads: clinical presentation and management. Circulation. 1997;95:2098–107.
Tlili G, Amroui S, Mesguich C, et al. High performances of 18F-fluorodeoxyglucose PET-CT in cardiac implantable device infections: a study of 40 patient. J Nucl Cardiol. 2015;22:800–3.
• Cautela J, Alessandrini S, Cammilleri S, et al. Diagnostic yield of FDG positron-emission tomography/computed tomography in patients with CEID infection: a pilot study. Europace. 2013;15:252–7. This study indicates that 18 F-FDG-PET/CT is highly accurate for the diagnosis of skin and pocket device infection, but much less accurate for detecting lead vegetations in infective endocarditis. The reliability of 18 F-FDG-PET/CT findings in management and decision-making may vary according to the type of device infection.
Ahmed FZ, James J, Cunnington C, et al. Early diagnosis of cardiac implantable electronic device generator pocket infection using 18F-FDG-PET/CT. Eur Heart J Cardiovasc Imaging. 2015;16:521–30.
Nishimura RA, Otto CM, Bonow RO, et al. AHA/ACC guideline for the management of patients with valvular heart disease. J Am Coll Cardiol. 2014;22:57–185.
Engelfriet P, Boersma E, Oechslin E, et al. The spectrum of adult congenital heart disease in Europe: morbidity and mortality in a 5 year follow-up period—the Euro Heart Survey on adult congenital heart disease. Eur Heart J. 2005;26:2325–33.
Loureiro-Amigo J, Fernández-Hidalgo N, Pijuan-Domènech A, et al. Infective endocarditis in adult patients with congenital heart disease. Experience from a reference centre. Enferm Infecc Microbiol Clin. 2016; pii: S0213-005X(16)00029-X doi:10.1016/j.eimc.2016.01.004.
Saiman L, Prince A, Gersony WM. Pediatric infective endocarditis in the modern era. J Pediatr. 1993;122:847–53.
Scholtens AM, Van Aarnhem EE, Budde RP. Effect of antibiotics on FDG-PET/CT imaging of prosthetic heart valve endocarditis. Eur Heart J Cardiovasc Imaging. 2015;16:1223.
Kestler M, Muñoz P, Rodríguez-Créixems M, et al. In collaboration with the Group for the Management of Infectious Endocarditis (GAME). Role of 18F-FDG PET in patients with infectious. Endocarditis. J Nucl Med. 2014;55:1–6.
Granados U, Fuster D, Pericas JM, et al. Diagnostic accuracy of 18F–FDG PET/CT in infective endocarditis and implantable cardiac electronic device infection: a cross-sectional study. 2016. J Nucl Med 57:1726–32.
Van Riet J, Hill EE, Gheysens O, et al. 18F-FDG PET/CT for early detection of embolism and metastatic infection in patients with infective endocarditis. Eur J Nucl Med Mol Imaging. 2010;37:1189–97.
Bonfiglioli R, Nanni C, Morigi JJ, et al. 18F-FDG PET/CT diagnosis of unexpected extracardiac septic embolisms in patients with suspected cardiac endocarditis. Eur J Nucl Med Mol Imaging. 2013;40:1190–6.
Schouten LR, Verberne HJ, Bouma BJ, Van Eck-Smit BL, Mulder BJ. Surgical glue for repair of the aortic root as a possible explanation for increased F-18 FDG uptake. J Nucl Cardiol. 2008;15:146–7.
• Pizzi MN, Roque A, Cuéllar-Calabria H. Infective versus inflammatory patterns in 18F-FDG-PET/CTA of prosthetic cardiac valves and valve-tube grafts. J Am Coll Cardiol Img. 2016;9(10):1224–7. Inflammatory changes are always a concern when images are acquired after recent surgery. In this study, the authors define the characteristic patterns of 18 F-FDG uptake and the typical anatomic changes that can aid in differentiating between inflammation and infection in these patients.
• Scholtens AM, Swart LE, Verberne HJ, Tanis W, Lam ME, Budde RP. Confounders in FDG-PET/CT imaging of suspected prosthetic valve endocarditis. J Am Coll Cardiol Img. 2016; doi:10.1016/j.jcmg.2016.01.024. 18 F-FDG-PET/CT is a novel technique, and the boundaries between normal and abnormal findings are relatively undefined. Awareness of confounding variants is essential in the context of suspected prosthetic valve endocarditis and cardiovascular infection, as this may prevent false-positive or false-negative readings. This article provides an overview of possible confounders which should be borne in mind when interpreting cardiac PET/CT studies.
Yaddanapudi K, Brunken R, Tan CD, Rodriguez ER, Bolen MA. PET-MR imaging in evaluation of cardiac and Paracardiac masses with histopathologic correlation. J Am Coll Cardiol Img. 2016;9(1):82–5.
Salomäki SP, Hohenthal U, Kemppainen J, et al. Visualization of pericarditis by fluorodeoxyglucose PET. Eur Heart J Cardiovasc Imaging. 2014;15:291.
Fan CM, Fischman AJ, Kwek BH, Abbara S, Aquino SL. Lipomatous hypertrophy of the interatrial septum: increased uptake on FDG PET. AJR. 2005;184:339–42.
Rahbar K, Seifarth H, Schäfers M, et al. Differentiation of malignant and benign cardiac tumors using 18F-FDG PET/CT. J Nucl Med. 2012;53:856–63.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Albert Roque, María N. Pizzi, Hug Cuéllar-Calàbria, and Santi Aguadé-Bruix declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Nuclear Cardiology
Rights and permissions
About this article

Cite this article
Roque, A., Pizzi, M., Cuéllar-Calàbria, H. et al. 18F–FDG-PET/CT Angiography for the Diagnosis of Infective Endocarditis. Curr Cardiol Rep 19, 15 (2017). https://doi.org/10.1007/s11886-017-0824-3
Published:
DOI: https://doi.org/10.1007/s11886-017-0824-3