
Abstract
Purpose
To develop a machine learning (ML) model based on radiomic features (RF) extracted from whole prostate gland magnetic resonance imaging (MRI) for prediction of tumour hypoxia pre-radiotherapy.
Material and methods
Consecutive patients with high-grade prostate cancer and pre-treatment MRI treated with radiotherapy between 01/12/2007 and 1/08/2013 at two cancer centres were included. Cancers were dichotomised as normoxic or hypoxic using a biopsy-based 32-gene hypoxia signature (Ragnum signature). Prostate segmentation was performed on axial T2-weighted (T2w) sequences using RayStation (v9.1). Histogram standardisation was applied prior to RF extraction. PyRadiomics (v3.0.1) was used to extract RFs for analysis. The cohort was split 80:20 into training and test sets. Six different ML classifiers for distinguishing hypoxia were trained and tuned using five different feature selection models and fivefold cross-validation with 20 repeats. The model with the highest mean validation area under the curve (AUC) receiver operating characteristic (ROC) curve was tested on the unseen set, and AUCs were compared via DeLong test with 95% confidence interval (CI).
Results
195 patients were included with 97 (49.7%) having hypoxic tumours. The hypoxia prediction model with best performance was derived using ridge regression and had a test AUC of 0.69 (95% CI: 0.14). The test AUC for the clinical-only model was lower (0.57), but this was not statistically significant (p = 0.35). The five selected RFs included textural and wavelet-transformed features.
Conclusion
Whole prostate MRI-radiomics has the potential to non-invasively predict tumour hypoxia prior to radiotherapy which may be helpful for individualised treatment optimisation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Prostate cancer is the commonest malignancy in men and a major cause of cancer-related death [1]. Radiation therapy (RT), including external beam radiation therapy (EBRT) and brachytherapy (BT), is an effective treatment for localised prostate cancer [2]. Despite advances in diagnostic imaging and RT delivery techniques, treatment failure remains common with biochemical failure occurring in almost half of high-risk patients at 10 years [3,4,5].
Tumour hypoxia, a low oxygen environment, is associated with RT resistance and metastatic disease in prostate cancer [6,7,8,9]. Identifying tumour hypoxia may help with patient selection for radiation boosting. Current methods of assessing hypoxia, such as using prostate biopsy samples to identify gene-based hypoxia biomarkers, or oxygen electrodes, are invasive and hindered by sampling errors due to multi-focal tumours and intra-tumoral heterogeneity [10]. Magnetic resonance imaging (MRI) offers a potential non-invasive method of assessing hypoxia that allows the whole prostate to be measured and assessed over time, i.e. before, during and following treatment to monitor response.
Radiomics is a quantitative method of imaging analysis using data-characterisation algorithms to derive imaging biomarkers [11]. Imaging-based radiogenomics offers promise in bridging the gap between medical imaging and histopathological or molecular/gene signatures, by integrating data generated from complementary data sources to improve the accuracy of predictive models [12]. Machine learning (ML) models based on radiomic features (RF) extracted from T2-weighted (T2w) prostate MRI have demonstrated good performance for detecting clinically significant cancer [13]. Radiomic signatures have also been shown to accurately predict molecular subtypes of cancers associated with a more invasive phenotype [14]. The application of ML to radiogenomic studies provides novel insights into tumour biology and has been evaluated in multiple tumour types [15,16,17]. Identifying hypoxia on T2w prostate MRI also has treatment implications given the role of MRI-guided RT, which already incorporates a T2w sequence into the standard workflow, therefore there is potential for dose escalation based on an imaging radiogenomic approach.
The aim of this study was to develop a ML model based on RFs extracted from whole gland prostate MRI for prediction of tumour hypoxia pre-radiotherapy.
Materials and methods
Dataset and study population
This retrospective study was approved by the United Kingdom North West Research Ethics Committee (Validation and qualification of a multiplex hypoxia biomarker for radiotherapy individualisation in prostate cancer study (IRAS 15/NW/0559)). Informed consent was obtained from all patients.
The study cohort consisted of 195 consecutive patients with histologically confirmed high-risk prostate cancer treated between 01/12/2007 and 31/08/2013 at either < Institution A > with EBRT (74 Grey (Gy) in 37 fractions) (N = 100) or at < Institution B > with EBRT (57 Gy in 19 fractions) or EBRT (37.5 Gy in 15 fractions) plus high dose rate (HDR) brachytherapy (BT) boost (single fraction 15 Gy) (N = 95).
Inclusion criteria were: (a) male patients with prostate cancer aged at least 18 years; (b) primary radiotherapy to treat their prostate cancer (either BT or EBRT); (c) available pre-treatment MRI and hypoxia gene signature data; (d) available clinical features (patient age, International Society of Urological Pathology (ISUP) grade, prostate specific antigen (PSA) and T-stage).
MRI acquisition
All patients underwent prostate MRI on 1.5 T MRI scanners which included a minimum of an axial T2w sequence encompassing the whole prostate. Imaging was performed using multiple different MRI scanners. Specific scanner acquisition parameters are listed in Supplementary Material Table 1.
Hypoxia gene signature
All patients were grouped into normoxia and hypoxia groups based on their pre-treatment prostate biopsy which was used as the ground truth for hypoxia status. The ribonucleic acid (RNA) from formalin-fixed, paraffin-embedded prostate biopsy specimens was extracted, and samples were processed using Affymetrix GeneChip (Clariom S Array) to calculate the expression of a 32-gene prostate hypoxia signature, based on pimonidazole staining (Ragnum signature) [9]. The gene enrichment analysis and construction of the gene signature is described by Ragnum et al. [9]. The normoxia and hypoxia split was based on a previously validated threshold [18].
Study pipeline
Adherence was made to the Checklist for Artificial Intelligence in Medical Imaging (CLAIM) (Supplementary Material), a tool for assessing the quality of multivariate prediction models involving ML techniques [19].
Image segmentation
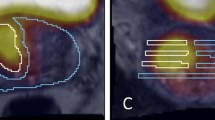
All imaging data were de-identified using a data masking method. The whole prostate gland and prostate tumour (if visible) were manually segmented by an experienced radiologist and confirmed by a specialist Uroradiologist. Segmentation was performed using RayStation (v9.1). Exported DICOM images were converted to Neuroimaging Informatics Technology Initiative (NIfTI) files and exported into PyRadiomics (v3.0.1) for analysis [20]. The Nyúl method, a histogram intensity-based normalisation technique, was applied to MRI data to render the dynamic signal intensity ranges comparable prior to RF extraction [21, 22].
A flowchart illustrating the methodological pipeline for RF-derived hypoxia prediction from segmentation through to ML model construction is shown in Fig. 1.

Flowchart demonstrating the methodological pipeline for the T2w MRI whole prostate gland radiomic model for predicting hypoxia Legend: NIfTI = Neuroimaging Informatics Technology Initiative, ICC = intraclass correlation coefficient, ComBat = imaging harmonisation method, LASSO = Least Absolute Shrinkage and Selection Operator, RFo = Random Forest.
Feature extraction
Eight RF classes [20] were extracted from each segmented region of interest (ROI) using PyRadiomics (v3.0.1) (https://pyradiomics.readthedocs.io/en/latest/index.html, accessed 09/02/2023). All RFs extracted and filters applied are detailed in Supplementary Material Table 2. Different numbers of bins (8, 16, 32, 64, 128, 256) and isotropic voxel sizes (1, 2, 3) were tested to assess the most robust quantisation/rebinning setting and confirm the number of bins with the largest set of robust features. To determine the most robust features against bin number and voxel size, approximately 10% of the total cohort was also re-segmented (n = 21). This created separate ROIs from which RFs were extracted and compared using interclass correlation coefficient (ICC).
The Image Biomarkers Standardization Initiative (IBSI) was adhered to, which provides a comprehensive review of each step involved in radiomic analyses, including nomenclature of RFs and required calibration datasets [23]. Number of bins was favoured over the bin width given the arbitrary nature of MRI intensity units. The ComBat Harmonisation method (https://github.com/Jfortin1/ComBatHarmonization, accessed 09/02/2023) (v0.2.10) was applied to extracted RFs to account for variation in scanner models, acquisition protocols and reconstruction settings which RFs are affected by [30, 31].
Feature selection
First, an unsupervised method of feature selection was applied to reduce the dataset using Pearson’s correlation coefficient. For each feature pair, correlations were assessed, a threshold of 0.8 was used to highlight highly correlated pairs and the feature in the pair with the largest average correlation to all other features was removed. Additional feature selection steps were performed using three different methods: a forward wrapper method (mlxtend 0.18.0); a univariate analysis method (scikit-learn v0.24.2); and a recursive feature extraction method (where applicable) (scikit-learn v0.24.2). A maximum of 5 features were chosen.
Machine learning (ML) model construction and statistical analysis
The dataset was split into training and test sets stratified around MRI scanner vendor and ISUP, with an 80:20 split using scikit-learn (v0.24.2) (https://scikit-learn.org/stable/whats_new/v0.24.html, accessed 09/02/2023). Six predictive ML methods (as listed under ML model construction in Fig. 1) were implemented with the Python library scikit-learn (v23.0) in order to incorporate the selected RFs into a binary classifier for distinguishing patients grouped as hypoxia or normoxia [24]. Methods used included ridge regression, random forest (RFo), elastic net, k-nearest neighbour (KNN), support vector machine (SVM), and least absolute shrinkage and selection operator (LASSO) regression. These models were trained to build classification models based on whole prostate T2w RFs, respectively.
Training of ML models and tuning of hyperparameters was performed using a Bayes search cv (scikit-optimize v0.8.1), with fivefold cross-validation stratified around hypoxia status (normoxia or hypoxia) with 25 repeats. The area under the curve (AUC) of the receiver operating characteristic (ROC) curve was calculated with confidence intervals and the DeLong method was used to compare AUCs, to assess how accurately the radiomic and clinical-only models could classify a tumour’s hypoxia status [25]. RFs and hyperparameters with the highest mean validation AUC which was within 0.05 of the mean training AUC were selected. A 0.05 cut-off was chosen to try and minimise selection of an overfitted model. The model which had the highest mean validation AUC overall was tested once on the unseen test set. The overall evaluation of clinical variables between the training and testing groups to ensure balanced groups was compared using the independent t test (continuous variables) and Chi-square test (categorical variables). The statistically significant level was set at 0.05.
Results
The demographics, pathology information and hypoxia status of the prostate tumours in the final study cohort, split by training and test cohort, are described in Table 1.
Machine learning model building
The best performing model with clinical variables alone was a ridge regression model (Fig. 2) which included age and tumour stage variables. Mean training AUC was 0.61 (Standard Deviation (SD) 0.02), and mean training validation AUC was 0.60 (SD 0.08). Mean test AUC was 0.57 (95% confidence interval (CI) 0.14). The ML models with added RFs outperformed the clinical-only model. Mean training and validation AUCs for the best performing radiomics-based ML models along with hyperparameters and selected RFs are shown in Table 2.

ROC curve of the best performing ridge regression hypoxia prediction model (test and training performance) using clinical features. Mean training AUC 0.61 (SD 0.02), mean training validation AUC 0.60 (SD 0.08). Mean test AUC 0.57 (95% CI 0.14)
The model within the highest mean validation AUC was a ridge regression model created using radiomic and clinical features. The best performing ML model is shown in Fig. 3 with a mean training AUC of 0.73 (SD 0.02), mean training validation AUC of 0.71 (SD 0.10) and mean test AUC of 0.69 (95% CI 0.14). The 5 selected RFs were logarithm grey level size zone matrix (GLSZM), Large Area Emphasis (LAE) and the following 3-dimensional wavelet features: LLH grey level co-occurrence matrix (GLCM) Cluster Prominence, HLL GLCM maximal correlation coefficient (MCC), HLH first-order Median, HHH GLCM MCC. No clinical features were selected despite integrating all clinical variables into the model.

ROC curve of the best performing ridge regression hypoxia prediction model (test and training performance) using radiomic features. Mean training AUC 0.73 (SD 0.02). Mean training validation AUC 0.71 (SD 0.10). Mean test AUC 0.69 (95% CI 0.14).
For the combined model with the highest AUC, performance metrics were: overall model accuracy 0.72, sensitivity 0.74, specificity 0.70, positive predictive value (PPV) 0.70, and negative predictive value (NPV) 0.74. The best performing clinical model had an overall accuracy of 0.56, sensitivity of 0.67, specificity of 0.53, PPV of 0.3, and NPV of 0.84. Confusion matrices are presented in Tables 3 and 4, respectively. The radiomics and clinical-only models showed no significant difference according to DeLong's testing (p = 0.35) (Fig. 4).

Mean ROC curves of the best performing radiomics and clinical-based ridge regression hypoxia prediction models with 95% confidence intervals highlighted
Discussion
The aim of this study was to develop a ML model based on RFs extracted from whole prostate gland T2w MRI for non-invasive prediction of tumour hypoxia identified in biopsies using a 32-gene signature [9]. The results showed that the integration of RFs from MRI helped improve the prediction of hypoxia in patients with prostate cancer, with the best ML model (ridge regression) having an AUC of 0.69 for the unseen internal test cohort compared to 0.57 for a model derived from only clinical variables. Although this change did not reach statistical significance, it still highlights the potential use of MRI to non-invasively assess hypoxia status in prostate cancer.
The benchmark for tumour hypoxia determination in this study was a hypoxia-associated gene expression (Ragnum) signature. This intrinsic molecular biomarker reflected the transcriptional profile associated with pimonidazole staining, an extrinsic marker of hypoxia, and was validated for prognostic significance in independent datasets [9]. Whole-mount prostate specimens were not available in the current cohort where all patients only received RT. By using the gene signature as the ground truth, we were able to provide a biological basis for the observed hypoxia-associated RFs selected by the ML models.
MRI-guided EBRT focal boosting to intra-prostatic lesions has been demonstrated to be safe and Level 1 evidence shows it improves biochemical control when compared to whole prostate EBRT [26]. Incorporating imaging radiogenomics into MRI-guided focal boosting of hypoxic tumours may further improve clinical outcomes given that hypoxic cells are three times more radioresistant than normoxic ones [8, 27]. Most prostate cancer patients undergo MRI routinely as part of diagnostic work-up, and T2w imaging is the most utilised sequence thereby potentially facilitating use of a T2w MRI hypoxia radiomics-based approach in the clinic. Despite the role of adaptive RT, there is no routine clinical use of any imaging methods to identify hypoxic regions. However, in the era of MRI-guided RT using MRI linear accelerators, there is potential to develop a radiomics-based hypoxia targeted radiotherapy methodological framework. This approach would also require robust harmonisation algorithms to account for the difference in field strength and MRI parameters on MR linear accelerators.
After prostate RT, the only validated biomarker for disease recurrence is prostate specific antigen (PSA) [28, 29]. The results of this preliminary study suggest that imaging biomarkers and RFs could offer further measurable longitudinal metrics that might be used to help guide post-treatment surveillance and survival predictions. This aligns with evidence from other tumours such as glioblastoma and renal cell cancer, which provide a biological basis for RFs [30, 31]. Beig et al. reported that RFs extracted from different regions of interest in 180 patients with glioblastoma such as enhancing tumour, necrotic tumour, and peri-tumoral regions were predictive of a hypoxia enrichment score based on 21 genes implicated in the hypoxia pathway of glioblastoma [32]. The top-eight features most associated with the hypoxia enrichment score included RFs which quantified structural heterogeneity and their imaging-based radiogenomic hypoxic signature was associated with survival [32]. Gao et al. derived a hypoxia-gene-related radiogenomic signature using RFs extracted from contrast-enhanced CT and found that this was significantly associated with prognosis in patients with renal cell cancer validating this in an independent cohort [31]. Such validation and insight into the biological characteristics of tumours is vital and needs to be replicated for prostate cancer pathways, which the current study attempts to address.
Previous research investigating the association between MRI and transcriptomic profiles in prostate cancer have suffered from low patient numbers, limiting transferability of results [33, 34]. To develop imaging biomarkers of prostate hypoxia, the availability of ‘ground truth’ data such as pathology or genomic profiling is critical to ensure the translational gap can be crossed allowing integration into routine care [35]. Leech et al. found that a radiomics model extracted from 88 T2w prostate MRIs (single axial slice used rather than a volume) could predict tumour hypoxia measured using pimonidazole stained prostatectomy specimens [36]. Their ML model used elastic net regularisation and repeated cross-validation to yield an AUC of 0.60 (SD 0.2) without a validation dataset but further demonstrates the feasibility of building a radiomics hypoxia model using T2w MRI. The RFs selected by their ML model were mainly shape-based features but also included the textural feature grey level size zone matrix (GLSZM) which was also one of the features selected by the best performing ML model in the current study. GLSZM quantifies grey level zones in an image, and GLSZM large area emphasis (LAE), one of the selected RFs in the best ML model in our study, measures the distribution of ‘large area size zones’, where a larger value indicates bigger zones with more coarse textures. Another RF selected was grey level co-occurrence matrix (GLCM) which reflects the spatial relationship among pixels and defines how frequently a combination of pixels is present. This potentially suggests a heterogeneous appearing prostate with more coarse textures associating with hypoxia.
There are a number of limitations to the study: Genomic profiling and MRIs were performed over several years and scanner technology and imaging protocols have evolved in the interim; imaging data used were all acquired on 1.5 T scanners and many did not have functional imaging sequences available as this was not routine at the time of the initial imaging acquisition. Similarly, the transcriptomic data were generated in small, old biopsies. As a result, only T2w imaging was used to develop radiomic models; whole prostate segmentations were used to extract RFs as not all cases had a visible tumour on anatomical imaging, and it was not possible to match the site of biopsy taken. Previous work has linked normal background prostate tissue with high-risk gene expression profiles highlighting the value for evaluating the whole gland [37]. Despite this study being a two-institution curated dataset, a further prospective validation cohort would allow for further testing of the reproducibility across different imaging equipment. Obtaining these radiogenomic datasets with matched clinical, imaging, pathology and genomic data remains challenging and requires further collaboration and formation of consortia with standardized methods for RF extraction. Establishing more multi-institutional collaborations with the potential to utilise novel transfer learning techniques will help expand our knowledge of genomics and imaging phenotypes in prostate cancer [38]. A general drawback to retrospective imaging research is the lack of imaging protocol standardisation, which differ significantly across institutions. In this study, ComBat harmonisation was used to minimize issues related to MRI data acquired on multiple scanners [39, 40]. Exploring the added role of functional MRI sequences in imaging hypoxia is vital to develop more sensitive diagnostic pathways. Hompland et al. investigated a novel MRI technique called intravoxel incoherent motion (IVIM) as an indirect measure of tumour hypoxia and validated this against the exogenous hypoxia marker pimonidazole [41]. Similarly, R2* maps from blood oxygen level-dependent (BOLD) MRI sequences have been found to have a high sensitivity for defining intra-prostatic tumour hypoxia [10]. A major barrier to clinical translation of these advanced imaging techniques is the poor spatial resolution that is required to fully sample the tumour microenvironment [42]. Utilising routinely acquired T2w MR data yields higher resolution prostate images allowing for better appreciation of structural differences. It is also less prone to artefacts compared to other functional sequences such as diffusion weighted imaging. Validating imaging biomarkers and RFs using gene expression signatures provides a biological basis but the external validation of any radiogenomic signature followed by further testing in the setting of a prospective randomised trial is essential to demonstrate value in clinical translation [43].
In conclusion, the current study suggests that whole prostate MRI-radiomics has the potential to non-invasively predict tumour hypoxia prior to radiotherapy. Further external validation of the hypoxia-associated radiomics model in predicting biochemical recurrence and clinical outcomes is required to determine the benefit of using the integrated information for patient stratification.
Abbreviations
- RT:
-
Radiation therapy
- EBRT:
-
External beam radiation therapy
- MRI:
-
Magnetic resonance imaging
- ML:
-
Machine learning
- RF:
-
Radiomic feature
- T2w:
-
T2 weighted
- Gy:
-
Grey
- HDR:
-
High dose rate
- BT:
-
Brachytherapy
- ISUP:
-
International Society of Urological Pathology
- PSA:
-
Prostate-specific antigen
- RNA:
-
Ribonucleic acid
- CLAIM:
-
Checklist for Artificial Intelligence in Medical Imaging
- NIfTI:
-
Neuroimaging Informatics Technology Initiative
- ROI:
-
Regions of interest
- ICC:
-
Interclass correlation coefficient
- IBSI:
-
Image Biomarkers Standardisation Initiative
- RFo:
-
Random forest
- SVM:
-
Support vector machine
- LASSO:
-
Least absolute shrinkage and selection operator
- AUC:
-
Area under the curve
- ROC:
-
Receiver operating characteristic
- CI:
-
Confidence interval
- GLSZM:
-
Grey level size zone matrix
- LAE:
-
Large Area Emphasis
- GLCM:
-
Grey level co-occurrence matrix
- MCC:
-
Maximal correlation coefficient
- PPV:
-
Positive predictive value
- NPV:
-
Negative predictive value
- LLH, HLL, HLH, HHH:
-
3D wavelet radiomic features
- IVIM:
-
Intravoxel incoherent motion
- BOLD:
-
Blood oxygen level dependent
References
Cronin KA, Lake AJ, Scott S, Sherman RL, Noone A-M, Howlader N et al (2018) Annual report to the nation on the status of cancer, part I: national cancer statistics. Cancer 124(13):2785–2800
Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M et al (2017) EAU-ESTRO-SIOG guidelines on prostate cancer part 1: screening diagnosis and local treatment with curative intent. Eur Urol [Internet] 71(4):618–629
Beckendorf V, Guerif S, Le Prisé E, Cosset JM, Bougnoux A, Chauvet B et al (2011) 70 Gy versus 80 Gy in localized prostate cancer: 5-year results of GETUG 06 randomized trial. Int J Radiat Oncol Biol Phys [Internet] 80(4):1056–1063
Zumsteg ZS, Spratt DE, Romesser PB, Pei X, Zhang Z, Kollmeier M et al (2015) Anatomical patterns of recurrence following biochemical relapse in the dose escalation era of external beam radiotherapy for prostate cancer. J Urol [Internet] 194(6):1624–1630
Jones CU, Hunt D, McGowan DG, Amin MB, Chetner MP, Bruner DW et al (2011) Radiotherapy and short-term androgen deprivation for localized prostate cancer. N Engl J Med 365(2):107–118
Turaka A, Buyyounouski MK, Hanlon AL, Horwitz EM, Greenberg RE, Movsas B (2012) Hypoxic prostate/muscle Po2 ratio predicts for outcome in patients with localized prostate cancer: long-term results. Int J Radiat Oncol 82(3):e433–e439
Lalonde E, Ishkanian AS, Sykes J, Fraser M, Ross-Adams H, Erho N et al (2014) Tumour genomic and microenvironmental heterogeneity for integrated prediction of 5-year biochemical recurrence of prostate cancer: a retrospective cohort study. Lancet Oncol 15(13):1521–1532
Milosevic M, Warde P, Ménard C, Chung P, Toi A, Ishkanian A et al (2012) Tumor hypoxia predicts biochemical failure following radiotherapy for clinically localized prostate cancer. Clin Cancer Res 18(7):2108–2114
Ragnum HB, Vlatkovic L, Lie AK, Axcrona K, Julin CH, Frikstad KM et al (2015) The tumour hypoxia marker pimonidazole reflects a transcriptional programme associated with aggressive prostate cancer. Br J Cancer 112(2):382–390
Hoskin PJ, Carnell DM, Taylor NJ, Smith RE, Stirling JJ, Daley FM et al (2007) Hypoxia in prostate cancer: correlation of BOLD-MRI with pimonidazole immunohistochemistry-initial observations. Int J Radiat Oncol Biol Phys [Internet] 68(4):1065–1071
Lambin P, Leijenaar RTH, Deist TM, Peerlings J, De Jong EEC, Van Timmeren J et al (2017) Radiomics: the bridge between medical imaging and personalized medicine. Nat Rev Clin Oncol [Internet] 4(12):749–762
Bodalal Z, Trebeschi S, Nguyen-Kim TDL, Schats W, Beets-Tan R (2019) Radiogenomics: bridging imaging and genomics. Abdom Radiol 44(6):1960–1984
Hectors SJ, Chen C, Chen J, Wang J, Gordon S, Yu M et al (2021) Magnetic resonance imaging radiomics-based machine learning prediction of clinically significant prostate cancer in equivocal <scp>PI-RADS</scp> 3 lesions. J Magn Reson Imaging 54(5):1466–1473
Binder ZA, Thorne AH, Bakas S, Wileyto EP, Bilello M, Akbari H et al (2018) Epidermal growth factor receptor extracellular domain mutations in glioblastoma present opportunities for clinical imaging and therapeutic development. Cancer Cell 34(1):163-177.e7
Kirienko M, Sollini M, Corbetta M, Voulaz E, Gozzi N, Interlenghi M et al (2021) Radiomics and gene expression profile to characterise the disease and predict outcome in patients with lung cancer. Eur J Nucl Med Mol Imaging 48(11):3643–3655
Fjeldbo CS, Hompland T, Hillestad T, Aarnes E-K, Günther C-C, Kristensen GB et al (2020) Combining imaging- and gene-based hypoxia biomarkers in cervical cancer improves prediction of chemoradiotherapy failure independent of intratumour heterogeneity. EBioMedicine 57:102841
Fan M, Xia P, Clarke R, Wang Y, Li L (2020) Radiogenomic signatures reveal multiscale intratumour heterogeneity associated with biological functions and survival in breast cancer. Nat Commun 11(1):4861
Yang L, Roberts D, Takhar M, Erho N, Bibby BAS, Thiruthaneeswaran N et al (2018) Development and validation of a 28-gene hypoxia-related prognostic signature for localized prostate cancer. EBioMedicine [Internet] 31:182–189
Mongan J, Moy L, Kahn CE (2020) Checklist for artificial intelligence in medical imaging (CLAIM): a guide for authors and reviewers. Radiol Artif Intell 2(2):e200029
van Griethuysen JJM, Fedorov A, Parmar C, Hosny A, Aucoin N, Narayan V et al (2017) Computational radiomics system to decode the radiographic phenotype. Cancer Res 77(21):e104–e107
Carré A, Klausner G, Edjlali M, Lerousseau M, Briend-Diop J, Sun R et al (2020) Standardization of brain MR images across machines and protocols: bridging the gap for MRI-based radiomics. Sci Rep 10(1):12340
Nyul LG, Udupa JK, Zhang X (2000) New variants of a method of MRI scale standardization. IEEE Trans Med Imaging 19(2):143–150
Zwanenburg A, Vallières M, Abdalah MA, Aerts HJWL, Andrearczyk V, Apte A et al (2020) The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 295(2):328–338
Pedregosa F, Varoquaux G, Gramfort A, Michel V, Thirion B, Grisel O, Blondel M, Prettenhofer P, Weiss R, Dubourg V, Vanderplas J (2011) Scikit-learn: Machine Learning in Python. J Mach Learn Res [Internet] 12:2825–2830
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44(3):837–845
Poon DMC, Yuan J, Yang B, Kerkmeijer LGW, Kishan AU, Murthy V et al (2022) Magnetic Resonance Imaging–guided Focal Boost to Intraprostatic Lesions Using External Beam Radiotherapy for Localized Prostate Cancer: A Systematic Review and Meta-analysis. Eur Urol Oncol 6(2):116–127
Bristow R, Berlin A, Dal Pra A (2014) An arranged marriage for precision medicine: hypoxia and genomic assays in localized prostate cancer radiotherapy. Br J Radiol 87(1035):20130753
Amaro A, Esposito AI, Gallina A, Nees M, Angelini G, Albini A et al (2014) Validation of proposed prostate cancer biomarkers with gene expression data: a long road to travel. Cancer Metastasis Rev 33(2–3):657–671
Stamey TA, Yang N, Hay AR, McNeal JE, Freiha FS, Redwine E (1987) Prostate-Specific Antigen as a Serum Marker for Adenocarcinoma of the Prostate. N Engl J Med 317(15):909–916
Tomaszewski MR, Gillies RJ (2021) The biological meaning of radiomic features. Radiology 298(3):505–516
Gao J, Ye F, Han F, Wang X, Jiang H, Zhang J. 2021 A Novel Radiogenomics Biomarker Based on Hypoxic-Gene Subset: Accurate Survival and Prognostic Prediction of Renal Clear Cell Carcinoma. Front Oncol, 11
Beig N, Bera K, Prasanna P, Antunes J, Correa R, Singh S et al (2020) Radiogenomic-based survival risk stratification of tumor habitat on Gd-T1w MRI is associated with biological processes in glioblastoma. Clin Cancer Res [Internet] 26(8):1866–1876
Ferro M, de Cobelli O, Vartolomei MD, Lucarelli G, Crocetto F, Barone B et al (2021) Prostate cancer radiogenomics—from imaging to molecular characterization. Int J Mol Sci 22(18):9971
Sun Y, Williams S, Byrne D, Keam S, Reynolds HM, Mitchell C et al (2019) Association analysis between quantitative MRI features and hypoxia-related genetic profiles in prostate cancer: a pilot study. Br J Radiol 92(1104):20190373
O’Connor JPB, Aboagye EO, Adams JE, Aerts HJWL, Barrington SF, Beer AJ et al (2017) Imaging biomarker roadmap for cancer studies. Nat Rev Clin Oncol 14(3):169–186
Leech M, Leijenaar RTH, Hompland T, Gaffney J, Lyng H, Marignol L (2023) Exploring hypoxia in prostate cancer with T2-weighted magnetic resonance imaging radiomics and pimonidazole scoring. Anticancer Res 43(1):351–357
Stoyanova R, Takhar M, Tschudi Y, Ford JC, Solórzano G, Erho N et al (2016) Prostate cancer radiomics and the promise of radiogenomics. Transl Cancer Res [Internet] 5(4):432–447
Hanczar B, Bourgeais V, Zehraoui F (2022) Assessment of deep learning and transfer learning for cancer prediction based on gene expression data. BMC Bioinformatics 23(1):262
Orlhac F, Lecler A, Savatovski J, Goya-Outi J, Nioche C, Charbonneau F et al (2021) How can we combat multicenter variability in MR radiomics? Validation of a correction procedure. Eur Radiol 31(4):2272–2280
Da-ano R, Masson I, Lucia F, Doré M, Robin P, Alfieri J et al (2020) Performance comparison of modified ComBat for harmonization of radiomic features for multicenter studies. Sci Rep [Internet] 10(1):1–12
Hompland T, Hole KH, kon, Ragnum HB, Aarnes EK, Vlatkovic L, Kathrine Lie A, et al (2018) Combined mr imaging of oxygen consumption and supply reveals tumor hypoxia and aggressiveness in prostate cancer patients. Cancer Res 78(16):4774–4785
Cao X, Rao Allu S, Jiang S, Jia M, Gunn JR, Yao C et al (2020) Tissue pO2 distributions in xenograft tumors dynamically imaged by Cherenkov-excited phosphorescence during fractionated radiation therapy. Nat Commun 11(1):573
Sun R, Limkin EJ, Vakalopoulou M, Dercle L, Champiat S, Han SR et al (2018) A radiomics approach to assess tumour-infiltrating CD8 cells and response to anti-PD-1 or anti-PD-L1 immunotherapy: an imaging biomarker, retrospective multicohort study. Lancet Oncol 19(9):1180–1191
Acknowledgements
Many thanks to Gareth Price for helping with the data anonymisation process.
Funding
Ananya Choudhury, Peter Hoskin and Catharine West are supported by the National Institute of Health Research (NIHR) Manchester Biomedical Research Centre, UK. Andrew Scarsbrook is supported by the Cancer Research UK (CRUK) Leeds Radiotherapy Research Centre of Excellence (RadNet C19942/A28832). Jim Zhong is supported by a CRUK Award (Leeds-Manchester Stella Erdheim Clinical PhD Fellowship—Grant Reference Number 95653117/95653118). This work was also supported by the Cancer Research UK Manchester Centre award (CTRQQR-2021\100010).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by JZ, RF, AlMcW, AD and JS. The first draft of the manuscript was written by Jim Zhong, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. The study was approved by the United Kingdom North West Research Ethics Committee (Validation and qualification of a multiplex hypoxia biomarker for radiotherapy individualisation in prostate cancer study (IRAS 15/NW/0559)).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhong, J., Frood, R., McWilliam, A. et al. Prediction of prostate tumour hypoxia using pre-treatment MRI-derived radiomics: preliminary findings. Radiol med 128, 765–774 (2023). https://doi.org/10.1007/s11547-023-01644-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-023-01644-3