
Abstract
Aim
This study investigated differences in cognitive function between former rugby and non-contact-sport players, and assessed the association between concussion history and cognitive function.
Methods
Overall, 366 former players (mean ± standard deviation [SD] age 43.3 ± 8.2 years) were recruited from October 2012 to April 2014. Engagement in sport, general health, sports injuries and concussion history, and demographic information were obtained from an online self-report questionnaire. Cognitive functioning was assessed using the online CNS Vital Signs neuropsychological test battery. Cohen’s d effect size statistics were calculated for comparisons across player groups, concussion groups (one or more self-reported concussions versus no concussions) and between those groups with CNS Vital Signs age-matched norms (US norms). Individual differences within groups were represented as SDs.
Results
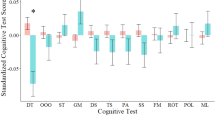
The elite-rugby group (n = 103) performed worse on tests of complex attention, processing speed, executive functioning, and cognitive flexibility than the non-contact-sport group (n = 65), and worse than the community-rugby group (n = 193) on complex attention. The community-rugby group performed worse than the non-contact group on executive functioning and cognitive flexibility. Compared with US norms, all three former player groups performed worse on verbal memory and reaction time; rugby groups performed worse on processing speed, cognitive flexibility and executive functioning; and the community-rugby group performed worse on composite memory. The community-rugby group and non-contact-sport group performed slightly better than US norms on complex attention, as did the elite-rugby group for motor speed. All three player groups had greater individual differences than US norms on composite memory, verbal memory and reaction time. The elite-rugby group had greater individual differences on processing speed and complex attention, and the community-rugby group had greater individual differences on psychomotor speed and motor speed. The average number of concussions recalled per player was greater for elite rugby and community rugby than non-contact sport. Former players who recalled one or more concussions (elite rugby, 85 %; community rugby, 77 %; non-contact sport, 23 %) had worse scores on cognitive flexibility, executive functioning, and complex attention than players who did not recall experiencing a concussion.
Conclusions
Past participation in rugby or a history of concussion were associated with small to moderate neurocognitive deficits (as indicated by worse CNS Vital Signs scores) in athletes post retirement from competitive sport.


Similar content being viewed by others


References
McCrory P, Meeuwisse WH, Aubry M, Cantu B, Dvořák J, Echemendia RJ, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. 2013;47(5):250–8.
King D, Gissane C, Brughelli M, Hume PA, Harawira J. Sport-related concussions in New Zealand: a review of 10 years of Accident Compensation Corporation moderate to severe claims and costs. J Sci Med Sport. 2014;17(3):250–5.
England Professional Rugby Injury Surveillance Project Steering Group. England Professional Rugby Injury Surveillance Project 2013–2014 Season Report. Twickenham. 2014.
Theadom A, Starkey NJ, Dowell T, Hume PA, Kahan M, Feigin V. Sports-related brain injury in the general population: an epidemiological study. J Sci Med Sport. 2014;17(6):591–6.
Quarrie KL, Murphy IR. Towards an operational definition of sports concussion: identifying a limitation in the 2012 Zurich consensus statement and suggesting solutions. Br J Sports Med. 2014;48(22):1589–91.
Carney N, Ghajar J, Jagoda A, Bedrick S, Davis-O’Reilly C, du Coudray H, et al. Executive summary of concussion guidelines step 1: systematic review of prevalent indicators. Neurosurgery. 2014;75:S1–2.
Kerr ZY, Register-Mihalik JK, Marshall SW, Evenson KR, Mihalik JP, Guskiewicz KM. Disclosure and non-disclosure of concussion and concussion symptoms in athletes: review and application of the socio-ecological framework. Brain Inj. 2014;28(8):1009–21.
Gardner A, Iverson GL, Williams WH, Baker S, Stanwell P. A systematic review and meta-analysis of concussion in rugby union. Sports Med. 2014;44(12):1717–31.
Kirkwood G, Parekh N, Ofori-Asenso R, Pollock AM. Concussion in youth rugby union and rugby league: a systematic review. Br J Sports Med. 2015;49(8):506–10.
Broglio SP, Eckner JT, Paulson HL, Kutcher JS. Cognitive decline and aging: the role of concussive and subconcussive impacts. Exer Sport Sci Rev. 2012;40(3):138–44.
Iverson GL, Brooks BL, Collins MW, Lovell MR. Tracking neuropsychological recovery following concussion in sport. Brain Inj. 2006;20(3):245–52.
Iverson GL, Gaetzy M, Lovell MR, Collins MW. Cumulative effects of concussion in amateur athletes. Brain Inj. 2004;18(5):433–43.
Hume PA, Quarrie K, Lewis G, Theadom A. IRB/NZR/AUT RugbyHealth project final report. A technical report to the International Rugby Board and New Zealand Rugby. Auckland: Sport Performance Research Institute New Zealand, Auckland University of Technology, New Zealand. 2015.
Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption—II. Addiction. 1993;88(6):791–804.
Gualtieri CT, Johnson LG. Reliability and validity of a computerized neurocognitive test battery CNS Vital Signs. Arch Clin Neuropsych. 2006;21(7):623–43.
Boyd A. CNS Vital Signs manual. 2015. http://www.cnsvitalsigns.com/WhitePapers/CNSVS-BriefInterpretationGuide.pdf. Accessed Feb 2015
Gualtieri CT, Johnson LG. Neurocognitive testing supports a broader concept of mild cognitive impairment. Am J Alzheimers Dis Other Demen. 2005;20(6):359–66.
Hopkins WG. A scale of magnitudes for effect statistics. In: Hopkins WG (ed). A new view of statistics. 2002. http://www.sportsci.org/resource/stats/effectmag.html. Accessed 26 Jan 2009.
Alberts JL, Linder SM. The utilization of biomechanics to understand and manage the acute and long-term effects of concussion. Kinesiol Rev. 2015;4(1):39–51.
DeKosky S, Ikonomovic M, Gandy S. Traumatic brain injury: football, warfare, and long-term effects. N Engl J Med. 2010;363:1293–6.
Hollis SJ, Stevenson MR, McIntosh AS, Shores EA, Collins MW, Taylor CB. Incidence, risk, and protective factors of mild traumatic brain injury in a cohort of Australian non professional male rugby players. Am J Sport Med. 2009;37(12):2328–33.
Shuttleworth-Edwards AB, Smith I, Radloff SE. Neurocognitive vulnerability amongst university rugby players versus noncontact sport controls. J Clin Exp Neuropsychol. 2008;30(8):870–84.
West S. Substance abuse among persons with traumatic brain injury: a review. Neurorehab Neural Repair. 2011;25(1):3–8.
Holsinger T, Steffens D, Phillips C, Helms M, Havlik R, Breitner J. Head injury in early adulthood and the lifetime risk of depression. Arch Gen Psychiatry. 2002;59(1):17–22.
Guskiewicz KM, Marshall SW, Bailes J, McCrea M, Harding HP, Matthews A, et al. Recurrent concussion and risk of depression in retired professional football players. Med Sci Sport Exer. 2007;39(6):903–9.
Lehman E, Hein M, Baron S, Gersic C. Neurodegenerative causes of death among retired National Football League players. Neurology. 2012;79(19):1970–4.
Casson IR, Siegel O, Sham R, Campbell EA, Tarlau M, DiDomenico A. Brain damage in modern boxers. JAMA. 1984;251(20):2663–7.
Gronwall D, Wrightson P. Delayed recovery of intellectual function after minor head injury. Lancet. 1974;304(7881):605–9.
Rabadi M, Jordan B. The cumulative effect of repetitive concussion in sports. Clin J Sports Med. 2001;11(3):194–8.
Austin D, Gabbett T, Jenkins D. Tackling in professional rugby league. J Strength Cond Res. 2011;25(6):1659–63.
Dretsch MN, Silverberg ND, Iverson GL. Multiple past concussions are associated with ongoing post-concussive symptoms but not cognitive impairment in active-duty army soldiers. J Neurotrauma. 2015;32(17):1301–6.
Arciniegas DB, Anderson CA, Topkoff J, McAllister TW. Mild traumatic brain injury: a neuropsychiatric approach to diagnosis, evaluation, and treatment. Neuropsychiatr Dis Treat. 2005;1:311–27.
Fleminger S, Ponsford J. Long term outcome after traumatic brain injury. Br Med J. 2005;331:1419–20.
Decq P, Gault N, Blandeau M, Kerdraon T, Berkal M, ElHelou A, et al. Long-term consequences of recurrent sports concussion. Acta Neurochir (Wien). 2016;158(2):289–300.
De Beaumont L, Brisson B, Lassonde M, Jolicoeur P. Long-term electrophysiological changes in athletes with a history of multiple concussions. Brain Inj. 2007;21:631–44.
De Beaumont L, Lassonde M, Leclerc S, Théoret H. Long-term and cumulative effects of sports concussion on motor cortex inhibition. Neurosurgery. 2007;61(2):329–36.
De Beaumont L, Theoret H, Mongeon D, Messier J, Leclerc S, Tremblay S, et al. Brain function decline in healthy retired athletes who sustained their last sports concussion in early adulthood. Brain. 2009;132(Pt 3):695–708.
Dean PJA, Steer A. Long-term effects of mild traumatic brain injury on cognitive performance. Front Hum Neurosci. 2013;7:30.
McCrory P, Meeuwisse WH, Kutcher JS, Jordan BD, Gardner A. What is the evidence for chronic concussion-related changes in retired athletes: behavioural, pathological and clinical outcomes? Br J Sports Med. 2013;47:327–30.
Alexander DG, Shuttleworth-Edwards AB, Kidd M, Malcolm CM. Mild traumatic brain injuries in early adolescent rugby players: long-term neurocognitive and academic outcomes. Brain Inj. 2015;29(9):1113–25.
Shuttleworth-Edwards AB, Radloff SE. Compromised visuomotor processing speed in players of Rugby Union from school through to the national adult level. Arch Clin Neuropsychol. 2008;23(5):511–20.
Guskiewicz KM, Marshall SW, Bailes J, McCrea M, Cantu RC, Randolph C, et al. Association between recurrent concussion and late-life cognitive impairment in retired professional football players. Neurosurgery. 2005;57(4):719–26.
Statistics New Zealand. Statistics New Zealand census data. Wellington. Statistics New Zealand. 2006. http://www.stats.govt.nz/Census/about-2006-census/information-by-variable/cigarette-smoking-behaviour.aspx. Accessed 15 Dec 2014.
Kerr ZY, Mihalik JP, Guskiewicz KM, Rosamond WD, Evenson KR, Marshall SW. Agreement between athlete-recalled and clinically documented concussion histories in former collegiate athletes. Am J Sport Med. 2015;43(3):606–13.
Kerr Z, Marshall S, Guskiewicz K. Reliability of concussion history in former professional football players. Med Sci Sport Exerc. 2012;44(3):377–82.
Kerr Z, Marshall S, Harding HJ, Guskiewicz K. Nine-year risk of depression diagnosis increases with increasing self-reported concussions in retired professional football players. Am J Sport Med. 2012;40(10):2206–12.
Arnaiz E, Almkvist O, Ivnik RJ, Tangalos EG, Wahlund LO, Winblad B, et al. Mild cognitive impairment: a cross-national comparison. J Neurol Neurosurg Psychiatry. 2004;75(9):1275–80.
Bruscoli M, Lovestone S. Is MCI really just early dementia? A systematic review of conversion studies. Int Psychogeriatr. 2004;16(2):129–40.
Quarrie KM, Gianotti S, Hopkins WG, Hume PA. Effect of nationwide injury prevention programme on serious spinal injuries in New Zealand rugby union. Br Med J. 2007;334:1150–3.
King DA, Hume PA, Brughelli M, Gissane C. Instrumented mouthguard acceleration analyses for head impacts in amateur rugby union players over a season of matches. Am J Sports Med. 2015;43(3):614–24.
King DA, Hume PA, Gissane C, Clark T. Similar head impact acceleration measured using instrumented ear patches in a junior rugby union team during matches in comparison with other sports. J Neurosurg Pediatr. 2016;18(1):65–72.
King D, Brughelli M, Hume PA, Gissane C. Concussions in amateur rugby union identified with the use of a rapid visual screening tool. J Neurol Sci. 2013;326(1–2):59–63.
King D, Gissane C, Hume PA, Flaws M. The King-Devick test was useful in management of concussion in amateur rugby union and rugby league in New Zealand. J Neurol Sci. 2015;351(1–2):58–64.
Acknowledgments
We thank Dr Martin Raftery (World Rugby/International Rugby Board [IRB]) for initiating the IRB/New Zealand Rugby/Auckland University of Technology (IRB/NZR/AUT) RugbyHealth project and for providing feedback on the technical report that formed the basis of this article. Thanks to Peter Griffiths and Serene Lorimer who provided research administration for the project, Dr Ian Murphy (New Zealand Rugby), Heath Mills (New Zealand Rugby Players Association) and Rob Nichol (New Zealand Cricket Players Association) who endorsed the project and helped with promotion of the study and recruitment of players. We also gratefully recognise the support of Alan Boyd, Chief Executive Officer (CEO) of CNS-VS, for his support and for providing advice on the analysis and interpretation of the data.
Contributors
Professor Patria Hume collaborated in designing the overarching IRB/NZR/AUT RugbyHealth project, was responsible for the original conception of the study, wrote the funding application, obtained ethical approval, helped recruit participants, helped with analyses of data, provided interpretation of the results, and co-authored the manuscript. Dr Alice Theadom determined the assessment protocols, helped recruit participants, provided interpretation of the results, and co-authored the manuscript. Associate Professor Gwyn Lewis helped recruit participants, helped with analyses of data, provided interpretation of the results, and co-authored the manuscript. Dr Ken Quarrie (New Zealand Rugby) initiated the IRB/NZR/AUT RugbyHealth project, analysed the data, provided interpretation of the results, and co-authored the manuscript. Scott Brown provided liaison for participants for the study, helped recruit participants, and co-authored the manuscript. Dr Rosamund Hill provided clinical interpretation advice and co-authored the manuscript. Professor Stephen Marshall provided statistical advice and co-authored the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The study was funded by World Rugby (IRB), the Sport Performance Research Institute New Zealand (SPRINZ), the National Institute for Stroke and Applied Neurosciences (NISAN), and the Health and Rehabilitation Research Institute (HRRI) of AUT, and NZR.
Competing interests
Kenneth L. Quarrie was employed by NZR prior to and throughout the duration of the project. World Rugby and NZR provided funding for the project. Patria A. Hume, Alice Theadom, Gwyn N. Lewis, Scott R. Brown, Rosamund Hill and Stephen W. Marshall declare that they have no conflicts of interest.
Ethical approval
The study was performed in accordance with the ethical standards of the Declaration of Helsinki, given ethics approval was obtained from the AUT Ethics Committee (AUTEC #12/252). Participants provided informed consent after reading a participant information sheet about the project.
Additional information
This article is part of the Topical Collection on Rugby Health.
Rights and permissions
About this article

Cite this article
Hume, P.A., Theadom, A., Lewis, G.N. et al. A Comparison of Cognitive Function in Former Rugby Union Players Compared with Former Non-Contact-Sport Players and the Impact of Concussion History. Sports Med 47, 1209–1220 (2017). https://doi.org/10.1007/s40279-016-0608-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-016-0608-8