
Abstract
Objectives
To review the rate of soft-shell headgear use in rugby union, consumer knowledge of the protection potential of soft-shell headgear, incidence of concussion reported in rugby headgear studies, and the capacity of soft-shell headgear to reduce acceleration impact forces.
Design
A systematic search was conducted in July and August 2021 using the databases SPORT Discus, PubMed, MEDLINE, CINAHL (EBSCO), Scopus, and Science Direct. The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol for this systematic review was registered on PROSPERO (registration number: CRD42021239595).
Outcome measures
Rates of headgear use, reports of estimated protection of headgear against head injury, incidence of concussion and magnitude of impact collisions with vs. without headgear, impact attenuation of headgear in lab studies.
Results
Eighteen studies were identified as eligible: qualitative (N = 4), field (N = 7), and lab (N = 7). Qualitative studies showed low rates of headgear use and varying understanding of the protection afforded by headgear. Field studies showed negligible association of headgear use with reduced impact magnitude in headgear vs. non-headgear cohorts. Lab studies showed increased energy attenuation for thicker headgear material, poorer performance of headgear after repetitive impacts and increased drop heights, and promising recent results with headgear composed of viscoelastic polymers.
Conclusions
Rates of adoption of soft-shell headgear remain low in rugby and any association between its use and reduction in acceleration impact forces remains unclear. Lab results indicating improved impact attenuation need to be validated in the field. Further headgear-related research is needed with youth and female rugby players.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The need for a systematic review into the effectiveness of rugby headgear takes place within a wider health context. Traumatic brain injury (TBI) is a major global health issue, affecting up to 55 million people in a given year [1]. The majority (70–90%) of TBI are classified as mild (mTBI), with sports-related concussion (SRC), including rugby, a significant contributor to these numbers [2]. In the United States it is estimated 1.1–1.9 million SRC occur every year in children aged 0–18 [3]. Sports-related concussion numbers are increasing in parallel with public awareness of concussion [4].
There is increasing concern regarding concussion in contact sports, including rugby union, and if practical measures, such as headgear use, can mitigate its risk [5, 6]. In most concussion cases, symptoms resolve spontaneously and within a month [7], but some players develop a post-concussive syndrome with a variety of somatic, cognitive, and emotional symptoms [8]. Various factors for reducing concussion incidence have been proposed including rule changes, playing techniques, and the use of protective equipment, including helmets and headgear [9].
Rugby union is a popular contact sport played by 9.6 million people in 123 countries [10]. Collisions are inherent in the game. Peak linear acceleration (PLA) forces have been recorded up to 165 g [11] and have occurred at velocities of up to 13.8 m/sec [12]. Rugby players are, therefore, at a higher risk of injury compared to other contact sports [13]. While there is no currently agreed threshold on what impact results in a concussion [14], data from professional rugby in England reports increasing incidence (up to 17.9 concussions per 1,000 player hours in the 2017–2018 season [15]) while a 2021 review listed rugby as the highest risk contact sport with incidence of 28.25 per 10,000 athlete exposures [16]. Rugby tends to be over-represented in concussion incidence numbers versus other sports [17] and concussion-related injuries account for 25% of all days lost from rugby participation [5].
Within this wider context, the current systematic review seeks to review the use and effectiveness of soft-shell headgear in rugby union, i.e. what is the established research base regarding:
-
(1)
Use rates of soft-shell headgear in rugby union
-
(2)
Consumer understanding of protection provided by soft-shell headgear in rugby union
-
(3)
The effectiveness of soft-shell headgear in rugby union to mitigate concussion and head injury
-
(4)
The capacity of soft-shell headgear to reduce linear and rotational impact forces
Regarding the first three aims, current rates of headgear use appear to be low. Barnes et al. quoted 36% of players wear headgear regularly [18], and this usage rate has remained essentially the same over the last twenty years ranging from 12 to 33% in earlier studies [5, 19]. There is wide variety in invested parties’ understanding of the protection headgear affords against head injury or concussion (37–62%) [18,19,20,21]. Measuring the effectiveness of this protection is more challenging to establish; Benson et al. [22] reported that although protective equipment, such as helmets, has been shown to be effective in concussion reduction in pursuits such as cycling and American football, less evidence has been demonstrated with rugby headgear [22].
Regarding the final aim, the need for the current paper addressing effectiveness of headgear in rugby union is timely as World Rugby (WR) recently approved a medical device trial process allowing thicker, denser headgear to be used in games designed to improve player welfare [23]. Previously WR had only permitted one class of headgear, and this was primarily used to prevent lacerations, scalp injury, and cauliflower ears. This change in WR policy has led to more recent studies incorporating headgear, such as NPro, which is composed of impact-reducing viscoelastic polymers [11, 24]. NPro claims its headgear is “scientifically proven to provide impact protection.” [25].
Previous systematic reviews have looked at headgear effectiveness across a diverse range of sports, leisure pursuits, and study designs: soft-shell headgear and concussion in youth collision sports [26], effectiveness of interventions in reducing brain injuries in rugby [27], concussion prevention of all protective equipment [22], all concussion prevention strategies [6], strategies to reduce concussion risk in all sport [28], concussion in rugby [17], incidence of concussion in youth sport [29], helmet design in sport [30] and considerations for requirements of soft-shelled headgear [31]. At the time of writing, no such review has been published looking specifically at rugby union headgear regarding the above aims.
Methods
The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [32].
Quality and level of evidence assessment
The review utilized the following reporting standards to evaluate article quality and reduce risk of bias:
Observational studies were analysed according to the Strengthening and Reporting of Observational Studies Epidemiology (STROBE) [33].
Qualitative studies were analysed according to the Standardized Reporting of Qualitative Research (SRQR) [34].
Laboratory studies were analysed according to an author-generated checklist based on recommendations adapted from Benson et al. [22]. This checklist was generated in consultation with co-author (ND) and was generated using recommendations from the Benson et al. article, namely that studies of this type are of sufficient power to determine true concussion risk, specify exact properties of tested equipment, assess headgear that is or would be used in gameplay, and study injury mechanisms that are consistent with examples from the field. The article further recommended a clear operational definition of concussion be used rather than the more generic term of head injury. Such parameters were included in the checklist visible in Table 6.
Data sources
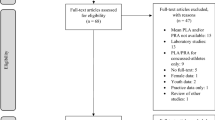
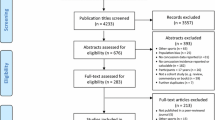
A systematic search was conducted in July and August 2021 using the databases SPORTDiscus, PubMed, MEDLINE, CINAHL (EBSCO), Scopus, and ScienceDirect (see Fig. 1). Reference lists of selected studies and relevant reviews were also hand-searched to identify pertinent articles not identified by initial search strategies.

PRISMA flowchart showing systematic exclusion of articles at each stage of the review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses
The protocol for this systematic review was registered on PROSPERO and can be accessed at https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=239595
Study selection
Studies were included when the population included rugby union players (junior, senior, male and female, amateur and professional) and coaches. Studies were included within the following parameters: incidence studies, observation studies, interventions, and perceptions of use. Studies were included with the following research designs: randomised controlled trials (RCTs), observational, intervention, surveys, questionnaires, focus groups.
Studies were excluded when they were reviews, commentaries, not related to the use of soft-shell headgear, or when related to sports other than rugby union.
Two review authors (SH and KA) independently screened manuscripts using title and abstract, selecting studies based on the inclusion of keywords (head injury, brain injury, concussion, rugby, rugby union, headgear, scrumcap, head guard, soft-shell headgear). The reviewers then screened the selected manuscripts in full text. The two review authors (SH and KA) identified the same studies to be included, some papers were included or excluded after review author (SH) performed a closer reading of each included study. Included studies have been reviewed using a narrative approach due to the heterogeneity present in their design. Due to this heterogeneity, a meta-analysis was not conducted.
Results
Of the 274 records identified after duplicates were removed, 41 were screened in full text for eligibility (the full text of one eligible study could not be accessed). Of these 41, 23 were excluded. Reasons for exclusion are listed in Fig. 1. After screening, 18 studies were included.
Study characteristics
All included studies were published between 2000 and 2021. Qualitative studies (N = 4) included three survey and one questionnaire design. Mixed methods designs were included in this section as they report qualitative data. A total of 870 participants (ranging from 63 to 545) took part in all studies, of which 106 were female (12.2%). Age ranged from 14 to 33, with one study looking exclusively at youth (under 15) and one study not stating its age range. Playing level ranged from junior (youth/under 15) to professional. All studies surveyed players, one study additionally surveyed coaches. No studies reported on socio-economic or racial factors. All studies reported rates of headgear use and perspectives on the level of protection provided by headgear. Four studies reported reasons for/against wearing headgear. Two studies reported players’ self-report on concussion incidence. Results are summarised in Table 1.
Field studies (N = 7) included three prospective cohort studies (PC), two randomised controlled trials (RCT), one retrospective cohort study (RC), and one survey design. A total of 9,905 participants took part in all studies, of which just 87 were female (0.88%). The effect studied regarding headgear was incidence of concussion of players wearing headgear vs. players not wearing headgear. One study additionally assessed modified vs. standard headgear, while another additionally assessed days absent from concussion in headgear vs. non-headgear users. Two studies reported time loss from concussion. All studies looked at concussion incidence during match-play, one study also looked at training. Although the Marshall et al. [5] study conducted telephone interviews, it was included in this category as its primary outcomes were injury rates. The Kahanov [20] study was included as it reported quantitative data (closed-ended questions) in its survey. Playing level ranged from under-15 to professional. Two studies exclusively looked at youth (under-20) populations. Results are summarised in Table 2
Lab studies (N = 7) included a variety of methods for dropping headforms onto a surface. Drop heights ranged from 20 to 91.2 cm. Numbers of headgear tested ranged from two to ten. Criteria for drop testing followed standards set by World Rugby (WR) [35] or the National Operating Committee on Standards for Athletic Equipment (NOCSAE) [36]. Six studies looked at repetitive impacts. All studies used a variety of impacts sites on the headforms. Five studies measured peak linear acceleration (g), two measured impact energy (J) or the Head Impact Criterion (HIC), and one measured impact velocity (m/s) or the Gadd Severity Index [37]. One study additionally measured peak rotational acceleration (rad/s/s). Results are summarised in Table 3.
Quality and levels of evidence results
Two reviewers (SH and ND) independently assessed the quality of studies.
Qualitative studies
Qualitative studies were analysed according to the Standards for Reporting Qualitative Research (SRQR) checklist [34]. Results can be seen in Table 4. Results show commonalities of research design principles present in most studies. Titles, abstracts, results, and discussion sections generally adhered to the checklist, although three studies [21, 38] provided only partial information for item 4 (purpose or research question). Methods sections were less adherent, with no studies providing adequate information for item 5 (qualitative approach and research paradigm) and one study [38] providing information for item 6 (researcher characteristics and reflexivity). Information on data collection methods, instruments, and processing was minimal in two studies [19, 21]. Similarly, the ‘other’ section of the checklist revealed discrepancies: one study did not provide information on conflicts of interest [19], and only one study provided information on funding [38].
Field studies
Observational field studies were analysed according to the Strengthening and Reporting of Observational Studies Epidemiology (STROBE) [33]. Results can be seen in Table 5. Direct comparison of all studies was problematic due to variability in research design and concussion definition. Common limitations of field studies included unclear objectives, lack of clearly defined variables (especially potential confounders), unclear explanation of quantitative variables (such as why groupings were chosen), and inadequate descriptions of study limitations.
Regarding headgear use, there is a general lack of specific information on headgear wearing rates such as not reporting on the number of participants who actually wore headgear in each group. The Hollis et al. and Kahanov et al. studies relied on a questionnaire or survey asking about headgear use at a single point in the season [39]. This is problematic, as the reported rates of concussion are reliant on accurate description of headgear use. The Marshall et al. study was found to be susceptible to self-report bias as the authors were reliant on obtaining injury data from players on a weekly basis, and such reports were gathered by telephone [40]. By contrast, other studies involved direct observation by trained personnel. Video verification was used in the Stokes et al. study (all games) [41] and the McIntosh and McCrory study (six randomly chosen games) [42].
Regarding validity, the Kemp study used a wide definition of concussion which may have overestimated incidence rates [43]. The Marshall et al. study included wide demographic variation (different age groups, levels of play, different genders) which may decrease the specificity of its findings towards a particular target population [40]. The McIntosh and McCrory study had a lack of control for confounding variables [42]. All other studies adjusted for confounding variables, thereby improving internal validity. External validity appeared sound; no evidence exists to suggest the staff, places, and facilities described in studies were not representative of the environments to which participants would normally be exposed.
Studies did not consider that higher risk-taking behaviour may negate benefits of headgear prevention, but there is also potential bias in incidence data if players wearing headgear played more conservatively. Training exposure was only captured in one study [40]. The Hollis et al., Stokes et al., and Marshall et al. studies included adjusted rate ratios accounting for previous injury [39,40,41], therefore the remaining three studies may have over-estimated incidence by not considering this variable [42,43,44].
Studies consistently refer to the challenging nature of objectively defining concussion. Participants may have sustained sub-clinical concussions or other head trauma, making them more susceptible to concussion despite the use of protective equipment. There is variation on the standards used to measure injury and concussion incidence: four studies used player-hours [39, 41, 43, 44], the remaining two used concussion time-loss [40, 42]. The Hollis et al. study lists its outcome as mTBI rather than concussion [39]. Baseline concussion history was only reported by Hollis et al. [39]. The Kahanov et al. study did not report an outcome measure of effect, had self-reported concussions, and did not use a denominator to calculate incidence rates [20].
Lab studies
Experimental lab studies were analysed. Direct comparison of all studies was problematic due to variability in measurements used to assess impact acceleration and attenuation. Given the lack of a standard quality assessment tool for lab studies, a checklist was generated using a model adapted from Benson et al. [22]. Results can be seen in Table 6. Lab-based study designs lack external validity, namely, game and practice conditions differ from laboratory settings and the impact forces required to produce concussion are not agreed upon [14]. All studies reported on the validity and variability of the testing apparatus used. Levels of evidence in lab studies are dependent on multiple factors.
All studies report on types of headgear studied. The McIntosh et al. study used a modified headgear model with increased bulk [45]. Commercially available headgear is more likely to be worn by players but tended to perform worse on impact tests. The three most recent studies used a no headgear condition to act as a control [11, 24, 46]. Therefore, these studies provided more valid comparisons of headgear performance vs. a baseline. The two McIntosh studies provided information on foam testing [45, 47]. All studies reported on the headgear used (density range 45–87 kg/m3; thickness range 7–20 mm). Two studies did not provide detail on the thickness and density of headgear used but do provide information on brands used [24, 46]. The Knouse et al. and Draper et al. studies provided the greatest detail in makeup of the type of headgear (honeycomb vs. flat panel), thickness, and density [11, 12]. The Hrysomallis and McIntosh studies (N = 3) did not report on the cellular makeup of the foam present in the headgear [45, 47, 48].
All studies except Hyrsomallis [48] used repetitive impact testing and its rationale for use, i.e. mirroring repetitive impacts experienced in gameplay. Number of repetitions varied from two to ten times. The Ganly and McMahon study carried out a separate repeated impact test on the NPro headgear, involving 1,920 impacts, to simulate up to three years of use [24]. All studies reported on the sites of impacts tested. Three studies reported on the lack of padding at the back of headgear [11, 12, 48], suggesting impacts received to the unprotected occipital region might result in higher impacts than front or side impacts. The Ganly and McMahon study included pendulum testing on two moving headforms thereby replicating on-field head-to-head contacts, but did not test impact to the back of the head [24]. The Draper et al. study justified inclusion of side impacts as the most common impact site in gameplay [11].
Most studies did not report testing headgear in different environmental conditions (wet, humid, temperature). Four studies [12, 45, 47, 48] reported testing took part in ambient temperature (20–22 °C) while the McIntosh et al. study reported testing headgear in ambient, hot (50 °C), and cold (− 10 °C) temperatures [47]. All studies reported using spherical headforms in testing, McIntosh and McCrory provided more detail in describing a deformable skin more like a human head [45]. Four studies [11, 24, 45, 47] reported the use of a Hybrid III headform [49]. Two studies reported on details of the glycerine “brain” encased inside a sealed cranium and included details on the “neck” of the headform [12, 48]. All studies reported on the details of the impact surface used. The McIntosh et al. study used a flat, rigid force plate which may not mimic impact of a spherical human head as effectively [47]. All studies reported on the makeup of the impact pad, with three studies reporting on the thickness of the impact pads used (1–1.6 cm, 1.3 cm, 2.5 cm, respectively) [11, 12, 47]. The Frizzell et al. study used an artificial pitch impact pad to mimic gameplay [46].
Regarding the measurement of rotational as well as linear acceleration, one study (Ganly & McMahon) reported data on peak rotational acceleration (PRA) but provided less detail on its results [24]. The Draper et al. study asserted there is no currently accepted method to measure PRA [11]. Regarding outcome values, two studies reported peak acceleration (g) values only [46, 47]. Three studies reported both peak acceleration and HIC [11, 45, 48]. The Knouse et al. study also used the Gadd Severity Index [12]. The Ganly and McMahon study also measured rotational acceleration (rads/s2) and velocity (km/h) [24], but two studies reported PRA is not currently able to be studied adequately under lab conditions at this time [11, 46].
All studies reported on the details of the drop testing rigs used to measure linear acceleration. The Ganly and McMahon study also used a pendulum rig to simulate head-to-head player contact [24]. All studies report on height and impact energy. The McIntosh et al. and Frizzell et al. studies did not report mass [46, 47]. The Knouse et al. and Frizzell et al. studies did not report velocity [12, 46]. The Knouse et al. and Draper et al. studies provided detail on the use of twin wires to guide the headform onto the anvil and reported on calibration of the testing rig prior to study commencing [11, 12].
Regarding the quoting of authority standards used in approving equipment and procedures, four studies reported on using NOCSAE standards [11, 24, 46, 48]. The Frizzell et al. study did not report on World Rugby standards for headgear [46]. The three most recent studies [11, 24, 46] quoted EN960 standards for headforms used [50]. The McIntosh et al. study provided minimal information on approval specifications for the testing rig [47], while the Hrysomallis study calculated mean impacts for concussion from previous field reports [48]. Frizzell et al. quoted popularity of artificial pitches in choosing its impact pad [46].
Finally, reporting on statistical analyses varied. The two McIntosh studies did not report statistical analysis used [45, 47]. The Hrysomallis study did not explain which statistical analysis was used in its methods section, but quoted correlation co-efficients in its results section [48]. The four remaining studies utilized multiple data analysis methods, which may improve internal validity [11, 12, 24, 46].
Discussion
The aim of this systematic review was to review the use and effectiveness of soft-shell headgear in rugby union. Despite the variation across different study types and designs, several commonalities and trends can be observed. The use of headgear in rugby fits within a larger framework of both (a) protective equipment use and injury prevention within the sport and (b) concussion mitigation strategies, including rule changes such as lower tackling height, and proper tackling techniques which may better protect the head in contact. Outcome variables (numbers of papers related to each objective of this review vs. study type) are summarised in Table 7, and the discussion section is organised according to each objective.
Use rates of soft-shell headgear in rugby union
Although helmets have a long history of use in sport [51] and headgear use has been sanctioned by World Rugby since 1993 [52] headgear usage rates in rugby remain low. To date Japan is the only country to mandate headgear use in rugby [52]. Marshall et al. reported overall headgear use of 14.2%, with 32.6% of schoolboys and just 1% of women players wearing it [5]. This is generally reflective of headgear use rates quoted in qualitative studies used in this review. Little evidence is present to suggest a change in headgear use trend, although junior players tend to wear headgear at higher rates [5, 38].
Many factors were cited for the use or non-use of headgear. Reasons cited in the wider literature include players being told to wear headgear by their parents [53] or due to parental concern over concussion as awareness of SRC increases [54, 55]. Other usage reasons were often repeated in studies included in this review. These may be broadly arranged into the following categories: cost, comfort, utility (scalp/laceration protection), utility (concussion prevention), and aesthetics. Even if studies can show improvement in one targeted area, namely utility: concussion prevention, the other categories may remain as barriers to increasing usage rates.
The qualitative studies in the review all report headgear usage rates, but some may not have high levels of external validity. One reason for this may be lack of representative samples used in these studies. Although female players represent 23% of players worldwide [28], just 10.6% of respondents in quoted studies were female [18,19,20,21, 38]. Although usage rates and attitudes towards headgear of female players appears to mirror that of males [53], better adherence to items 5 (qualitative approach and research paradigm) and 6 (researcher characteristics and reflexivity) on the SRQR checklist could result in higher reporting quality for gender, socio-economic, and socio-cultural factors. No included qualitative studies adequately addressed these issues in their methodology.
External validity may also be impacted by issues of compliance in headgear use and reliance on self-reporting. McIntosh et al. expressed concern over consistency of headgear use throughout the season [44]. Other studies mentioned players may only wear headgear due to another extraneous factor, such as when recovering from head or scalp injury [18, 38]. In a clinical commentary on the McIntosh et al. study, Swartz and Marshall describe this lack of compliance as a “profound” limitation of the study [56]. This issue may be partially solved by having participants as own controls. If players choose to wear headgear then compliance may improve as by doing so they are demonstrating an understanding of the reasons for headgear use. Subsequently, the reliability of results in studies with similar designs may increase.
Consumer understanding of protection provided by soft-shell headgear in rugby union
Multiple relevant points regarding understanding of protection were raised by qualitative and field studies. Several studies reported the supposed link between use of protective equipment and the concept of risk compensation first described by Hagel a21nd Meeuwisse [57]. Of note Menger et al. reported players who believed headgear prevented concussion were four times more likely to play aggressively []. This concern has been mentioned in media reports [58], but has not been backed up by other studies. Patton and McIntosh found that players who stated they would “tackle harder” when wearing headgear were less likely to continue to hold that opinion after a season of playing [31]. Rivara et al., in a consensus statement, concluded there is insufficient data to suggest such risk compensation exists [59].
Generally, studies show players were not confident in the ability of headgear to prevent concussion. Pettersen and Kahanov et al. reported more than half of the players in their studies believe headgear “often” or “sometimes” prevents concussion [19, 20]. This is not generally reflected in the wider literature however, and a more recent study reported just 10% of participants wore headgear to prevent concussion [18]. Moreover Reid et al. reported 98% of their study’s participants recognise headgear does not prevent SRC [60]. Although conflation of the terms head injury and concussion is problematic, this may represent a trend in increased awareness of headgear effectiveness and concussion knowledge in general. The validity of this trend may be backed up by Zuckerman et al. who found no significant difference in performance on neuro-cognitive tests between cohorts of helmeted and un-helmeted athletes after sustaining an SRC [61].
These findings are particularly relevant to the youth population. Junior players tend to wear headgear at higher rates and may have more confidence in its protective qualities [5, 18,19,20,21]. Children play contact sport at a higher rate than adults and are generally over-represented in concussion numbers [2, 4, 62]. Kuhn et al. reported concern over children regarding the relative size of their heads compared to their body, their less developed neck musculature resulting in higher risk of injury at the cranio-cervical juncture, and that children may experience greater angular acceleration given tangential impact [30]. The authors suggest none of these factors would be lessened by the use of headgear.
The effectiveness of soft-shell headgear in rugby union to mitigate concussion and head injury
The outcomes of all studies suggest the effectiveness of headgear in preventing or mitigating the effects of concussion remains unclear. Qualitative studies generally did not report incidence, but Kahanov et al. listed 32 concussions in participants wearing headgear vs. 104 without (but no effect of measurement was given) [20]. In field studies incidence varied, but only Kemp et al. reported a significant protective effect of headgear with an incidence in the headgear group of 2.0/1,000 players hours vs. 4.6 for the non-headgear group [43]. Hollis et al. (2009) reported reduced risk for players always wearing headgear (IRR 0.57) [39]. Lab studies, particularly more recent studies involving more recently developed technology, reported generally more promising findings, but these have yet to be generalised to the field [11, 24, 46]. Although not looked at specifically in this paper, animal studies have found headgear offered significant protection from moderate mTBI symptoms in animal models [63].
Regardless of the quality of reporting in the reviewed studies multiple factors regarding concussion pathophysiology cannot be adequately addressed. Lab and field studies focus on direct impact to the head, but TBI and concussion can also be caused by non-direct, inertial impacts (commonly referred to as “whiplash”) for which helmets or headgear likely offer little protection [14]. The Concussion in Sport Group (CISG) defines this as a blow “elsewhere on the body with an impulsive force transferred to the head” [64]. The acceleration-deceleration of these events has been suggested as injurious to the brain in contact sports [51, 65,66,67]. Moreover, Sone et al. suggested it is more difficult to design helmets that reduce low-impact accelerations and peak pressures that are distributed throughout the brain [51].
Rugby has relatively few catastrophic injuries [68, 69] suggesting repetitive, low impact collisions may be more strongly associated with concussion. King et al. estimated the average amateur rugby player can expect 77 impacts per game [70]. Many of these impacts are low impact, whereas large linear forces, such as one causing a skull fracture, is not necessarily associated with TBI [71]. Moreover, multiple studies show the tackle as the primary concussion mechanism in gameplay [68, 72] and that lowering tackle height does not decrease concussion incidence [73, 74]. This suggests the inertial and rotational forces of tackle impacts, even without direct contact to the head, can still result in concussion. Similarly, the headforms used in lab studies often lack a “neck” and therefore cannot replicate rotational impacts typically associated with concussion [75].
An obstacle in attempting to compare these studies is a lack of a consistent operational definition of concussion. Although all field studies reported some definition of concussion, or reported concussion was verified by a physician or trainer, reviews often quote this as being a potential source of bias [6, 22, 26, 27, 64]. In addition to having trained personnel making observations in the field, it has been suggested that video analysis with software coding [72, 76,77,78,79] and the use of instrumentation such as mouthguards [70, 80] or skin patches [81, 82] would help in verification of collision events [31, 69].
The capacity of soft-shell headgear to reduce linear and rotational impact forces
Despite recent lab studies showing promising impact attenuation of NPro and Gamebreaker units [11, 24], the most recent field study [41] did not find evidence of headgear reducing concussion risk, suggesting the trend over time has not changed. Although headgear is positively correlated with prevention of scalp and laceration injuries [83] concussion risk appears to be mostly unchanged. This is inclusive of the youth population, where headgear usage rates are higher. Another confounding variable is the lack of knowledge and agreement on the concussion threshold. King et al. reported concussive events as low as 54.9 g [70], but Guskiewicz and Mihalik concluded the threshold is elusive and may be irrelevant [14]. Therefore, clarification of the size of an impact that will likely result in concussion remains unclear, but scales such as the Head Impact Criterion (HIC) remain a useful way to measure impact severity [11].
Biomechanical lab studies conducting drop tests using headforms have recently produced more promising results in impact attenuation of headgear [11, 24, 46]. Lab studies tend to use more objectively measurable outcomes, such as HIC and NOCSAE [37, 84]. Recently the need for experimental validation in all theoretical aspects of biomechanical lab studies has been emphasized [85, 86]. Challenges in the generalisation of these studies remain though. Draper et al. stated that peak rotational acceleration (PRA) cannot be adequately studied as no accepted method of quantifying it currently exists [11]. Hernandez et al. suggested headform testing is unable to produce acceleration directions common in field impacts due to the physical limitations of lab equipment [75]. Rowson and Duma stated combined information on PRA and PLA is needed to assess the probability of concussion [87].
The makeup and design of rugby headgear is also relevant to this analysis. In lab studies as early as 2000 authors were making recommendations for minimum thickness of 12.5–16 mm to provide adequate thickness for impact attenuation [45, 47, 48]. Concern was also raised by Knouse et al. regarding the relatively open back design of rugby headgear, potentially increasing the likelihood of occipital region concussions [13]. Earlier studies reported flat panel headgear had superior attenuation performance [12, 47] compared to honeycomb headgear designs, but McIntosh et al. only reported this difference at higher drop heights [47]. In reviews of these earlier studies, Benson et al. described the results as inconclusive [22] while Patton and McIntosh (2016) suggested including oblique tests would better assess concussion risk reduction [31].
More recent studies, conducted since World Rugby’s approval of headgear as a medical device, have reported on the density of the foam used in headgear. The better performing headgear in two studies were either composed of open-cell polyurethane foam or ethylene vinyl acetate (EVA) foam with a layer of impact-absorbing foam composed of viscoelastic polymers [11, 24]. These studies suggest better impact attenuation than previous studies. Frizzell et al. reported superior impact reduction on the side of the head [46], which is significant as the temporo-parietal region has been reported as the most common site for head impact during play [79, 88]. Although increased density may help with impact attenuation, increased headgear bulk may influence wearing preference, as well as increasing mass on top of the player’s neck [48]. The most recent reviews did not look at lab studies [26, 64].
Directions for future research
Despite the risk of concussion in rugby much of the literature mentions the generally positive impact of youth sports outweighing its risks [59]. More research is needed in multiple areas, namely (a) the involvement of female players and teams; (b) the use of instrumented mouthguards and better systems of surveillance; (c) more field studies to validate lab findings; (d) a greater focus on youth populations; (e) objective measurement of impacts and collisions in field studies, rather than using concussion incidence as the primary outcome measure; (f) to establish a threshold for concussions and an understanding of against what types of impacts protection is required; (g) improved methods to study headgear performance at impact protection; and (h) reducing concussion risk itself within the framework of rugby rules and regulations.
An additional consideration for headgear-based field studies regards the ethical considerations around performing randomized trials involving headgear vs. no-headgear cohorts [51] and the fact blinding cannot be used in direct observational studies. Additionally, the problem of using concussion incidence as an outcome measure remains due to a lack of clear operational definition, ongoing issues with the accuracy of reporting, and disagreement over the threshold required for concussive injury [22, 31, 64]. If studies purport to measure concussion, or an impact that may result in concussion, then a consistent operational definition of concussion should be clearly stated [17, 26, 59]. If a survey or questionnaire is given to players asking about head injury this may skew results. Head injury is a wider term which includes skull fracture, lacerations, facial fractures, dental injuries, and eye injuries and so should be avoided in concussion studies [22].
Current best practice suggests using more objective outcome measurement of collision impacts and matching these to physician-verified concussive events. This is valid as the link between head impacts and concussion has been well documented [5, 17, 67]. Ideally more than one measurement (such as video analysis and instrumentation) should be used to rule out false positives and quantify collision frequency, velocity, and acceleration. Results of field studies could then be replicated under lab conditions to confirm findings. If such headgear is shown to be effective in impact attenuation in the lab and in the field this could result in more players electing to wear it.
The wider literature also strongly suggests combining any use of headgear and protective equipment with a wider program of concussion prevention. This may include collaboration with coaches (Salmon et al. reported coaches as the primary point of contact for concussion reporting [62]), and education programs such as RugbySmart [89, 90]. Evidence on physical conditioning and rule changes in preventing concussion is more equivocal. Garnett et al., in a scoping review, showed limited results (especially in the adolescent population) [91] while Hislop et al. demonstrated reduced concussion incidence in an intervention group who had undertaken an exercise programme [92]. Two studies reported increased concussion rates when rugby laws were changed to lower tackle height [73, 74].
Other factors should be considered when assessing the role of protective equipment in rugby. Discussion of concussion mitigation speaks to a wider issue of injury safety. Rugby in New Zealand remains very popular, but youth participation rates have fallen by 24.1% in the last twenty years [93]. Parental concerns regarding safety in rugby and other football codes, has been raised in the media where it is often linked to concussion and decreasing playing numbers [94, 95]. Parental concerns regarding sport injury safety and risk have been mentioned in the literature with particular emphasis given to rugby and other football codes [96, 97]. Future studies should consider these variables.
Limitations
This systematic review was subject to multiple limitations. The heterogeneity of included studies resulted in difficulty comparing studies across different designs and populations. This necessitated a narrative approach to analysis which may hinder objectivity and negated the ability to perform a meta-analysis. Comparison between study designs (qualitative vs. field vs. lab) is problematic, but even comparison within these areas is difficult due to their heterogeneity. This is particularly true in field studies, which may use varying outcome measures. Moreover, the results of these diverse studies are challenging to generalize to a wider research area. The efficacy of helmets and headgear are specific to a particular sport (in this case rugby), necessitating the use of smaller, more localized cohorts, thereby decreasing the statistical power of findings. Any discussion of headgear must also involve a long list of confounding variables in its use and effectiveness, such as reasons for and against wearing headgear (qualitative studies), differences in age and skill level (field studies), and testing in different environmental conditions (lab studies). If studies purport to measure concussion, or an impact that may result in concussion, then a consistent operational definition of concussion should be clearly stated. Head injury is a more generic term and should not be conflated with concussion.
Conclusion
This review focused on the perceived and measurable ability of headgear to reduce concussion in rugby union. As concussion is difficult to define, future research could focus on measuring collisions. Such research could benefit from multiple verification measures such as instrumented mouthguards. Qualitative studies show improved understanding of headgear use, while also highlighting the need for further education. While recent lab studies show promising results in new headgear design, these results need to be replicated in the field. Any recommendations for headgear use must be used in conjunction with clear protocols regarding rules of the game, head injury assessment, education, and tackling techniques. Other risk factors, such as concussion history, should also be considered. Psychological, gender, and socio-cultural factors may also play a role in the implementation of any concussion prevention strategy, of which headgear use may be considered one component.
Data availability statement
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- TBI:
-
Traumatic brain injury
- mTBI:
-
Mild traumatic brain injury
- SRC:
-
Sports-related concussion
- PLA:
-
Peak linear acceleration
- PRA:
-
Peak rotational acceleration
- WR:
-
World rugby
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- STROBE:
-
Strengthening and Reporting of Observational Studies Epidemiology
- SRQR:
-
Standardized Reporting of Qualitative Research
- RCT:
-
Randomised controlled trial
- PC:
-
Prospective cohort study
- RC:
-
Retrospective cohort study
- NOCSAE:
-
National Operating Committee on Standards for Athletic Equipment
- HIC:
-
Head impact criterion
- CISG:
-
Concussion in sport group
- EVA:
-
Ethylene vinyl acetate
References
GBD (2019) Traumatic brain injury and spinal cord injury collaborators. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol 18(1):56–87
CDC. The management of traumatic brain injury in children: Opportunities for action. Centers for Disease Control. 2018. Available from: https://www.cdc.gov/traumaticbraininjury/pdf/reportstocongress/managementoftbiinchildren/TBI-ReporttoCongress-508.pdf. Accessed 6 Oct 2021.
Bryan MA, Rowhani-Rahbar A, Comstock RD, Rivara F (2016) Sports- and recreation-related concussions in US youth. Pediatrics 138(1):e20154635
Karlin AM (2011) Concussion in the pediatric and adolescent population: “Different population, different concerns.” PM R 3(10 Suppl 2):S369–S379
Marshall SW, Spencer RJ (2001) Concussion in rugby: the hidden epidemic. J Athl Train 36(3):334–338
Schneider DK, Grandhi RK, Bansal P, Kuntz GE, Webster KE, Logan K, Myer GD (2017) Current state of concussion prevention strategies: A systematic review and meta-analysis of prospective, controlled studies. Br J Sports Med 51(20):1473–1482
McCrory P, Meeuwisse W, Dvorak J, Aubry M, Bailes J, Broglio S, Vos PE (2017) Consensus statement on concussion in sport: the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med 51(11):838–847
Beauchamp MH, Aglipay M, Yeates KO, Desire N, Keightley M, Anderson P, Zemek R (2018) Predictors of neuropsychological outcome after pediatric concussion. Neuropsychology 32(4):495–508
Bonfield CM, Shin SS, Kanter AS (2015) Helmets, head injury and concussion in sport. Phys Sportsmed 43(3):236–246
WR. Global participation in rugby. World Rugby. 2018. https://resources.world.rugby/worldrugby/document/2020/07/28/212ed9cf-cd61-4fa3-b9d4-9f0d5fb61116/P56-57-Participation-Map_v3.pdf. Accessed 6 Oct 2021.
Draper N, Kabaliuk N, Stitt D, Alexander K (2021) Potential of soft-shelled rugby headgear to reduce linear impact accelerations. J Healthc Eng. 2021:5567625
Knouse CL, Gould TE, Caswell SV, Deivert RG (2003) Efficacy of rugby headgear in attenuating repetitive linear impact forces. J Athl Train 38(4):330–335
Hume PA, Theadom A, Lewis GN, Quarrie KL, Brown SR, Hill R, Marshall SW (2017) A comparison of cognitive function in former rugby union players compared with former non-contact-sport players and the impact of concussion history. Sports Med 47(6):1209–1220
Guskiewicz KM, Mihalik JP (2011) Biomechanics of sport concussion: quest for the elusive injury threshold. Exerc Sport Sci Rev 39(1):4–11
RFU. England professional rugby injury surveillance project. Rugby Football Union. 2019. Available from: https://www.englandrugby.com/dxdam/89/8994c1ba-17df-47a3-a4c6-8878ed6728d0/England%20PRISP%2018.19.pdf. Accessed 6 Oct 2021.
Van Pelt KL, Puetz T, Swallow J, Lapointe AP, Broglio SP (2021) Data-driven risk classification of concussion rates: a systematic review and meta-analysis. Sports Med 51(6):1227–1244
Gardner AJ, Iverson GL, Williams WH, Baker S, Stanwell P (2014) A systematic review and meta-analysis of concussion in rugby union. Sports Med 44(12):1717–1731
Barnes A, Rumbold JL, Olusoga P (2017) Attitudes towards protective headgear in UK rugby union players. BMJ Open Sport Exerc Med 3(1):e000255
Pettersen JA (2002) Does rugby headgear prevent concussion? Attitudes of Canadian players and coaches. Br J Sports Med 36(1):19
Kahanov L, Dusa MJ, Wilkinson S, Roberts J (2005) Self-reported headgear use and concussions among collegiate men’s rugby union players. Res Sports Med 13(2):77–89
Menger R, Menger A, Nanda A (2016) Rugby headgear and concussion prevention: Misconceptions could increase aggressive play. Neurosurg Focus 40(4):E12
Benson BW, Hamilton GM, Meeuwisse WH, McCrory P, Dvorak J (2009) Is protective equipment useful in preventing concussion? A systematic review of the literature. Br J Sports Med 43(Suppl 1):i56-67
WR. Laws by number. World Rugby. n.d. https://www.world.rugby/the-game/laws/law/4. Accessed 3 Sep 2021.
Ganly M, McMahon JM (2018) New generation of headgear for rugby: Impact reduction of linear and rotational forces by a viscoelastic material-based rugby head guard. BMJ Open Sport Exerc Med 4(1):e000464
NPro. AFL and rugby helmets. 2022. https://n-pro.com.au/. Accessed 8 Apr 2022.
Makovec Knight J, Nguyen JVK, Mitra B, Willmott C (2021) Soft-shell headgear, concussion and injury prevention in youth team collision sports: a systematic review. BMJ Open 11(6):e044320
Cusimano MD, Nassiri F, Chang Y (2010) The effectiveness of interventions to reduce neurological injuries in rugby union: a systematic review. Neurosurgery 67(5):1404–1418
Emery CA, Black AM, Kolstad A, Martinez G, Nettel-Aguirre A, Engebretsen L, Schneider K (2017) What strategies can be used to effectively reduce the risk of concussion in sport? A systematic review. Br J Sports Med 51(12):978–984
Pfister T, Pfister K, Hagel B, Ghali WA, Ronksley PE (2016) The incidence of concussion in youth sports: a systematic review and meta-analysis. Br J Sports Med 50(5):292–297
Kuhn EN, Miller JH, Feltman B, Powers AK, Sicking D, Johnston JM (2016) Youth helmet design in sports with repetitive low- and medium-energy impacts: a systematic review. Sports Eng 20(1):29–40
Patton DA, McIntosh AS (2016) Considerations for the performance requirements and technical specifications of soft-shell padded headgear. Proc Inst Mech Eng P J Sport Eng Technol 230(1):29–42
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71
Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, Initiative S (2007) Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. Epidemiology 18(6):805–835
O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA (2014) Standards for reporting qualitative research: a synthesis of recommendations. Acad Med 89(9):1245–1251
WR. Regulation 12 schedule 1. World Rugby. 2016. https://www.world.rugby/news/155053. Accessed 22 Dec 2021.
NOCSAE. Standards. National Operating Committee on Standards for Athletic Equipment. n.d. https://nocsae.org/standards/. Accessed 9 Sep 2021.
Chou CC, Nyquist GW (1974) Analytical studies of the head injury criterion (HIC). SAE Trans 83:398–410
Finch CF, McIntosh AS, McCrory P (2001) What do under 15 year old schoolboy rugby union players think about protective headgear? Br J Sports Med 35(2):89–94
Hollis SJ, Stevenson MR, McIntosh AS, Shores A, Collins MW, Taylor CB (2009) Incidence, risk, and protective factors of mild traumatic brain injury in a cohort of Australian nonprofessional male rugby players. Am J Sports Med 37(12):2328–2333
Marshall SW, Loomis DP, Waller AE, Chalmers DJ, Bird YN, Quarrie KL, Feehan M (2005) Evaluation of protective equipment for prevention of injuries in rugby union. Int J Epidemiol 34(1):113–118
Stokes KA, Cross M, Williams S, McKay C, Hagel BE, West SW, Kemp S (2021) Padded headgear does not reduce the incidence of match concussions in professional men’s rugby union: A case-control study of 417 cases. Int J Sports Med 42(10):930–935
McIntosh AS, McCrory P (2001) Effectiveness of headgear in a pilot study of under 15 rugby union football. Br J Sports Med 35(3):167–169
Kemp SP, Hudson Z, Brooks JH, Fuller CW (2008) The epidemiology of head injuries in English professional rugby union. Clin J Sport Med 18(3):227–234
McIntosh AS, McCrory P, Finch CF, Best JP, Chalmers DJ, Wolfe R (2009) Does padded headgear prevent head injury in rugby union football? Med Sci Sports Exerc 41(2):306–313
McIntosh AS, McCrory P (2000) Impact energy attenuation performance of football headgear. Br J Sports Med 34(5):337–341
Frizzell ERA, Arnold GP, Wang W, Abboud RJ, Drew TS (2018) Comparison of branded rugby headguards on their effectiveness in reducing impact on the head. BMJ Open Sport Exerc Medic 4(1):e000361
McIntosh AS, McCrory P, Finch CF (2004) Performance enhanced headgear: a scientific approach to the development of protective headgear. Br J Sports Med 38(1):46–49
Hrysomallis C (2004) Impact energy attentuation of protective football headgear against a yielding surface. J Sci Med Sport 7(2):156–164
Humanetics. Hybrid iii 50th male. 2020. https://humanetics.humaneticsgroup.com/products/anthropomorphic-test-devices/frontal-impact/hybrid-iii-50th-male/hybrid-iii-50th-male. Accessed 9 Sep 2021.
iTeh I. Headforms for use in the testing of protective helmets. 2013. https://standards.iteh.ai/catalog/standards/cen/c5c9c77c-c6ed-472d-81a4-733a056b5093/en-960-2006. Accessed 9 Sep 2021.
Sone JY, Kondziolka D, Huang JH, Samadani U (2017) Helmet efficacy against concussion and traumatic brain injury: a review. J Neurosurg 126(3):768–781
Wilson BD (1998) Protective headgear in rugby union. Sports Med 25(5):333–337
Romiti M, McIntosh A, Grimison M (2005) Attitudes, beliefs and headgear wearing patterns of female rugby players. J Sci Med Sport 8(1):93
Clacy A, Sharman R, Goode N, Salmon PM, Lovell GP (2015) Responsibilities in the prevention of concussion in community rugby union. Procedia Manuf. 3:1173–1180
Lin AC, Salzman GA, Bachman SL, Burke RV, Zaslow T, Piasek CZ, Upperman JS (2015) Assessment of parental knowledge and attitudes toward pediatric sports-related concussions. Sports Health. 7(2):124–129
Swartz EE, Marshall SW (2011) Should helmets be worn in rugby? Athl Train Sports Health Care 3(1):12–14
Hagel B, Meeuwisse W (2004) Risk compensation: a “side effect” of sport injury prevention? Clin J Sport Med 14(4):193–196
Briggs S. Headguards in rugby would add to the concussion problem, not solve it says doctor. The Telegraph. 2014. Headguards in rugby would add to the concussion problem, not solve it, says doctor (telegraph.co.uk). Accessed 8 Oct 2021.
Rivara FP, Tennyson R, Mills B, Browd SR, Emery CA, Gioia G, Patricios J (2020) Consensus statement on sports-related concussions in youth sports using a modified Delphi approach. JAMA Pediatr 174(1):79–85
Reid D, Hume P, Whatman C, Theadom A (2020) Knowledge, attitudes, and behaviours of New Zealand physiotherapists to sports-related concussion. NZ J Physiother 48(1):19–28
Zuckerman SL, Lee YM, Odom MJ, Forbes JA, Solomon GS, Sills AK (2015) Sports-related concussion in helmeted vs Unhelmeted athletes: Who fares worse? Int J Sports Med 36(5):419–425
Salmon DM, McGowan J, Sullivan SJ, Murphy I, Walters S, Whatman C, Romanchuk J (2020) What they know and who they are telling: Concussion knowledge and disclosure behaviour in New Zealand adolescent rugby union players. J Sports Sci 38(14):1585–1594
Candy S, Ma I, McMahon JM, Farrell M, Mychasiuk R (2017) Staying in the game: a pilot study examining the efficacy of protective headgear in an animal model of mild traumatic brain injury (mTBI). Brain Inj 31(11):1521–1529
Gardner AJ, Quarrie KL, Iverson GL (2019) The epidemiology of sport-related concussion: what the rehabilitation clinician needs to know. J Orthop Sports Phys Ther 49(11):768–778
Barth JT, Freeman JR, Broshek DK, Varney RN (2001) Acceleration-deceleration sport-related concussion: the gravity of it all. J Athl Train 36(3):253–256
Evans RW (2010) Persistent post-traumatic headache, postconcussion syndrome, and whiplash injuries: the evidence for a non-traumatic basis with an historical review. Headache 50(4):716–724
Spiotta AM, Shin JH, Bartsch AJ, Benzel EC (2011) Subconcussive impact in sports: a new era of awareness. World Neurosurg 75(2):175–178
McIntosh AS, McCrory P, Finch CF, Wolfe R (2010) Head, face and neck injury in youth rugby: incidence and risk factors. Br J Sports Med 44(3):188–193
Patton DA (2016) A review of instrumented equipment to investigate head impacts in sport. Appl Bionics Biomech. 2016:1–16
King D, Hume PA, Brughelli M, Gissane C (2015) Instrumented mouthguard acceleration analyses for head impacts in amateur rugby union players over a season of matches. Am J Sports Med 43(3):614–624
Kleiven S (2013) Why most traumatic brain injuries are not caused by linear acceleration but skull fractures are. Front Bioeng Biotech. https://doi.org/10.3389/fbioe.2013.00015
Hendricks S, O’Connor S, Lambert M, Brown JC, Burger N, Mc Fie S, Viljoen W (2016) Video analysis of concussion injury mechanism in under-18 rugby. BMJ Open Sport Exerc Med 2(1):e000053
Stokes KA, Locke D, Roberts S, Henderson L, Tucker R, Ryan D, Kemp S (2021) Does reducing the height of the tackle through law change in elite men’s rugby union (The Championship, England) reduce the incidence of concussion? A controlled study in 126 games. Br J Sports Med 55(4):220–225
White AJ, Piggin J, Batten J, Turner G, Pearce A, Bullingham R, Anderson E (2021) Ethics and injury risk in world rugby and England rugby tackle-height trial. Br J Sports Med 55(4):183–184
Hernandez F, Shull PB, Camarillo DB (2015) Evaluation of a laboratory model of human head impact biomechanics. J Biomech 48(12):3469–3477
Hendricks S, Till K, den Hollander S, Savage TN, Roberts SP, Tierney G, Jones B (2020) Consensus on a video analysis framework of descriptors and definitions by the rugby union video analysis consensus group. Br J Sports Med 54(10):566–572
Hutchison MG, Comper P, Meeuwisse WH, Echemendia RJ (2015) A systematic video analysis of national hockey league (NHL) concussions, part i: Who, when, where and what? Br J Sports Med 49(8):547–551
Lincoln AE, Caswell SV, Almquist JL, Dunn RE, Hinton RY (2013) Video incident analysis of concussions in boys’ high school lacrosse. Am J Sports Med 41(4):756–761
McIntosh AS, McCrory P, Comerford J (2000) The dynamics of concussive head impacts in rugby and Australian rules football. Med Sci Sports Exerc 32(12):1980–1984
Camarillo D, Mattson J, Flynn M, Yang S, Shull P, Shultz R, Garza D (2013) Head contacts in collegiate football measured with an instrumented mouthguard. Br J Sports Med 47(5):e1.27-e1
King D, Hume PA, Gissane C, Clark TN (2016) Similar head impact acceleration measured using instrumented ear patches in a junior rugby union team during matches in comparison with other sports. J Neurosurg Pediatr 18(1):65–72
Wu LC, Nangia V, Bui K, Hammoor B, Kurt M, Hernandez F, Camarillo DB (2016) In vivo evaluation of wearable head impact sensors. Ann Biomed Eng 44(4):1234–1245
Jones SJ, Lyons RA, Evans R, Newcombe RG, Nash P, McCabe M, Palmer SR (2004) Effectiveness of rugby headgear in preventing soft tissue injuries to the head: a case-control and video cohort study. Br J Sports Med 38(2):159–162
NOCSAE. Standard performance specification for newly manufactured football helmets. 2021. Available from: https://nocsae.org/wp-content/uploads/2018/05/1501096770ND00217m17aMfrdFBHelmetsStandardPerformance.pdf. Accessed 6 Sep 2021.
Penta F, Amodeo G, Gloria A, Martorelli M, Odenwald S, Lanzotti A (2018) Low-velocity impacts on a polymeric foam for the passive safety improvement of sports fields: Meshless approach and experimental validation. Appl Sci 8(7):1174
Whyte T, Stuart C, Mallory A, Ghajari M, Plant D, Siegmund GP, Cripton PA (2019) A review of impact testing methods for headgear in sports: Considerations for improved prevention of head injury through research and standards. J Biomech Eng 141(7):1–29
Rowson S, Duma SM (2013) Brain injury prediction: assessing the combined probability of concussion using linear and rotational head acceleration. Ann Biomed Eng 41(5):873–882
King D, Hume P, Gissane C, Brughelli M, Clark T (2016) The influence of head impact threshold for reporting data in contact and collision sports: Systematic review and original data analysis. Sports Med 46(2):151–169
Gianotti SM, Quarrie KL, Hume PA (2008) Evaluation of RugbySmart: a rugby union community injury prevention programme. J Sci Med Sport 12(3):371–375
Quarrie K, Gianotti S, Murphy I, Harold P, Salmon D, Harawira J (2019) Rugbysmart: Challenges and lessons from the implementation of a nationwide sports injury prevention partnership programme. Sports Med 50(2):227–230
Garnett D, Patricios J, Cobbing S (2021) Physical conditioning strategies for the prevention of concussion in sport: A scoping review. Sports Med Open 7(1):31
Hislop MD, Stokes KA, Williams S, McKay CD, England ME, Kemp SPT, Trewartha G (2017) Reducing musculoskeletal injury and concussion risk in schoolboy rugby players with a pre-activity movement control exercise programme: a cluster randomised controlled trial. Br J Sports Med 51(15):1140–1146
NZSSSC. 2000 - 2020 change & trends in school sport representation by sport. School Sport NZ. 2021. https://www.nzsssc.org.nz/Education/School-Sport-NZ-Census-Reports. Accessed 15 Feb 2022.
NZ Herald. Smashed by players twice their size: Junior rugby's big problem. New Zealand Herald. 2014. https://www.nzherald.co.nz/nz/smashed-by-players-twice-their-size-junior-rugbys-big-problem/6M6NH5M5HD3XZ6C3JCOAPLWTRY/#:~:text=It%20was%20that%20the%20tackler,are%20putting%20children%20at%20risk. Accessed 8 Oct 2021.
Tso M. Rugby losing ground at high schools as students turn to other sports. Stuff. 2020. https://www.stuff.co.nz/sport/rugby/119251701/rugby-losing-ground-at-high-schools-as-students-turn-to-other-sports#:~:text=One%20of%20the%20Wellington%20region%27s,likes%20of%20basketball%20and%20futsal. Accessed 15 Feb 2022.
Boufous S, Finch C, Bauman A (2004) Parental safety concerns – a barrier to sport and physical activity in children? Aust NZ J Public Health 28(5):482–486
Telford A, Finch CF, Barnett L, Abbott G, Salmon J (2012) Do parents’ and children’s concerns about sports safety and injury risk relate to how much physical activity children do? Br J Sports Med 46(15):1084–1088
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Manuscript selection was performed by Kathryn Andrews and Stefan Henley. Quality of studies were independently assessed by Nick Draper and Stefan Henley. The first draft of the manuscript was written by Stefan Henley and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
The authors declare no financial or non-financial interests directly or indirectly related to this work.
Ethical approval and Informed consent
Ethical approval and informed consent were not sought for this systematic review as it does not involve direct research with human participants. The protocol for this systematic review was registered on PROSPERO and can be accessed at https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=239595.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Henley, S., Andrews, K., Kabaliuk, N. et al. Soft-shell headgear in rugby union: a systematic review of published studies. Sport Sci Health 19, 765–782 (2023). https://doi.org/10.1007/s11332-023-01058-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-023-01058-8