
Abstract
Introduction
The purpose of this study is to determine the incidence of residual common bile duct (CBD) stones after preoperative ERCP for choledocholithiasis and to evaluate the utility of routine intraoperative cholangiography (IOC) during laparoscopic cholecystectomy (LC) in this patient population.
Methods
All patients who underwent preoperative ERCP and interval LC with IOC from 5/96 to 12/05 were reviewed under an Institutional Review Board (IRB)-approved protocol. Data collected included all radiologic imaging, laboratory values, clinical and pathologic diagnoses, and results of preoperative ERCP and LC with IOC. Standard statistical analyses were used with significance set at p < 0.05.
Results
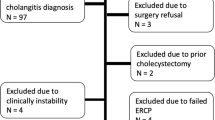
A total of 227 patients (male:female 72:155, mean age 51.9 years) underwent preoperative ERCP for suspicion of choledocholithiasis. One hundred and eighteen patients were found to have CBD stones on preoperative ERCP, and of these, 22 had choledocholithiasis diagnosed on IOC during LC. However, two patients had residual stones on completion cholangiogram after ERCP and were considered to have retained stones. Therefore, 20 patients overall were diagnosed with either interval passage of stones into the CBD or a false-negative preoperative ERCP. In the 109 patients without CBD stones on preoperative ERCP, nine patients had CBD stones on IOC during LC, an 8.3% incidence of interval passage of stones or false-negative preoperative ERCP. In both groups, there was no correlation (p > 0.05) between an increased incidence of CBD stones on IOC and a longer time interval between ERCP and LC, performance of sphincterotomy, incidence of cystic duct stones, or pathologic diagnosis of cholelithiasis.
Conclusions
The overall incidence of retained or newly passed CBD stones on IOC during LC after a preoperative ERCP is 12.9%. Although the natural history of residual CBD stones after preoperative ERCP is not known, the routine use of IOC should be considered in patients with CBD stones on preoperative ERCP undergoing an interval LC.

Similar content being viewed by others

References
Koo KP, Traverso LW (1996) Do preoperative indicators predict the presence of common bile duct stones during laparoscopic cholecystectomy? Am J Surg 171:495–499
Traverso LW, Hauptmann EM, Lynge DC (1994) Routine intraoperative cholangiography and its contribution to the selective cholangiographer. Am J Surg 167:464–468
Ludwig K, Bernhardt J, Lorenz D (2002) Value and consequences of routine intraoperative cholangiography during cholecystectomy. Surg Laparosc Endosc Percutan Tech 12:154–159
Sbeih F, Aljohani M, Altraif I, Khan H (1998) Role of endoscopic retrograde cholangiopancreatography before and after laparoscopic cholecystectomy. Ann Saudi Med 18:117–119
Sultan S, Baillie J (2004) Recurrent bile duct stones after endoscopic sphincterotomy. Gut 53:1725–1727
Vezakis A, Davides D, Ammori BJ, Martin IG, Larvin M, McMahon MJ (2000) Intraoperative cholangiography during laparoscopic cholecystectomy. Surg Endosc 14:1118–1122
Hungness ES, Soper NJ (2006) Management of common bile duct stones. J Gastrointest Surg 10:612–619
Tranter SE, Thompson MH (2002) Comparison of endoscopic sphincterotomy and laparoscopic exploration of the common bile duct. Br J Surg 89:1495–1504
Williams GL, Vellacott KD (2002) Selective operative cholangiography and perioperative endoscopic retrograde cholangiopancreatography (ERCP) during laparoscopic cholecystectomy: a viable option for choledocholithiasis. Surg Endosc 16:465–467
Cuschieri A, Lezoche E, Morino M, Croce E, Lacy A, Toouli J, Faggioni A, Ribeiro VM, Jakimowicz J, Visa J, Hanna GB (1999) E.A.E.S. multicenter prospective randomized trial comparing two-stage vs single-stage management of patients with gallstone disease and ductal calculi. Surg Endosc 13:952–957
Rhodes M, Sussman L, Cohen L, Lewis MP (1998) Randomised trial of laparoscopic exploration of common bile duct versus postoperative endoscopic retrograde cholangiography for common bile duct stones. Lancet 351:159–161
Thornton DJ, Robertson A, Alexander DJ (2002) Laparoscopic cholecystectomy without routine operative cholangiography does not result in significant problems related to retained stones. Surg Endosc 16:592–595
Collins C, Maguire D, Ireland A, Fitzgerald E, O’Sullivan GC (2004) A prospective study of common bile duct calculi in patients undergoing laparoscopic cholecystectomy: natural history of choledocholithiasis revisited. Ann Surg 239:28–33
Boerma D, Rauws EA, Keulemans YC, Janssen IM, Bolwerk CJ, Timmer R, Boerma EJ, Obertop H, Huibregtse K, Gouma DJ (2002) Wait-and-see policy or laparoscopic cholecystectomy after endoscopic sphincterotomy for bile-duct stones: a randomised trial. Lancet 360:761–765
Bresadola V, Intini S, Terrosu G, Baccarani U, Marcellino MG, Sistu M, Scanavacca F, Bresadola F (2001) Intraoperative cholangiography in laparoscopic cholecystectomy during residency in general surgery. Surg Endosc 15:812–815
Amott D, Webb A, Tulloh B (2005) Prospective comparison of routine and selective operative cholangiography. ANZ J Surg 75:378–382
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pierce, R.A., Jonnalagadda, S., Spitler, J.A. et al. Incidence of residual choledocholithiasis detected by intraoperative cholangiography at the time of laparoscopic cholecystectomy in patients having undergone preoperative ERCP. Surg Endosc 22, 2365–2372 (2008). https://doi.org/10.1007/s00464-008-9785-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-9785-3