
Abstract
Backgrounds
A two-stage procedure involving endoscopic retrograde cholangiopancreatography (ERCP), followed by cholecystectomy, is one of the primary treatments of concomitant gallstones and choledocholithiasis. However, negative findings on ERCP and migrating gallstones after cholecystectomy are major concerns. This study aimed to identify the prevalence of unnecessary ERCP and to develop and validate a predictive nomogram using preoperative factors in patients who underwent a two-stage procedure.
Methods
Consecutive 931 patients were treated with the two-stage procedure for evident gallstones and suspected choledocholithiasis. After the cholecystectomy, a cholangiogram was performed to confirm the absence of the migrating gallstones. The patients were divided into derivation (n = 652) and validation (n = 279) cohorts.
Results
A total of 26.5% (247/931) patients had unnecessary ERCP (negative choledocholithiasis, 14.6%; migrating gallstones, 11.9%). No stones on images (P < 0.001), total bilirubin < 1.2 mg/dL (P = 0.006), and common bile duct diameter < 8.0 mm (P = 0.004) were independent factors associated with negative finding on ERCP with a validated nomogram area under the curve (AUC) of 0.72 (95% confidence interval [CI] 0.64–0.80). For migrating gallstones after cholecystectomy, radiolucent gallstones (P < 0.001), gallstone size ≤ 6.4 mm (P = 0.001), cystic duct stones (P < 0.001), gallbladder wall thickness ≥ 3.2 mm (P = 0.003), and low-lying cystic duct (P < 0.001) were independent factors with a validated nomogram AUC of 0.77 (95% CI 0.68–0.87).
Conclusions
About one fourth of the patients may have unnecessary ERCP in the two-stage procedure. Based on our nomogram using preoperative factors, high-risk patients who are more likely to perform unnecessary ERCP could be considered for the one-stage procedure.


Similar content being viewed by others


References
Ko CW, Lee SP. Epidemiology and natural history of common bile duct stones and prediction of disease. Gastrointest Endosc 2002; 56: S165–169.
Peng WK, Sheikh Z, Paterson-Brown S, Nixon SJ. Role of liver function tests in predicting common bile duct stones in acute calculous cholecystitis. Br J Surg 2005; 92: 1241–1247.
Tazuma S. Gallstone disease: Epidemiology, pathogenesis, and classification of biliary stones (common bile duct and intrahepatic). Best Pract Res Clin Gastroenterol 2006; 20: 1075–1083.
Lee A, Min SK, Park JJ, Lee HK. Laparoscopic common bile duct exploration for elderly patients: as a first treatment strategy for common bile duct stones. J Korean Surg Soc 2011; 81: 128–133.
Riciardi R, Islam S, Canete JJ, Arcand PL, Stoker ME. Effectiveness and long-term results of laparoscopic common bile duct exploration. Surg Endosc 2003; 17: 19–22.
Fitzgibbons RJ, Jr., Gardner GC. Laparoscopic surgery and the common bile duct. World J Surg 2001; 25: 1317–1324.
Wandling MW, Hungness ES, Pavey ES, Stulberg JJ, Schwab B, Yang AD et al. Nationwide Assessment of Trends in Choledocholithiasis Management in the United States From 1998 to 2013. JAMA Surg 2016; 151: 1125–1130.
Rhodes M, Sussman L, Cohen L, Lewis MP. Randomised trial of laparoscopic exploration of common bile duct versus postoperative endoscopic retrograde cholangiography for common bile duct stones. Lancet 1998; 351: 159–161.
Zhu HY, Xu M, Shen HJ, Yang C, Li F, Li KW et al. A meta-analysis of single-stage versus two-stage management for concomitant gallstones and common bile duct stones. Clin Res Hepatol Gastroenterol 2015; 39: 584–593.
Oria A, Alvarez J, Chiappetta L, Spina JC, Hernandez N, Iovaldi M et al. Choledocholithiasis in acute gallstone pancreatitis. Incidence and clinical significance. Arch Surg 1991; 126: 566–568.
Kohut M, Nowakowska-Dulawa E, Marek T, Kaczor R, Nowak A. Accuracy of linear endoscopic ultrasonography in the evaluation of patients with suspected common bile duct stones. Endoscopy 2002; 34:299–303.
Adams MA, Hosmer AE, Wamsteker EJ, Anderson MA, Elta GH, Kubiliun NM et al. Predicting the likelihood of a persistent bile duct stone in patients with suspected choledocholithiasis: accuracy of existing guidelines and the impact of laboratory trends. Gastrointest Endosc 2015; 82: 88–93.
Trotman BW, Soloway RD. Pigment gallstone disease: Summary of the National Institutes of Health--international workshop. Hepatology 1982; 2: 879–884.
Kim IS, Myung SJ, Lee SS, Lee SK, Kim MH. Classification and nomenclature of gallstones revisited. Yonsei Med J 2003; 44: 561–570.
Ding G, Cai W, Qin M. Single-stage vs. two-stage management for concomitant gallstones and common bile duct stones: a prospective randomized trial with long-term follow-up. J Gastrointest Surg 2014; 18: 947–951.
Lu J, Cheng Y, Xiong XZ, Lin YX, Wu SJ, Cheng NS. Two-stage vs single-stage management for concomitant gallstones and common bile duct stones. World J Gastroenterol 2012; 18: 3156–3166.
Maple JT, Ben-Menachem T, Anderson MA, Appalaneni V, Banerjee S, Cash BD et al. The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointest Endosc 2010; 71: 1–9.
He H, Tan C, Wu J, Dai N, Hu W, Zhang Y et al. Accuracy of ASGE high-risk criteria in evaluation of patients with suspected common bile duct stones. Gastrointest Endosc 2017; 86: 525–532.
Narvaez Rivera RM, Gonzalez Gonzalez JA, Monreal Robles R, Garcia Compean D, Paz Delgadillo J, Garza Galindo AA et al. Accuracy of ASGE criteria for the prediction of choledocholithiasis. Rev Esp Enferm Dig 2016; 108: 309–314.
Ebrahim M, Sorensen LT, Jorgensen LN, Kalaitzakis E. Current clinical algorithms for predicting common bile duct stones have only moderate accuracy. Dig Endosc 2018; 30: 477–484
Sethi S, Wang F, Korson AS, Krishnan S, Berzin TM, Chuttani R et al. Prospective assessment of consensus criteria for evaluation of patients with suspected choledocholithiasis. Dig Endosc 2016; 28: 75–82.
Garrow D, Miller S, Sinha D, Conway J, Hoffman BJ, Hawes RH et al. Endoscopic ultrasound: a meta-analysis of test performance in suspected biliary obstruction. Clin Gastroenterol Hepatol 2007; 5: 616–623.
Tse F, Liu L, Barkun AN, Armstrong D, Moayyedi P. EUS: a meta-analysis of test performance in suspected choledocholithiasis. Gastrointest Endosc 2008; 67: 235–244.
Prachayakul V, Aswakul P, Bhunthumkomol P, Deesomsak M. Diagnostic yield of endoscopic ultrasonography in patients with intermediate or high likelihood of choledocholithiasis: a retrospective study from one university-based endoscopy center. BMC Gastroenterol 2014; 14: 165.
Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA 2003; 289: 1639–1644.
Pierce RA, Jonnalagadda S, Spitler JA, Tessier DJ, Liaw JM, Lall SC et al. Incidence of residual choledocholithiasis detected by intraoperative cholangiography at the time of laparoscopic cholecystectomy in patients having undergone preoperative ERCP. Surg Endosc 2008; 22: 2365–2372.
Bansal VK, Misra MC, Garg P, Prabhu M. A prospective randomized trial comparing two-stage versus single-stage management of patients with gallstone disease and common bile duct stones. Surg Endosc 2010; 24: 1986–1989.
Koc B, Karahan S, Adas G, Tutal F, Guven H, Ozsoy A. Comparison of laparoscopic common bile duct exploration and endoscopic retrograde cholangiopancreatography plus laparoscopic cholecystectomy for choledocholithiasis: a prospective randomized study. Am J Surg 2013; 206: 457–463.
Prasson P, Bai X, Zhang Q, Liang T. One-stage laproendoscopic procedure versus two-stage procedure in the management for gallstone disease and biliary duct calculi: a systemic review and meta-analysis. Surg Endosc 2016; 30: 3582–3590.
Iranmanesh P, Frossard JL, Mugnier-Konrad B, Morel P, Majno P, Nguyen-Tang T et al. Initial cholecystectomy vs sequential common duct endoscopic assessment and subsequent cholecystectomy for suspected gallstone migration: a randomized clinical trial. JAMA 2014; 312: 137–144.
Enochsson L, Lindberg B, Swahn F, Arnelo U. Intraoperative endoscopic retrograde cholangiopancreatography (ERCP) to remove common bile duct stones during routine laparoscopic cholecystectomy does not prolong hospitalization: a 2-year experience. Surg Endosc 2004; 18: 367–371.
Bencini L, Tommasi C, Manetti R, Farsi M. Modern approach to cholecysto-choledocholithiasis. World J Gastrointest Endosc 2014; 6: 32–40.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
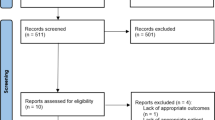
Supplementary Figure 1
The flow protocol of the study. ERCP, endoscopic retrograde cholangiopancreatography; ENBD, endoscopic nasobiliary drainage; CBD, common bile duct (PNG 127 kb)
Supplementary Figure 2
Nomogram to predict (A) negative choledocholithiasis on ERCP and (B) migrating gallstones after two-stage procedure. CBD, common bile duct; GB, gallbladder (PNG 1156 kb)
Supplementary Figure 3
(PNG 1208 kb)
ESM 4
(DOCX 19 kb)
Rights and permissions
About this article

Cite this article
Lee, H.W., Park, D.H., Lee, J.H. et al. Prevalence and Predictors of Unnecessary Endoscopic Retrograde Cholangiopancreatography in the Two-Stage Endoscopic Stone Extraction Followed by Laparoscopic Cholecystectomy. J Gastrointest Surg 23, 1578–1588 (2019). https://doi.org/10.1007/s11605-018-04090-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-018-04090-z