
Abstract
Purpose
Prophylactic antibiotics (PA) and immunoglobulin replacement (IGRT) are commonly used in specific antibody deficiency (SAD); however, optimal treatment is not well-established. Our purpose is to compare treatment outcomes with IGRT and/or PA among SAD patients.
Methods
A retrospective chart review of SAD patients treated at two tertiary centers between January 2012 and May 2017 was performed. Clinical and laboratory data, and rates of infections prior to and after treatment with IGRT or PA were analyzed. Descriptive analyses, between-group comparisons of rates of infection after 1 year of treatment, and a stepwise logistic regression model were employed to explore factors contributing to treatment outcomes.
Results
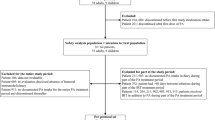
We identified 65 SAD patients with mean age were 18 years (2–71 years). The baseline mean number of infections in the PA group and IGRT group was 4.71 (SD 3.15) and 7.73 (SD 6.65), respectively. Twenty-nine (44.6%) received IGRT, 7 (10.7%) received PA, 7 (10.7%) received both IGRT and PA, 15 (23.1%) failed PA and switched to IGRT, and 7 did not receive any specific treatment. After 1 year of treatment, the difference in the mean number of infections in PA vs. IGRT was not statistically significant [2.86 (2.73) vs. 4.44 (4.74), p = 0.27]. Reporting autoimmunity increased the odds for persistent infections (OR = 4.29; p = 0.047), while higher IgG levels decreased the odds for persistent infections (OR = 0.68, p = 0.018).
Conclusions
PA and IGRT are equally effective as first line in preventing infections in SAD patients. However, patients who fail PA would benefit from IGRT.


Similar content being viewed by others


Abbreviations
- SAD:
-
Specific antibody deficiency
- PA:
-
Prophylactic antibiotics
- IGRT:
-
Immunoglobulin replacement therapy
- TCH:
-
Texas Children’s Hospital
- CHOP:
-
Children’s Hospital Philadelphia
- PID:
-
Primary immunodeficiency
References
Ambrosino DM, Siber GR, Chilmonczyk BA, Jernberg JB, Finberg RW. An immunodeficiency characterized by impaired antibody responses to polysaccharides. N Engl J Med. 1987;316:790–3.
Epstein MM, Gruskay F. Selective deficiency in pneumococcal antibody response in children with recurrent infections. Ann Allergy Asthma Immunol. 1995;75:125–31.
Zora JA, Silk HJ, Tinkelman DG. Evaluation of postimmunization pneumococcal titers in children with recurrent infections and normal levels of immunoglobulin. Ann Allergy. 1993;70:283–8.
Sanders LA, Rijkers GT, Kuis W, Tenbergen-Meekes AJ, de Graeff-Meeder BR, Hiemstra I, et al. Defective antipneumococcal polysaccharide antibody response in children with recurrent respiratory tract infections. J Allergy Clin Immunol. 1993;91:110–9.
Hidalgo H, Moore C, Leiva LE, Sorensen RU. Preimmunization and postimmunization pneumococcal antibody titers in children with recurrent infections. Ann Allergy Asthma Immunol. 1996;76:341–6.
Gross S, Blaiss MS, Herrod HG. Role of immunoglobulin subclasses and specific antibody determinations in the evaluation of recurrent infection in children. J Pediatr. 1992;121:516–22.
Orange JS, Ballow M, Stiehm ER, Ballas ZK, Chinen J, De La Morena M, et al. Use and interpretation of diagnostic vaccination in primary immunodeficiency: a working group report of the Basic and Clinical Immunology Interest Section of the American Academy of Allergy, Asthma & Immunology. J Allergy Clin Immunol. 2012;130:S1–24.
Perez E, Bonilla FA, Orange JS, Ballow M. Specific antibody deficiency: controversies in diagnosis and management. Front Immunol. 2017;8:586.
Bonilla FA, Khan DA, Ballas ZK, Chinen J, Frank MM, Hsu JT, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol. 2015;136:1186–205 e1-78.
Javier FC III, Moore CM, Sorensen RU. Distribution of primary immunodeficiency diseases diagnosed in a pediatric tertiary hospital. Ann Allergy Asthma Immunol. 2000;84:25–30.
Modell V, Knaus M, Modell F, Roifman C, Orange J, Notarangelo LD. Global overview of primary immunodeficiencies: a report from Jeffrey Modell Centers worldwide focused on diagnosis, treatment, and discovery. Immunol Res. 2014;60:132–44.
Bonilla FA, Bernstein IL, Khan DA, Ballas ZK, Chinen J, Frank MM, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. Ann Allergy Asthma Immunol. 2005;94:S1–63.
Bonilla FA, Khan DA, Ballas ZK, Chinen J, Frank MM, Hsu JT, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol. 2015;136:1186–205 e78.
Leiva LE, Monjure H, Sorensen RU. Recurrent respiratory infections, specific antibody deficiencies, and memory B cells. J Clin Immunol. 2013;33(Suppl 1):S57–61.
Orange JS, Ochs HD, Cunningham-Rundles C. Prioritization of evidence-based indications for intravenous immunoglobulin. J Clin Immunol. 2013;33:1033–6.
Bayry J, Kazatchkine MD, Kaveri SV. Shortage of human intravenous immunoglobulin—reasons and possible solutions. Nat Clin Pract Neurol. 2007;3:120–1.
Orange JS, Grossman RJ, Navickis MM, Wilkes WJ. Impact of trough IgG on pneumonia incidence in primary immunodeficiency: a meta-analysis of clinical studies. Clin Immunol. 2010;137:21–30 SRC - GoogleScholar.
Azizi G, Ahmadi M, Abolhassani H, Yazdani R, Mohammadi H, Mirshafiey A, et al. Autoimmunity in primary antibody deficiencies. Int Arch Allergy Immunol. 2016;171:180–93.
Farmer JR, Ong MS, Barmettler S, Yonker LM, Fuleihan R, Sullivan KE, et al. Common variable immunodeficiency non-infectious disease endotypes redefined using unbiased network clustering in large electronic datasets. Front Immunol. 2017;8:1740.
Wilson SP, Ballas ZK. Progression of specific antibody deficiency (SAD) to common variable immunodeficiency (CVID). J Allergy Clin Immunol. 2010;125:AB73.
Acknowledgments
The research is partially supported by the Jeffery Modell Foundation, and supported in part by the Intramural Research Program of the NIH, NIAID. Joud Hajjar received the USIDnet and the Clinical immunology society travel grants for an oral presentation summarizing this work.
Authorship Contributions
Conceptualization: [Joud Hajjar]; Methodology: [Joud Hajjar], Formal analysis and investigation: [Joud Hajjar, Carleigh Kutac, An Nguyen, Gregory Constantine, Maha Syed and Kathleen Sullivan], Writing—original draft preparation: [Joud Hajjar, Maha Syed]; Writing—review and editing: [all authors]; Supervision: [Joud Hajjar, Jordan Orange and Kathleen Sullivan].
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 24 kb)
Rights and permissions
About this article

Cite this article
Joud Hajjar, Nguyen, A.L., Constantine, G. et al. Prophylactic Antibiotics Versus Immunoglobulin Replacement in Specific Antibody Deficiency. J Clin Immunol 40, 158–164 (2020). https://doi.org/10.1007/s10875-019-00716-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-019-00716-2